
Abstract
Background/Aim:
To compare the effectiveness ceftaroline-rifampicin (CR) and vancomycin-rifampicin (VR), against methicillin-resistant Staphylococcus aureus (MRSA) in a rabbit meningitis model, to compare the effects on brain tissues in terms of inflammation and apoptosis and to test the antibiotics via in vitro time-kill and synergy tests.
Method:
Meningitis was induced using MRSA strain ATCC 43300. After 28 hours, the rabbits were split into three groups: control, VR, and CR. A CSF culture was taken at the start (T0) and end of treatment (EOT)—the 24th hour of treatment. At EOT, the animals’ brain tissues were examined for inflammation and apoptosis. The study strain was tested for a 24-hour time kill assay.
Results:
At the EOT, statistically significant differences were observed between the treatment groups in terms of reducing the cerebrospinal fluid (CSF) bacterial count, achieving partial or complete treatment response, and exhibiting lower levels of neuronal apoptosis compared with the control group. However, there was no significant difference in all three parameters and in survival between the two treatment groups. The CR group exhibited a noticeable decrease in inflammation than the control group, but no significant difference was found between the control group versus VR and VR versus CR group. Rifampicin did not improve antibacterial efficacy in the in vitro time-kill assay.
Conclusion:
The CR arm showed better complete response and inflammation, but both treatments were similar in other parameters. CR combination was found as effective as VR combination for treating MRSA meningitis.
Introduction
Healthcare-associated central nervous system infections are severe and cause mortality rates ranging from 20% to 55%. Methicillin-resistant Staphylococcus aureus (MRSA) is a common cause of this condition. 1 Current guidelines recommend vancomycin as the preferred initial therapy for MRSA meningitis, with linezolid, daptomycin, and trimethoprim/sulfamethoxazole as alternatives. Rifampicin enhances the effectiveness of combined antibiotics such as vancomycin and is recommended for use in infected CSF shunts or drainage catheters.2–4
Fifth-generation cephalosporins, ceftaroline and ceftobiprole are effective against MRSA. Ceftaroline is U.S. Food and Drug Administiration (FDA) approved for certain infections but lacks extensive data on MRSA-related central nervous system (CNS) infections, with limited case-report evidence and no comparative studies with rifampicin.5,6
Herein, we investigated the antibacterial and antiapoptotic effects of ceftaroline-rifampicin (CR) and vancomycin-rifampicin (VR) combinations in a rabbit MRSA meningitis model.
Materials and Methods
Meningitis model in rabbits
This study utilized Dacey and Sande’s experimental meningitis model.7–9 White New Zealand rabbits (2.5–3 kg) were anesthetized with ketamine (35 mg/kg) and xylazine (5 mg/kg) via intramuscular injection.8,10 After 10–15 minutes, MRSA strain ATCC 43300 [vancomycin minimum inhibitory concentration (MIC): 1 mg/L, ceftaroline MIC: 1 mg/L, rifampicin MIC: 0.01 mg/L] was injected intracisternally (0.3 mL; 3 × 107 cfu/mL) using a 22 G spinal needle (Hayat Ticaret, Istanbul, Turkey) to cause meningitis.7–9,11–13 After inoculation, 28 hours were waited for the development of infection. The presence of ≥103 cfu/mL and pleocytosis in the CSF samples at the start of antibiotic treatment (T0 = 28 h after bacterial inoculation) indicated meningitis.8,10
The rabbits were divided into three groups: a control group and two treatment groups (VR and CR). The control group received no antibiotics. VR group was administered 20 mg/kg IV vancomycin (Vancotek®, Koçak Farma) and 15 mg/kg oral rifampicin (Rifcap®, Koçak Farma) via nasogastric catheter, both at T0 and fifth hours. CR group received 58 mg/kg of ceftaroline (Omvelin®, Pfizer, Istanbul, Turkey) every 12 hours as a 12-hour IV infusion, and rifampicin at the same dose and frequency. Dose selection aimed to maintain serum peak and trough concentrations similar to human observations.10,14,15
CSF sampling was conducted at T0 and after 24 hours of treatment (EOT). 9 At the EOT, all animals were humanely euthanized using high-dose anesthetics (ketamine and xylazine). 16
Evaluation of antibacterial activity
CSF samples were collected at T0 and EOT. The number of white blood cells per cubic millimeter was measured, and quantitative bacterial culture was performed on sheep blood agar at full and 1/10 dilutions with saline. The bacterial colonies were counted after 48 hours of incubation at 37°C. 13 At EOT, complete response was defined as no growth, partial response as a decrease in bacteria, and non-response as no change or increase.8,10
Evaluation of apoptosis
Histological analysis
Brain tissues from sacrificed rabbits were fixed in 4% paraformaldehyde at 4°C for 24 hours for light microscopy. 16 Then tissues were dissected and transferred into the same fixation solution for 24 hours and underwent subsequent routine histological procedure and embedded in paraffin. Afterward, 5 μm sections were obtained with a microtome (Leica RM2145, Germany) and stained with hematoxylin-eosin (H&E) and cresyl violet (Sigma C5042).
TUNEL technique
Apoptotic cells in cerebral tissues were detected and counted using the terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL) technique with the Roche in situ Cell Death Detection Kit, POD (Roche, Mannheim, Germany). TUNEL positivity was assessed by light microscopy (BX-51 light microscope, C-5050 digital camera; Olympus, Melville, NY, USA) at a magnification of ×400. 17
In vitro time-kill analysis and synergy testing
We performed time-kill assay with macrodilution method.13,18 The antibiotics (rifampicin, ceftaroline, and vancomycin) were tested at MICX1 and MICX5 of their respective MIC values. Also, in vitro synergy tests were conducted using CR and VR combinations, with final concentrations tested at MICX1 and MICX5.
We revived the ATCC 43300 MRSA strain in sterile human serum and diluted it to a bacterial density of approximately 104 cfu/mL, similar to that detected in the CSF of rabbits at T0. 13 Samples were cultured twice in 5% sheep blood agar at 0, 2, 8, 12, and 24 hours. After 24 hours of incubation at 37°C, bacteria count per cubic millimeter was determined. The average bacterial colony counts from twice-inoculated samples were converted to log10 to generate a time-based killing curve.19,20 Bactericidal effect was defined as ≥3 log10 cfu decrease after 24 hours.20,21 Lorian’s criteria for synergism, additive effect, and antagonism were applied.18,22–24
Statistical evaluation
The statistical analysis was done using IBM SPSS 25.0 software. Colony counts in CSF and the decrease in colony counts were evaluated using Mann-Whitney U and Kruskal-Wallis tests, respectively, for continuous variables. Fisher exact test, exact chi-square tests were used for evaluating categorical variables such as death and bacteriological response.
To count TUNEL (+) cells, 10 different areas of 10 sections were counted at ×400 magnification and averaged. Inflammatory cells were also counted at ×400 magnification and scored: 0: <3, 1: 3–10, 2: 11–20, 3: 21–30, 4: 31–40, and 5: >41 cells. Shapiro-Wilk test was performed for normality test. Normally distributed data were tested with one-way analysis of variance. The homogeneity of variances was tested by Levene’s test for the data with significant results between groups. Pairwise comparisons were made with Bonferroni post hoc test for groups with equal variance and Dunnett T3 post hoc test for those without equal variance. The significance level was determined as p ≤ 0.05.
Ethical approval
The study was approved by the Ege University Animal Experiments Local Ethics Committee (No. 2018-007).
Results
In vivo tests
Meningitis model in rabbit
The study started with 42 rabbits. At the end of the 28-hour incubation period (T0), 26 animals fulfilled the above defined criteria for meningitis (Table 1).
Distribution and Survival of Rabbits According to Groups at 0th (T0) and 24th (EOT) Hour
EOT = end of treatment.
Mean number of bacteria in the rabbit CSF at the T0 was similar in the three groups (p: 0.506). At EOT, a significant decrease in bacterial concentrations was observed in both treatment groups, compared with the control group (p: 0.034). However, there was no significant difference between the two treatment groups (p: 0.541). Furthermore, the difference in the mean colony counts of the three groups at EOT was significant (p: 0.00144; Table 2).
Bacteriological Evaluation of CSF Samples
Bacteria quantities are expressed as colony forming units in log10.
No significant difference in between the three groups at the T0 (p: 0.506).
The log10 equivalent of the rabbits with a colony count of 0 at the end of the treatment, was considered to be 0, but not "undefined. Significant difference in the mean colony counts of the three groups at EOT (p: 0.00144).
No significant difference between VR vs. CR (p: 0.541).
EOT = end of treatment; VR = vancomycin-rifampicin; CR = ceftaroline-rifampicin.
When evaluating the three groups in terms of their partial or complete response (considering animals with T0 data but died before the EOT as non-responders), a significant difference was observed between the three groups (CR: 9/10 vs. VR: 7/8 vs. C: 1/8, p: 0.000788). The difference in complete or partial response between the control group and the CR group (C: 1/8 vs. CR: 9/10, p: 0.0029) as well as the control group versus the VR group (C:1/8 vs. VR:7/8, p: 0.0101) was statistically significant. However, there was no significant difference between the two treatment groups (VR: 7/8 vs. CR: 9/10, p: 1).
In terms of complete response, the CR group showed a significant difference when compared with the control group (CR: 7/10 vs. C: 0/8, p: 0.004). However, there was no significant difference between the VR group and the control group (VR: 3/8 vs. C: 0/8, p: 0.200) or between the CR and VR groups (CR: 7/10 vs. VR: 3/8, p: 0.341).
There was no statistically significant difference in EOT mortality among the three groups (p: 0.288), between the VR group and the control group (p: 0.558), the CR group and the control group (p: 1), or the VR and CR groups (p: 0.466) (Table 1).
Histopathological evaluation
Hematoxylin-eosin and cresyl echt violet staining
Vasogenic, cytotoxic and interstitial edema, and related neuronal damage developed only in the control group. The meningeal vessels displayed dilatation, pleocytosis, edema, and intense inflammation (Figs. 1 and 2, Table 3). Vascular damage, edema, and hemorrhage were observed deep in the cortex and choroid plexus (Fig. 1). Throughout the hippocampal tissue, widespread edema and dilatation of the vessels were observed. In the cornu ammonis (CA) 2, CA3, and CA4 regions, degeneration of neurons was accompanied by disruption of cell rows because of edema, particularly in the CA3 and CA4 regions. Mossy fibers and Schaffer collateral fibers were decreased and their organization was disrupted (Fig. 3). Cresyl echt staining revealed that Nissl granules of hippocampal pyramidal neurons had an appearance compatible with chromatolysis (Fig. 3).
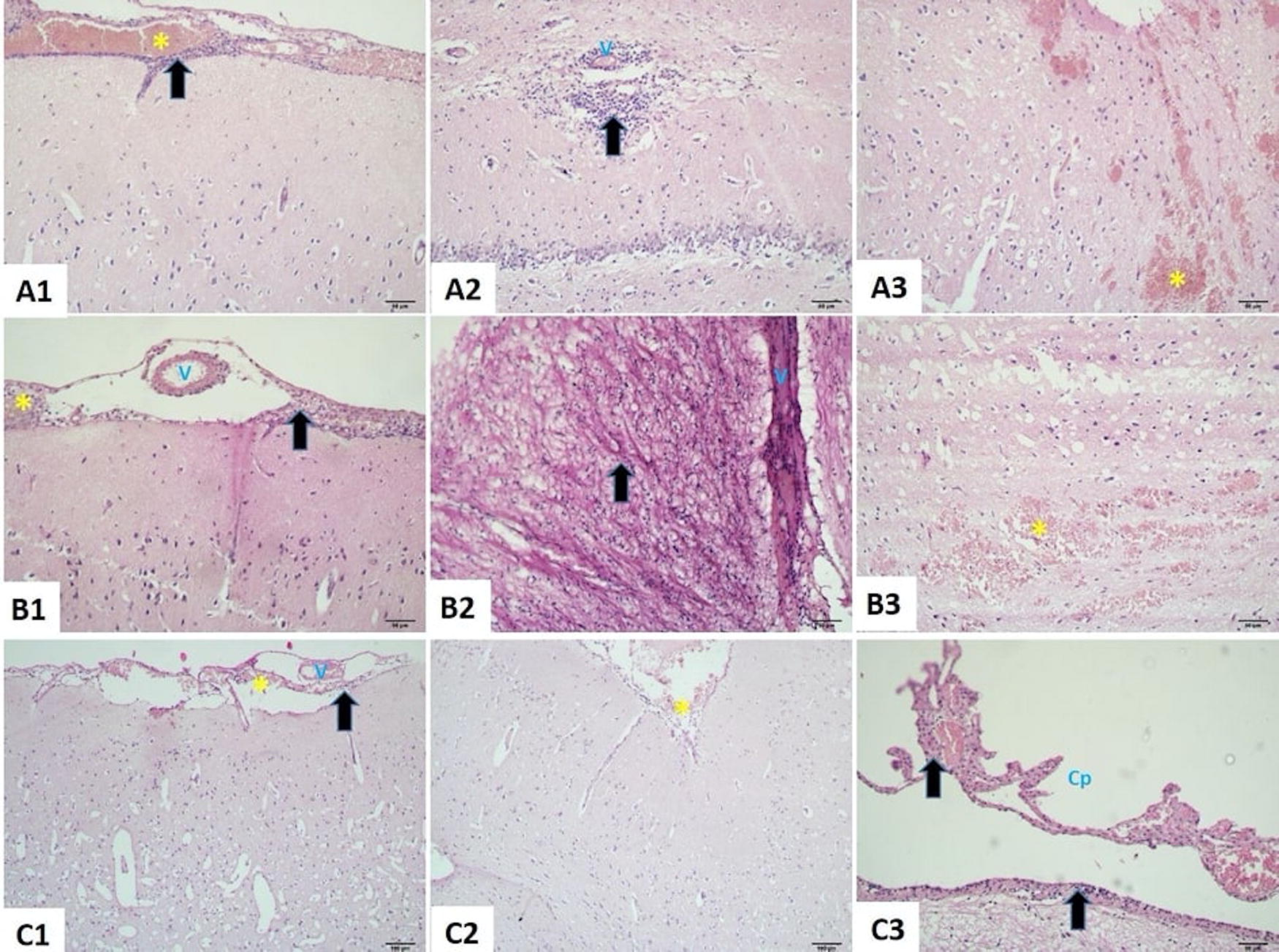
Histopathological appearance of the experimental groups with H&E staining.

Distribution of leukocyte infiltration according to groups. Star = p < 0.05 versus control; SD = standard deviation.
Statistical Analysis of Histological Findings
Data are presented as mean ± standard deviation. n = 7.
p < 0.05 versus control.
Control versus CR: p: 0.032; control versus VR: p: 0.98; VR versus CR: p: 0.247.
VR = vancomycin-rifampicin; CR = ceftaroline-rifampicin; TUNEL = terminal deoxynucleotidyl transferase dUTP nick end labeling.
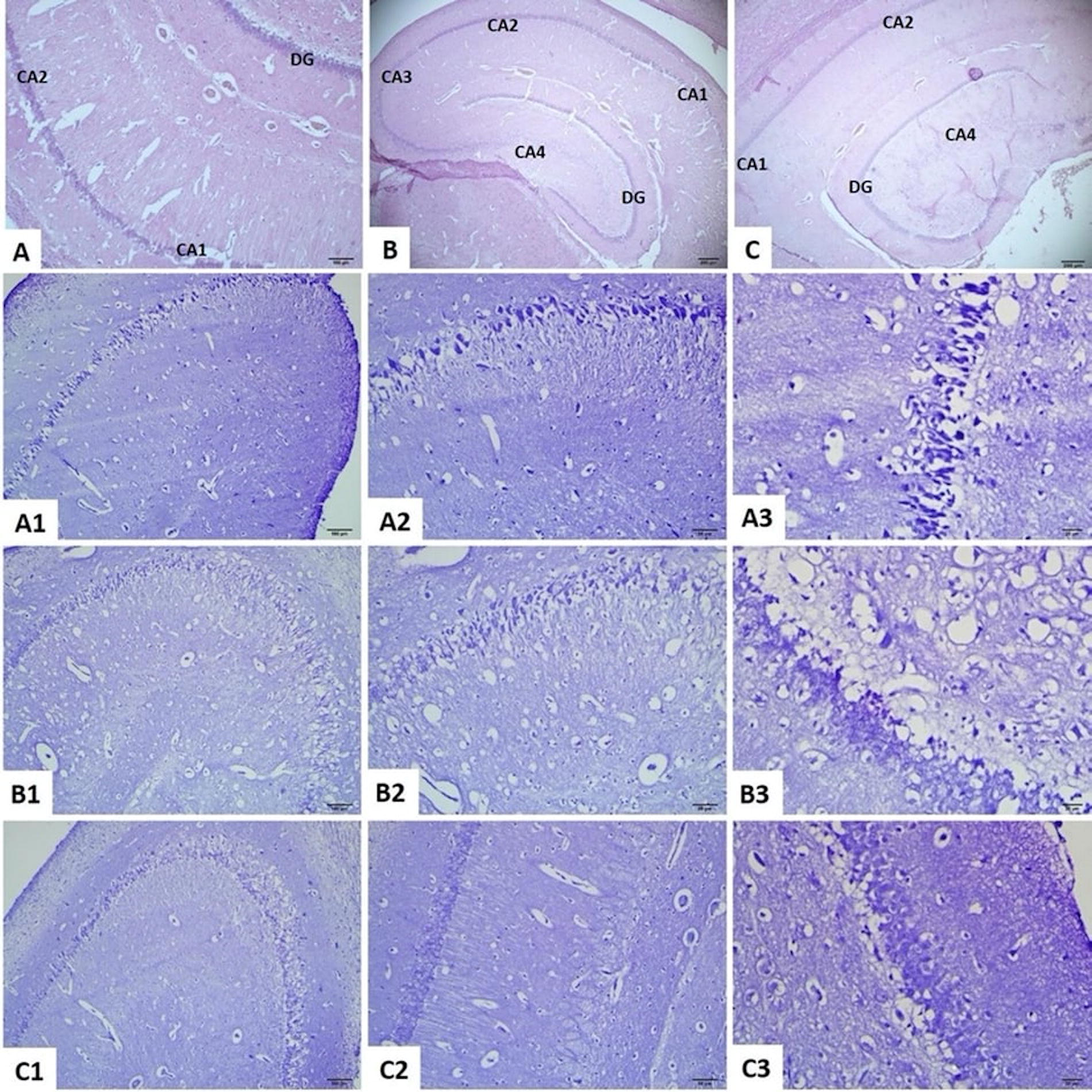
Histopathological appearance of the hippocampal area in the experimental groups with H&E and cresyl echt violet staining.
Inflammation in the meninges decreased significantly in the comparison of CR group versus control group (p = 0.032) but not in the VR group versus control group (p = 0.987) (Figs. 1 and 2, Table 3). Although dilatation, pleocytosis, and edema were observed in the vessels, these findings were attenuated when compared with the control group. Vascular damage and hemorrhage were found deep in the cortex in the VR group, whereas no hemorrhagic area was found in the CR group. Moderate inflammation and edema were observed in the choroid plexus in the VR group, and mild inflammation was observed in the CR group (Fig. 1). In both groups, degeneration of neurons in CA3 and CA4 and disruption of cell lineages were observed in the hippocampal area, accompanied by moderate to diffuse edema. Edema and loss of Mossy fibers and Schaffer collateral fibers were at a low level (Fig. 3). Chromatolysis-like changes in hippocampal neurons were less in both treatment groups compared with the control group, and normal cells were found in many areas (Fig. 3).
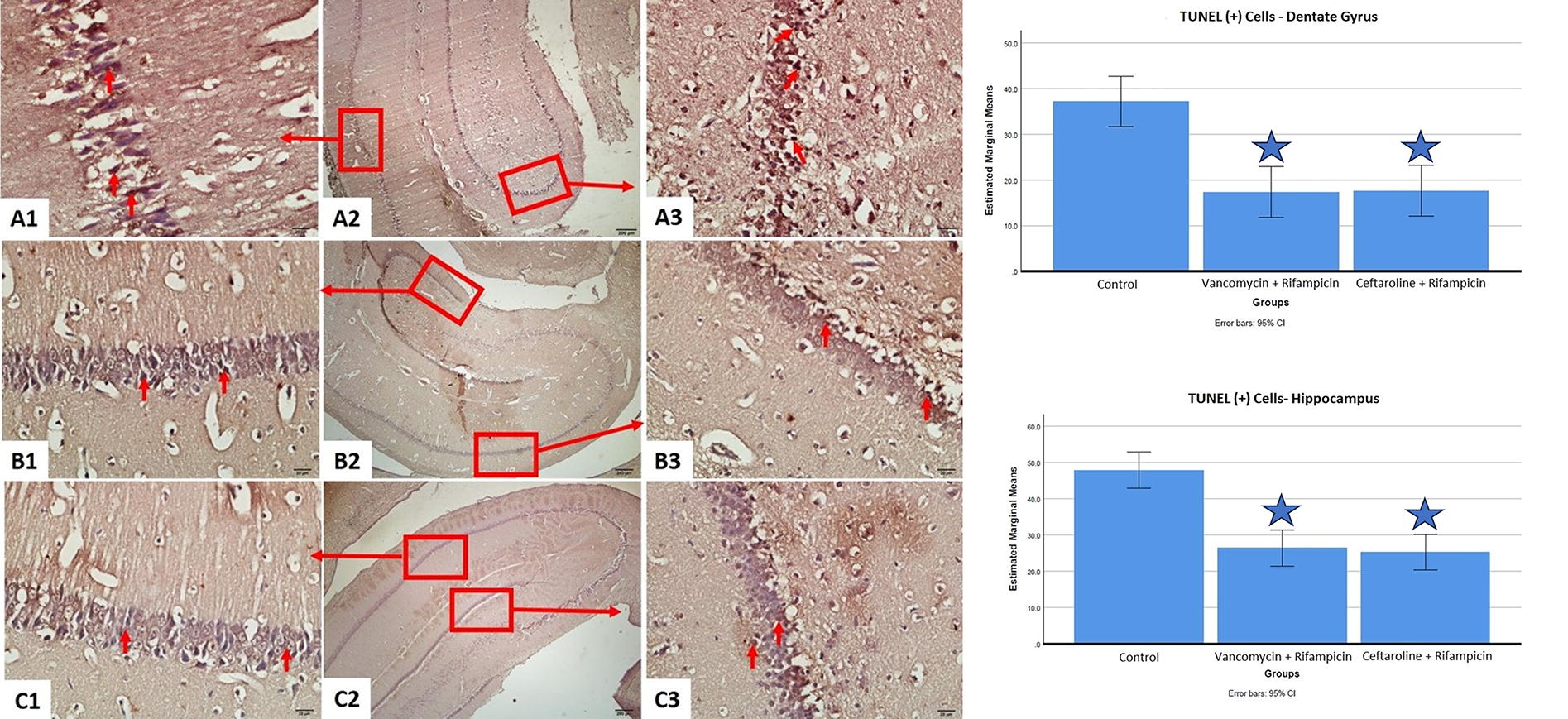
Histopathological appearance of the experimental groups with TUNEL staining and comparison of TUNEL (+) cell count in dentate gyrus and hippocampus.
TUNEL staining
In the control group, TUNEL-positive cells were observed throughout the hippocampus, with a greater density in CA3 and CA4 (Fig. 4). In the VR and CR groups, TUNEL-positive cells were also more concentrated in CA3 and CA4, but significantly fewer in number compared with the control group (respectively, p < 0.001 and p < 0.001; Fig. 4). However, when comparing the two treatment groups, there was no significant difference in the number of TUNEL-positive cells in both the hippocampus and dentate gyrus (p > 0.999; Table 3).
Evaluation of inflammation score
In the control group, leukocyte infiltration was significantly greater compared with the CR but similar to VR. There was no significant difference between the VR versus CR groups (Fig. 2 and Table 3).
In vitro tests
Time-kill assay
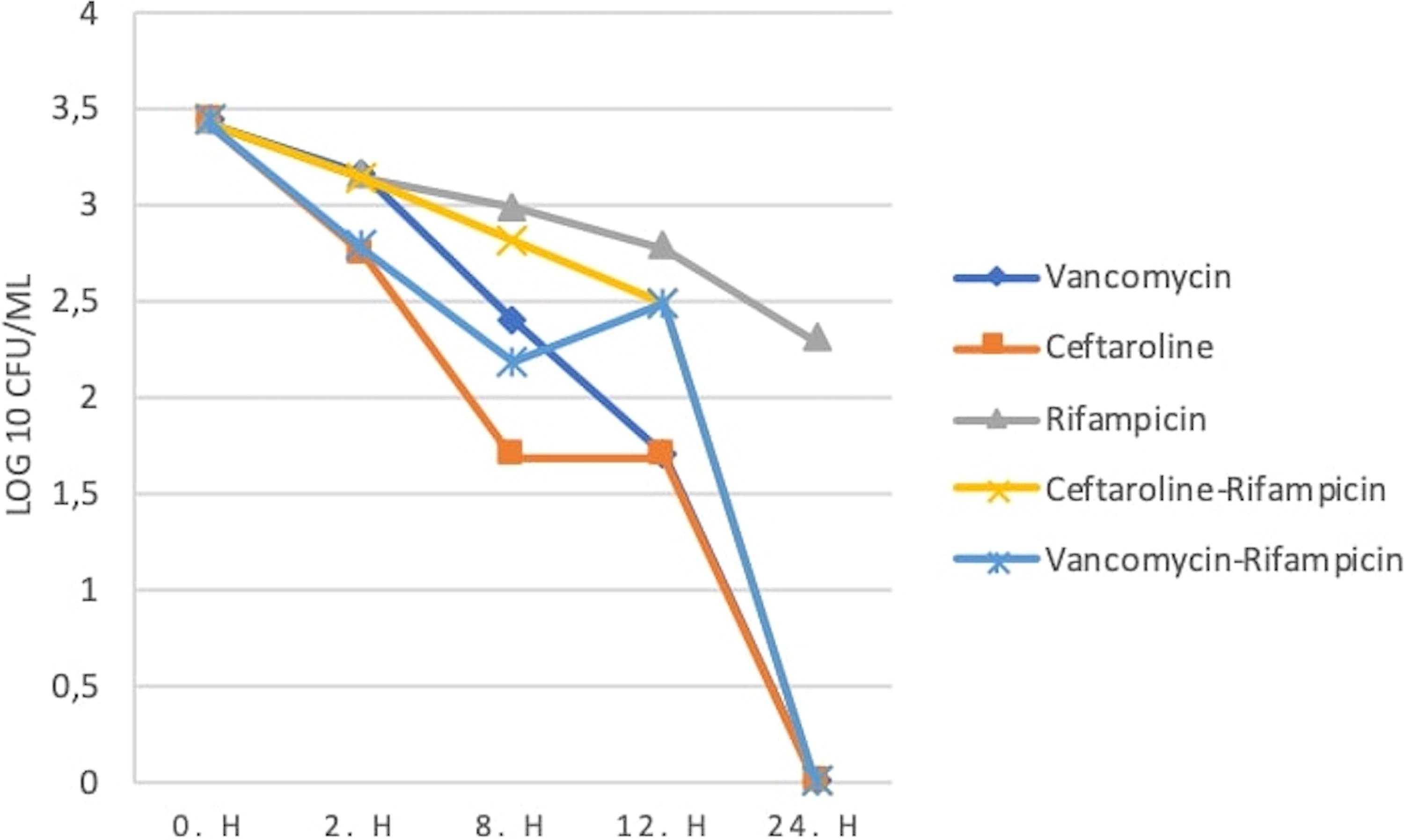
In the in vitro time-kill assay, sterility was achieved within 24 hours using vancomycin and ceftaroline at MICX1 and MICX5 concentrations (see Figs. 5 and 6).

In vitro time-dependent killing curve (MICX1) of the antibiotics used in the experiment on ATCC 43300 MRSA strain *, **. *MIC equivalent concentrations were used for single or combined use of antibiotics (vancomycin: 1 mg/L, ceftaroline: 1 mg/L, rifampicin: 0.01 mg/L). **in log10 (the log10 equivalent of those with a bacterial count of 0 was considered to be 0, but not undefined). MRSA = methicillin-resistant Staphylococcus aureus.
In vitro time-dependent killing curve (MICX5) of the antibiotics used in the experiment on ATCC 43300 MRSA strain *, **. *In single or combined use of antibiotics, concentrations five times the MIC values were used (vancomycin: 5 mg/L, ceftaroline: 5 mg/L, rifampicin: 0.05 mg/L). **in log10 (the log10 equivalent of those with a bacterial count of 0 was considered to be 0, but not undefined). MRSA = methicillin-resistant Staphylococcus aureus.
Although the concentration of rifampicin at MICX5 did not achieve sterility, bacterial count decreased after 24 hours. In contrast, MICX1 showed no reduction and even a slight increase after 24 hours (Figs. 5 and 6). Vancomycin-rifampicin combination at MICX1 and MICX5 concentrations sterilized within 24 hours (Figs. 5 and 6). Ceftaroline-rifampicin combinations decreased bacteria numbers in all concentrations but only MICx5 sterilized (Figs. 5 and 6).
Synergy test
Vancomycin-rifampicin and CR combinations decreased bacterial concentration compared with baseline. Compared with individual drugs, the combinations had an additive but not synergistic or antagonistic effect (Figs. 5 and 6).
Discussion
MRSA meningitis has high mortality rates (10%–42.8%) because of antibiotic resistance and the difficulty of major antibiotics in crossing the blood-brain barrier.25,26 Although vancomycin and rifampicin are primary treatments, they may fail, necessitating new options.3,4,27,28
Animal studies, case reports, and off-label use support ceftaroline’s potential unapproved use for severe infections such as meningitis and endocarditis.29,30 Several studies have examined the effect of CR combination on resistant gram-positive bacteria, but no data exist for MRSA meningitis.21,31,32 Our study used rabbits to compare CR with VR. Both groups received antibiotics simulating human pharmacokinetics.14,15,33–37 Rifampicin was administered orally because of lack of IV form.10,38,39
Three studies have tested ceftaroline’s effectiveness in treating meningitis. Cottagnoud et al. compared ceftaroline with ceftriaxone and a ceftriaxone-vancomycin combination (CV) in penicillin-sensitive and resistant pneumococcal meningitis. 33 In an eight-hour experiment, ceftaroline 40 mg/kg and vancomycin 20 mg/kg were administered at zeroth and fourth hour. Ceftaroline resulted in a greater bacterial reduction in penicillin-susceptible strains than ceftriaxone (p: <0.05). Ceftaroline also outperformed the CV in the penicillin-resistant group, with a greater bacterial reduction and killing rate (respectively; p: 0.03, p < 0.009). Ceftaroline CSF penetration was 14%. Stucki et al. found that ceftaroline had a significantly greater bacterial killing rate than cefepime in meningitis models caused by Klebsiella pneumoniae (K. pneumoniae) and Escherichia coli (E. coli) (respectively; p < 0.007, p < 0.0016). 40 The MIC values predicted the results in the E. coli-infected arm, but why the K. pneumoniae-infected arm with a greater ceftaroline MIC had greater bactericidal activity was unclear. Our experiment did not show any significant difference between the VR and CR arms. Compared with the above-mentioned studies, both arms had relatively less decrease in CSF bacterial load, which may be associated with differences in bacterial strains, antibiotic dose, and duration.
Mermer et al. examined the antibacterial effect of ceftaroline and vancomycin on MRSA meningitis. 9 After 24 hours, no significant difference was found between the two groups, similar to our study. But, decrease rates were non-significantly greater in our study. The greater dose of ceftaroline given to rabbits and the addition of rifampicin might have led to a greater decrease in bacterial load.21,33,40 However, comparing our data with Mermer et al.’s, no significant difference was found in initial bacterial counts (p: 0.173) or between the vancomycin monotherapy versus VR and CR arms in both studies (p: 0.203; p: 0.072). The ceftaroline arm in their study also showed no significant difference compared with our VR and CR arms (p: 0.104; p: 0.230).
Multiple studies assessed the effectiveness of VR combination in MRSA meningitis. Sato et al. tested the efficacy of nafcillin, vancomycin, rifampicin, and amikacin alone or in combination in an experimental meningitis model with methicillin-sensitive Staphylococcus aureus (MSSA) and MRSA. In the MSSA group, treatment outcomes were similar. However, in the MRSA group, the VR combination, single use of rifampicin, and nafcillin-rifampicin combination were superior to other regimens. 41 Cabellos et al. compared the efficacy of linezolid, vancomycin, rifampicin monotherapies, and combinations in an experimental meningitis model with MRSA and glycopeptide-intermediate S. aureus strains. However, the difference in mortality and decrease in bacteria in the CSF was not statistically significant. 23 Case reports suggest VR combination may be efficient in MRSA meningitis, but its superiority over vancomycin alone is debated. 42 , 43 Our study did not have a vancomycin monotherapy arm, but the difference between the VR arm and Mermer et al.’s vancomycin arm was not significant.
To our knowledge, no experimental study has evaluated ceftaroline and rifampicin combination for meningitis. The only report of this combination for meningitis is Balouch et al. 6 A few animal studies and case reports have used ceftaroline and rifampicin together but not for meningitis. 44
The inflammatory response and neuronal damage from reactive oxygen products contribute to CNS damage in bacterial meningitis. Autopsy studies and animal models show neurological damage linked to apoptosis, especially in the dentate gyrus.16,45–47 Cell wall-targeting antibiotics may exacerbate this by releasing proinflammatory cellular components, whereas rifampicin, which does not damage the cell wall, may mitigate apoptosis. Spreer et al. conducted a rabbit model of pneumococcal meningitis. They found that pre-treatment with rifampicin before ceftriaxone reduced bacterial release, inflammation, and apoptosis compared with ceftriaxone-only treatment. 16 Böttcher et al. found that rifampicin treatment in a Streptococcus pneumoniae (S. pneumoniae) meningitis model resulted in lower reactive oxygen release and apoptotic cell density compared with ceftriaxone. 48 To our knowledge, there is no study on ceftaroline’s apoptotic effect in meningitis. Vancomycin versus daptomycin research in a mouse model infected with S. pneumoniae showed no apoptosis difference between treatment groups. 49 Our study observed fewer TUNEL (+) cells in the hippocampus and dentate gyrus in treatment groups compared with the control. No significant difference was found between treatment groups. The CR group showed less inflammation than the control. Despite not including monotherapy arms, the presented study provides the first analysis of antibiotic therapy impact on apoptosis in MRSA meningitis.
Comparative in vitro studies on MRSA-ATCC 43300 strain show that vancomycin and ceftaroline have varying time-kill kinetics. Bardak-Özcem et al. found no significant differences between vancomycin and daptomycin within eight hours, whereas Mermer et al. reported ceftaroline sterilized bacteria at all concentrations within eight hours, unlike vancomycin.9,20 In our study, both antibiotics eliminated all bacteria within 24 hours, with differences from previous reports likely because of initial bacterial amounts and experiment duration.9,20
Limited studies have assessed the antibacterial effects of VR and CR combinations on MRSA in vitro. Gatin et al. found that adding rifampicin reduced bacterial counts more effectively than monotherapy, but the time-kill curve was similar in both combination arms. Also, no antibiotic achieved sterilization within 24 hours. 21 Unlike Gatin et al., we did not observe a positive effect of adding rifampicin on bacterial killing kinetics in the time-kill assay, possibly because of different MRSA strains and initial bacterial concentration levels. 21
In vitro evaluations of vancomycin and rifampicin on MRSA strains have shown mixed results, with limited synergistic effects observed by Kang et al. and Silva et al.24,50 However, our in vitro analysis did not show any synergistic effect. To our knowledge, no other studies have examined the synergistic effects of the VR combination on the ATCC 43300-MRSA strain.
Our study has several limitations. (1) We did not compare combination therapies to monotherapy in vivo because it was already been done and (2) ceftaroline drug concentrations could not be measured using high-performance liquid chromatography (HPLC) in any center in our country, bioassay was not feasible because of the simultaneous use of two antibiotics. 9 However, extending the duration of our experiment to 24 hours might have been beneficial for analyzing survival, and we believe that the apoptosis data will contribute to the literature.
Conclusion
CR combination was as effective as VR combination in terms of antibacterial efficacy and survival. Although the VR and control groups had similar treatment responses, the CR group had a significant difference: Histopathological examination revealed significantly less inflammation in the CR group compared with the control group, but no significant difference was observed between the control group and VR group.
Footnotes
Data Availability
The datasets generated during and/or analyzed during the current study are not publicly available but are available from the corresponding author upon reasonable request.
Authors’ Contributions
D.A.: Conceptualization, methodology, investigation, resources, writing—original draft, project administration. T.T., E.B., and G.S.-I.: Investigation, writing—review and editing. C.T.: Investigation, formal analysis, writing—review and editing. F.I.: Investigation. Y.U.: Investigation, formal analysis, writing—review and editing. S.A.: Visualization, investigation. T.Y., H.P., B.A., M.T., B.G., E.K., D.B.E., and S.U.: Visualization, writing—review and editing. H.S.: Formal analysis. O.R.S.: Conceptualization, methodology, investigation, resources, writing—review and editing, project administration, supervision.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
Ege University Scientific Research Foundation Coordination Unit (project id: 20680) provided funding for this study. The funders had no influence on study design, data collection, interpretation, or publication.