
Abstract

To the Editor:
T
A 26-year-old male sought help for a swollen and painful left wrist joint with limited mobility. He did not go to the hospital for any examination and treatment before, but only treated with acupuncture and traditional Chinese herbal patches. He had no history of underlying diseases or tuberculosis exposure. Physical examination indicated swelling and tenderness on the ulnar side of the left wrist, as well as decreased finger abduction strength. Phalen's test, reverse Phalen's test, Durkan's test, and Tinel's sign were all positive. The range of motion in the left wrist was limited, and the left-hand grip strength was decreased.
Laboratory tests suggested that interferon-γ release assay (IGRA) was positive and tuberculin skin test was strong positive. The radiograph showed bone destruction in each carpal bone, part of the articular surfaces of metacarpal bones, and the second to fifth proximal metacarpal bones, suggesting the possibility of joint tuberculosis (Fig. 1). Magnetic resonance imaging (MRI) showed that large or nodular abnormal signal shadows existed in the bones of the proximal carpometacarpal joint of the left wrist, and the joint surfaces of the second to fifth metacarpal bones were blurred, whereas the joint space was slightly narrowed, so infectious lesions were considered, probably tuberculosis (Fig. 2). Computed tomography (CT) of the chest showed there were no obvious abnormalities in the lungs (Fig. 3).

Radiograph of the left hand. The radiograph showed bone destruction in each carpal bone, part of the articular surfaces of metacarpal bones, and the second to fifth proximal metacarpal bones, suggesting the possibility of joint tuberculosis.

Magnetic resonance imaging (MRI) of the left hand. The image showed that large or nodular abnormal signal shadows existed in the bones of the proximal carpometacarpal joint of the left wrist, and the joint surfaces of the second to fifth metacarpal bones were blurred, whereas the joint space was slightly narrowed, so infectious lesions were considered, probably tuberculosis.
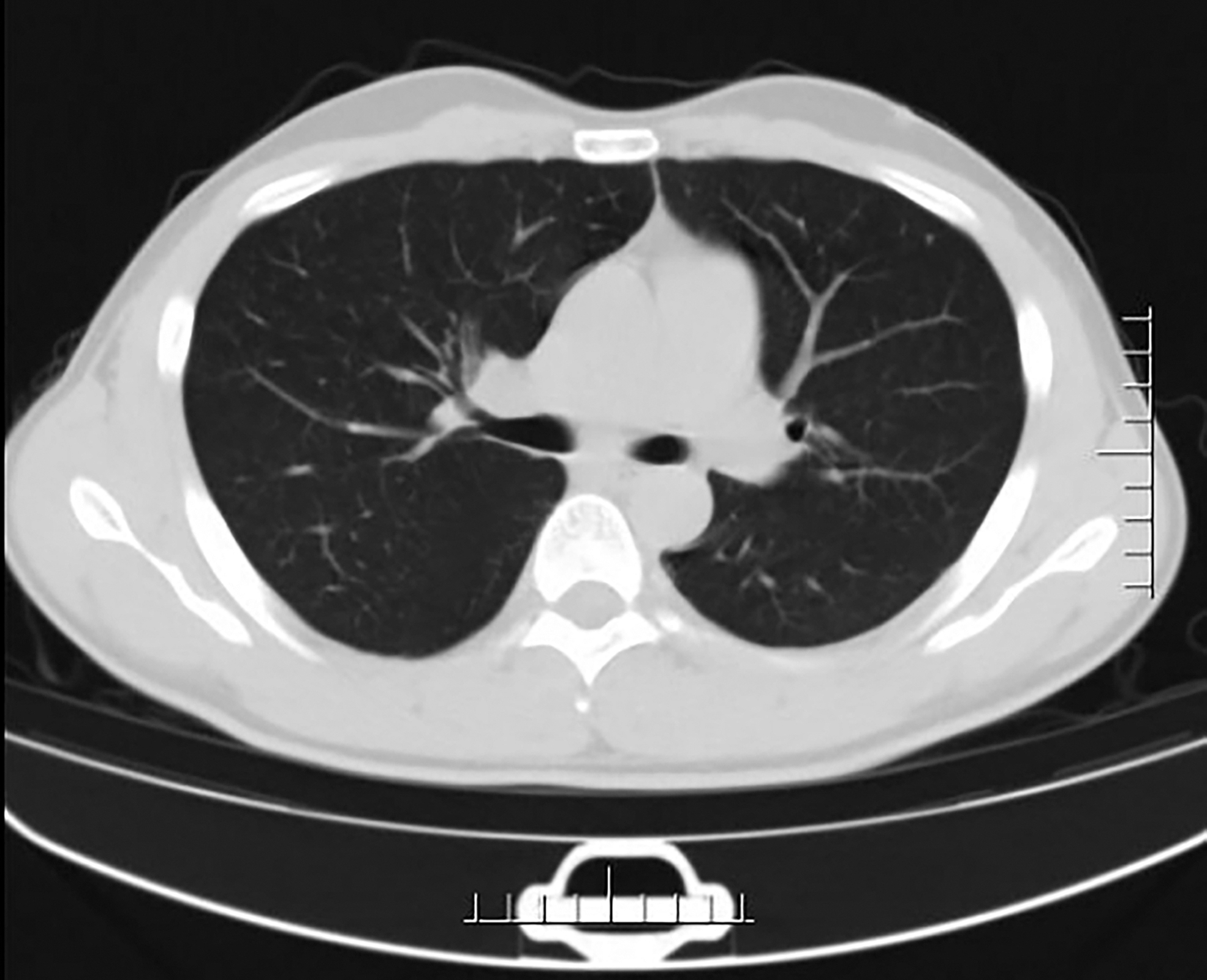
Computed tomography (CT) of the chest. From the image, no obvious abnormalities in the lungs were observed.
On the basis of the patient's data and test results, tuberculosis of the left wrist joint was highly suspected. After consultation, the diagnosis of tuberculosis of the left wrist joint was confirmed. The patient had no indication for emergency surgery and requested discharge to receive antituberculosis drug treatment. However, the therapeutic effect was not satisfactory, so the patient came to receive lesion resection surgery on the left wrist joint. The pathologic findings indicated that the synovium and necrotic tissue of the left wrist joint showed granulomatous inflammation with massive necrosis, considering tuberculosis (Fig. 4). In addition, polymerase chain reaction (PCR) assay for the detection of Mycobacterium tuberculosis was positive and acid-fast staining was negative. The pathologic findings further confirmed our diagnosis. The patient continued to receive antituberculosis drug treatment and recovered well after the surgery.
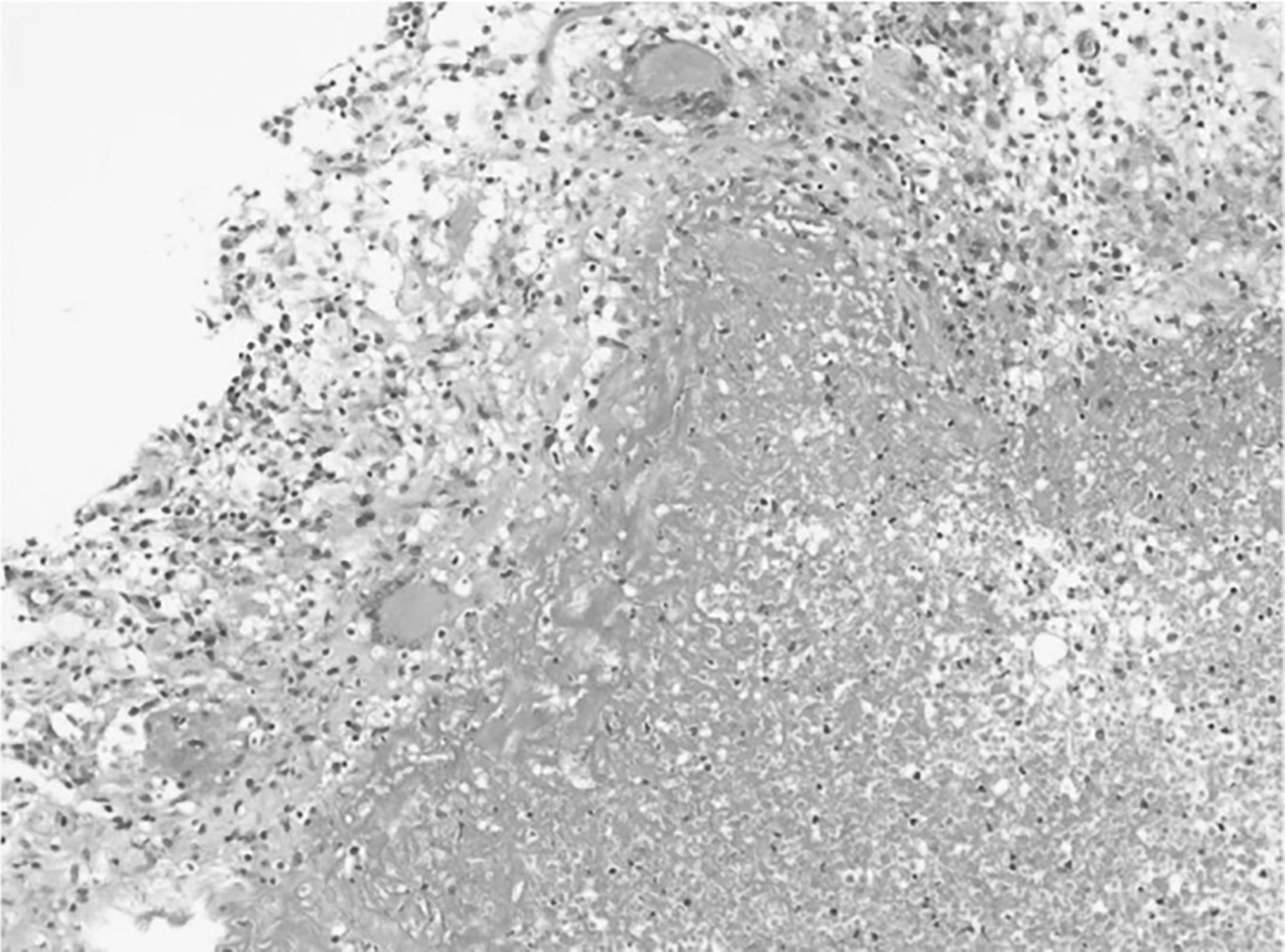
The pathologic picture. The pathologic findings indicated that the synovium and necrotic tissue of the left wrist joint showed granulomatous inflammation with massive necrosis, considering tuberculosis.
The correct diagnosis of tuberculosis of the wrist joint is still a difficult problem because of its rare incidence and lack of typical clinical manifestations. If it cannot be diagnosed and treated in time, it will result in hand deformity and severe hand dysfunction. It is not able to be distinguished from other wrist joint diseases solely by imaging appearances. Thus, pathologic examination is the key to diagnosis of tuberculosis of the wrist joint. Timely antituberculosis treatment after diagnosis can often achieve good therapeutic effects. However, surgery may be required to remove the lesions or rebuild joint function in some patients with poor response to medications or with more severe lesions.