
Abstract
Background:
Complicated intra-abdominal infections (cIAIs) require a combined tactic, of source control and antimicrobial therapy. This study aimed to evaluate the safety and efficacy of oral step-down antimicrobial therapy in cIAIs after initial intravenous (IV) antimicrobial therapy.
Methods:
This retrospective cohort study included hospitalized adult patients diagnosed with a cIAI who received more than seven days of IV therapy from March 2017 to October 2021. Exclusion criteria included primary/peritoneal dialysis-related peritonitis, necrotizing pancreatitis, fistulizing inflammatory bowel disease, or upper gastrointestinal tract infection. Patients were assigned into two groups: IV-only or oral step-down therapy. The primary outcome was infection recurrence, defined as re-initiation of antimicrobial agents after a treatment-free period of more than or equal to three days. Secondary outcomes included treatment escalation, repeat source control procedure, treatment-related complications, and all-cause mortality.
Results:
The cohort consisted of 248 patients (199 IV-only and 49 oral step-down). Patients receiving IV-only therapy had a shorter median antimicrobial duration than the oral step-down group (13 vs. 23 d; p <0.0001). Infection recurrence occurred in 26 (13.1%) and 6 (12.2%) patients in the IV-only and oral step-down groups, respectively (p = 0.88). Treatment escalation, repeat source control, and 28-day mortality were similar between groups. Oral step-down therapy resulted in more adverse drug events (10.2% vs. 3.0%; p = 0.04).
Discussion:
Transition to oral step-down after initial IV therapy had a similar rate of infection recurrence as IV-only therapy but was associated with a longer duration of antimicrobial therapy and an increased rate of adverse drug reactions. Larger randomized non-inferiority studies are needed to confirm this approach.
Background
Complicated intra-abdominal infections (cIAI) are often a gastrointestinal (GI) emergency, potentially leading to significant morbidity and mortality.1,2 Optimal management incorporates early source control and appropriate antimicrobial therapy. Together, these mitigate cIAI-associated complications while promoting rapid recovery of patients with critical illness.1,3–5
The Surgical Infection Society recommends timely source control and short antimicrobial courses (i.e., 4 d once adequate source control is achieved or up to seven days when source control is not achieved) and, if applicable, oral step-down therapy to complete the short duration of therapy for IAI. 3 Inadequate source control should prompt additional interventions to obtain source control. 3 However, a subset of patients may fail to undergo adequate source control, in particular because of surgical anatomy, risk, and/or underlying immunocompromised state, resulting in a longer duration of therapy often associated with worse treatment outcomes. 6 For these more complex patients, intravenous (IV) antimicrobial agents are often prescribed until repeat radiographical imaging and/or resolution of signs and symptoms of infection demonstrate clinical cure of the cIAI.
In other serious invasive infections, such as bacteremia, endocarditis, and osteomyelitis, early transition to oral therapy, following an initial course of 3–7 days of IV antibiotic agents, has been shown to be equally efficacious to continued IV therapy.7–9 In cIAI, the data supporting the efficacy and safety of early oral step-down therapy is limited. Several factors may lead clinicians to favor continued IV therapy, or outpatient parenteral antimicrobial therapy (OPAT), for the treatment of cIAI, one of which is the concern for the infection- and surgery-related impairment of the GI tract leading to malabsorption and tolerability of oral antibiotic agents. However, prolonged IV antibiotic therapy in the outpatient setting is associated with untoward complications, such as secondary infections, thromboses, and lower quality of life because of the constraints of IV therapy.7–9 If shown to be efficacious, oral step-down therapy is an attractive option that may enhance safety, convenience, and patient satisfaction in those requiring a longer antimicrobial duration for cIAI.
The objective of this study was to evaluate differences in infection recurrence between continued IV and oral step-down antimicrobial therapy for the treatment of cIAIs requiring prolonged antimicrobial course.
Methods
Study design and participants
This single-center retrospective cohort study included adult patients who were hospitalized at The University of Texas Southwestern Medical Center (UTSW) between March 1, 2017, and October 31, 2021, with a diagnosis of IAI and received IV antimicrobial agents for longer than 7 days during hospital stay. This IV antimicrobial duration was selected to identify more complicated cases of IAI (cIAI) and to exclude IAIs needing only shorter course (i.e., 4–7 d) because of achieved source control. The oral step-down group consisted of patients whose antimicrobials were transitioned to oral therapy on or after day eight. The group was further divided into early (transitioned to oral therapy after 8–14 d of IV therapy) and delayed oral step-down (transitioned after ≥14 d IV therapy) for a subgroup analysis. The IV-only cohort received their entire therapeutic course with IV antimicrobial agents.
Patients with the following were excluded from the study: (1) diagnosis of primary peritonitis, peritoneal dialysis catheter-associated peritonitis, necrotizing pancreatitis, and fistulizing inflammatory bowel disease (because these conditions require an alternative management tactic than other typical cIAIs); (2) diagnosis of upper or rectal GI infection (as the focus of this study was on the abdominal region only); (3) receipt of antimicrobial agents for infection prophylaxis; (4) repeat hospitalizations during the study period (in order to avoid patients who switched from IV to oral antibiotics then back to IV therapy upon re-admission); (5) concomitant non-IAI requiring antimicrobial therapy; and (6) receipt of care for >24 h at another acute facility before transferring to the study hospital.
An initial list of patients used for screening was extracted from the institution’s electronic medical record database based on intra-abdominal infection 10th revision of the International Classification of Diseases (ICD-10) codes. Data collected included patient demographics, comorbidities, medications, hospital length of stay, infection-related data (i.e., intra-abdominal infection type, organ of origin, microbiologic culture results, infectious diseases [ID] consultation), and therapy-related data (i.e., type and timing of source control procedure, antimicrobial agents utilized, and duration of therapy). Study data were collected and managed using REDCap (Research Electronic Data Capture) tools hosted at UTSW.10,11
Outcomes
The primary outcome was infection recurrence, defined as the re-initiation of antimicrobial treatment with the same or broader-spectrum regimen after a treatment-free period of ≥3 days up to 14 days after completion of treatment. Secondary outcomes included treatment escalation, repeat source control intervention(s), treatment-related complications, and all-cause mortality (28 and 90 d). Treatment escalation was defined as the addition of, or switch to, a new antimicrobial with a broader spectrum of activity than the previously used antimicrobial for reasons other than drug intolerance/allergic reaction, cost/acquisition issues, or newly available microbiologic data necessitating an antimicrobial switch. Repeat source control interventions were defined as any unplanned, repeat source control procedure during ongoing antimicrobial treatment. Treatment-related complications included antimicrobial-related adverse effects (i.e., dermatologic reactions, GI upset, diarrhea, nausea/vomiting, and any patient-specific reported reaction); Clostridioides difficile infection; and OPAT-related complications (i.e., line-related thromboembolism and infection). Line-related complications were collected via a review of outpatient follow-up encounter notes; mortality was collected via chart review only.
Statistical analysis
Continuous data were reported using medians with interquartile ranges, and categorical data were reported using percentages. Mann-Whitney U test and χ2 or Fisher exact test were used to compare continuous and categorical data, respectively. Results with p <0.05 were considered statistically significant. Statistical analysis was conducted using GraphPad Prism v.9.2.0 for Windows (GraphPad Software Inc., San Diego, CA, USA).
The study was approved by the Institutional Review Board at UTSW. Partial results of this study were presented at the 2022 ID Week Conference (Washington, DC).
Results
A total of 534 patients underwent screening. Reasons for exclusion included concomitant non-IAI requiring antimicrobial therapy (n = 174), IAI of upper GI source (n = 25), antimicrobial indication for post-surgical prophylaxis (n = 44), IV antimicrobial duration less than or equal to seven days (n = 38), and GI bleed (n = 5). The final analysis included 248 patients (199 IV-only and 49 oral step-down) (Fig. 1).
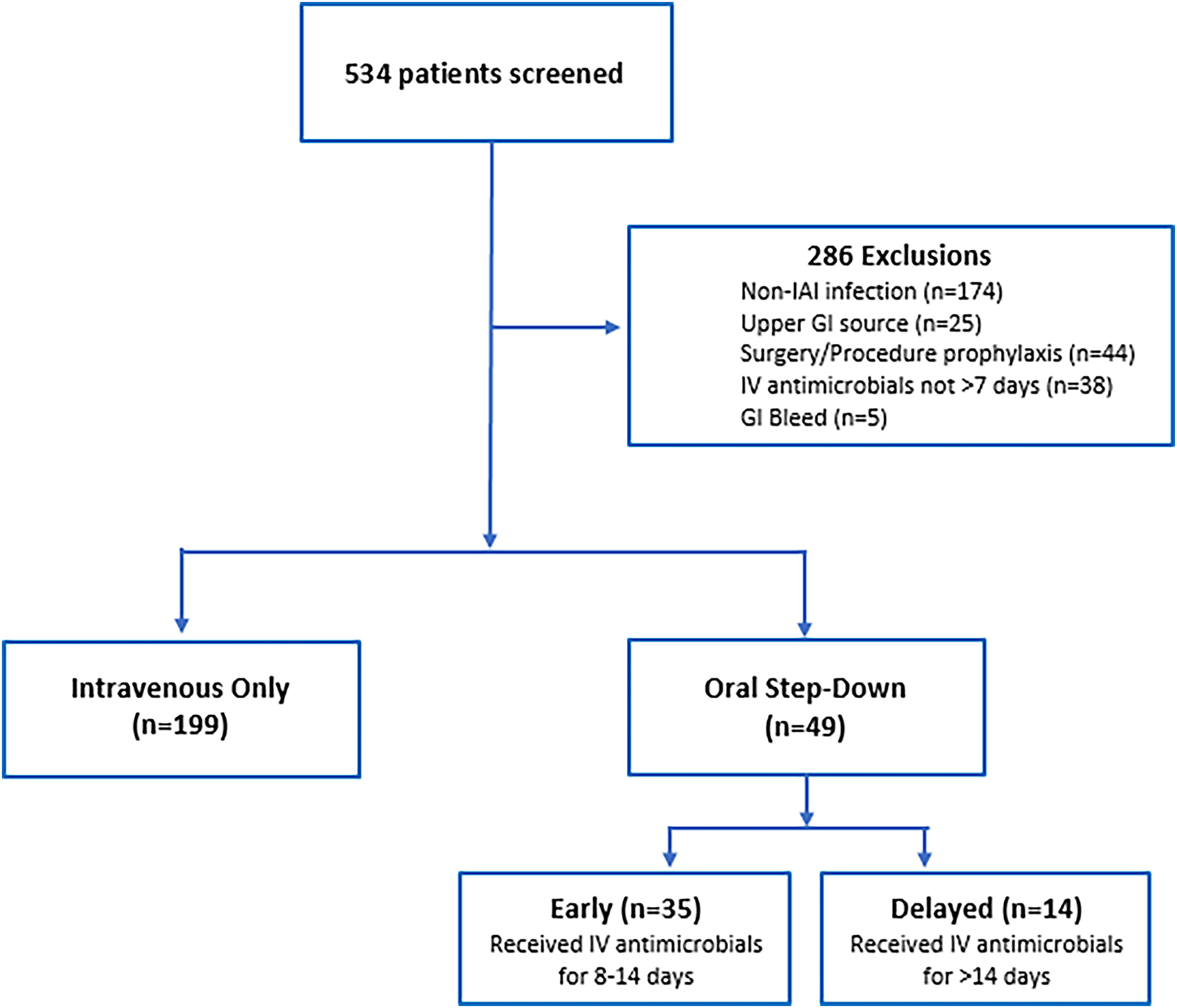
Breakdown of patients screened, excluded, and included in the final analysis.
Table 1 summarizes key baseline characteristics for the IV-only and oral step-down groups. The IV-only group had a higher percentage of male patients compared with the oral step-down group (52% vs. 33%, p = 0.017); otherwise, baseline characteristics were well-balanced between treatment groups. The cohort overall had a significant number of patients with GI malignant disease (19%) and/or those who were classified as immunocompromised (28%), predominantly because of concomitant immunosuppressive therapy.
Baseline Characteristics for IV-Only and Oral Step-Down Therapy
IQR = interquartile range; GI = gastrointestinal; IV = intravenous.
Table 2 provides a comparison of infection-related characteristics between IV-only and oral step-down therapy. The small and large intestines were the most common infectious organs of origin (56%). Oral intolerance was observed in only 18% of the IV-only cohort.
Comparison of Infection- and Treatment-Related Data Between Treatment Groups
Regarding infection management, both groups were treated similarly relative to receipt of any source control procedure, time to first procedure, and overall number of procedures performed (Table 2). The length of stay was six days longer in the IV-only group (19 d vs. 13 d, p <0.0001) than in the oral step-down group, and the duration of antimicrobial therapy was 10 days longer in the oral step-down group (23 d vs. 13 d, p <0.0001) (Table 2). Although not statistically significant, a higher number of patients in the oral step-down group were evaluated by the inpatient ID consultation services (49% vs. 38%, p = 0.168) (Table 2). The two most common oral regimens utilized were amoxicillin/clavulanate (n = 19) and a combination of ciprofloxacin (n = 18) and metronidazole (n = 21).
Overall, <50% of patients had a documented positive intra-abdominal culture (Table 3). The majority of positive cultures isolated gram-negative organisms, with Escherichia coli being the most common in the IV-only group and Bacteroides spp. being the most common in the oral step-down group. Enterococcus spp. was the predominant gram-positive organism observed in both groups. A full comparison of microbiologic data is shown in Table 3.
Microbiologic Data for IV Only and Oral Step-Down Therapy
Other bacteria: Aeromonas spp., Clostridium tertium, Diphtheroids, Enterobacter cloacae complex, Eubacterium spp., Mycobacterium avium complex, Proteus mirabilis, Raoultella ornithinolytica.
Other fungus: Candida glabrata, Candida krusei, Candida lusitaniae, Aspergillus spp.
The primary outcome, infection recurrence, occurred in 26 (13%) and 6 (12%) patients in the IV-only and oral step-down groups, respectively (p = 0.88) (Table 4). Repeat cultures were not obtained in 69% of patients during recurrent episodes (Table 4). Treatment escalation (41% vs. 43%; p = 0.834) and repeat source control procedures (37% vs. 31%, p = 0.39) were similar between both treatment groups (Table 4). Both 28- and 90-day all-cause mortality were not statistically different, although 28-day mortality was found to be numerically higher in the IV-only group (10% vs. 2%, p = 0.138) (Table 4). Adverse drug reactions, which mostly consisted of dermatologic and GI reactions, were the only secondary outcome found to be statistically higher in the oral step-down group (10% vs. 3%, p = 0.044). Other treatment-related complications were all similar among treatment groups (Table 4).
Primary and Secondary Outcomes Between IV Only and Oral Step-Down Therapies
In a subgroup analysis, no differences in primary and secondary outcomes were observed between early (transitioned after 8–14 d of IV antibiotic) and delayed oral step-down (transitioned after ≥14 d of IV antibiotic) (Supplementary Table S1).
Discussion
Our study evaluated the safety and efficacy of oral step-down therapy for the treatment of cIAI requiring longer treatment durations (i.e., >7 d). Oral step-down therapy had a comparable rate of infection recurrence to the IV-only approach, supporting oral step-down therapy as an alternative tactic to IV-only therapy in the treatment of cIAI.
Previous studies assessing the risk for mortality from cIAIs have identified that inadequate source control is a major risk factor.5,12 Inadequate source control may also contribute to a clinical decision to extend the duration of antimicrobial therapy. Although the majority of patients underwent some type of source control procedure, the retrospective nature of the study and limitations on data and imaging available in the medical record did not allow us to rigorously assess the adequacy of source control procedures in this cohort. Therefore, clinical concerns about inadequate source control could have contributed to the longer antimicrobial durations used in this study’s patient population overall, and unmeasured imbalances between groups may have biased toward one treatment approach and influenced the primary and secondary clinical outcomes.
Intrinsic risk factors associated with cIAI-associated mortality include increased age, liver disease, kidney disease, and immunocompromise.12,13 A significant proportion of both treatment groups had these risk factors, and notably ∼30% of the cohort was immunocompromised. Hassinger et al. identified that longer antimicrobial durations did not prevent treatment failure in cIAI in high-risk patients 14 ; however, there are limited data defining the optimal treatment duration and the appropriateness of utilizing the oral step-down approach in immunocompromised populations. This study provides additional support for the use of oral step-down therapy in select high-risk patients who require longer treatment durations, although a more definitive prospective, controlled study in high-risk populations is necessary.
As noted, baseline high-risk factors for treatment failure, including GI malignant disease and underlying immunocompromise, were similar between both groups. Additional risk factors such as higher baseline severity of infection in the IV-only group are suggested by significantly longer hospital length of stay and a trend toward higher number of repeat source control procedures and 28-day mortality. Despite these potential confounders or differences in disease severity, no statistical differences in infection recurrence or mortality were observed.
Conversely, the study found a shorter length of stay for those transitioned to oral antimicrobial agents. This finding may be explained by lower baseline disease severity and earlier clinical stability for discharge with transition to oral therapy. However, there was an unexpected finding of longer overall treatment duration observed in this oral step-down group. The oral step-down group had fewer source control procedures documented in the index hospitalization while at the same time having potentially lower baseline disease severity. Therefore, we hypothesize that concerns for inadequate source control in the setting of relative clinical stability may have led to clinical decisions to discharge on continued oral suppressive antimicrobial therapy with plans for future source control procedures if unresponsive to medical therapy, although this was not confirmed.
The frequency of treatment-related complications associated with OPAT in this study was very low (<1%) relative to prior studies.7,8 Notably, patients on oral step-down therapy experienced a higher rate of adverse events, primarily dermatologic and GI reactions, which may reflect the longer overall antimicrobial durations increasing the probability and capture of an event. The rate of adverse events in the IV-group was lower than previously reported rates of ∼20%, which is possibly related to the shorter duration of therapy (median 13 d) or incomplete capture of events from some patients not being followed by a formal OPAT service (∼16% followed by OPAT).15,16 Despite the longer antimicrobial duration, the oral step-down therapy group did not have a higher number of C. difficile infections. This may be the result of the utilization of antimicrobial agents with variable associated C. difficile risk and differences in underlying risks between cohorts not captured (e.g., proton pump inhibitor use, prior colonization). 17
This study had several limitations including the retrospective, single-center design limiting the capture of confounders and generalizability; disproportionate number of high-risk and immunocompromised patients relative to other practice setting may limit generalizability to lower risk populations; limited sample of oral step-down therapy with higher distribution of IV-only to oral step-down; inability to rigorously assess adequacy of source control; low number of microbiologically confirmed cIAI relative to cultures obtained; no formal assessment of appropriateness of antimicrobial agents; inability to prospectively ascertain all of the clinical reasons for IV-only therapy (only ∼18% had oral intolerance); and no formal classification of community-acquired versus health-care–associated infection.
Conclusion
In patients requiring prolonged durations of therapy for cIAI, the transition to oral step-down after initial IV antimicrobial therapy had a similar rate of infection recurrence as IV-only therapy, although the oral step-down therapy was associated with a longer total duration of antimicrobial exposure and an increased incidence of adverse drug reactions. Larger randomized non-inferiority studies are warranted to confirm this approach.
Footnotes
Acknowledgments
The authors would like to thank Donglu Xie for her assistance in data acquisition.
Authors’ Contributions
Conceptualization/data curation/methodology: All authors contributed equally. Project administration/supervision/validation: E.G. and J.M.S. Writing—original draft: S.A. Writing—reviewing and editing: All authors contributed equally.
Patient Consent Statement
The study does not include factors necessitating patient consent.
Author Disclosure Statement
The authors have no related conflicts of interest to declare.
Funding Information
This study did not receive any grant from funding agencies in the public, commercial, or not-for-profit sections.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.