
Abstract
Background:
Diarrheal illness is a prominent public health worry in developing countries, resulting in high mortality among children. Sociodemographic characteristics and geographic settings are the main effective factors for the increased incidence of childhood diarrhea. Aeromonas is a neglected organism capable of causing dysentery and diarrhea. The aim of this systematic review and meta-analysis was to determine the prevalence of Aeromonas as an agent in the causation of diarrhea in Asian children.
Methods:
We conducted a systematic review using Web of Science, PubMed, Wiley Online Library, Science Direct, and Google Scholar for peer-reviewed articles published between January 2000 and February 2023. We considered studies that found Aeromonas in diarrheal stool. A random-effects model was used to determine the pooled prevalence of Aeromonas.
Results:
Our search returned 2,057 articles, with 17 articles from seven Asian nations being included in the systematic review. The pooled prevalence of Aeromonas was 4.5% (95% confidence interval [CI]: 2.9%–6.8%), with heterogeneity (I2 = 96.85; p < 0.001). There was a greater prevalence in areas with high population living in poverty (12.2%; 95% CI: 5.8%–24%) and lower-middle-income countries (5.0%; 95% CI: 2.7%–9.0%). In addition, the prevalence of Aeromonas was greater in South Asia (10.0%; 95% CI: 5.6%–17.2%), in India (12.9%; 95% CI: 6.8%–23%), and in countries with open defecation rate of 5%–25% (11.3%; 95% CI: 6.3%–19.2%).
Conclusion:
The prevalence of Aeromonas-associated diarrhea in children in Asia estimated in the present study highlighted the high burden of Aeromonas in some parts of Asia.
Diarrheal diseases continue to be a severe global problem in young children, accounting for around 27% of diarrheal deaths. 1 It should be emphasized that 2,195 children die per day from diarrhea, which is more than malaria, AIDS, and measles combined. 2 The genus Aeromonas is a gram-negative facultative anaerobic coccobacillus, which mostly behaves as opportunistic microorganisms. 3 This genus is recognized as the cause of a wide range of illnesses in human beings,4,5 including extraintestinal diseases, especially in immunocompromised individuals, including necrotizing fasciitis, hepatobiliary tract infections, septicemia, urinary tract infections, and surgical site infections. 6 Diarrheal disease is the more prevalent manifestation of Aeromonas infection. 7 Gastroenteritis can present as moderate diarrhea, Shigella-like dysentery, or severe cholera-like watery diarrhea. 8 Different case–control studies have indicated that Aeromonas is responsible as a pathogen in 1%–88% of children with diarrhea and in 0%–45% of the control group. 9 Aeromonas is a co-pathogen found in the majority of gastroenteritis patients, having been isolated alongside other enteropathogens. 10 Acute gastroenteritis causes more deaths in children in impoverished nations than in industrialized countries. 11
Several bacterial infections have been mostly linked to diarrhea bouts (20%–40%), including Escherichia coli, Campylobacter jejuni, Salmonella spp., Yersinia enterocolitica, Vibrio cholerae, Plesiomonas spp., and Aeromonas spp. 12 Aeromonas is among the main five enteropathogens causing diarrhea in children in Asia. 13 It should be mentioned that Aeromonas species are the most prevalent cause of diarrhea in children 14 and that the death rates for bacteremia that spreads from the gastrointestinal tract are between 30% and 70%. 15 Diarrheal diseases pose a serious challenge to public health on a global scale, 16 especially as the second top-killer illness in low-income countries among children. 17 Aeromonas enteric infections are the predominant species isolated from clinical specimens in industrialized regions,18,19 even with a similar prevalence in Africa, Latin America, and Asia, 20 in a high association with clinical patterns such as malignant disease, hospitalization, admission to the intensive care unit, and extraintestinal infection. 21
Socioeconomic conditions affect the prevalence of infectious diseases by indirect connection with the life quality, accessibility to healthcare, water and sanitation quality score, the chance to benefit from various hygienic methods, and behavior and awareness connecting to the prevention of disease. 22 Disparate studies have been performed in several parts of Asia at different times to evaluate the prevalence of Aeromonas in children with diarrhea. In a study that was conducted on a global scale, it was shown that Aeromonas is more prevalent in countries with a high population and poor health conditions. 23 For children in Asia, this is the first meta-analysis that identifies the pooled prevalence of diarrhea linked to Aeromonas. It appears that assessing the combined prevalence of this underappreciated virus throughout Asia is required.
Patients and Methods
Search tactic
This study follows the Preferred Reporting Items for Systematic Review and Meta-analysis criteria (http://www.prisma-statement.org/). We searched the Web of Science, PubMed, Wiley Online Library, Science Direct, and Google Scholar for peer-reviewed articles with restrictions on publication language. Only articles released between January 2000 and February 2023 were included in the search parameters. Special keywords, including Aeromonas, children, diarrhea, and Asia, were selected alone or in combination with “OR” and/or “AND” operators. To find further articles, we manually looked through the screened articles’ reference lists. Articles with epidemiologic results were selected. Endnote version X9 (Clarivate Analytics, Philadelphia, PA, USA) was used to import all of the articles. Children and English were the study groups and language’s respective boundaries.
Inclusion and exclusion criteria
We used predetermined inclusion and exclusion criteria to evaluate the titles and abstracts found in the first search. The following criteria were applied to the eligibility of articles for inclusion: (a) The research had to be done on Asian children who were afflicted with Aeromonas; (b) the studies must have evaluated the presence of Aeromonas in diarrheal stool; (c) the study must have been designed cross-sectional; (d) the studies must have declared the number of participants testing positive for Aeromonas; and (e) the studies must have been peer-reviewed and published.
Articles that did not fit the requirements for inclusion were not accepted (e.g., studies not carried out in Asia, articles available only as abstracts, studies performed on animals, cohort, case–control, commentaries, case reports, editorials, confusing studies, posters, and short communication and review articles).
Data extraction
For inclusion in the full-text review, the titles and abstracts of the retrieved articles were separately evaluated by two researchers (H.S. and S.G.K.). All articles that might be linked were thoroughly reviewed. The following specifications of each related study were elicited: First author, country, year of publication, type of samples, sample size, positive samples, type of study, prevalence of Aeromonas, and method. Disagreements were settled by reading the articles again and having a conversation with M.A., the third member of the research team.
Quality assessment
The quality was assessed using the 10-point Newcastle–Ottawa Scale. 24 Each study received a maximum score of 10 points based on three factors: subject selection (0–5 points), subject comparability (0–2 points), and outcome (0–3 points). The total score for the following studies was given out: 0–4, 5–6, 7–8, and 9–10 points for unsatisfactory, satisfactory, good, and very good investigations. 25
Data synthesis and statistical analyses
Data analyses were performed in Comprehensive Meta-Analysis software. The original publications were described using forest plots, funnel plots, tables, and illustrations. Random-effects models were used to estimate the pooled prevalence assessments to take into consideration the heterogeneity that frequently arises in meta-analyses. The evaluated pooled prevalence rate with a 95% confidence interval (CI) was presented. We employed the I2 statistics to evaluate heterogeneity. I2 values <25%, 50%, and 75%, respectively, are regarded as low, moderate, and high heterogeneity. 26 p-Values were considered statistically significant if they were <0.05.
Results
Selection and characterization of included studies
Twenty-six full-text studies were chosen for eligibility evaluation out of 2,057 articles that were obtained from internet databases. Nine full-text publications were disregarded for various reasons, such as case–control study data, review articles, irrelevant content, and critical evaluation. Critical evaluation led to the inclusion of 17 publications in the meta-analysis14,27–42 (Fig. 1). From the eligible articles for this investigation, 35,273 diarrhea stools were tested for Aeromonas. A total of 1,525 of them tested positive for Aeromonas. The studies that met the eligibility requirements had sample sizes ranging from 83 to 26,444. Seventeen included articles in our review were done in one of seven Asian countries (Table 1). Among them, 5, 4, 3, 2, 1, 1, and 1 came from India, Iran, Iraq, Bangladesh, Indonesia, Malaysia, and Taiwan, respectively.

Flow diagram of studies reviewed, screened, and included.
Characteristics of the Included Studies and Quality Assessment Score
Quality assessment
Upon evaluating the quality of the studies, it was found that out of the 17 articles, 8 had an overall score of 0–4 (unsatisfactory studies), 7 had an overall score of 5–6 (satisfactory studies), and 2 had an overall score of 7–8 (good studies). Table 1 shows that none of the included studies were deemed very good.
Aeromonas prevalence in children with diarrhea and subgroup analysis
The frequency of Aeromonas among children in Asia was 4.5% (95% CI: 2.9%–6.8%), with significant heterogeneity (I2 = 96.85; p < 0.001) (Fig. 2). A subgroup analysis was carried out according to sociodemographic characteristics (population living in poverty and income level) and geographic region of Asia (East, West, South, and Southeast Asia), country, and open defecation rate (proportion of people practicing open defecation).

Forest plots for the prevalence of Aeromonas in Asia.
Subgroup analysis revealed differences in Aeromonas prevalence in areas with high population living in poverty (167.49 million) (12.2%; 95% CI: 5.8%–24%) (Fig. 3) and lower-middle-income countries (5.0%; 95% CI: 2.7%–9.0%) (Fig. 4). The calculated cumulative prevalence of Aeromonas was highest in South Asia (10%; 95% CI: 5.6%–17.2%), 4.5% (95% CI: 1.5%–12.6%) in Southeast Asia, 2.3% (95% CI: 0.5%–9.9%) in East Asia, and 2.2% (95% CI: 1.1%–4.0%) in West Asia (Supplementary Fig. S1). Analyses according to countries revealed that the highest and lowest prevalence was in India with 12.9% (95% CI: 6.8%–23.0%) and Iran with 1.4% (95% CI: 0.6%–3.2%), respectively (Supplementary Fig. S2). Furthermore, the illness was more common in nations where the rate of open defecation ranged from 5% to 25% (11.3%; 95% CI: 6.3%–19.2%) (Supplementary Fig. S3).

Subgroup analysis of the prevalence of Aeromonas based on population living in poverty.
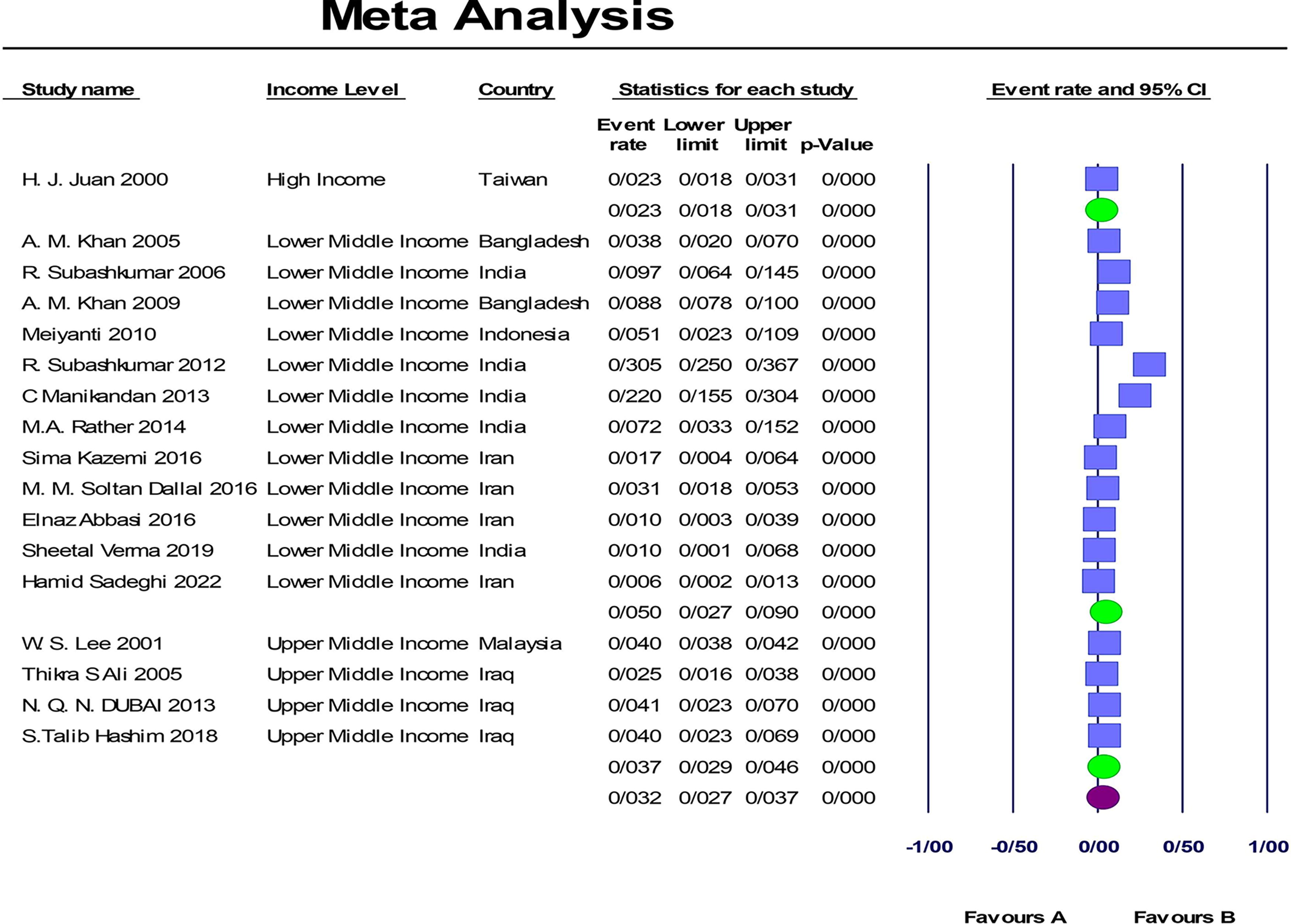
Subgroup analysis of the prevalence of Aeromonas based on income level.
Time series analysis
The trend in Aeromonas infection among Asian children with diarrhea has slightly increased from 2000 to 2010. A notable increase in the right direction was observed in prevalence between 2012 and 2014. Furthermore, from 2016 to 2022, there was a marginal decline in prevalence when compared with previous years (Supplementary Fig. S4).
Publication bias
The funnel plot (Supplementary Fig. S5) asymmetry shows no evidence of publication bias using Egger’s test for a regression intercept (p = 0.70) and Begg and Mazumdar rank correlation (p = 0.56) (Supplementary Fig. S6). There was no variability between studies in terms of publication year in the meta-regression analysis (p = 0.34) (Supplementary Fig. S7).
Discussion
According to present information about the epidemiology, ecology, and pathogenicity of Aeromonas, researchers should suppose that the Aeromonas infections tend to continue as an important health problem in the future. 43 Wastewater taken from aquaculture farms, veterinary clinics, hospitals, and industries makes aquatic environments major diffusers of multi-resistant pathogens. 44 Therefore, Aeromonas, as normal inhabitants of aquatic ecosystems, have a broad profile of antibiotic resistance and are always isolated from fish and animals. 45
This systematic review and meta-analysis shows the status of Aeromonas infection in Asia. The pooled prevalence of Aeromonas among children with diarrhea was evaluated to be 4.5% (95% CI: 2.9%–6.8%). These findings confirm that Aeromonas infection is a great public health problem in Asia, and inhabitants of the countries should be conscious of this prevalence. Heterogeneity across articles was high (I2 = 96.85%). We identified several parameters that could shed light on the sources of variability and have consequences for public health. Differences across the sociodemographic factors, geographical regions, and the open defecation rate contributed somehow to the heterogeneity. Qamar et al. showed that odds ratio (OR) of Aeromonas was greater in the presence of Shigella, which indicates the importance of sociodemographic factors in Aeromonas-associated diarrhea even in the presence of other pathogens. They reported that age, degree of stunting, and the presence of dysentery and co-infection with other pathogens, specially Shigella, are remarkable features of Aeromonas-associated diarrhea. 46 Ferdous et al. showed that cholera and Shigellosis are diarrhea illnesses associated with poverty. 47 Likewise, a second study showed that wealth has a positive effect on improving health status. 48
On the basis of prior study, the prevalence of childhood diarrhea burden is greater in low-middle-income countries in comparison with high-income countries. 1 Comparatively, our meta-analysis showed a portion of the population living in poverty and the income level of the countries is a substantial factor for Aeromonas-associated diarrhea, although these findings were reported for only 17 studies carried out in Asia. South Asia has the highest incidence according to the subgroup evaluation, with a pooled prevalence of 10.0% (95% CI: 5.6%–17.2%). This study displays evidence that Aeromonas is one of the main causes of diarrhea in children in South Asia. The current systematic and meta-analysis provided a greater view of the prevalence of Aeromonas in South Asian countries. According to these results, we suggested that comprehensive epidemiological studies on Aeromonas should also be carried out in other Asian countries. The prevalence of Aeromonas among Asian countries was different from 0.6% in Iran 14 to 30.5% in India. 32 These differences could be on account of various geographical factors in diverse parts of the world.49,50 The estimated pooled prevalence in this study approximately agrees with other epidemiologic studies of Aeromonas in children, including Saba Talib Hashim in Iraq (4.0%), Lee in Malaysia (4.0%), and Dubai in Iraq (4.1%).28,33,39 The highest prevalence estimation was documented in studies conducted in India 12.9% (95% CI: 6.8%–23.0%) followed by Bangladesh 6.0% (95% CI: 2.3%–15.2%). In addition, variations of prevalence between different studies in the same country were also observed, especially in India from 1.0% to 30.5%. Variances in local risk factors, such as public health and hygiene standards, are most likely the cause of these variances in diarrheal illnesses. 51 The prevalence of Aeromonas in children with diarrhea was greater in countries with an open defecation rate of 5%–25% (11.3%; 95% CI: 6.3%–19.2%).
These findings underscore the necessity for interventional initiatives to focus on children to ensure optimal preventative tactics with appropriate case management and timely treatment.
Conclusion
This study approves that Aeromonas-associated diarrhea infection remains high in children in South Asian countries and in people living in areas with high open defecation rates. Children with Aeromonas should receive the appropriate treatment from healthcare professionals to avoid complications and lessen the possibility that they will infect other children in the community.
Strengths and Limitations
This study has some strengths: The comprehensive literature search and the obvious exclusion and inclusion criteria. More importantly, it benefits from the absence of bias in publications. Nevertheless, there are some limitations: The majority of the studies included in this meta-analysis failed to provide clear and consistent information about the antibiotic resistance pattern. In addition, the age and gender of patients were not reported clearly in most of the included articles.
Footnotes
Acknowledgments
The authors would like to express their profound gratitude to the personnel of the Medical Microbiology Research Center at Qazvin University of Medical Sciences in Qazvin, Iran. All authors confirm that their research is supported by the Qazvin University of Medical Sciences, which is primarily involved in education or research.
Authors’ Contributions
S.G.K. and H.S.: Design study, conceptualization, literature search, data collection, interpretation, writing––original draft, and methodology and reviewing. H.S.: Analysis. R.S. and H.S.: Writing––reviewing and editing. M.A., F.N., and M.V.: Methodology and validation. S.G.K.: Supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.