
Abstract
Background:
The objective of this study was to investigate the clinicopathologic and etiologic characteristics of urinary tract infections in patients with cervical cancer who had undergone radical operation with ureteral stent insertion.
Patients and Methods:
We conducted a retrospective analysis on the medical records of 24 patients who underwent radical operation for cervical cancer with indwelling ureteral stents at Shanghai General Hospital between April 2019 and December 2022.
Results:
A total of 15 patients experienced urinary tract infections, resulting in an infection rate of 62.5%. Although postoperative adjuvant chemotherapy might have been a potential risk factor for urinary tract infections, the difference was not statistically significant (p = 0.074). A total of 30 pathogen strains were isolated, with Escherichia coli being the most prevalent. Notably, two strains of carbapenem-resistant Enterobacteriaceae were identified. The majority of patients (70.83%) had ureteral stents in place for 3–12 months. As the duration of stent insertion exceeded 2 months, we noted a decrease in antibiotic sensitivity against the same pathogen. Furthermore, fungal infections became more prevalent when the stent placement duration surpassed 4 months.
Conclusions:
The incidence of urinary tract infection is exceptionally high in patients with locally advanced cervical cancer and who have undergone radical operation with ureteral stent insertion. E. coli strains exhibited relative resistance to penicillins and cephalosporins. With prolonged stent placement, there was a notable diminution in antibiotic sensitivity against the same pathogen, and the microbial profile shifted from bacteria to fungi. This study provides valuable insights for the determination of the optimal timing for stent removal or replacement and for the selection of effective antibiotics to treat urinary tract infections for patients with indwelling ureteral stents, so as to ultimately prevent severe infections and mitigate disease burden.
Background
Despite the widespread promotion of early cervical cancer screening and human papilloma virus (HPV) vaccination programs, cervical cancer continues to be one of the most prevalent malignant diseases in women. 1 It is estimated that there were 604,127 new cases and 341,831 deaths attributed to cervical cancer in 2020 worldwide 2 and 13,960 new cases and 4,310 deaths from cervical cancer in the United States alone in 2023. 3 Although radical hysterectomy is standard management for early-stage cervical cancer, such as IB1, IB2, and selected IIA, 1 the close anatomical proximity of the genital and urinary tracts poses a risk of urinary tract injury during gynecological operations. One study from China showed that radical hysterectomy with pelvic lymph node dissection for cervical cancer stages IA2, IB1, IB2, IIA1, and IIA2 exhibited a complication rate of 34.41%, with adjacent tissue injuries occurring in 7.68% of patients—most frequently involving the ureters, followed by the bladder. 4 Another study from The Netherlands depicted the occurrence of ureter and bladder injury in early cervical cancer (IB1 and IIA1) in women who underwent radical hysterectomy with pelvic lymphadenectomy at 4%. 5 Ureteral injuries cause pain and affect a patient’s quality of life; therefore, prompt and adequate intervention is paramount in managing ureteral injuries. For example, early detection and treatment of urinary tract injuries can mitigate deterioration of renal function and result in a favorable prognosis. 6
Although prophylactic ureteral stenting prior to major gynecologic operation can prevent ureteral injuries and reduce the risk of urologic complications, the benefits of this procedure are controversial.6–10 With indwelling ureteral stents, authors have reported bacterial adhesion onto the indwelling implant surfaces and encrustation and stone formation as risk factors associated with adverse effects.11,12 Stent-related complications comprise abdominal discomfort, urinary tract infections, stent displacement, and stent encrustation, with urinary tract infections being the most prevalent.11,13 Most studies revealed an incidence of urinary tract infections, but few investigators have uncovered the pathogenic bacteria involved and their antibiotic sensitivities. There is also no consensus on the indications for prophylactic ureteral stent placement or the optimal timing for their removal in patients with cervical cancer. Generally, the ureteral stents should be removed or replaced every 3–12 months on the basis of their surface modifications and material composition, and this often causes urinary tract infections and exerts a negative impact on postoperative adjuvant therapy. In this study, we retrospectively analyzed the clinicopathologic and etiologic characteristics of patients with cervical cancer having indwelling ureteral stents and complicated by urinary tract infections.
Patients and Methods
Study setting and design
We enrolled patients who underwent radical hysterectomy accompanied by pelvic lymphadenectomy for cervical cancer and who underwent double-J ureteral stent placement, between April 2019 and November 2022. None of the patients had any recent history of inflammatory or infectious diseases, nor any recent antibiotic use. Prior to the diagnosis of cervical cancer, the patients were in good health and were free from any infectious diseases. We comprehensively analyzed various factors, including patient age, height, weight, diagnosis, clinical stage, pathologic stage, maximal diameter of the cervical cancer, pathologic type, squamous cell carcinoma antigen (SCC-Ag) concentrations before operation, HPV type, lymph node metastasis, neoadjuvant chemotherapy, surgical duration, radiotherapy, postoperative chemotherapy, indwelling time for the ureteral stents, renal function at the time of stent removal, occurrence of urinary tract infections during the period after stent placement, and pathogens isolated from urinary tract infections and drug sensitivity of these pathogens to common antibiotics. All patients received prophylactic antibiotic therapy for more than 2 days postoperatively. Urinalysis and urine culture were conducted selectively in symptomatic patients during the indwelling duration of the ureteral stent. All patients underwent kidney, ureter, and bladder radiological examination to confirm the position of the ureteral stents within 72 h after operation.
The patients were assigned to two groups on the basis of the presence or absence of urinary tract infections: a urinary tract–infected group and a noninfected group. Clinicopathologic characteristics between the two groups were analyzed and compared with thoroughly. We investigated and summarized every strain of pathogenic microorganism for each patient when ureteral stents were in place. Furthermore, antibiotic sensitivity of these pathogenic microorganisms was also studied comprehensively.
Statistical analysis
The mean and standard deviation values were calculated for the following characteristics: patient age, height, weight, BMI, the number of lymph nodes removed, the number of metastatic lymph nodes, surgical duration, the SCC-Ag value prior to treatment, duration of indwelling ureteral stent, creatinine concentrations during stent removal, urea nitrogen concentrations during stent removal, and glomerular filtration rate (GFR) during stent removal. Independent t-tests were employed to assess the correlation between the quantitative characteristics and the incidence of urinary tract infections. Categorical variables such as clinical stages, final pathologic stages, pathologic types, infected HPV types, neoadjuvant chemotherapy, postoperative chemotherapy, and radiotherapy are summarized using frequencies and percentages. The chi-squared and Fisher exact tests were applied to determine the association between these categorical variables and the occurrence of urinary tract infections. A p-value <0.05 was considered to be statistically significant. We conducted all statistical analyses using IBM SPSS version 26.0.
Results
Patient characteristics
A cohort of 24 patients with cervical cancer who underwent radical operation with JJ stent insertion was enrolled and subsequently followed-up. The general demographics and clinical features of these patients are presented in Supplementary Table S1. The average maximal diameter of the tumors measured 4.68 cm, indicating that the majority of these patients harbored locally advanced cervical cancer (LACC). Moreover, the average SCC-Ag value was 5.79 ng/mL, markedly elevated compared with the normal range and congruent with the size of the tumors. An overview diagram illustrating the patients with indwelling ureteral stents indwelling who experienced urinary tract infections is shown in (Fig. 1).

Overview diagram of the process of urinary tract infections in patients with ureteral stents indwelling.
Characteristics associated with clinicopathology and indwelling JJ stents
The incidence of urinary tract infections was as high as 62.5% in our cohort. Notably, 87.5% (21/24) of the patients enrolled in this study were at FIGO stage IB3 to IVA, collectively termed as LACC. Approximately 58.33% (14/24) of the patients exhibited a maximal tumor diameter exceeding 4 cm, and HPV16-positivity was observed in 65% (13/24) of the patients. More than half of the patients underwent postoperative chemotherapy and radiotherapy. Prior to and during operation, JJ stents were inserted in 79.14% of the patients: only a minor fraction (12.5%) had their stents in place for less than 3 months, whereas the majority (70.83%) retained their JJ stents for a duration of 3–12 months. It is worth noting that there is no extant standardized protocol regarding the duration of ureteral stent placement for these patients, particularly those with LACC. Because the presence of numerous pathologic risk factors, the patients were more inclined to undergo radiotherapy. Radiotherapy, however, was associated with an augmented incidence of ureteral strictures and radiation cystitis, necessitating the retention of stents until the completion of radiotherapy. We conducted an assessment of the ureteral condition after the completion of radiotherapy, and the decision to remove or replace the stents was made on the basis of the presence of ureteral obstructions, ureteral stones, urinary tract infections, or other relevant factors. The average and median durations for stent placement for our patients with radiotherapy were 7.63 months and 7 months, respectively, compared with 5.58 months and 5 months, respectively, for those individuals who did not receive radiotherapy. During stent removal, 40.91% of the patients manifested abnormal creatinine concentrations, 36% exhibited abnormal urea nitrogen concentrations, and 50% had abnormal GFR values. Of all the pathogens we identified, gram-positive bacteria accounted for 69.23% and fungi comprised 19.23% of the isolates (Supplementary Table S2).
Analysis of factors associated with urinary tract infections
Various factors such as age, height, weight, BMI, the number of lymph node resections, the number of lymph node metastases, the SCC-Ag value prior to treatment, creatinine concentrations during stent removal, urea nitrogen concentrations during stent removal, and GFR value during stent removal were compared with between patients with and without urinary tract infections (Fig. 2). However, none of these factors were determined to be a definitive risk factor for urinary tract infections, that is, these factors exhibited no correlation with the occurrence of urinary tract infections.
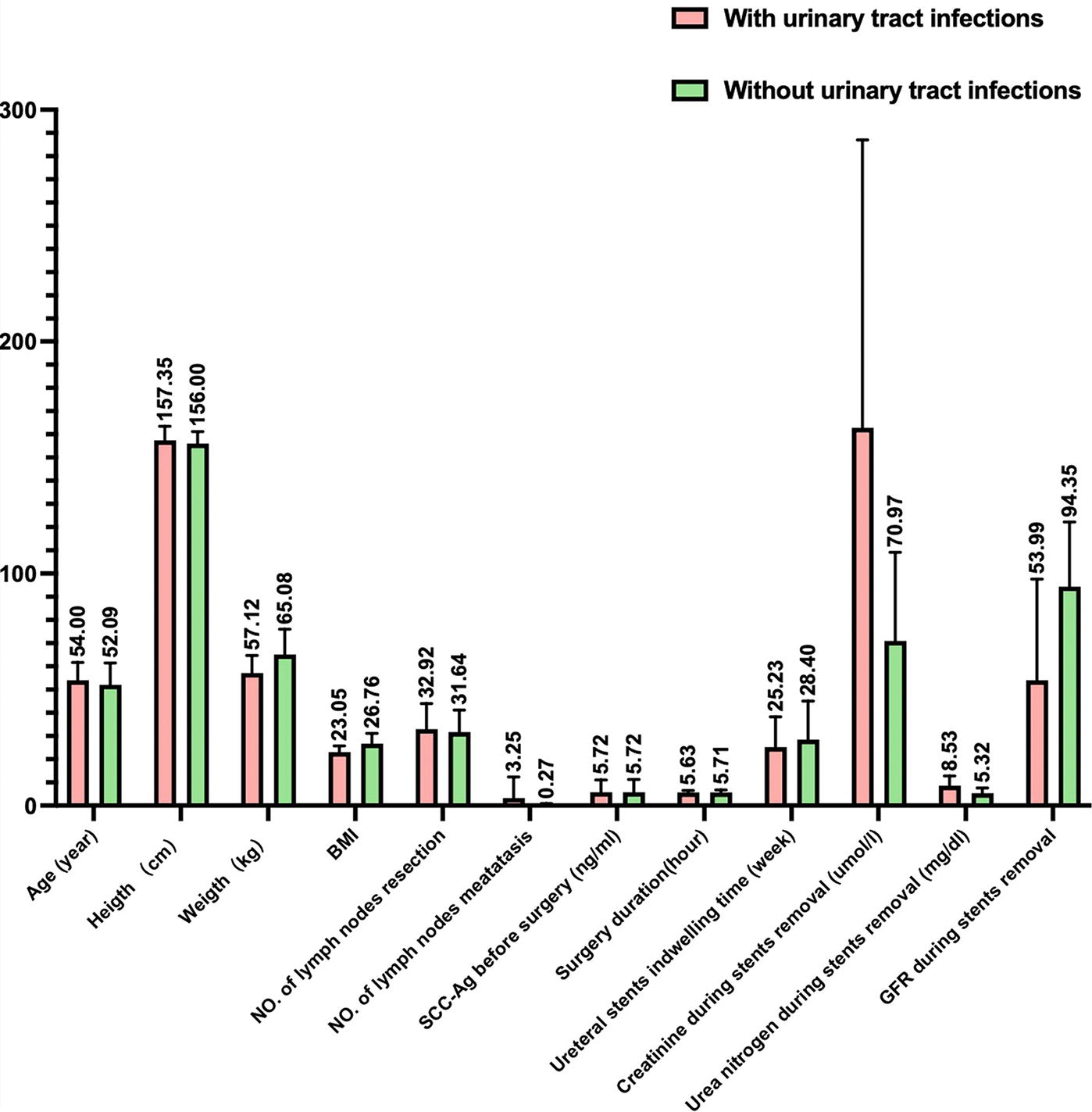
Analysis of clinicopathologic factors in patients with cervical cancer having ureteral stents indwelling on the basis of the presence or absence of urinary tract infections.
When we also assessed whether factors such as FIGO stage, pathologic type, HPV type, neoadjuvant chemotherapy, radiotherapy, and postoperative chemotherapy were associated with urinary tract infections, it appeared that postoperative adjuvant chemotherapy might have been more likely to cause urinary tract infections; however, there were no statistical differences (p = 0.074). We attribute this to the limited dataset within this study. Nevertheless, all other factors were confirmed to be not related to urinary tract infections (Supplementary Table S3).
Distribution of pathogens causing urinary tract infections in patients
A total of 30 strains of pathogenic microorganisms were detected in 15 patients with urinary tract infections, including three strains of gram-positive bacteria (Enterococcus faecalis and Staphylococcus epidermidis), 22 strains of gram-negative bacteria (primarily Escherichia coli [E. coli] and Klebsiella pneumoniae), and five strains of fungi (principally Candida albicans). Importantly, we identified two strains of carbapenem-resistant Enterobacteriaceae (CRE) (Table 1).
Pathogens of Urinary Tract Infections in Patients with Cervical Cancer Having Radical Operation with Ureteral Stents Indwelling
CRE = carbapenem-resistant Enterobacteriaceae.
The pathogens that caused urinary tract infections varied during the period in which JJ stents were in place. Five of 24 patients (20.83%) experienced infections with two different types of pathogens, whereas 12.50% (3/24) exhibited infections with three or more types of pathogens (Tables 1 and 2). An antibiotic sensitivity analysis for E. coli, the most common pathogen of urinary tract infections, revealed resistance to ampicillin, ceftriaxone, cefotaxime, cefazolin, and cefuroxime. We observed moderate sensitivity toward ciprofloxacin, levofloxacin, trimethoprim/sulfamethoxazole, aztreonam, ceftazidime, cefepime, and ampicillin/sulbactam. The majority of E. coli strains were sensitive to imipenem, meropenem, piperacillin/tazobactam, tigecycline, and amikacin (Supplementary Table S4 and Fig. 3). Urine culture and antibiotic sensitivity test results demonstrated that as the duration of indwelling JJ stents increased, the pathogens that caused the urinary tract infections became more complex and challenging to manage. Two important trends emerged: (1) the pathogens shifted from common to rare types and even to fungi; and (2) antibiotic resistance substantially increased for the same pathogen. We ascertained that the sensitivity of antibiotics to the same pathogen declined when the ureteral stents were in place for more than 2 months. Furthermore, fungal infections were more likely to occur when the stents were in place for more than 4 months.
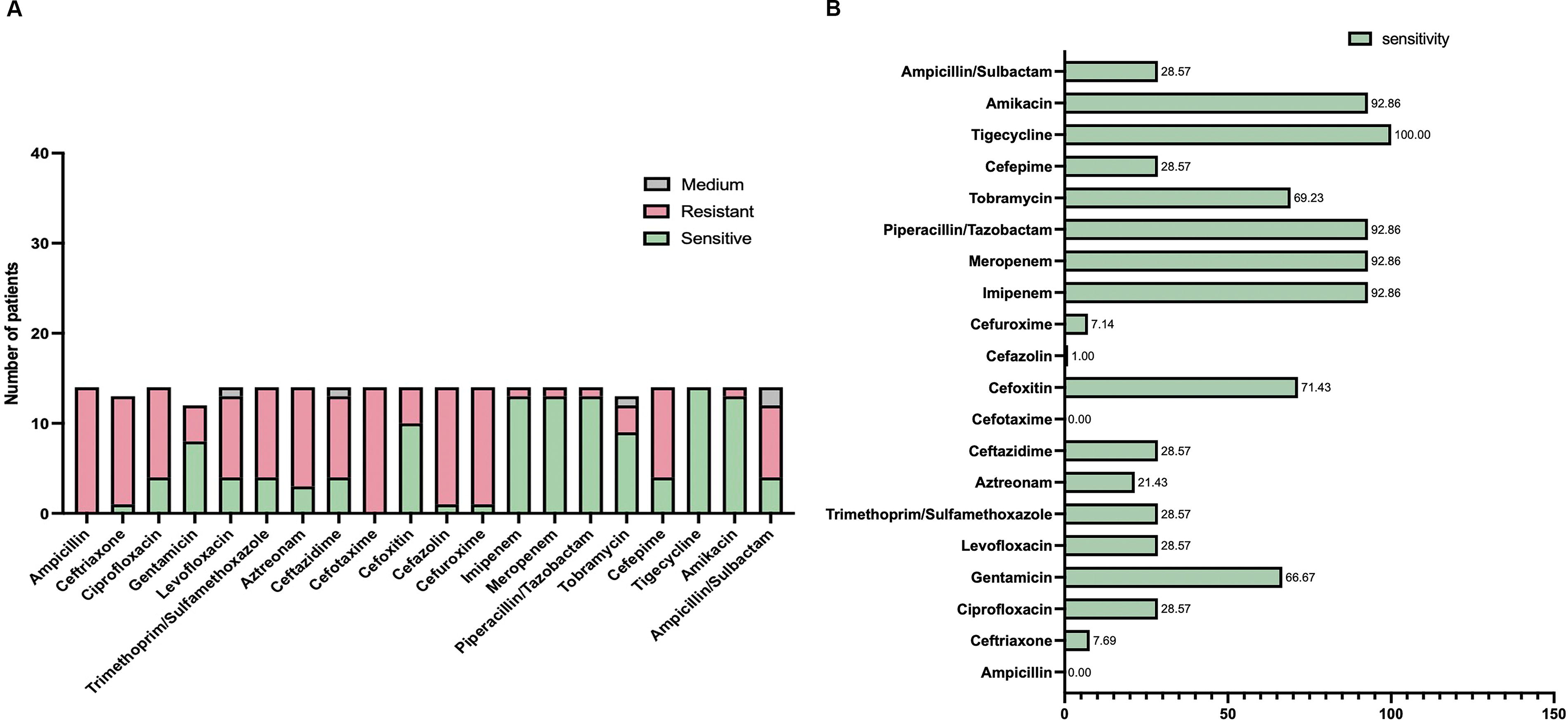
Analysis of antibiotic susceptibility of E. coli isolated from urinary tract infections in patients with cervical cancer having radical operation with indwelling ureteral stents.
Pathogens of Urinary Tract Infections During Ureteral Stents Placement and Factors Related to Severe Complications of Renal Fistula
CRE = carbapenem-resistant Enterobacteriaceae.
Finally, 16.7% (4/24) of the patients underwent percutaneous nephrostomy because refractory urinary tract infections or vesicovaginal fistulas.
Discussion
Cervical cancer is the most prevalent gynecologic malignant disease, and for early-stage cervical cancer, surgical intervention—specifically radical hysterectomy combined with pelvic lymphadenectomy—constitutes the primary treatment approach. When high-risk factors are present, postoperative radiotherapy and chemotherapy are required. Open radical hysterectomy is currently one of the most common treatments for early-stage cervical cancer, with a 5-year disease-free survival rate exceeding 90%.14–16 In the surgical management of patients with early-stage cervical cancer, urinary system complications frequently arise because the proximity of the cervix to the bladder and other urologic structures 17 ; and these complications can produce considerable personal, economic, and societal burdens, profoundly impacting patients’ quality of life and substantially increasing treatment costs. Ureteral stents are indispensable in numerous urologic procedures, including the management of ureteral strictures, renoureteral stones, and iatrogenic injuries of the ureter during complex abdominal operation.18,19 However, the use of prophylactic ureteral stents to mitigate injury and associated complications in patients with cervical cancer remains controversial, and the optimal duration for indwelling ureteral stents is not well defined. 20
Primary treatment modalities (surgery, radiotherapy, and chemotherapy) for cervical cancer may harm the ureter, leading to ureteral strictures. Consequently, some physicians tend to insert ureteral stents during operation to prevent and reduce urinary-related complications,21,22 advocating for stent placement as instrumental in facilitating the intraoperative identification of the ureter and reducing the incidence of postradiotherapy ureteral strictures. Once the ureter is injured, the ureteral stents might serve as a tool for early diagnosis, prognostic assessment, and treatment monitoring. 23 A retrospective study conducted by Redan and McCarus involving 151 patients who underwent pelvic operation with the insertion of lighted ureteral stents found no ureteral injuries during or after operation. Thus, these authors concluded that prophylactic placement of lighted ureteral stents was both safe and cost-effective. 24 However, many studies have indicated that preoperative ureteral stenting does not reduce the onset of urologic complications during or after pelvic operation.8,25 Hwang et al. retrospectively reviewed medical records of 146 patients with cervical or endometrial cancer who underwent laparoscopic radical hysterectomy with lymphadenectomy and found that two patients experienced postoperative urologic complications among 13 patients (8.9%) with prophylactic double ureteral stents, and nine patients (6.2%) developed postoperative urologic complications regardless of stent placement. 25 Chou et al., in a 12-year randomized trial, did not find a statistical difference in the incidence of ureteral injury between patients with (1.20% [19/1,583]) or without (1.09% [17/1,558]) bilateral prophylactic ureteral catheterization. 8 Another study also showed that prophylactic ureteral stent insertion did not affect the rate of ureteral injury and reflected a lower cost-effectiveness than expected. 18
Given that the stent is a non-native object within the body, it may potentially elicit discomfort for patients, facilitate bacterial colonization, induce hematuria, evoke irritative voiding symptoms, and promote the deposition of urine components26–28 ; and these stent-related complications substantially augment the patient’s burden and detract from their overall quality of life.17,29,30 Urinary tract infection constitutes one of the most prevalent and critical complications associated with indwelling ureteral stents. Studies have indicated a relatively high incidence of stent-associated urinary tract infections, ranging from 13% to 28%.31–33 Although the use of prophylactic antibiotics might increase the development of further resistance and not prevent the attachment and biofilm formation of urinary tract pathogens that are already resistant, it might serve as an effective method to kill potential urinary tract invaders before they adhere to the surface of the ureteral stents. 34 However, some investigators found that antibiotic prophylaxis or concomitant antibiotic administration did not appear to reduce the incidence of stent-related urinary tract infections.35,36 Although there are no specific guidelines concerning antibiotic prophylaxis for ureteric stent placement, the American Urological Association and the European Association of Urology both recommended periprocedural antibiotic prophylaxis for patients undergoing these procedures.36,37 Consequently, the determination of the bacterial sensitivity to antibiotics and the identification of antibiotic-resistant forms of bacteria would optimize antibiotic therapy during ureteral stent use.
A majority of studies on ureteral stent insertion for patients with cervical cancer currently focus on the detrimental consequences associated with urinary tract injuries, whereas few authors have examined urinary tract infections with stents. Consequently, an even more limited number of studies have documented the pathogenic flora of urinary tract infections.
This study encompassed 24 patients who underwent radical operation for cervical cancer and had indwelling ureteral stents. Cephalosporins combined with metronidazole were the most common prophylactic antibiotics administered to patients in this study. The literature mainly chose cefoxitin, trimethoprim–sulfamethoxazole, or nitrofurantoin as prophylactic antibiotics.38,39 Notably, 73.91% of the patients received postoperative chemoradiotherapy. The incidence of urinary tract infections rose to 62.5%, markedly exceeding the range reported by previous studies.31–33 Various factors—including age, height, weight, BMI, the number of lymph node resections and metastases, SCC-Ag concentrations prior to operation, FIGO stage, pathologic type, HPV type, neoadjuvant chemotherapy, and radiotherapy—were all confirmed to be unrelated to the occurrence of urinary tract infections. However, we did observe a nonstatistically significant tendency toward an association between postoperative adjuvant chemotherapy and urinary tract infections. We attribute the lack of significance to the relatively small sample size and the high proportion of patients with LACC in the present study. Additionally, the prolonged placement of ureteral stents emerged as a pivotal factor in promoting and inducing urinary tract infections; and this is supported by the literature, whereby the management of stent-associated infection depended upon the frequent replacement and early removal of stents.12,17 The primary pathogenic microbes implicated in these infections were E. coli, K. pneumoniae, E. faecalis, S. epidermidis, and C. albicans. Many authors have also reported that E. coli was often the most commonly cultured and identified organism in patients with stents, which was similar to this study.40,41 With an extended duration of ureteral stent placement, we noted a decrease in drug sensitivity among the same pathogens and an increase in antibiotic resistance; and the microbial spectrum shifted from bacteria to fungi over time. Notably, we identified two cases of CRE, and the urinary tract infection rate in this study was substantially greater than that reported in previous analyses. We hypothesize the primary reasons for this increased incidence as follows: first, the majority of patients in this study possessed LACC that was characterized by large tumors and high surgical complexity; second, a substantial proportion of patients underwent postoperative chemoradiotherapy that exacerbated the occurrence of ureteral complications; and final, the average duration of ureteral stent placement exceeded 3 months.
This study has several limitations. First, patient sample size was comparatively modest, encompassing only 24 individuals, and this could partially account for the disparity in the incidence of urinary tract infections that we observed in contrast to other reports in the literature. Second, the design of our study was retrospective, and all surgical procedures were performed by only one surgeon. Consequently, the interpretation of our results must be approached with caution. Randomized studies are needed in the future to establish the role of perioperative ureter stenting for urologic complications in patients with LACC having radical pelvic operation.
Conclusions
The rate of urinary tract infections in our study was as high as 62.5%, far exceeding that reported in other studies. We attribute the elevated incidence of infections to the following reasons: (1) the majority of patients included had LACC with large tumors and high surgical difficulty; (2) a substantial proportion of patients underwent postoperative chemoradiotherapy; and (3) the average duration of ureteral stent placement was relatively prolonged. Although no statistically significant difference was observed, postoperative adjuvant chemotherapy emerged as a potential risk factor for urinary tract infections. We herein demonstrated that gram-negative bacteria, particularly E. coli, were the most prevalent pathogens causing urinary tract infections. Notably, the E. coli exhibited resistance to penicillins and cephalosporins but remained generally sensitive to carbapenems and glycylcyclines. With the duration of ureteral stent placement exceeding 2 months, the sensitivity of the same pathogen toward corresponding antibiotics decreased, and this was accompanied by a gradual increase in drug resistance. Furthermore, the pathogenic microbes in individual patients transitioned from weakly pathogenic bacteria to highly pathogenic bacteria, ultimately culminating in fungal infections; these typically occurred after the ureteral stents were in place for more than 4 months. This suggests that the pathogens that caused the urinary tract infections in this study became increasingly complex and challenging to manage with prolonged ureteral stent placement.
Footnotes
Acknowledgment
Authors’ Contributions
C.J.: Data curation, formal analysis, investigation, visualization, and writing—original draft. H.B.: Data curation, investigation, and project administration. J.X. and Chengjuan J.: Conceptualization, funding acquisition, investigation, methodology, project administration, supervision, and writing—review and editing. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Data Availability
All data and materials are accessible in the supplementary information. Patient data from this study are available upon request because there are ethical restrictions on sharing the data publicly. Approval to conduct the study was received from the corresponding author (Dr. Chengjuan Jin, Email:
Ethics Approval and Consent to Participate
All clinical data and information were collected after informed consent was obtained from the patients or their guardians. Ethical approval of this study was obtained from the ethics committee of Shanghai General Hospital.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This work was supported by the National Natural Science Foundation of China (grant no. 82002736) and Nosocomial Infection Management Project Foundation of Shanghai General Hospital (grant no. SYYG20221027).