
Abstract
Background:
Finegoldia magna is a species of anaerobic gram-positive coccus considered part of human microbiota. It has been described as a cause of skin and soft tissue infections, but it is not a common cause of operation-related infections.
Objectives:
Describe the characteristics, treatment, and results of musculoskeletal infection by F. magna treated in our center.
Methods:
We performed a descriptive, retrospective observational study. Clinical records of all musculoskeletal surgical infections treated in our department between 2012 and 2022 were reviewed. We selected the patients with a positive culture for F. magna. Risk factors for infection, patient’s medical records, previous operation performed, time from surgical procedure to infection, susceptibility tests, antibiotic and surgical treatment for the infection, and recovery rate were registered for the analysis.
Results:
Twenty patients have positive cultures for F. magna, representing 15.5% of the anaerobic infections. Eleven of them were arthroplasties, three fracture synthesis, two foot operations, two spinal operations, and two soft tissue operations. All patients underwent operation and antibiotic treatment. The most commonly used antibiotic scheme was amoxicillin followed by amoxicillin-rifampicin. Eighty percent of the patients achieved a complete clinical recovery with a mean of 2.1 surgical procedures. Patients with polymicrobial infections required twice the number of operations (p = 0.047) and exhibited a failure rate of 36% compared with 0% for monomicrobial cases (p = 0.043).
Conclusions:
Orthopedic infections caused by F. magna are infrequent, but they usually have good outcomes. Polymicrobial infection with F. magna exhibits poorer clinical results and requires a greater number of operations compared with monomicrobial ones.
Introduction
Finegoldia magna is a species of gram-positive anaerobic coccus (GPAC), formerly known as Peptostreptococcus magnus. Despite being a component of the normal microbiota, it possesses the potential to induce opportunistic infections, including soft-tissue abscesses, endocarditis, and orthopedic infections such as necrotizing fasciitis, osteosynthesis infections, and periprosthetic joint infections (PJIs).1–3
Implants are extensively used in orthopedic surgical procedure, addressing both fractures and osteoarthritis, and infection represents a dreadful complication of these procedures. 4 The primary pathogens responsible for orthopedic implant infections are Staphylococcus aureus, Streptococcus spp., and Enterobacteriaceae. Less commonly, anaerobic bacteria are identified, with Cutibacterium acnes being the predominant species, followed by F. magna. 4
F. magna belongs to the category of GPACs, which are human commensal organisms. These bacteria inhabit various surfaces, including the mouth and skin, as well as the gastrointestinal and urogenital tracts.5,6 Although F. magna is the only species of clinical importance in this genus, it is a rare cause of PJI, accounting for 5%–15% of all anaerobic isolates.1–4,6–9
F. magna is the most pathogenic species because of the presence of specific virulence factors.1,4,7,10 F. magna hinders wound epithelialization by secretin collagenases, protein FAF (F. magna adhesion factor), a crucial factor inhibiting integrins, and SufA protein, responsible for collagen degradation. 6 Furthermore, it is able to adhere to inert surfaces and form biofilm. 11 Notably, it diminishes the immune response through the FAF protein, neutralizing neutrophil activity, and the L-protein, which reduces B lymphocyte activity while blocking antibody action.5,6 Although F. magna is related to the Clostridia class, it does not usually present the same virulence factors; as a result, it is uncommon to see necrotizing fasciitis caused by this particular pathogen.
It can present itself as both chronic and acute infections, but it is more frequently involved in chronic infections.4,8 In addition, in a high percentage of cases, it appears as part of a polymicrobial infection with other bacteria, especially S. aureus, although it also can cause monomicrobial infections.1,6,9
Low resistance rates (10%–20%) to penicillin, metronidazole, clindamycin, linezolid, and cefoxitin have been described, similar to the rest of other members of the GPAC group.1,3,4,9 However, a greater resistance rate has been observed for erythromycin and tetracycline.1,12
PJI treatment, either knee or hip, depends fundamentally on the onset of the infection. In acute infections (<3–4 wks), a debridement with implant retention plus targeted antibiotic therapy (DAIR) could be an effective treatment. 13 Chronic or recurring infections are more challenging, a complete replacement of the joint must be performed (in a 1-stage or 2-stage manner) followed by targeted antibiotic agents.7,13
Management of fracture-related osteosynthesis infections relies on the degree of consolidation. If the fracture is consolidated, it is safer to remove the material and debride. If there are no signs of consolidation, the best option could be the extraction of the material, use of an external fixation during the targeted antibiotic therapy, and later add bone graft and new osteosynthesis material. 14
For all musculoskeletal infections, it is possible to find important damage to the surrounding soft tissues. If there is exposure of noble structures such as bones, tendons, or even osteosynthesis material, a covering flap must be performed. 15 There are rescue therapies when all of the above fails, such as antibiotic suppression, arthrodesis, or even amputation.13,14
In the literature, clinical cases of infections caused by F. magna leading to necrotizing fasciitis and soft tissue abscesses can be found.1,11,16 Some series of cases could be found of PJIs caused by F. magna in studies about anaerobic infections.2–4,7,8,17
Methods
Our main objective was to describe the characteristics, treatment, and results of musculoskeletal infection by F. magna treated in our center.
We performed a descriptive, retrospective observational study. We reviewed the clinical records of all musculoskeletal infections treated in our department between 2012 and 2022. Patients with positive cultures for F. magna that fit the criteria of infection with at least one year of follow-up were included in the study.
All samples (synovial fluid, biopsies, implant sonication) were cultured on aerobic and anaerobic media (Schaedler-5% sheep blood agar, BioMérieux, France). Anaerobic media were incubated in an anaerobic atmosphere for 7 days, extending to 14 days if infection was clinically suspected. Microorganisms were identified using MALDI-ToF (Vitek MS, BioMérieux, France), and antimicrobial susceptibility testing was performed using E-test strips according to CLSI criteria. In selected cases, a multiplex PCR was performed for diagnosis (Unyvero i60ITI, Curetis AG).
Data were obtained from the electronic and written medical records and transferred onto a structured data sheet. Data and information collected included age, gender, body mass index (BMI), American Society of Anesthesiologists (ASA) classification, Charlson Comorbidity Index (CCI) score, medical history, localization of the infection, surgical technique, antibiotic therapy, culture antibiogram, duration of treatment, outcome post-treatment, and delay between operation and bacterial identification.
The surgical technique was chosen by the orthopedic surgeon in consultation with an infectious diseases specialist. A good clinical recovery with no signs of inflammation was considered as a favorable outcome. We considered poor outcome or treatment failure if patients needed chronic suppression antibiotic treatment, no re-implantation of the prosthesis, amputation, or infection-related death.
Intra-operative bone tissue, synovial membranes, and either prosthesis or osteosynthesis hardware were obtained for the microbiologic diagnosis. All patients received an empiric intravenous antibiotic regimen with vancomycin and ceftazidime following operation until antimicrobial susceptibility was available, when antibiotic treatment was changed to targeted therapy.
Relevant data were inserted into an electronic database (Microsoft® Excel for Windows® Microsoft Corp, Redmond, WA) for further analysis. Mean and standard deviation (SD) were used to describe quantitative variables and frequency and percentage for qualitative variables. Quantitative variables were compared using Student’s t-test, whereas we used either chi-squared test or Fisher exact test for qualitative variables. This study was approved by the Ethics Research Comittee of our institution (reference EO053-21_FJD).
Results
From 2,048 patients with musculoskeletal infections treated in our institution between 2010 and 2022, 20 had a positive culture for F. magna, representing 0.97% of all infections and 15.5% of all anaerobic infections. It was the second most frequent anaerobic infection, after C. acnes, which represented up to 79.32% of the anaerobic infections.
In our sample, 45% of the patients were male, with an average age of 55 years (SD ± 15). The mean duration from operation to the onset of infection was 8.9 months (SD ± 11). Notably, only 8 out of 20 patients (40%) developed the infection within the initial three months post-operation, whereas 7 out of 20 patients (35%) manifested symptoms more than one year after the surgical procedure. The patients’ data are summarized in Table 1.
Comparison Between Monomicrobial and Polymicrobial Infections Caused by Finegoldia magna
ASA = American Society of Anesthesiologists; x¯ = mean; CCI = Charlson Comorbidity Index; BMI = body mass index; N = number; SD = standard deviation. The bold p-values denote statistical significance.
Regarding infection risk factors, 45% of patients had a smoking habit, 10% had a history of cancer and autoimmune disease, and 5% had conditions such as renal insufficiency, chronic obstructive pulmonary disease, liver disease, and immunosuppression. The average ASA score was 2 (SD 0.5), the mean CCI was 1.5 (SD ± 1.5), and the average BMI was 29.5 (SD ± 5.3).
In 16/20 cases (80%), F. magna tested positive in ≥2 synovial tissue samples; in 5/20 cases (25%), sonication fluid culture was positive; in 2/20 cases (10%), both were positive; and in 1 patient (5%), the microbiologic diagnosis was made through multiplex PCR. In our series, 11/20 patients (55%) had a polymicrobial infection, S. aureus being the most frequent concomitant bacteria in 8/11 (72%).
In our sample, 11 patients had infections following joint arthroplasty as follows: 5 total hip arthroplasties (THAs), 3 total knee arthroplasties (TKAs), 2 total shoulder arthroplasties (TSAs), and 1 total elbow arthroplasty (TEA). Among the five THA cases, three were successfully treated with a single DAIR, one underwent one-stage revision with satisfactory results, and one required prosthesis removal after two unsuccessful DAIR procedures. The three TKA patients presented complex challenges as follows: one needed a gastrocnemius flap in addition to two DAIR procedures, another underwent arthrodesis after two DAIR procedures, and the third ended up with suppressive antibiotic therapy after four surgical procedures. Both TSA cases were managed with two-stage revisions, one yielding satisfactory outcomes and the other necessitating resection arthroplasty despite two attempted revisions. The lone TEA patient achieved infection eradication after 2 two-stage revisions.
Concerning the three patients with fracture osteosynthesis infections (one ankle fracture, one tibial plateau fracture, and one pelvic ring fracture), all were initially treated with debridement and removal of osteosynthesis material, with a single surgical procedure proving sufficient for infection healing without further complications.
Two patients experienced infections following hallux valgus correction operation, both requiring two debridements. However, one did not heal and, ultimately, underwent first toe amputation. In two cases of prior spinal arthrodesis infections, both patients had positive outcomes with a single debridement. Finally, two patients with soft tissue operation infections—direct repair of the Achilles tendon and drainage of a hand hematoma—attained favorable results with a single debridement operation.
The sensitivity to various antibiotic agents is reflected in Figure 1. Twenty-one percent of strains were resistant to clindamycin, and only 5% resistant to penicillin. There were no cases of resistance against metronidazole, cefoxitin, imipenem, and amoxicillin. No resistant strains were detected against vancomycin, rifampicin, or linezolid when Staphylococcus spp. breakpoints were used. The most commonly used antibiotic regimen was amoxicillin with clavulanic acid in 7/20 cases (35%), followed by amoxicillin in combination with rifampicin in 5/20 cases (25%) and amoxicillin with clindamycin in 2/20 cases (10%).
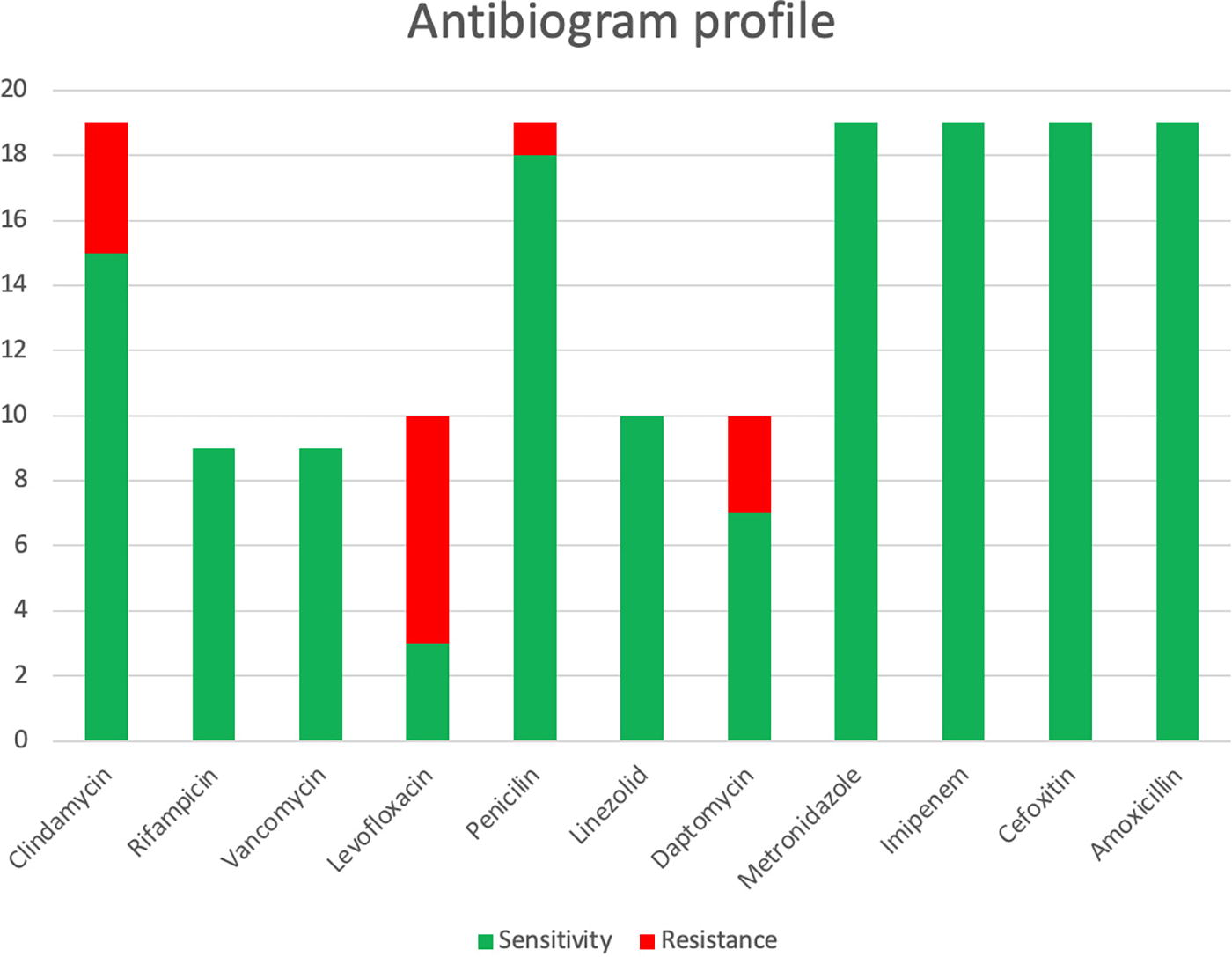
Antibiogram profile of Finegoldia magna strains.
Our patients required a mean of 2.1 operations (1.5 SD) after diagnosis of infection to achieve infection eradication, which was achieved satisfactorily in 80% of patients (16/20). Two patients requiered prosthesis removal (one THA and one TSA), one patient had antibiotic suppression therapy (TKA), and one patient needed an amputation to eradicate the infection (hallux valgus operation). There were no infection-related deaths. Interestingly, we found that patients with F. magna infections in the context of polymicrobial infections had worse outcomes in terms of failure (p = 0.043). All patients who did not achieve healing belonged to this group and also required two times more surgical procedures, 1.3 versus 2.7; p = 0.047. These differences cannot be attributed to the chronicity of the infections, as there are no differences in the percentage of chronic and acute infections between both groups (p = 0.582). Analyzing this group of patients, we found that they had more prevalence of risk factors compared with the monomicrobial group, but only the difference in ASA was statistically significant (1.7 vs. 2.1; p = 0.046) (Table 1). Interestingly, when we analyzed the strains of these patients, they showed differences too with a greater resistance rate to clindamycin, tetracycline, and penicillin, although only the last one reached statistical significance.
Discussion
F. magna is a GPAC, previously named P. magnus. Although it is part of the normal human microbiota, it can cause orthopedic operation-related infections. 1 It is capable of causing opportunistic infections because of its ability to delay wound healing, evade the immune system, and generate biofilm.1,2,4,6,7,10 It is the most virulent bacteria among GPACs, and it is the second most common anaerobic pathogen in infections after C. acnes, with a prevalence of 15% among all anaerobes,4,7 the same prevalence we found in our study.
Although it is described to particularly affect immunocompromised patients or those with substantial infection risk factors, 6 the patients in our study had few or none of these risk factors, with only 10% experiencing any form of immunosuppression. A noteworthy finding, consistent with literature,2,4,8 is its involvement in chronic infections more than acute ones, with 40% being acute and 60% chronic in our study. One reason for this delayed onset could be the indolent nature of F. magna infections, which may take longer to show symptoms. No patient in our study suffered from F. magna bacteremia. This finding aligns with the typically localized nature of F. magna infections.
Regarding the antibiotic resistance of the strains identified in our patients, we found no resistance to rifampicin, vancomycin, and linezolid, consistent with the previous literature.3,4 As for clindamycin, we observed a 21% resistance rate, similar to findings in the literature except1,3 for one study reporting more than double this rate. 9 Only one strain resistant to penicillin was found, accounting for 5%, slightly greater than reported in the literature.1,3,4,9
For proper infection treatment in orthopedic operation, precise microbiologic diagnosis is essential. That is why sonication has gained much significance in the last years.18,19 In our study, 25% of patients had a microbiologic diagnosis through this technique. The most commonly used antibiotic in our sample to treat F. magna infections was amoxicillin, either as monotherapy or in combination with rifampicin or clindamycin primarily, patterns similar to those found in the literature. 4
In our study, although the final decision regarding surgical treatment was made by each patient’s surgeon, standard treatment guidelines for orthopedic infections were followed.13,14 DAIR was performed for acute infections, with revision operation, in one or two stages, in case of failure or for chronic infections. For consolidated osteosynthesis infections, debridement and removal of material were conducted, and for soft tissue infections, debridements were performed. Soft tissue defects were addressed with grafts or flaps depending on the bed and extent. In cases of recurrent infections or failure of previous treatments, various alternatives were considered as follows: non-re–implantation of prostheses, antibiotic suppression, or even amputation.
We experienced a relatively high treatment failure rate (20%). However, previous literature already indicates that these infections may yield poor outcomes. 4 F. magna can cause monomicrobial infections or be involved in polymicrobial infections,1,6 and in our study, we observed that the clinical presentation of those infections is entirely different. Monomicrobial F. magna infections have better outcomes with a high rate of complete infection remission, and the majority only requires a single operation for recovery. In contrast, polymicrobial infections exhibit a high failure rate and double operations compared with the monomicrobial group. It is already known that polymicrobial infections tend to have worse outcomes.20,21 This is partly attributed to the fact that patients in these cases generally have a poorer baseline condition with more risk factors, a finding also observed in our study, with a significant increase of the ASA. Interestingly, we also discovered that strains of F. magna in polymicrobial infections displayed a greater rate of antibiotic resistance.
This study is the largest case series about F. magna orthopedic infections and provides a deeper view of the importance of these infections in orthopedic operation. Nevertheless, it has some limitations. First of all, it is a descriptive retrospective and observational study with bias associated with these types of studies. Second, patients had different types of infections so results may differ depending on the surgical site and syndrome. Third, although it is one of the studies on orthopedic operation infection caused by F. magna with a greater number of patients, it remains a low number. Further studies with larger number of patients should be performed to achieve more solid results, especially for antimicrobial susceptibility of these isolates. In addition, the fact that analyzed data derived from only one hospital may have biased our findings because of local epidemiology differences.
Conclusions
Orthopedic surgical procedure infections caused by F. magna are infrequent, but their proper treatment is crucial. Monomicrobial infections show good outcomes, whereas when F. magna is identified in a polymicrobial infection, they exhibit poorer clinical results, patients require a greater number of surgical procedures, and strains are more antibiotic resistant.
Footnotes
Authors’ Contributions
S.G.: Data collection, formal analysis, and writing—original draft. J.E.: Supervision and writing—review and editing. C.O.-P.: Data collection. A.B.-G.: Validation and supervision. A.A.: Conceptualization, supervision, and writing—review and editing.
Author Disclosure Statement
The authors declare that they have no conflicts of interest relevant to the content of this article.
Funding Information
None of the authors has received financial payments or other benefits from any commercial entity related to the subject of this article.