
Abstract
Background:
There is a lack of consensus on the optimal antibiotic regimen for pediatric appendicitis, and conflicting data exist regarding the need for extended-spectrum use in this population. We implemented an antibiotic stewardship program with a standard, preferred antibiotic regimen for both uncomplicated and complicated appendicitis and hypothesized that clinical outcomes would be equivalent.
Methods:
This is a single-institution, retrospective study of pediatric patients (≤18 y) who underwent appendectomy for acute appendicitis between October 2015 and May 2022. We used institutional data from our stewardship program supplemented by manual chart review. Patients were assigned to pre- and post-pathway cohorts on the basis of appendectomy date. Patients were further stratified on the basis of whether they met criteria for complicated appendicitis on the basis of intra-operative findings.
Results:
There were 752 patients that were included: 346 (46.0%) in the pre-pathway cohort and 406 (54.0%) in the post-pathway cohort. The pre-pathway cohort had a higher rate of complicated appendicitis (40.2 vs. 25.6%). However, pre- and post-pathway cohorts had similar rates of post-operative infections, readmissions, and reoperations. When separated by complicated operative findings, patients with uncomplicated appendicitis had a shorter length of stay post-pathway implementation (p < 0.001). After controlling for complicated operative findings and pertinent covariates, the preferred antibiotic regimen was independently associated with decreased odds of post-operative organ space surgical site infections (SSI) (adjusted odds ratio 0.22, 95% CI: 0.05–0.99).
Discussion:
Antibiotic stewardship to increase the use of a standardized, preferred antibiotic regimen did not result in worse clinical outcomes. The preferred regimen was significantly associated with a decreased rate of organ space SSI, even when controlling for complicated operative findings. The mechanism of this finding requires additional study.
Key Take-Aways
Many institutions have found equivalent outcomes after narrowing antibiotic regimens for uncomplicated and complicated pediatric appendicitis.
At our institution, a standard, preferred antibiotic regimen was associated with lower odds of post-operative organ space infection in immunocompetent patients who underwent appendectomy.
Introduction
Antibiotic stewardship is the process of selecting appropriate antibiotics to balance adequate treatment of infection while avoiding toxicity and development of resistant organisms. Appendectomies are the most common abdominal operation performed in the pediatric population, and the annual incidence of appendicitis in the United States is rising.1,2 Antibiotics play a key role in the management of uncomplicated and complicated appendicitis; however, there are conflicting data about which agents maximize treatment efficacy without toxicity or antimicrobial resistance.
In the last two decades, antibiotic treatment practices for appendicitis have been significantly refined. Prospective randomized trial data analysis in children with perforated appendicitis compared with ceftriaxone and metronidazole to a historical three-agent regimen. 3 The authors demonstrated a more efficient and cost-effective regimen with no difference in abscess rate or wound infections using ceftriaxone and metronidazole. Since that time, several large database studies have been conducted citing non-inferiority of narrow-spectrum antibiotics in both uncomplicated and complicated appendicitis, and in some cases, decreased adverse outcomes when antibiotics are narrowed for uncomplicated cases.4–6 However, a recent dual institution randomized trial compared with piperacillin/tazobactam to ceftriaxone/metronidazole and demonstrated lower rates of intra-abdominal abscess and fewer post-operative emergency department visits, causing many centers to reevaluate their preferred antibiotic regimen. 7
In November 2018, our institution implemented a standard pathway for all cases of pediatric appendicitis, utilizing a preferred antibiotic regimen. This study was designed to evaluate clinical outcomes in uncomplicated and complicated appendicitis. The primary outcome of this study was the impact of the preferred regimen on post-operative organ space surgical site infection. Secondary outcomes included length of stay (LOS), total surgical site infections (SSI), percutaneous drain placements, 30-day readmissions, and reoperations.
Methods
Study design and data source
We performed a single-institution retrospective cohort study using a combination of three data sources: our institutional National Surgical Quality Improvement Project Database (NSQIP-P), antibiotic stewardship database, and manual review of the medical record. The NSQIP-P database samples laparoscopic and open appendectomies and patient information, and outcomes are collected by a trained surgical case reviewer. The antibiotic stewardship database includes all medication administration record data during a given encounter. This is a single institution study, which examined NSQIP-Pediatric data supplemented by manual chart review. This approach was chosen to allow standardized definitions of patients to be used and to decrease study team bias during chart review. Additionally, NSQIP-P is our primary resource for tracking our outcomes in a risk adjusted way. During the study period from October 2015 to May 2022, cases from 10 pediatric surgeons were included in the study. Surgeries were performed primarily laparoscopically (97.1%), with no significant variation in technique. The entries from these databases were merged for all pediatric patients treated for acute appendicitis, then merged with our institutional pharmacy antibiotic stewardship dashboard. This dashboard includes records of all patients who received antibiotics including type and date. We abstracted all other information—including incomplete patient data—by manual review of the electronic medical record.
Pathway implementation
A quality improvement project was implemented in November 2018 with the aim of standardizing antibiotic regimen on the basis of stewardship principles for both uncomplicated and complicated pediatric appendicitis. Pathway design included multidisciplinary input from surgeons, infectious disease specialists, and infectious disease pharmacists. As part of pathway design, we reviewed our institutional antibiogram and noted that our rates of community acquired pseudomonas infections were similar to national averages and that it was not commonly cultured from intra-abdominal abscesses, which increased buy-in from stakeholders but did not guide antibiotic selection. Patients receive a preferred antibiotic regimen after diagnosis, prior to surgery (ceftriaxone/metronidazole or ciprofloxacin/metronidazole for penicillin-allergic patients). Patients with intra-operative evidence of complicated appendicitis additionally receive antibiotics post-operatively for a course of 7–10 days. This includes oral antibiotics on discharge to complete their course. This flexible duration was included on the basis of guidelines from the Surgical Infection Society Guidelines, which recommend 5 days of post-operative antibiotics for perforated appendicitis with adequate source control, longer courses for inadequate source control, and more than 7 days for patients who develop an abscess post-operatively. 8 This was agreed upon after discussion with a multi-disciplinary team with the intention of providing as short a course as possible. Patients without evidence of perforation received no antibiotics post-operatively.
The pathway includes a specific “pediatric appendicitis antibiotics” order panel in the electronic medical record that includes clinical decision support for the recommended type and dosing of antibiotics.
Study cohort selection and assignment
We included patients <18 years old. Patients were excluded if they did not undergo appendectomy during index hospitalization, if a percutaneous drain was placed prior to appendectomy, or if the primary indication for the procedure was not acute appendicitis. Patients were also excluded if they had a comorbidity that was associated with a significant immunocompromised status (oncologic comorbidity, active chemotherapy treatment).
Patients were then assigned to pre- or post-implementation cohorts on the basis of the date of appendectomy. If a patient received any doses of non-preferred antibiotics, they were labeled as having received a “non-preferred” regimen.
Patients were considered to have complicated appendicitis if any of the following intra-operative findings were present in the operative note: visible hole in the appendix, extraluminal fecalith, intra-abdominal abscess, or fibrinopurulent exudate in more than one quadrant. In accordance with the NSQIP-P definitions, gangrenous appendicitis without any of the intra-operative findings was considered uncomplicated. We selected this definition as it is the standardized definition used in NSQIP-P to classify patients as either simple or complicated appendicitis. 9
Data collection
We collected demographic, clinical, and operative data, including operative findings. Post-operative outcomes included overall length of stay, post-operative SSI, 30-day readmission, 30-day reoperation, placement of a percutaneous drain, placement of a peripherally inserted central catheter, and evidence of C. difficile infection. Our primary outcome was the impact of preferred regimen antibiotic use on organ space surgical site infection. Secondary outcomes included post-operative complications.
Statistical analysis
All statistical analysis was performed using Stata 17 (College Station; TX: StataCorpLLC). We reported demographic and clinical variables for the total population and then stratified by antibiotic cohort. For continuous variables, we performed bivariate analysis using Wilcoxon rank-sum tests. Fisher exact test and Chi-squared analysis were used for categorical variables. All analyses were performed with significance determined by p-value <0.05. Missing data were supplemented by manual chart review.
We performed logistic regression using “preferred antibiotic regimen” as the key independent variable and each adverse post-operative outcome as the dependent variable. Fully adjusted models included age, gender, race, ethnicity, payor, ASA class, complicated operative findings, and if the operative date occurred post-pathway implementation. A backwards stepwise approach was used to remove non-significant covariates using a significance level of 0.05. This study was approved by the University of North Carolina Institutional Review Board (23-0265).
Results
There were 752 patients ≤18 years old that underwent appendectomy for acute appendicitis between September 2015 and May 2022. The cohorts were stratified into pre- and post-pathway cohorts. There were 346 (46.0%) patients in the pre-pathway cohort and 406 (54.0%) in the post-pathway cohort. Figure 1 shows the percentage of patients receiving the preferred antibiotic regimen across study years. Pre-pathway, the preferred regimen (ceftriaxone/metronidazole or ciprofloxacin/metronidazole) was used in 7.5% of patients versus 87.0% post-pathway (p < 0.001). Of the patients that did not receive the preferred regimen, they most often received piperacillin/tazobactam (85%) or a carbapenem (13%).
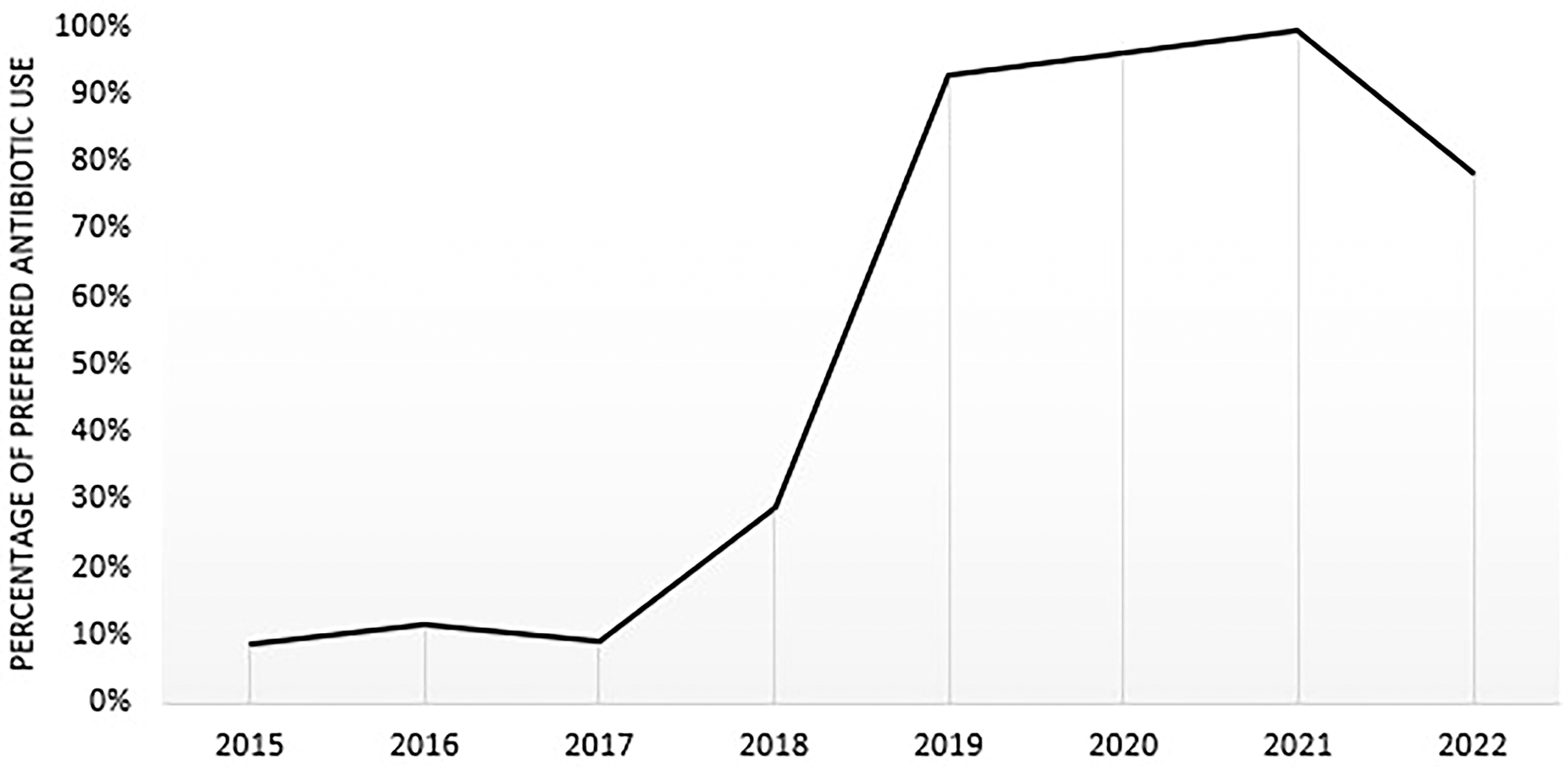
Preferred antibiotic utilization across study years.
The cohorts did not statistically differ in age, gender, race, ethnicity, or payor type (Table 1). There was a higher percentage of patients with complicated appendicitis in the pre-pathway cohort (40.5% vs. 24.3%, p < 0.001).
Demographic and Clinical Factors, Total Population and Stratified by Antibiotic-Type
AIAN = American Indian/Alaska Native, ASA = American Society Anesthesiologists.
There were no statistically significant differences in clinical outcomes between pre- and post-pathway patients, except for a decreased length of stay post-pathway (2 vs. 1 d, p = 0.0001) (Table 2). Length of stay also differed in pre- and post-pathway cohorts when patients were stratified into uncomplicated versus complicated intra-operative findings (Tables 3 and 4). Patients with uncomplicated appendicitis had a shorter length of stay post-pathway; patients with complicated appendicitis had a longer length of stay post-pathway implementation. There were no other outcome differences pre- and post-pathway even when stratified on the basis of complicated operative findings.
Post-Operative Outcomes Stratified by Pre- and Post-Pathway Implementation
SSI = surgical site infection, PICC = peripherally inserted central catheter.
Uncomplicated Appendicitis Post-Operative Outcomes Pre- and Post-Pathway Implementation
SSI = surgical site infection; PICC = peripherally inserted central catheter.
Complicated Appendicitis Post-Operative Outcomes Pre- and Post-Pathway Implementation
SSI = surgical site infection; PICC = peripherally inserted central catheter.
On logistic regression, the use of the preferred antibiotic regimen was associated with a decreased likelihood of post-operative organ space SSI (adjusted odds ratio 0.22, 95% CI: 0.05–0.99) when controlling for demographic and clinical factors (Table 5). The use of the preferred antibiotic regimen did not significantly impact the odds ratio for any other adverse post-operative outcome.
Adjusted Odds Ratios for the Impact of Preferred Regimen Antibiotics on Post-Operative Outcomes
Adjusted for age, gender, race, ethnicity, payor, complicated operative findings, pathway status, ASA score.
SSI = surgical site infection; OR = odds ratio; aOR = adjusted odds ratio; CI = confidence interval.
Discussion
This single-institution, retrospective study included all pediatric appendectomies performed in immunocompetent patients between September 2015 and May 2022 at an academic children’s hospital. In our population, the pre- and post-pathway implementation cohorts had comparable demographics. Pre-pathway patients had higher rates of complicated operative findings and longer lengths of stay. However, adverse post-operative outcome rates were similar pre- and post-pathway. On regression analysis when controlling for demographic and clinical factors—including whether the patient had complicated appendicitis—NSA use was associated with lower odds of post-operative organ space SSI.
Several retrospective studies using multi-hospital databases have found that narrower-spectrum antibiotic use in appendicitis is non-inferior to extended-spectrum agents. Cameron et al. used NSQIP intra-operative findings and length of stay criteria to classify patients with uncomplicated appendicitis and found equivalent outcomes between narrow and extended-spectrum antibiotics. 10 A second multicenter, retrospective trial explored the role of post-operative extended spectrum agents for complicated appendicitis while adjusting for hospital prescribing practices. 11 They found that the rate of intra-abdominal abscess was greater with extended-spectrum agents, but that this effect was mitigated after adjustment for hospitals with high narrow-spectrum antibiotic use. 11
These findings remain contested. Two large studies have found significant differences in post-operative outcomes when comparing narrow- versus extended-spectrum antibiotic use. A multicenter retrospective study by Kronman et al. included uncomplicated and complicated appendicitis patients that underwent appendectomy. The authors found that extended spectrum antibiotic use was associated with higher odds of 30-day readmission and reoperation in patients with complicated, but not uncomplicated, appendicitis. Conversely, the IMPPACT trial, a randomized clinical trial comparing piperacillin/tazobactam (PT) with ceftriaxone/metronidazole in pediatric patients with perforated appendicitis, found that PT use was significantly associated with lower odds of intra-abdominal abscess formation. 7
Even with randomized trial evidence in this population, the IMPPACT group’s findings have not led to new recommendations to use broad spectrum agents in this population. 12 In addition to concerns about antibiotic resistance, the argument against use of broad-spectrum antibiotics in appendicitis suggests that the majority of organisms that are associated with appendicitis are covered by narrow-spectrum antibiotics. 13 Second, unnecessary broad-spectrum coverage may result in a disruption in immune response and healing. Previous research has shown that any level of exposure to antibiotics has been linked to gut microbiome dysbiosis. In a study of adult treatment-naïve Crohn, patients, Gevers et al. found that exposure to antibiotics significantly increased dysbiosis. 14 A study of pre-school children performed by Palleja et al. supports these findings and demonstrated significant long-lasting changes to intestinal microbiome composition and metabolism after antibiotic exposure. 15
Despite efforts to standardize clinical presentation definitions, there is still significant variation in antibiotic selection, even within hospital systems.6,7,16 Additionally, many existing studies that explore outcomes with extended versus narrow-spectrum antibiotic use in appendicitis use large databases that rely on use of subjective inclusion and exclusion criteria. Our study uses an institutional pharmacy database to determine the type and dosing of antibiotics for each patient encounter. This methodology allows for nuanced cohort assignment where we could note any extended-spectrum exposure over the entire course of hospitalization, rather than inference using a cut-off date. Additionally, we used the presence of specific NSQIP-defined intra-operative findings to determine whether a case was uncomplicated or complicated.
One limitation of our study is that uses a single institution database. Therefore, antibiotic administration or post-operative complications seen at care facilities outside our system for wound complication or admission may not be captured in the medical record. We would not have access to this data and these complications may not have been captured. Second, we did not collect final pathology data to confirm whether patients had appendicitis. Our antibiotic pathway includes a scoring system for stratification that has been shown at other institutions to decrease the negative appendectomy rate to <2%, so there is likely a very small portion of patients that had negative appendectomies. 13
We noted a longer LOS in patients after the transition to our clinical pathway, and in spite of fewer infections after implementation, an increase in LOS was identified. We examined patients to identify an explanation for longer length of stay, but it was unclear why LOS increased, which is one of the limitations of this study and other similar, non-randomized retrospective studies. This finding does not appear to be associated with changes in clinical care as discharge criteria, laparoscopic versus open approach, and ASA were similar between the two cohorts. Additionally, the incidence of complicated appendicitis was higher and even after subgroup analysis an explanation for this difference was not identified. On review of the data and multi-disciplinary discussion, it did not appear to be related to antibiotic selection and we continue to use the same antibiotics examined in this article at our institution.
Finally, we did not examine total antibiotic course, including oral antibiotics prescribed on discharge. We hypothesize this has minimal effect on our findings, as our institutional practice is to complete a 7-day total post-operative antibiotic course for complicated appendicitis, a practice that did not change after narrow-spectrum pathway implementation. Some studies have demonstrated that oral antibiotic use even in complicated appendicitis does not impact post-operative morbidity. 17
In our population, antibiotic stewardship through use of a standardized, preferred antibiotic regimen was associated with decreased odds of deep organ space SSI after adjusting for clinical factors and operative findings. Despite randomized clinical trial evidence, center-specific recommendations and antibiotic stewardship should include robust tracking of institutional outcomes, as most-effective regimens may differ between populations and geography. In addition to concerns of antimicrobial resistance, minimizing the use of extended-spectrum antibiotics in pediatric appendicitis may have benefits at the individual patient level.
Footnotes
Authors’ Contributions
U.A.: Conceptualization, methodology, formal analysis, data curation, writing-original draft, writing-review & editing. N.K.: Conceptualization, methodology, data curation, writing-review & editing. W.W.: Conceptualization, methodology, data curation, writing-review & editing. Z.W.: Writing-original draft, writing-review & editing. A.E.: Writing-original draft, writing-review & editing. M.D.: Software, validation, data curation. A.A.: Writing-original draft, writing-review & editing. S.M.: Writing-original draft, writing-review & editing. A.C.: Writing-original draft, writing-review & editing. M.P.: Conceptualization, methodology, formal analysis, data curation, writing-original draft, writing-review & editing, supervision.
Author Disclosure Statement
The authors have no competing interests to declare. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Funding Information
The authors have no funding to report associated with this study or the preparation of the article.