
Abstract
Background:
Most studies on surgical site infections (SSIs) use the US Centers for Disease Control and Prevention (CDC) guidelines, which excludes inflammation or cellulitis without fever. The aim of this study was to evaluate antibiotic prescription trends in the post-operative period among patients undergoing breast operation. We explore the outcomes of patients receiving antibiotic agents outside of the CDC-defined SSI.
Patients and Methods:
A retrospective review of patients undergoing breast operation from January 2021 to May 2021 was conducted. Solely reconstructive and cosmetic cases were excluded. The primary outcome was the prevalence of antibiotic prescription in the absence of CDC-defined SSI, excluding routine prophylactic antibiotic agents, with analysis of associated factors.
Results:
A total of 754 breast surgical procedures were included. Seventy-seven patients (10.2%) were prescribed outpatient antibiotic agents. CDC-defined SSI occurred in 5.3% (n = 40), mostly involving tissue expander/implant-based reconstruction (47.5%, n = 19). However, 37 (4.9%) did not progress to meet the CDC criteria for SSI.
Patients prescribed outpatient antibiotic agents without CDC-defined SSI did not have increased rates of diabetes mellitus, obesity, or current smoking. These patients were more likely to have a surgical drain (48.6% vs. 28.4%, p = 0.02), plastic surgery involvement (32.4% vs. 18.0%, p = 0.048), and a post-operative seroma (32.4% vs. 8.1%, p < 0.001) and or or cellulitis (18.9% vs. 0%, p < 0.001).
Conclusion:
Patients are prescribed antibiotic agents after breast operation based on clinical judgment for indications other than CDC-defined SSI. Post-operative wound morbidity including seroma and cellulitis could be contributing to these antibiotic prescriptions. Further study is needed to determine whether providers are preemptively treating SSIs appropriately or over-treating non-infectious wound complications.
Surgical site infection (SSI) represents a known complication after breast operation, which can lead to prolonged hospitalization, poor patient satisfaction, need for reoperation, delay in adjuvant therapies, and increased cost. However, when investigating and reporting SSIs after breast operation, differing definitions used can result in wide variation in observed infection rates ranging from 2% to 19%.1–5 The American Society of Breast Surgeons Consensus Guideline on Preoperative Antibiotics and Surgical Site Infection in Breast Surgery recommends that standardized definitions be employed when SSIs are used as a quality measure but does not endorse a specific definition. 6
The US Centers for Disease Control and Prevention (CDC) outlines a definition for hospitals to use when monitoring post-operative SSIs, 7 and most studies exploring SSIs after breast operation use this definition. Notably, cellulitis alone at the incision (redness, warmth, swelling) is specifically not considered a superficial incisional SSI, and additional CDC guidance for breast infections notes that prescription of antibiotic agents for inflammation or cellulitis in the absence of fever is also not considered an SSI. 7 Given these specific exclusions might be missed in quality monitoring and research, our aim in this study was to evaluate antibiotic prescription trends during the post-operative period after breast operation. Moreover, we aimed to correlate between antibiotic prescription and CDC-defined SSI. We hypothesize that antibiotic prescription outside of CDC-defined SSI criteria might decrease wound complications.
Patients and Methods
After approval from the Institutional Review Board, a cohort of patients undergoing breast operation from January to May 2021 were obtained from an institutional operative database. Inclusion criteria were all adult patients undergoing operation involving resection of breast tissue or axillary lymph nodes at a combination of quaternary and community regional hospitals within the same hospital system and included operations performed by both fellowship-trained breast surgeons and community general surgeons. Also included were breast reconstruction cases performed at the time of breast resection, but solely reconstructive and cosmetic breast operations were excluded.
The medical record was then reviewed for patient demographics, comorbidities, intra-operative details, post-operative CDC-defined SSI, antibiotic agents prescribed during the peri-operative period and reason for prescription, and other wound-related complications including cellulitis, seroma, hematoma, and re-operation. Details to classify infection and other wound-related complications after operation were obtained from provider documentation in post-operative clinic/hospital notes.
The CDC categorizes SSIs by depth (superficial, deep, and organ/space), gives criteria which constitute SSI, and provides additional guidance for specific surgical procedures. Per the 2021 CDC surveillance guidelines for breast operation, superficial infections were recorded within 30 days of the index surgical operation, deeper infections within 90 days, and if a tissue expander or implant was placed then infections were monitored within 1 year of placement. These definitions and time periods were used in this study to categorize and record SSIs. Specific definitions can be found on the CDC website in the Patient Safety Component of the National Healthcare Safety Network. 7
The primary outcome was antibiotic prescription for wound-related concerns in the post-operative period. This excluded prophylactic antibiotic agents for implant/tissue expander placement or indwelling surgical drains. Descriptive statistics were used to provide basic information about the patient cohort and highlight potential relationships between collected variables. Data were analyzed to determine the rate of antibiotic prescription in the absence of CDC-defined SSI, with uni-variable analysis to identify factors associated with this outcome, where a p value of ≤ 0.05 was considered statistically significant. For uni-variable analysis, patients with a diagnosed CDC-defined SSI were excluded as predictors of breast infection after operation have been defined, and antibiotic treatment for infection is assumed. Data analysis was performed using R statistical programming software (R Foundation for Statistical Computing, Vienna, Austria). 8
Results
A total of 754 breast surgical procedures were included. Of these, 35% (n = 266) were for benign breast disease and 65% (n = 488) for malignant disease. Most patients underwent excisional biopsy or a partial mastectomy, with a majority not requiring lymph node excision (Table 1). Of the procedures performed for breast cancer, 48.9% (n = 239) included breast conservation without reconstruction, whereas 21.7% (n = 106) were mastectomy with reconstruction (tissue expander or direct to implant) (Table 2).
Demographic and Pre-Operative Variables of Patient Cohort with Uni-Variable Comparison of Patients Who Received Post-Operative Antibiotics for a Wound Concern to Patients Who Did Not Receive Antibiotic Agents for a Wound-Related Concern
Patients with post-operative surgical site infection excluded.
SD = standard deviation; COPD = chronic obstructive pulmonary disease; ASA = American Society of Anesthesiologists.
Operative Variables of Patient Cohort with Uni-Variable Comparison of Patients Who Received Post-Operative Antibiotic Agents for a Wound Concern to Patients Who Did Not Receive Antibiotic Agents for a Wound Related Concern
Patients with post-operative surgical site infection excluded.
SLNB = sentinel lymph node biopsy; ALND = axillary lymph node dissection; PVP = povidone.
The rate of CDC-defined SSI in the overall cohort was 5.3% (n = 40), with a majority of those in cases with tissue expander or implant-based reconstruction (47.5%, n = 19). A total of 77 patients (10.2%) were prescribed antibiotic agents during outpatient follow-up. Among those, 26 (34%) had antibiotic agents prescribed at the time of CDC SSI diagnosis, 14 (18%) were diagnosed with a CDC SSI ≥1 day later, and 37 (48%) did not progress to meet the CDC criteria for SSI (Fig. 1). Most common documented reasons for antibiotic prescription in the absence of CDC-defined SSI included erythema only (n = 13, 35.1%), wound healing issues (n = 9, 24.3%), and cellulitis (n = 7, 18.9%) (Supplementary Fig. S1).
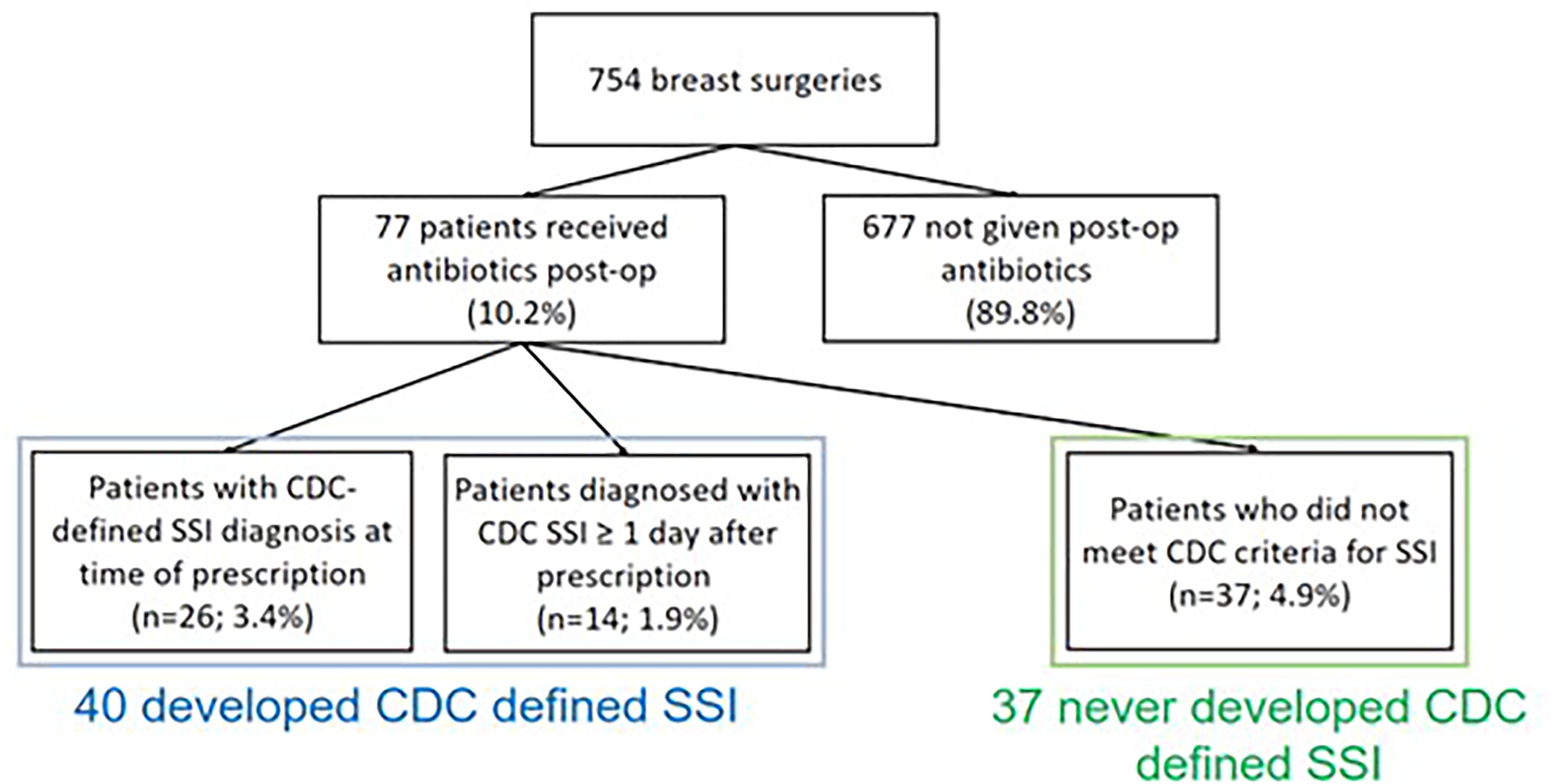
Breakdown of patient cohort by post-operative antibiotic prescription for wound-related concern and the US Centers for Disease Control and Prevention-defined surgical site infection.
After excluding patients with a CDC-defined SSI, patients who were prescribed antibiotic agents did not have increased rates of variables traditionally associated with infection such as presence of diabetes mellitus, greater body mass index, or current smoking (Table 1). Patients prescribed antibiotic agents were more likely to have a surgical drain (48.6% vs. 28.4%, p = 0.02), to have had a plastic surgeon involved in their care (32.4% vs. 18.0%, p = 0.048), and trended toward greater rates of mastectomy with reconstruction (24.3% vs. 14.0%, p = 0.09) compared with those not prescribed outpatient antibiotic agents (Table 2).
Patients prescribed antibiotic agents were also more likely to have been diagnosed with a post-operative seroma (32.4% vs. 8.1%, p < 0.001) and cellulitis (18.9% vs. 0%, p < 0.001) compared with those not prescribed outpatient antibiotic agents (Table 3). Re-operation for wound-related concerns was greater among those prescribed outpatient antibiotic agents at 13.5% (5/37, for debridement of non-healing non-infected tissue, all occurred after antibiotic prescription) compared with 0.7% for those not prescribed outpatient antibiotic agents (5/677, for drainage of delayed hematomas/seromas, p < 0.001).
Post-Operative Variables of Patient Cohort with Uni-variable Comparison of Patients Who Received Post-Operative Antibiotic Agents for a Wound Concern to Patients Who Did Not Receive Antibiotic Agents for a Wound Related Concern
Patients with post‐operative surgical site infection excluded.
Discussion
In our study of 754 breast surgical procedures, we found that 10% of patients are prescribed non-prophylactic antibiotic agents during post-surgical follow-up, but only a portion of these were for a SSI as defined by the CDC. Erythema alone at the surgical site was the most common reason for antibiotic prescription, followed by wound healing issues and cellulitis. Even without developing an SSI, patients prescribed antibiotic agents experienced greater rates of re-operation for wound-related concerns (13.5% vs. 0.7%) than those not prescribed antibiotic agents.
Antibiotic use in patients undergoing breast operation has been extensively explored in medical literature. Investigations have centered around the pre-operative period including intravenous doses prior to incision,9–13 intra-operative including antibiotic irrigation for implants,14,15 as well as post-operative prophylactic antibiotic agents both before16,17 and after 18 hospital discharge and prophylaxis specifically for indwelling surgical drains.19,20 Still, many studies report conflicting results, strong evidence is lacking, 13 and randomized trials are ongoing. 21 Notably, all of these investigations surround prescription of prophylactic antibiotic agents to prevent infection.
To our knowledge, this is the first investigation exploring non-prophylactic antibiotic prescription in the post-operative period after breast operation. This is likely because other studies focus on the outcome of SSI, possibly assuming that antibiotic prescription outside of prophylaxis is only used in the treatment of an SSI when it is found. Our study shows this may not be the case, and that for every patient prescribed antibiotic agents to treat a CDC-defined SSI, there was another treated with antibiotic agents who did not develop a CDC-defined SSI. Moreover, the patients who later on met the criteria could represent treatment failure whereas the patients who never met the criteria could represent treatment success.
Practitioners documented multiple reasons for prescribing an antibiotic, which ranged from only erythema near the surgical site to evidence of cellulitis including warmth, swelling, and redness. In addition to the physical exam findings which prompted the prescription, our study explored other factors that could have influenced practitioners to prescribe antibiotic agents outside of the CDC-defined infection. We did not find that patient characteristics traditionally associated with SSI were also associated with antibiotic prescription such as diabetes mellitus, smoking, pre-operative immunosuppression, or chronic obstructive pulmonary disorder,4,22 which could have suggested that practitioners were prescribing antibiotic agents to patients at greater risk for infection. We did find that this group had a greater incidence of wound complications including seroma and cellulitis (some of which prompted the antibiotic prescription). Additionally, a greater rate of re-operation for wound-related concerns shows that antibiotic prescribers identified a greater-risk group not captured by the CDC SSI definition.
The ultimate effect of antibiotic prescription in this population is still unknown. Antibiotic prescriptions could treat early infections, which do not yet meet the CDC criteria for SSI. Evidence in favor of this option includes the fact that a portion of our patients received antibiotic agents to treat cellulitis. In theory, the antibiotic agents could resolve the local infection around the incision before further progression. Another option is that antibiotic prescription in the absence of CDC-defined SSI constitutes over-treatment. Some of our patients were prescribed antibiotic agents with only erythema near the incision or a documented seroma. With erythema as the only sign, it is difficult to distinguish infection from non-infectious inflammatory processes, and although seromas can present a nidus for infection, there is no recommendation for antibiotic prescription unless the seroma becomes infected. 23 Antibiotic treatment is not without risks, 24 and thus proper stewardship is imperative. However, it is likely both early treatment and over-treatment are occurring in this population. A study by Landes et al. showed that antibiotic over-prescription was present in 27.5% of breast procedures performed by plastic surgeons. 25
The other issue may lie with the CDC definition of SSI. Cellulitis, which is most commonly caused by gram-positive bacteria including β hemolytic streptococcus and methicillin-sensitive Staphylococcus aureus, is considered an infection of the deep dermis and subcutaneous tissues. 26 Others have shown that cellulitis accounts for a large portion of wound morbidity after breast operation. 27 and that the exclusion of cellulitis starting with the 2010 CDC definition reduces the SSI rate by a factor of 3. 28 We confirmed that excluding cellulitis misses patients who in our study were all treated with antibiotic agents, which is not only clinically appropriate but may have prevented some of those infections from progressing to meet the CDC criteria for SSI. Others have also shown that restrictions in the 2020 CDC definition of SSI regarding time from operation to diagnosis and additional procedures after operation restricting diagnosis misses clinically relevant infections after breast operation. 29 This matters because most studies that explore SSIs after breast operation use the CDC definition, and national databases such as the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) also use it to track SSI rates after surgical procedures.
There are limitations to this study which deserve mention. With breast operations considered clean cases, rates of infection are generally low. Even with a cohort of 754 individual operations, there were still only 39 infections, with rates of antibiotic prescription in the absence of SSI similarly low. As such, multi-variable analysis could not be performed to identify factors independently associated with antibiotic prescription in the absence of SSI. Larger studies are needed to better understand national trends in antibiotic prescription after breast operation, and their role in infection prevention versus over-treatment. Additionally, this is a retrospective study which carries with it the limitations of retrospective data. Specifically, outcomes such as infection and wound complications are only captured with accurate documentation in the medical record, and recent research has shown that the electronic medical record can frequently miss variables if there is not adequate documentation. 30
We showed that patients who are prescribed antibiotic agents during follow-up after breast operation do not always meet the criteria for SSI according to the CDC but are at greater risk of wound morbidity. This represents a gray zone in the post-surgical treatment of breast disease that deserves further investigation. To do this, future research needs to clearly define SII, and if using the CDC definition, needs to also report rates of cellulitis and post-operative antibiotic prescriptions. The ACS NSQIP should add these variables for collection in patients who undergo breast operation so that national trends in early infection and antibiotic prescription can be explored.
Footnotes
Authors’ Contributions
Study conception and design: C.K.G., K.N., and Z.A. Data acquisition and analysis: C.K.G., M.M., J.H.C., H.H., K.W., K.N., and S.A.S. Drafting of the article: C.K.G., M.M., J.H.C., and H.H. Critical revision: All authors.
Data Sharing
Owing to the nature of the research, for ethical and legal restrictions, supporting data are not available.
Author Disclosure Statement
There are no conflicts of interest to report in any of the authors and no external sources of funding for this research.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.