
Abstract
A 27-year-old female underwent bilateral mastectomy with left axillary dissection and had immediate breast reconstruction with textured silicone implants and acellular dermal graft (ADG) reinforcement of the inferior quadrants. The patient was maintained on oral antibiotics postoperatively and initially did well. However, she subsequently presented with fever, erythema, and tenderness in the left chest and was admitted for intravenous antibiotic therapy. Despite improvement of her symptoms, she ultimately cultured positive for Staphylococcus aureus and had the tissue expander and the ADG material explanted. These explanted specimens were immediately examined with confocal microscopy using Live/Dead staining under hydrated conditions for the presence of bacterial biofilms. Biofilm bacteria were clearly visualized adherent to both the tissue expander shell and also to the ADG surface. This is the first direct demonstration of viable bacteria in biofilm configuration on the surface of a tissue expander and acellular dermal graft after breast reconstruction.
Clinical History
A 27-year-old female was diagnosed with T3N2aM0 invasive ductal carcinoma of the left breast. She underwent induction chemotherapy followed by bilateral total mastectomy with left axillary node dissection. She had immediate bilateral breast reconstruction using 350 cc textured silicone tissue expanders with acellular dermal graft (ADG) reinforcement in the inferior quadrants. The expanders were filled to 140 cc volume, and two Jackson-Pratt drains were placed on either side. She was discharged on postoperative day two on oral Duricef.
On postoperative day six the patient noted pain and redness at her left inferior drain site. She was found to have an ∼1.5 cm area of localized erythema at the drain site only, no fluctuance, no fever, and the drainage remained serosanguineous. She was empirically switched to ciprofloxacin. Two days later the inferior drain was removed, and the erythema surrounding the drain site was markedly improved. Five days later she was asymptomatic, with no signs of infection in the left breast. The second left-sided drain was left in place due to continued serosanguineous output.
Nine days later (postoperative day 22) the patient presented with pain and tenderness in the left breast. She was afebrile but was noted to have some left breast erythema. The patient was started again on oral Duricef, having completed her course of ciprofloxacin. However, later that same day, the patient presented to the Emergency Room with fever to 39.1°C. She was again noted to have blanching erythema of the left breast, with some induration and tenderness to palpation, but no fluctuance. White blood cells were measured at 6,400, with 79% neutrophils on differential. Blood cultures were taken (which ultimately showed no growth). The patient was admitted for intravenous antibiotic therapy with vancomycin.
Three days later (postoperative day 25), the patient’s clinical symptoms and signs had all improved substantially, but she had cloudy drainage from her remaining left sided drain. Cultures from this material were positive for Staphylococcus aureus. The patient was therefore returned to the operating room for explantation of her prosthesis. Intraoperatively, the patient was noted to have turbid fluid between the ADG and the implant. An exuberant response of granulation tissue was also noted in the infected pocket, but there was no vascularization or incorporation of the ADG at all. The expander prosthesis, as well as all suture material and the ADG, were removed and the field irrigated with bacitracin. Fresh Jackson-Pratt drains were placed, and the wound closed.
Postoperatively, the patient was maintained on oral Bactrim for seven days. She experienced no complications, and her wound healed uneventfully. She subsequently underwent successful delayed left breast reconstruction with tissue expansion and placement of a prosthesis (but without ADG). The immediate right breast reconstruction was successful and never demonstrated any evidence of infection.
Confocal Laser Scanning Microscopy and Viability Staining
Immediately after the explantation, clinical residual material (in approx. 1 cm2 pieces) was taken from the expander and the ADG and transported in a humidified sterile specimen container to the research microscopy lab. The specimens were placed in a 60 mm polystyrene Petri dish and anchored to the base by placing gently with tweezers on a few drops of cooled molten low temperature agar. We stained the specimens with the DNA-specific BacLight Live/Dead kit (Molecular Probes, Eugene, Oregon, USA) by drop pipetting as previously described. 1 This stain has two components: SYTO9, which stains live cells green, and propidium iodide, which stains dead cells red. The specimen was examined in transmission and confocal mode using either a 10X air objective or a 63X long working distance water immersion objective. This procedure avoided dehydration. We visualized the expander material using transmitted light (grey) and the ADG was visualized by red autofluorescence.
Results
As seen in Figure 1A, the square cell texturing of the expander was clearly evident by low power microscopy and patches of green fluorescence on the surface and along some of the edges of the squares indicated the presence of biofilm. Higher magnification revealed that the biofilm consisted of clusters of live cocci (Fig. 1B), consistent with the clinical culture of S. aureus from this patient. Diffuse green staining surrounding individual cells and clusters of cells was indicative of extracellular DNA, which is a known component of staphylococcal biofilms. 2 A high density biofilm with numerous clusters of live cocci was also found on the surface and within the matrix of the ADG (Fig. 2). We estimated the density of viable bacteria was approximately 8,000 live cells/clusters per mm2 of projected area of ADG.
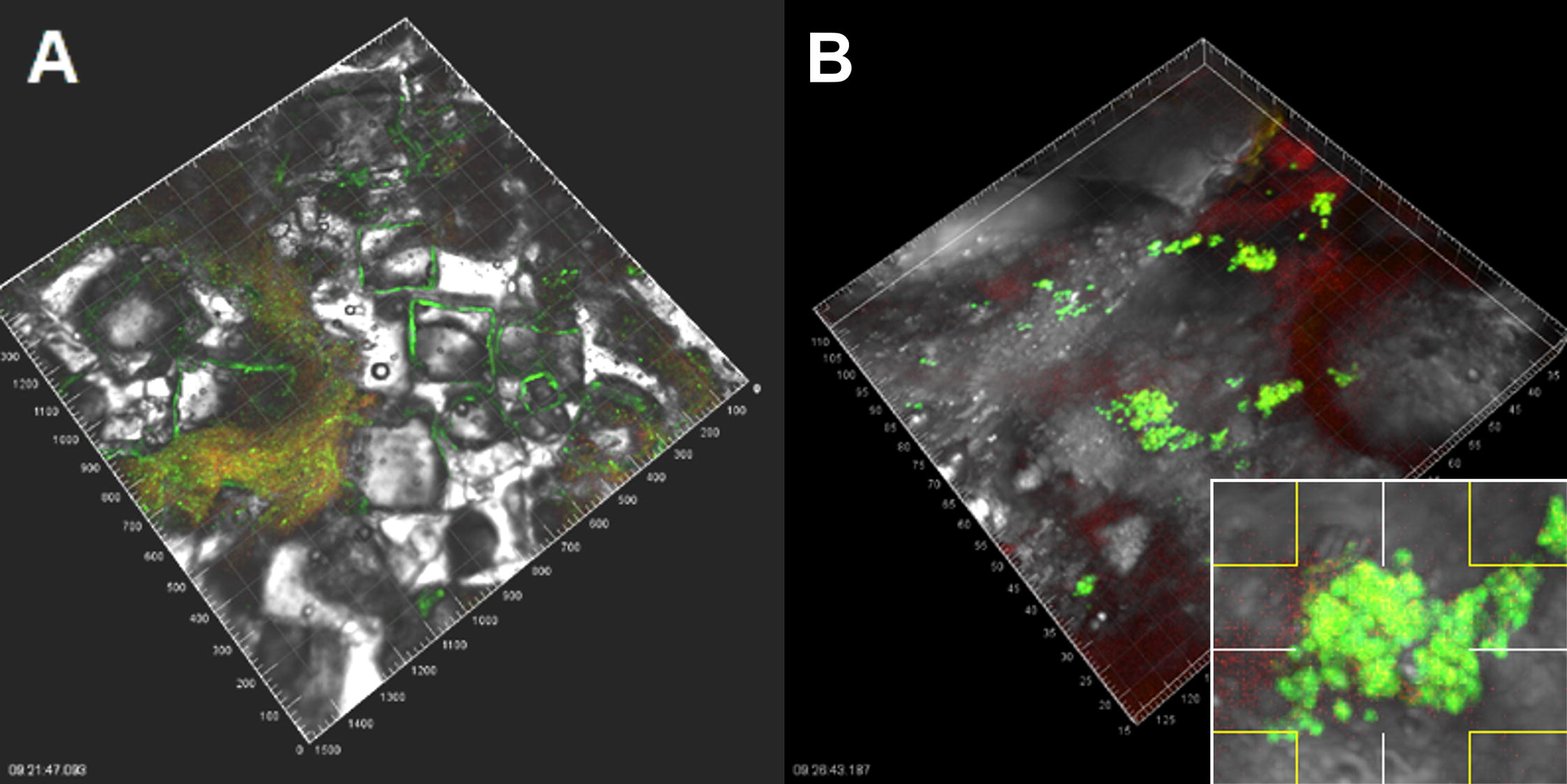
Patches of biofilm attached to the textured surface of the expander.

Clusters and single cells of live cocci (stained green) growing on, and within, the acellular dermal graft (autofluorescing red). Inset is a high magnification image showing cocci in a representative cluster.
Discussion
Infection of a tissue expander for breast reconstruction is a known complication with an incidence reported up to 24%. 3 Independent risk factors for postoperative infection that were present in this patient include immediate reconstruction after mastectomy, axillary lymph node dissection, use of surgical drains, and use of acellular dermal grafts. With these clinical risks in mind, the patient was maintained on prophylactic antibiotics for a total of 16 days postoperatively, but still developed an active infection that presented unequivocally on postoperative day 22. It is impossible to know for certain when the infecting bacteria were introduced, but most postoperative infections of implanted materials are thought to arise from bacterial inoculation at the time of implantation.
Bacterial biofilms are communities of bacteria residing within an extracellular polymeric substance matrix on an implant or tissue surface. Bacteria in biofilm configuration behave notably differently from their planktonic counterparts in several ways: they are often recalcitrant to culture by standard microbiological methods, they are resistant to host defense mechanisms, and they are insensitive to standard antibiotic therapy even if lacking a genetic mechanism for antibiotic resistance. The bacteria observed in this patient were clearly viable despite six days of Duricef, a full course of ciprofloxacin, and three days of intravenous vancomycin, consistent with the properties of a biofilm. The biofilm paradigm likely explains the development and persistence of a frank infection in this patient despite extensive postoperative antibiotics. In this case a successful culture of the causative organism (S. aureus) was ultimately obtained, although in many biofilm infections culture results may remain negative.
Biofilms have been suggested to contribute to a number of pathologies associated with breast implants, including capsular contracture 4 and the development of breast implant-associated anaplastic large cell lymphoma, 5 but to date a viable biofilm on a breast prosthesis has never been directly demonstrated. Previous studies have imputed the existence of breast-implant associated biofilms either from image analysis of electron micrographs of explants (which have been processed and fixed) or from sonication studies, wherein bacteria grown in standard microbiological culture are presumed to have derived from a surface-adherent biofilm after sonication-assisted dissociation of explanted specimens. For example, Danino et al. 6 found spherical objects at capsular interfaces by electron micrography that they identified as biofilm bacteria despite negative cultures in all instances. By comparison, Rieger et al. 7 used sonication and culture to identify bacteria in capsular specimens after implant exchange. They found positive cultures in 28% of specimens from aesthetic implant capsules and in 44% of specimens from reconstructive implant capsules after mastectomy. The only study that appears to have specifically attempted to identify living biofilms on explanted breast prostheses and capsules was undertaken by Poppler et al. 8 They found no evidence of living biofilms in five specimens examined by Live/Dead staining; electron micrography also showed structures consistent with biofilm in only one out of 26 specimens examined.
This study is therefore the first to directly visualize biofilm bacteria resident on both an explanted tissue expander surface and on explanted ADG used in breast reconstruction. The latter observation is particularly interesting in that it may provide some explanation for why the use of ADG is a risk factor for postoperative infection. When ADG is used in breast reconstruction, it interposes a functionally avascular tissue surface between the avascular surface of the expander and the vascularized surface of the mastectomy skin flap. This creates a potential space between two avascular surfaces that would likely be an attractive place for bacteria to establish and form biofilms, heightening the risk of infection. Unfortunately, once formed, there remains to date no reliable way to address biofilm infection absent the complete removal of the compromised implanted material, as was done here.
Footnotes
Acknowledgments
The authors acknowledge the assistance of Dr. Sandeep Kathju in the preparation of this article.
Authors’ Contributions
A.K. investigated and assembled the clinical history; L.N. and P.S. carried out the confocal micrography; A.K. and P.S. wrote the initial draft of the article; all authors approved the final draft.
Author Disclosure Statement
The authors have no conflicts of interest to report.
Funding Information
The authors have no funding source to acknowledge.