
Abstract

To the Editor:
Fish bone foreign bodies are common foreign bodies in the upper gastrointestinal tract. It is rare for fish bones to pass through the wall of the esophagus and be embedded in the thyroid parenchyma. Here, we report a case of a fish bone embedded in the thyroid gland, and one end of the bone scratched the wall of the common carotid artery.
A 38 years old female, had throat pain and discomfort after swallowing fish bones by mistake, and she attempted to swallow the fish bone by swallowing rice balls. The pain in the throat decreased after swallowing the rice ball, but the sensation of a foreign body in the throat persisted. The patient was immediately referred to a local hospital, where a fiberoptic laryngoscope showed a scratch in the esophagus and no fish bones were found. One day later, the pain in the neck and throat on the right side of the pharynx worsened, accompanied by burning pain in the neck and traction pain in the ear. The patient then presented to our hospital. CT of the neck showed a dense shadow in the upper esophagus approximately level C7, penetrating the right lateral wall and involving the right lobe of the thyroid gland, with one end adjacent to the common carotid artery (Fig. 1). Ultrasound of the neck revealed a 2.45-cm strip of enhanced echo in the parenchyma of the lower right lobe of the thyroid gland, which was inserted diagonally from the right lateral wall of the esophagus into the right lobe of the thyroid gland and ended close to the wall of the right common carotid artery (Fig. 2). Routine blood test showed WBC 14.04 × 109/L, NEU 11.54 × 109/L, NEU-R 82.2%. The patient underwent cervical foreign body exploration through lateral neck incision. A foreign body was detected in the lower pole of the right thyroid lobe. The foreign body was a fish bone about 3 cm in length. There was a little bleeding in the lower pole of the thyroid gland, and no purulent secretion was observed. The wall of the right common carotid artery was scratched by a sharp object, the scratch was superficial, and the artery wall was intact. There was no obvious oozing or active bleeding. The carotid artery pulse was good, and no palpable tremor was found. Exploration revealed that the common carotid artery did not require special treatment. A negative pressure drainage tube was placed in the neck to keep the drainage unobstructed. The patient was treated with intravenous ceftazidime and levofloxacin to prevent infection and abscess formation. Postoperative neck CT showed uneven density in the right lobe of the thyroid gland, and there was no evidence of pseudoaneurysm in the right carotid artery.
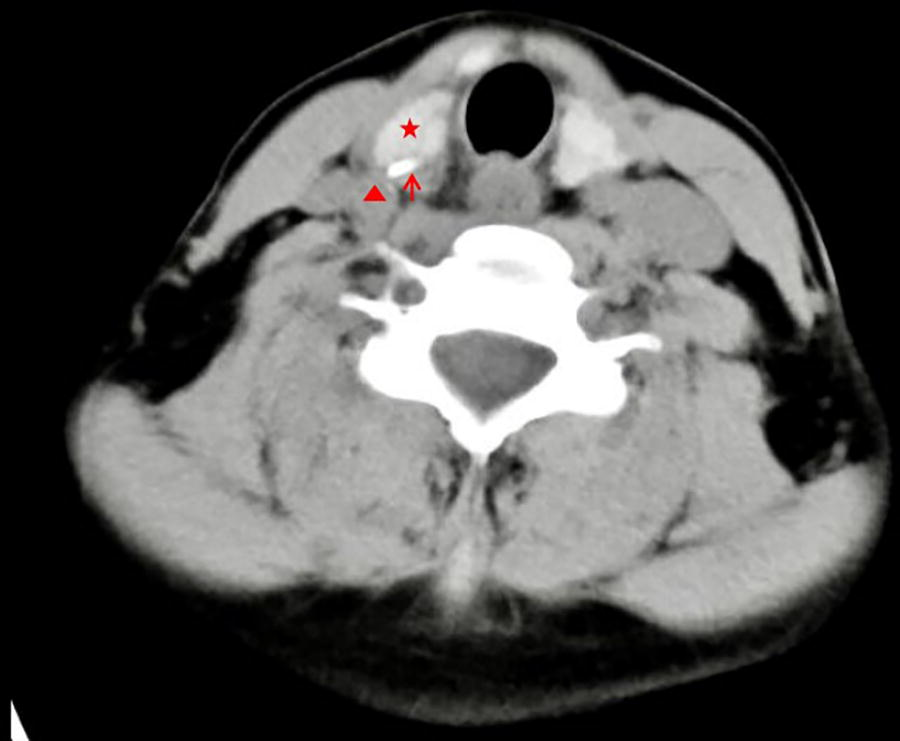
Neck CT: There was a dense shadow (arrow) in the upper esophagus approximately level C7, penetrating the right lateral wall and involving the right lobe of the thyroid gland (pentagram), with one end adjacent to the common carotid artery (triangle).

Neck Ultrasound: There was a strip-shaped enhanced echo (arrow) with a length of 2.5 cm in the lower parenchyma of the right lobe of the thyroid gland (pentagram), and its tip was close to the wall of the right common carotid artery (triangle).
Fish bone foreign bodies are often embedded in palatine tonsil, epiglottis creek, pyriform fossa, esophagus, etc. A few fish bones may penetrate the esophageal wall into the neck soft tissue, thyroid, and even injure the carotid artery.1–2 Pain and foreign body sensation occurred in the posterior pharyngeal wall after entrapment of the fish bone. Rough swallowing of rice balls and the frequent movement of local muscles during normal eating and speaking may lead to the migration of fish bones through the esophageal wall and the soft tissue around the esophagus, and the pain and other symptoms may be relieved. At this point, laryngoscope or gastroscope cannot detect the fish bones that have entered the surrounding soft tissue. Ultrasound and CT can clearly show the size, shape, position of the fish bone, and the relationship between the fish bone and the surrounding soft tissue, which can complement each other. Because of the bony structure and gas interference, it is difficult to show the retropharyngeal space and the foreign body behind the sternum by ultrasound, but CT can clearly show it. CT scan planes only include transverse, coronal and sagittal views, which is generally difficult to display the foreign body completely in one plane. Ultrasound can display any plane centered on the foreign body, and ultrasound has the characteristics of strong repeatability and real-time, which is helpful for preoperative and intraoperative localization of the foreign body in the neck, and provides a basis for surgeons to choose surgical methods. Ultrasound has no radiation, so it is also suitable for children. Fish bones with bacteria and the wound left by fish bones through the esophagus may lead to axillary infection in the neck and mediastinum. Therefore, it is necessary to keep the drainage unblocked by negative pressure drainage tube, indwelling gastric tube and the use of antibiotics after operation. For patients with suspected foreign bodies such as fish bones, esophagoscopy or gastroscopy should be performed to remove the foreign bodies. If no foreign body was found by esophagoscopy, and the foreign body was considered to have penetrated the esophagus into the tissue space, neck CT and neck ultrasound were performed to determine whether there was a foreign body and the relationship between the foreign body and the surrounding tissue,3–4 Lateral neck incision or thoracotomy was performed to remove the foreign body.
Ethics Approval and Consent to Participate
Informed consent from patients was obtained for this study, and their anonymous information will be published in this article.
Footnotes
Author Disclosure Statement
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
No funding was received for this article.