
Abstract
Background:
Hydatid cysts, caused by Echinococcus granulosus, are uncommon in the breast but are observed in endemic regions of the Eastern Mediterranean. This study evaluates the diagnosis and treatment of this rare occurrence of breast hydatid cyst and its spontaneous rupture.
Case Presentation:
A 33-year-old female patient presented to our clinic with a mass in the right breast that had been growing for 9 months and causing intermittent pain. Physical examination revealed a well-defined, firm mass with regular borders and some soft areas. Ultrasonography reported a complicated cyst(?). While awaiting the report of breast magnetic resonance imaging, the patient returned to the hospital because of the discharge of white material from the breast. Examination revealed a laminar membrane from the perforated area. Under sedation, the cyst was evacuated, vesicles were removed, and the cyst cavity was irrigated with 3% saline for drainage.
Conclusions:
Although breast hydatid cyst is rare, it should be considered in the differential diagnosis, especially in endemic regions. Magnetic resonance imaging and drainage, combined with prophylactic albendazole, represent a safe and effective diagnostic and treatment approach.
Hydatid cyst is a parasitic disease caused by Echinococcus granulosus and is commonly observed in our region. 1 These cysts most frequently occur in the liver but can rarely be found in the breast with an incidence rate of 0.27%. 2 Despite its rare occurrence in the breast, this condition should be taken seriously as it can mimic both benign and malignant diseases. Radiologic imaging methods are used for diagnosis, and in most cases, a definitive diagnosis is made through histologic examination following operation. 3 In our case, the diagnosis was easily established before operation by the detection of spontaneous rupture of the cyst and the characteristic laminar membrane, which is pathognomonic.
Case Description
A 33-year-old female patient from an endemic region of hydatid cysts presented with a progressively increasing swelling and pain in the right breast for more than 9 months. On physical examination, a well-defined, firm mass with occasional soft areas and regular borders was palpated 4 cm away from the nipple at the 7 o’clock position of the right breast. There weren’t overlying skin changes, erythema, induration, fluctuance, or nipple abnormalities. Pathology was not detected upon palpation of the left breast or both axillae, and adenopathy was not noted.
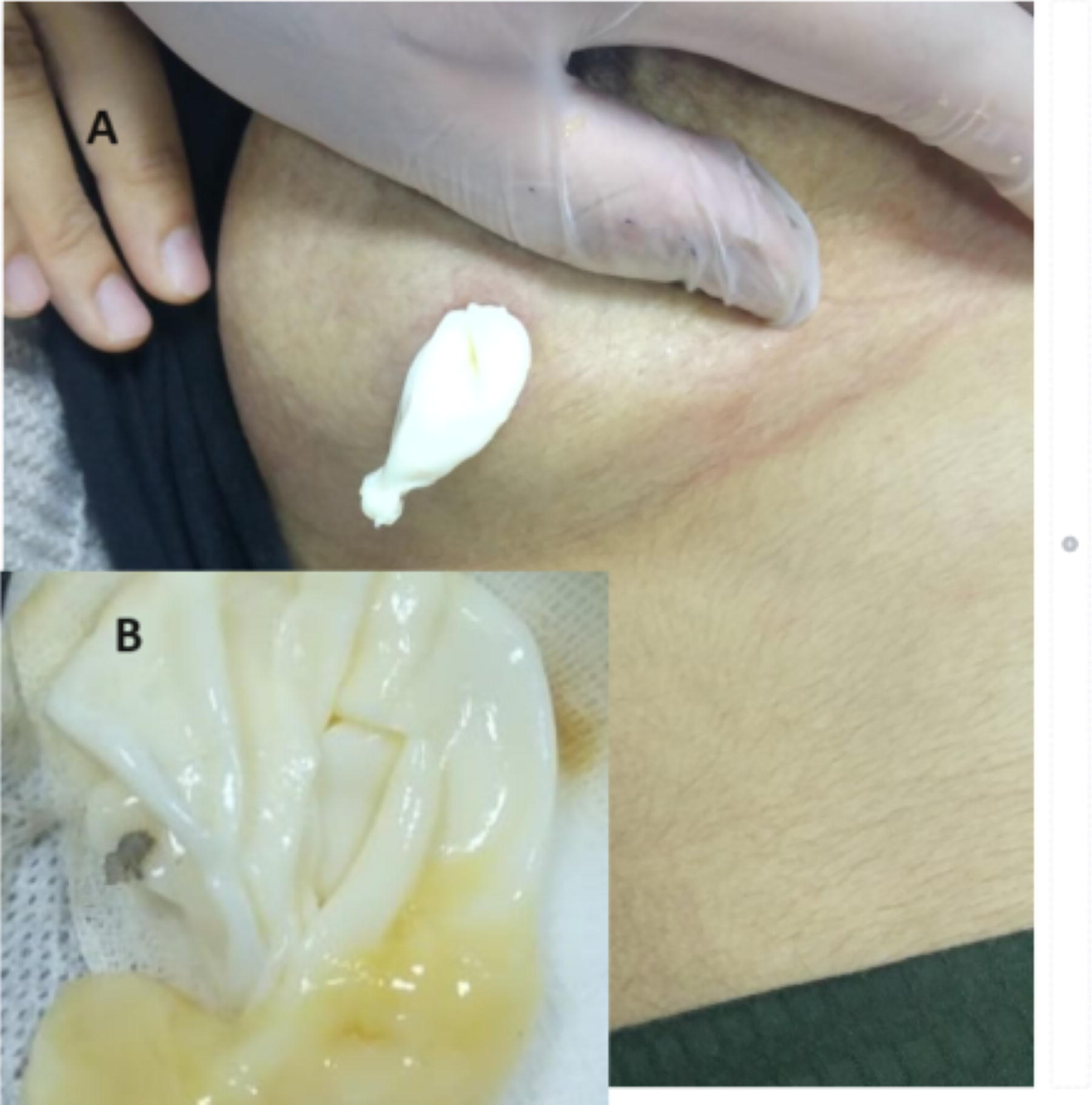
Breast ultrasonography (USG) revealed a complex cyst in the right breast, measuring 6 × 7 cm, with irregular borders, heterogeneous structure, and thin septations. The cyst walls appeared thick and irregular (complex cyst?). According to the USG findings, if a hydatid cyst had been considered, it would have been classified as type 2 according to the Gharbi classification. However, owing to the inability to establish a definitive diagnosis and the patient’s young age, it was decided to proceed with breast magnetic resonance imaging (MRI) for further evaluation. One week after the MRI request, the patient returned to the clinic because of the discharge of white tissue from the breast (Fig. 1). During examination, a white laminar membrane was observed protruding from the breast. Suspecting a hydatid cyst with spontaneous rupture, the previously obtained MRI images were urgently reviewed by radiology. The MRI showed a 6 × 7 cm cyst with thick and irregular walls. Hyperintense signals were observed in the fluid content. The laminar membrane was detached from the pericyst, and it exhibited a floating membrane appearance (Fig. 2).
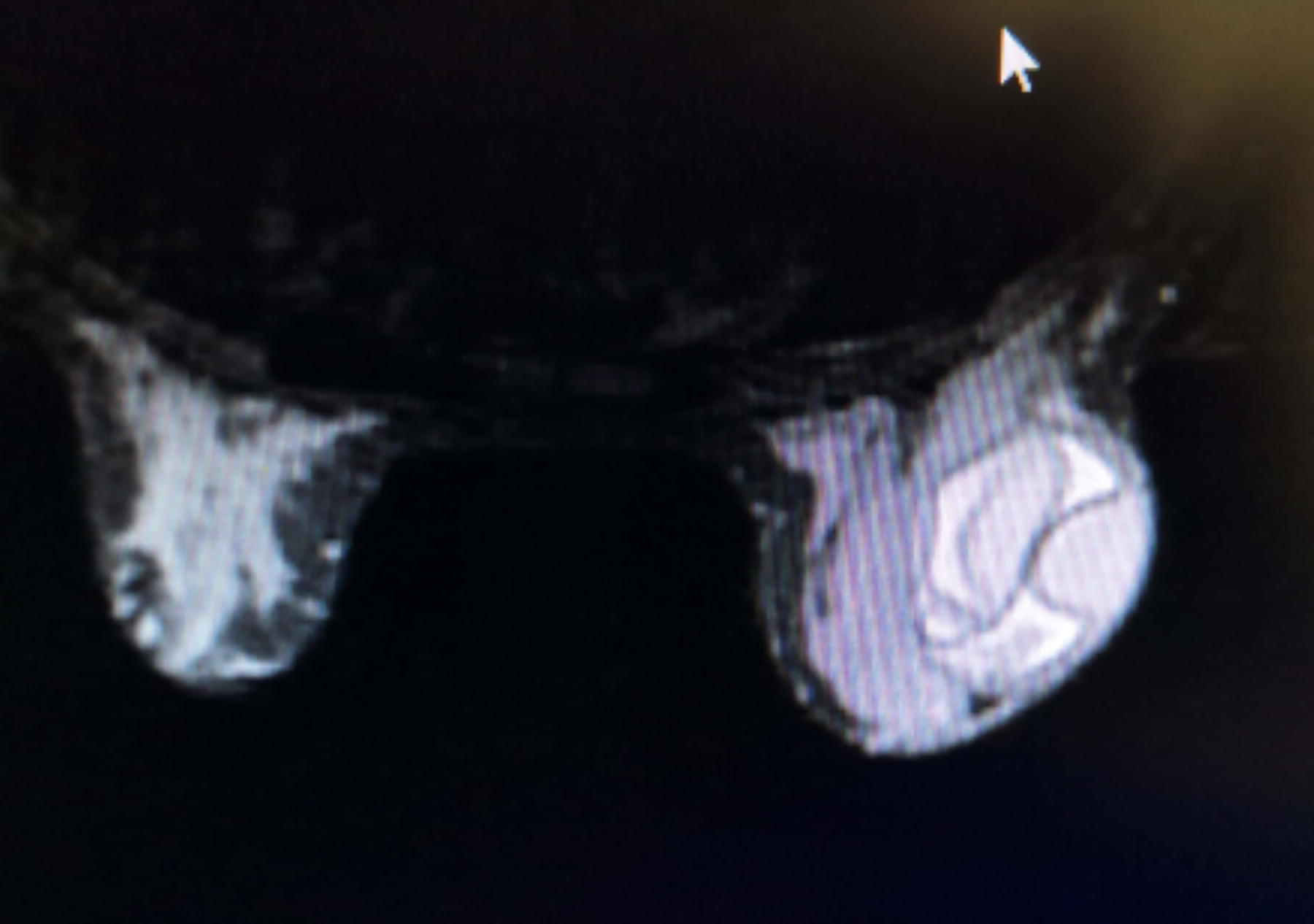
The cyst exhibits thick and irregular walls, with hyperintense signals in its fluid content, and features a laminar membrane detached from the pericyst, presenting a floating membrane appearance.
Under sedation in the operating room, the cyst cavity was explored. Vesicles were removed (Fig. 1), and the cyst cavity was thoroughly irrigated with 3% saline for drainage. Chest radiograph and liver USG showed no pathology. The patient received albendazole therapy at a dose of 10 mg/kg/day for 8 weeks. During the 12-month follow-up, the patient was scheduled for visits every 3 months in the first 6 months. No local or distant recurrence was detected upon reevaluation 6 months later.
The patient was informed about the content and purpose of the article, and written consent was obtained before proceeding with its writing.
Discussion
Breast hydatid cyst is a condition that is rarely observed, with an incidence rate of ∼0.27%. 2 It may occur solely in the breast or as a result of disseminated hydatidosis. 2 It is generally observed in women aged between 30 and 50 years. 3 In our case, a 33-year-old female patient noticed the swelling in her breast but did not seek medical attention for ∼9 months because of the absence of symptoms. This scenario is often associated with painless and slow-growing masses that can remain asymptomatic for years, depending on their location and size within the organ.
Upon the growth and increased pain of the cyst, the patient presented to our clinic. Physical examination revealed a painless mass, prompting an USG for diagnostic purposes. However, USG findings did not definitively distinguish between benign and malignant conditions in the breast, which may not suffice for a conclusive diagnosis of breast hydatid cyst. 4 Therefore, considering the patient’s young age, breast MRI was requested. The literature suggests fine-needle aspiration biopsy or core needle biopsy for diagnosis, 5 but we do not recommend these procedures for diagnosing hydatid cysts at our clinic. Diagnosis of hydatid disease should be ruled out before surgical excision or biopsy to prevent leakage of cyst contents and associated risks of allergy and hydatidosis. 6 Biopsy could perforate the cyst wall and promote dissemination in surrounding tissues, rendering our recommended drainage procedure insufficient. To minimize recurrence, total cystectomy with excision of surrounding healthy tissue is essential despite potential cosmetic implications in the breast. In surgery, our fundamental principle is to preserve normal tissue integrity as much as possible.
Approximately 1 week after the MRI was performed, the patient returned to the clinic because of the discharge of white material from her breast. Upon examination, it was observed that a laminar membrane, characteristic of a hydatid cyst, had emerged from the site of spontaneous perforation. Subsequent review of the previously conducted MRI confirmed support for the diagnosis of a hydatid cyst. In cases where diagnosis cannot be established with USG in young patients, breast MRI is recommended at our clinic.
In endemic regions, when evaluating any organ where cysts can settle, differential diagnosis of hydatid cyst should always be considered. Delayed diagnosis or treatment can lead to serious complications. Spontaneous perforation of the cyst is a rare occurrence. If it had occurred in an organ such as the liver, it could lead to anaphylactic shock. In this patient, likely because of the cyst being only in contact with the skin and early detection, no complications have developed.
Under sedation, the contents of the cyst were evacuated, and irrigation with physiologic saline was performed. The cyst contents were completely emptied without leaving any vesicles inside, and the surgical incision was left open. In the treatment of hydatid cysts, total cystectomy, subtotal cystectomy, or drainage alone can be performed. While total cystectomy is generally recommended to minimize recurrence, in our clinic, we typically recommend drainage alone for hydatid cyst treatment. This procedure was applied to this patient as well. Additionally, the decision to leave the breast incision open instead of opting for complete resection and primary closure was made in accordance with our clinic’s standard practices. This approach, despite being in an endemic region, there may not be a difference in recurrence compared with other surgical approaches. 7
Following each operation, every patient received albendazole therapy at a dose of 10 mg/kg/day to reduce the likelihood of recurrence. 1 Albendazole is a commonly used anti-parasitic agent for treating hydatid cysts; however, alternatives such as mebendazole or praziquantel may also be considered. Current data do not show a clear superiority among these medications. On the basis of our experience in endemic regions, we prefer albendazole as the first choice and recommend a treatment duration of 3–6 months. This duration may vary depending on individual patient factors and clinical response. During the 12-month follow-up period with USG examinations scheduled every 3 months in the first 6 months, no local or distant recurrence was detected when re-evaluated 6 months later in the absence of pathology.
In the literature, the average age of the cases we reviewed was 45.2 years (28–75).2–5 In patients under 40, diagnosis was made solely by USG, while in those over 30, both USG and mammography were used.2–5 As our patient was 33 years old, mammography was not performed. Fine-needle aspiration biopsy (FNAB) was performed in only two cases,2–5 but owing to the risk of rupture, dissemination, and allergic reactions, we do not recommend FNAB for diagnosing hydatid cysts. One patient had cysts in both breasts and the liver, while the other cases were confined to a single breast.2–5 We screen all patients diagnosed with hydatid cysts, and screening is mandatory in multi-centric or bilateral cases. All patients underwent surgical treatment with no observed recurrences.2–5 In our clinic, albendazole is administered instead of operation in patients with comorbidities or where surgical removal is not feasible.
Conclusions
Breast hydatid cyst disease, despite its rare occurrence, should be considered in the differential diagnosis in endemic regions. When USG is inadequate for diagnosis in young patients, MRI is recommended. Drainage is a safe and effective approach for treatment, followed by prophylactic albendazole therapy. Successful outcomes can be achieved with accurate diagnosis and treatment, aiming to improve patient health and minimize the risk of recurrence.
Footnotes
Author’s Contributions
All stages of the article were edited by Y.D. as the sole author.
Funding Information
All expenses for compiling the article were covered by the author. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sector.
Author Disclosure Statement
The author has no relevant conflicts of interest to disclose.