
Abstract
Objective:
This study intended to evaluate the clinical efficacy and safety of colistin sulfate aerosol inhalation in combination with ceftazidime–avibactam for the treatment of pulmonary carbapenem-resistant Klebsiella pneumoniae (CRKP) infection during the peri-operative period of liver transplantation.
Materials and Methods:
A retrospective analysis was designed to investigate 52 patients who developed pulmonary CRKP infection after liver transplantation between December 1, 2019, and November 30, 2022. On the basis of whether they received colistin sulfate aerosol inhalation, the patients were divided into the treatment group (n = 29) and the control group (n = 23). The baseline information, infection status, CRKP enzyme type, inflammatory markers, liver and kidney function, and prognosis were compared and analyzed.
Results:
There were no significant differences in patient characteristics, infection status, and drug resistance enzyme type between the treatment group (treated with colistin sulfate aerosol inhalation and ceftazidime and avibactam sodium for injection) and the control group (treated with ceftazidime and avibactam sodium for injection alone). Colistin sulfate aerosol inhalation treatment reduced concentrations of inflammatory markers, with post-treatment white blood cell count, procalcitonin, and C-reactive protein significantly lower than pre-treatment levels (p < 0.05). Except for C-reactive protein at 14 days (p = 0.032), the two groups had no significant differences in other indicators. There were no significant differences in alanine aminotransferase, aspartate aminotransferase, total bilirubin, and glomerular filtration rate after treatment, indicating no discernible alteration in liver and kidney function. In addition, the treatment group took a significantly shorter time to normalize body temperature compared with the control group (p = 0.025), but there were no significant differences in the cure with no colonization rate and all-cause mortality rate between the two groups.
Conclusions:
The combination of colistin sulfate aerosol inhalation and ceftazidime and avibactam sodium for injection is effective in treating pulmonary CRKP infection during the peri-operative period of liver transplantation. It does not impose an additional burden on liver and kidney function, providing a new treatment option for this type of infection.
Introduction
Liver transplantation is the preferred treatment for end-stage liver disease and hepatocellular carcinoma.1,2 For liver transplant recipients, the post-operative one-year survival rate can reach 90%, and the 10-year survival rate can surpass 70%.3,4 However, patients undergoing liver transplantation are more susceptible to multidrug-resistant bacterial infections because of compromised immune function,5,6 which is a major cause of early post-operative mortality.7,8
Currently, multidrug-resistant bacteria are the most common cause of nosocomial infections in liver transplant recipients, including methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus, Clostridium difficile, and gram-negative bacteria, 9 with an incidence rate of approximately 34%. 10 Reports have shown a continuous increase in resistance rates of gram-negative bacteria to imipenem and meropenem, with Klebsiella pneumoniae exhibiting resistance rates of 3.0% and 2.9% in 2005, which have increased to 23.1% and 24.4% based on data collected until 2021. 11 Carbapenem-resistant Klebsiella pneumoniae (CRKP), a gram-negative bacterium, is associated with clinical infections such as pneumonia, urinary tract infections, sepsis, surgical site infections, and meningitis.12–14 The mortality rate of CRKP infections (42.14%) is greater than that of carbapenem-susceptible Klebsiella pneumoniae infections (21.16%), 15 and the incidence of CRKP infections in intensive care unit (ICU) (59.62%) is significantly greater than that in non-ICU patients (22.18%).16,17
Currently, there are limited antimicrobial agents available for treating CRKP infections, 18 including tigecycline, polymyxins, ceftazidime–avibactam, and several aminoglycosides. 19 However, tigecycline has low concentrations in the blood stream and may not be the preferred treatment for blood stream infections. 20 In 2021, the Infectious Diseases Society of America (IDSA) guidelines recommended the combination of ceftazidime–avibactam and aztreonam for treating CRKP infections. 21 Zhang et al. demonstrated substantial bactericidal effects of ceftazidime–avibactam alone or in combination with aztreonam against Klebsiella pneumoniae carbapenemase (KPC) or New Delhi metallo-β-lactamase (NDM) carbapenemase-producing Klebsiella pneumoniae in both in vitro and in vivo experiments. 22 However, there have been reports of ceftazidime–avibactam resistance in CRKP strains in China, with metallo-β-lactamase production, blaKPC-2 point mutations, and high KPC expression being the main mechanisms of resistance. 23 Therefore, rapid selection of appropriate drugs and effective control of peri-operative infections in liver transplantation become crucial when ceftazidime–avibactam treatment is ineffective.
Colistin sulfate, also known as polymyxin E, is an effective antibiotic against all multidrug-resistant gram-negative bacteria. 24 In addition to intravenous administration, it can also be delivered via aerosol inhalation, thereby increasing the drug concentration in lung tissue and treating multidrug-resistant gram-negative bacteria infections with certain clinical efficacy.25,26 Aerosol inhalation of colistin sulfate maximizes its contact with pulmonary infection sites, thereby improving treatment effectiveness, whereas greatly reducing the systemic toxic side effects associated with intravenous injection. 27 Choe et al. evaluated the clinical outcomes and safety of colistin treatment in critically ill pneumonia patients caused by CRKP, with data supporting that the combination of aerosol inhalation and intravenous injection of greater doses of colistin increases the eradication rate of carbapenem-resistant gram-negative bacteria (60%) and reduces the 30-day mortality rate (23%), without increasing kidney toxicity. 28 Furthermore, a randomized controlled trial also found that adjunctive inhalation of fosfomycin/tobramycin shortens the duration of treatment for ventilator-associated pneumonia caused by extensively drug-resistant Acinetobacter baumannii. 29 Therefore, aerosol inhalation of colistin sulfate holds potential clinical application in the adjunctive treatment of multidrug-resistant gram-negative bacteria infections.
Currently, there is a lack of research on the efficacy of colistin sulfate in the treatment of pulmonary CRKP infections during the peri-operative period of liver transplantation in China. This study explored the effects of intravenous injection of ceftazidime/avibactam during the peri-operative period of liver transplantation, combined with adjunctive aerosol inhalation of colistin sulfate, and monitored the liver and kidney functions of the patients to evaluate the treatment effectiveness and quality of life, providing new insights and options for the treatment of CRKP infections after liver transplantation.
Materials and Methods
Study design and patient selection
A retrospective analysis was conducted on the medical records of 52 patients who were admitted to Shulan (Hangzhou) Hospital from December 1, 2019, to November 30, 2022, and who developed pulmonary CRKP infections after liver transplantation. On the basis of whether the patients received adjunctive treatment of colistin sulfate aerosol inhalation, they were divided into the treatment group (n = 29) and the control group (n = 23). The control group was treated with ceftazidime and avibactam sodium (2.5 g, tid, Pfizer Inc.) for injection, whereas the treatment group received aerosol inhalation of colistin sulfate therapy (250,000 IU, bid, Shanghai Pharma New Asia Pharma Co., Ltd) in addition to the same treatment. Aerosol inhalation therapy was conducted using a vibrating mesh nebulizer.
Inclusion criteria were as follows: age between 18 and 75 years; occurrence of pulmonary CRKP infection during the peri-operative period (one week before surgery to one month after surgery); confirmation of CRKP positivity through sputum/pharyngeal swab culture or second-generation sequencing of bronchoalveolar lavage fluid; patients with at least one of the following imaging findings on chest computed tomography: newly appeared pulmonary inflammatory infiltration, increased or worsening severe pulmonary infiltration, consolidations, pulmonary abscesses, multiple patchy consolidations, or increased pulmonary markings; patients exhibiting persistent cough, dyspnea, chest pain, accompanied by purulent or viscous sputum production; and patients with elevated white blood cell (WBC) count (≥10 × 109/L). Exclusion criteria were as follows: the presence of malignant tumors; allergy to study drugs; and the presence of mental disorders or communication barriers.
Respiratory therapy interventions
In both the treatment and control groups, patients routinely received nebulized ipratropium bromide (500 mg) three times daily (tid) after the onset of infection to prevent potential bronchospasm caused by either the infection or the medication.
Outcome measures
Statistical analysis
Statistical analysis and graphical representation were performed using SPSS 25.0 and GraphPad Prism 8 software. Measurement data were presented as mean ± standard deviation and independent sample t-tests were used for intergroup comparisons. Enumeration data were presented as n (%) and compared with chi-square tests or Fisher exact test. A p value of <0.05 was considered statistically significant.
Results
Baseline characteristics of patients
In the treatment group (aerosol inhalation of colistin sulfate + intravenous injection of ceftazidime–avibactam), there were 24 male patients, accounting for 82.76% of the total, with a mean age of 51.03 ± 11.39 years. Fever was present in 25 patients, accounting for 86.21%. The top three primary diseases were hepatitis B virus–related liver failure, with 18 cases (62.07%), hepatic cirrhosis caused by hepatitis B, with 10 cases (34.48%), and hepatic encephalopathy, with 8 cases (27.59%). In the control group (treated with intravenous injection of ceftazidime–avibactam alone), there were 20 male patients, accounting for 86.96% of the total, with a mean age of 56.21 ± 11.30 years. Fever was present in 21 patients, accounting for 90.30%. The top three primary diseases were hepatitis B virus–related liver failure, with 14 cases (60.87%), hepatic cirrhosis caused by hepatitis B, with 12 cases (52.17%), and primary liver cancer, with 12 cases (52.17%). There were no significant differences between the two groups (p > 0.05) (Table 1).
Patient Baseline Characteristics
The causes of CRKP infection in both groups were categorized into three types: pre-operative colonization, post-operative onset, and donor-derived colonization. In the treatment group, there were 12 cases of pre-operative colonization and 17 cases of post-operative onset. In the control group, there were six cases of pre-operative colonization and 17 cases of post-operative onset. Among all patients who were pre-operatively included, only one case in the treatment group received polymyxin B (500,000 IU, q 12 h) for 20 days before surgery, whereas the remaining patients did not receive any antibiotic treatment. The main sites of concomitant infections in both groups were septicemia and abdominal cavity infection, with Candida being the predominant concomitant infectious microorganism (Table 2). The distribution of drug-resistant enzyme types in CRKP infections in both groups is shown in Table 3. The predominant resistance gene was KPC (25 cases vs. 19 cases), followed by NDM, KPC + NDM, and oxacillinase-48 (OXA-48), with no significant differences between the two groups (p = 0.344).
Incidence of Infections in Two Groups of Patients
CRKP = carbapenem-resistant Klebsiella pneumonia.
Enzyme Types of CRKP Infections
CRKP = carbapenem-resistant Klebsiella pneumonia; KPC = Klebsiella pneumoniae carbapenemase; NDM = New Delhi metallo-β-lactamase; OXA-48 = oxacillinase-48.
Laboratory examination indicators before and after treatment in both groups
Comparison of inflammatory markers before and after treatment in both groups
The results of inflammatory markers before and after treatment in both groups are shown in Figure 1. In the treatment group, WBC, PCT, and CRP were significantly lower after 7 and 14 days of treatment compared with before treatment (WBC: 15.03 vs. 8.61 vs. 7.03, p < 0.01; PCT: 6.33 vs. 1.76 vs. 0.77, p < 0.05; CRP: 89.79 vs. 39.98 vs. 25.62, p < 0.05). However, in the control group, there was no significant difference in PCT before and after treatment, whereas WBC and CRP were significantly lower after 7 and 14 days of treatment compared with those before treatment (WBC: 12.72 vs. 9.41 vs. 7.11, p < 0.05; CRP: 128.04 vs. 54.65 vs. 51.57, p < 0.001). There were no statistically significant differences in WBC and PCT between the treatment and control groups, either before or after 7 or 14 days of treatment. However, the CRP level on day 14 after treatment was significantly lower in the treatment group than in the control group (25.62 vs. 51.57, p = 0.032).
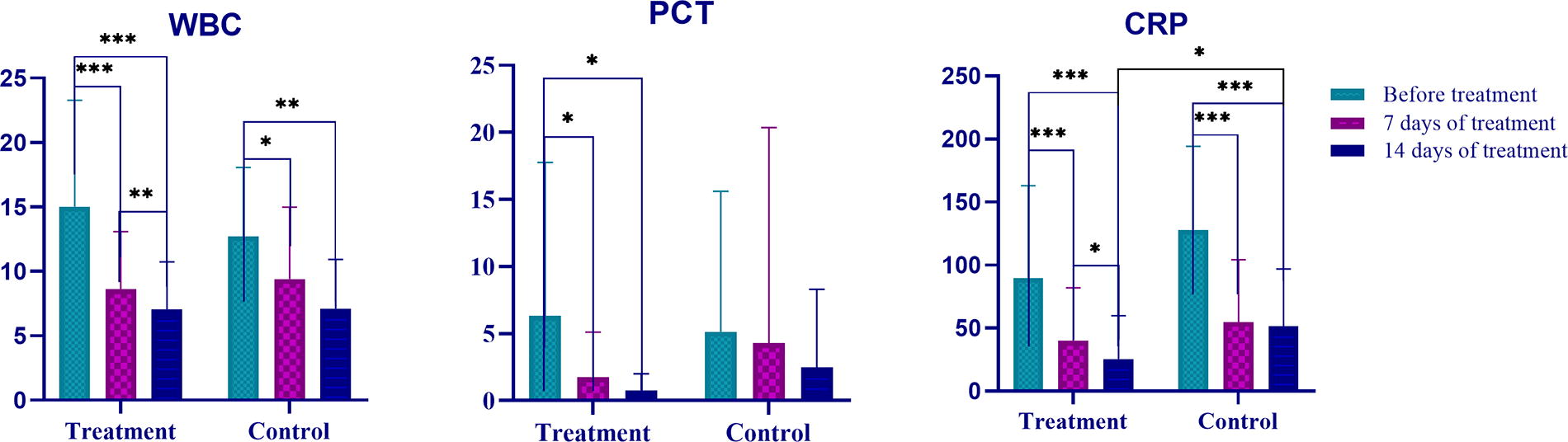
Changes in inflammatory markers before and after treatment in both groups. *p < 0.05; **p < 0.01; ***p < 0.001.
Comparison of liver and kidney function markers before and after treatment in both groups
The changes in liver and kidney function markers before and after treatment in both groups are shown in Figure 2. In the treatment group, there were significant differences in ALT and AST after 7 and 14 days of treatment (ALT: 121.54 vs. 55.34 vs. 51.71, p < 0.01; AST: 177.86 vs. 33.93 vs. 32.29, p < 0.05), and TB was significantly lower after 7 and 14 days of treatment compared with before treatment (92.00 vs. 43.41 vs. 27.00, p < 0.01). There were no significant differences in GFR and SCR before and after treatment. In the control group, there were no significant differences in ALT, AST, and SCR before and after treatment, whereas TB was significantly lower after 7 and 14 days of treatment compared with the concentration before treatment (60.68 vs. 35.18 vs. 25.81, p < 0.05). GFR was significantly lower after 7 and 14 days of treatment compared with the concentration before treatment (85.40 vs. 103.70 vs. 104.43, p < 0.05). There were no significant differences in ALT, AST, TB, and GFR between the treatment and control groups, either before or after treatment. However, the concentration of SCR was significantly different between the treatment and control groups before treatment (SCR: 63.35 vs. 120.18, p = 0.034, p = 0.034). The results are shown in Table 4.
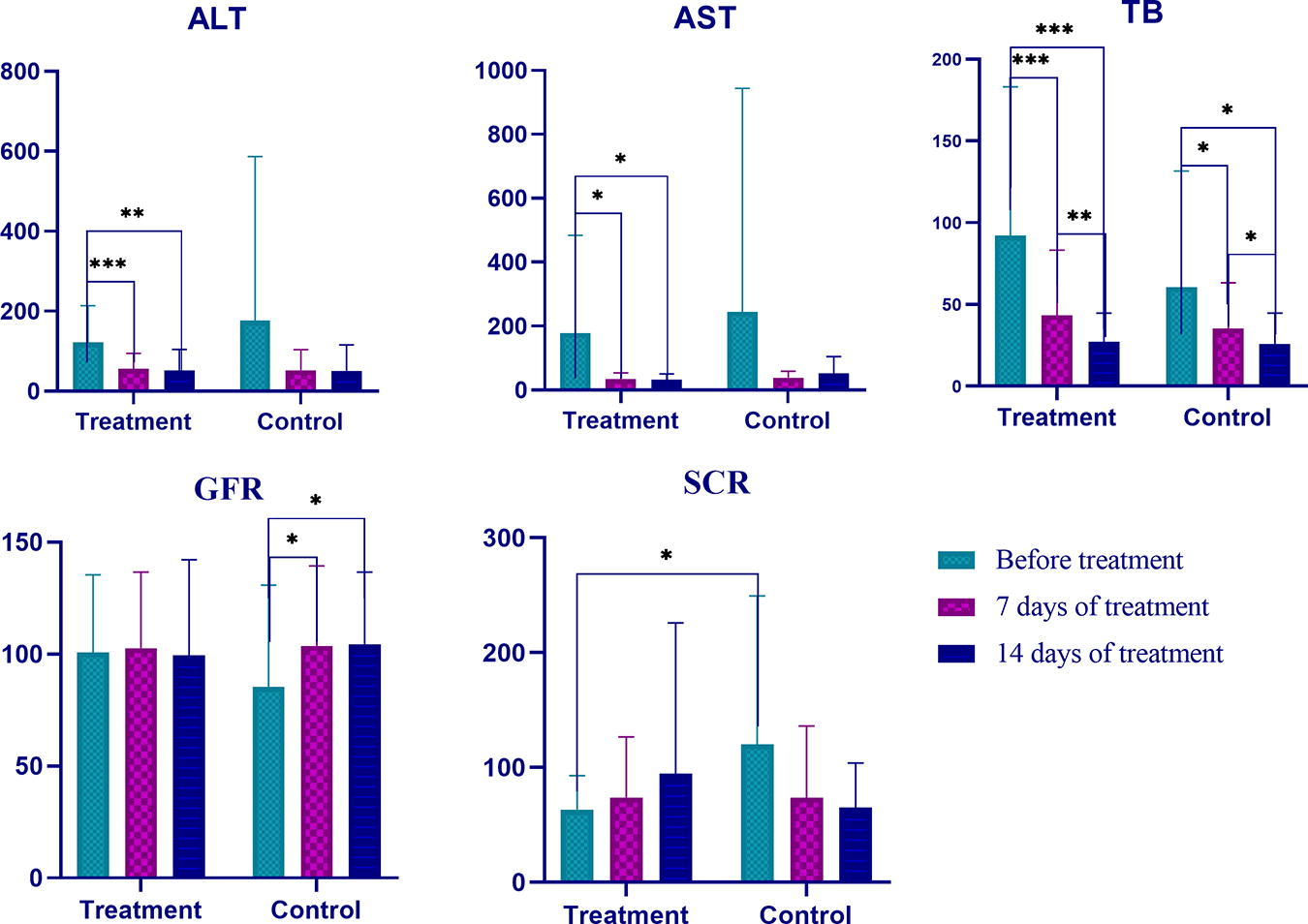
Status of liver and kidney function before and after treatment in both groups. *p< 0.05; **p < 0.01; ***p < 0.001.
Liver and Kidney Function Before and After Treatment in Both Groups
ALT = alanine aminotransferase; AST = aspartate aminotransferase; TB = total bilirubin; GFR = glomerular filtration rate; SCR = serum creatinine; d0 = before treatment; d7 = 7 days of treatment; d14 = 14 days of treatment.
d0 vs. d7 with significant difference.
d7 vs. d14 with significant difference.
d0 vs. d14 with significant difference.
Comparative analysis of post-treatment prognosis in both groups
There were no significant differences between the treatment and control groups in pre-treatment Tmax, cure with no colonization rate, proportion of infections leading to mechanical ventilation >24 hours, duration of mechanical ventilation because of infection, and all-cause mortality rate. However, the time for the treatment group to normalize body temperature was significantly lower than that for the control group (6.96 vs. 13.19, p = 0.025). The results are shown in Table 5.
Prognosis of Two Groups
Discussion
In this study, we treated patients with peri-operative pulmonary CRKP infections following liver transplantation using aerosol inhalation of colistin sulfate combined with injection of ceftazidime–avibactam. The results revealed that CRKP infections primarily originated from pre-operative colonization and post-operative onset, with septicemia and abdominal cavity infection being the main sites of infection. The predominant resistance mechanism in both groups was KPC. During the treatment process, the inflammatory markers in the treatment group significantly decreased after 7 and 14 days of treatment, whereas there were no significant changes in PCT in the control group. There were no significant differences in WBC and CRP between the two groups before or after treatment, but the PCT level on day 14 after treatment was significantly lower in the treatment group than in the control group. The ALT, TB, GFR, and SCR levels did not show significant differences between the two groups after treatment, but the AST level on day 14 after treatment was significantly lower in the treatment group than in the control group. Post-treatment prognosis indicators, such as pre-treatment Tmax, cure with no colonization rate, and all-cause mortality rate, did not show significant differences between the treatment and control groups. Of note, the duration of mechanical ventilation was significantly shorter in the treatment group than in the control group, suggesting that aerosol inhalation of colistin sulfate may help reduce the duration of mechanical ventilation following CRKP infection and improve patient outcomes without causing additional hepatic or renal burden.
Previous studies have found that adjunctive nebulized antibiotic agents can enhance the effectiveness of pneumonia treatment.29,30 Tian et al. found a high rate of heteroresistance to colistin and tigecycline in clinical isolates of CRKP, and the combination of colistin and tigecycline showed effective bactericidal activity against heteroresistant strains. 31 We speculate the possible reason is that colistin sulfate can disrupt the integrity of the bacterial outer membrane, allowing tigecycline to accumulate within the bacterial cell. Tigecycline binds to the 30S ribosomal subunit of bacteria, inhibiting protein synthesis and exerting its antibacterial ability. 32 However, colistin sulfate is a concentration-dependent antibiotic, and its systemic diffusion is limited even in the presence of a damaged alveolar–capillary barrier.33,34 Therefore, the dosing of aerosol inhalation of colistin sulfate should consider both the injected dose and the lung deposition dose. 35 For example, Ratjen et al. observed the efficacy of administering 2 million IU of colistin to 30 patients with cystic fibrosis (CF) and found that high-concentration inhaled colistin can treat patients with CF infected with Pseudomonas aeruginosa. 36 Furthermore, in a study on the pharmacokinetics of ventilator-associated pneumonia, it was found that a dose of 1 million IU tid of inhaled colistin is insufficient to treat lung infections caused by multidrug-resistant strains. 37 In our study, the dose of nebulized colistin sulfate was only 250,000 IU bid. Therefore, the lack of significant differences in WBC and CRP between the two groups in our study may be attributed to the relatively low dose of nebulized colistin sulfate, with the main therapeutic effect being attributed to intravenous injection of ceftazidime–avibactam.
Mechanical ventilation is a therapeutic approach commonly used to support patients with respiratory insufficiency.38,39 It can be classified into non-invasive mechanical ventilation (mask) and invasive mechanical ventilation (endotracheal intubation and ventilator). 40 Although there were no significant changes in the resolution of inflammation, the duration of mechanical ventilation decreased after aerosol inhalation of colistin sulfate, indicating an improvement in respiratory function and a faster liberation from ventilator dependence. We speculate that colistin sulfate kills bacteria by membrane disruption or promoting the exchange of phospholipids between vesicles, causing osmotic imbalance and leading to bacterial swelling and lysis, 41 thus reducing pulmonary mucus and improving airway patency. However, the differences between the two groups were not significant, possibly because of considerable individual variability (with two patients in the control group requiring tracheostomy because of infection and ICU-acquired weakness, leading to mechanical ventilation times exceeding 800 h) and a small sample size. In addition, this study found that the time for body temperature to return to normal in the treatment group was significantly shorter than that in the control group. A possible reason is that colistin sulfate also possesses anti-inflammatory properties. 42 Its primary target is the lipopolysaccharide (LPS) of outer membranes of gram-negative bacteria, and it exerts its antibacterial effect by directly interacting with the lipid A component of LPS,43,44 which leads to faster control of inflammation in the body and thus a quicker return to normal body temperature. Although this study did not show substantial changes in the resolution of inflammation with colistin sulfate, it still had some degree of impact on controlling pulmonary inflammation.
According to an investigation by the IDSA, the use of colistin is associated with greater mortality and increased hepatorenal toxicity than other antibiotic agents. 45 In our study, ALT, AST, and TB all improved after treatment, indicating successful liver transplantation. There were no significant differences in ALT, TB, GFR, and SCR between the two groups after treatment. Although the AST level in the treatment group was significantly lower than that in the control group, it remained within the normal range, suggesting that aerosol inhalation of colistin sulfate did not impose an additional burden on liver and kidney function. The possible reason for this is the different routes of administration. Intravenous administration of colistin sulfate can impose a certain burden on the kidneys, with approximately 50% of the total dose of colistin sulfate excreted in the urine. 46 In contrast, aerosol inhalation of colistin sulfate can maximize the precise delivery of the drug to the target site and effectively eliminate CRKP in the target site. 33 Compared with intravenous infusion, systemic exposure to colistin sulfate after nebulization is significantly reduced, 47 thereby reducing the risk of nephrotoxicity. 48 This is consistent with the findings of Nadeem and Lee, who suggested that local administration of colistin can effectively treat infections while reducing systemic toxicity.49,50 Therefore, the treatment regimen of aerosol inhalation of colistin sulfate combined with intravenous injection of ceftazidime–avibactam can reduce the time required for body temperature to return to normal concentration, improve recovery speed, and relatively not increase side effects.
Although nebulized colistin inhalation as a novel treatment modality demonstrated good therapeutic efficacy and safety in this study and provided a new option for the treatment of CRKP infections in liver transplantation, there are still some limitations. First, the sample size of this study was small, and it was a single-center study. Future research should include more multicenter studies with large sample sizes to validate the results. Second, we did not conduct long-term follow-up of the patients, thus unable to explore the durability of treatment effects. Further investigations with extended follow-up periods are needed to observe treatment outcomes. Finally, this study did not explore the optimal dosage and duration of nebulized colistin sulfate. Future studies should investigate different dosage and duration groups to find the optimal inhalation dose and treatment duration.
Footnotes
Authors’ Contributions
Conceptualization: X.L. and J.L. Data curation: Z.W. and L.Z. Formal Analysis: X.L. and J.L. Funding acquisition: X.L. and S.Z. Investigation: Z.W. and L.Z. Methodology: J.L. and S.Z. Project administration: Z.W. and L.Z. Resources: G.J. Software: G.J. Supervision: J.M. Validation: J.M. Visualization: G.J. Writing—original draft: X.L., J.L., S.Z., and Z.W. Writing—review and editing: Z.W., L.Z., and G.J.
Ethics Approval and Consent to Participate
This study is approved by the Ethics Committee of Shulan (Hangzhou) Hospital (KY2024063).
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article.
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
This study is supported by