
Abstract
Background:
The risk of poor surgical site healing in patients with spinal tuberculosis due to M. tuberculosis infection is known to be higher than in other surgical patients. Early identification and diagnosis are critical if we are to reduce the disability and mortality associated with spinal tuberculosis. We aimed to develop and validate a novel predictive score for predicting the risk of poor surgical site healing in patients following surgical procedure for spinal tuberculosis.
Patients and Methods:
We retrospectively analyzed the clinical data of patients with spinal tuberculosis who were hospitalized in the orthopedic ward of four regional medical centers in Guizhou Province between January 2015 and October 2022. Univariate and LASSO analysis was used to identify risk factors, construct and evaluate predictive models and novel predictive score for poor surgical site healing following the surgical procedure. Subsequently, 110 patients, admitted to four regional medical centers in Guizhou Province between January 2023 and February 2024, were used as an external prospective validation cohort to test the predictive efficacy of the prediction model.
Results:
Seven predictors were identified as risk factors for poor surgical site healing in patients undergoing surgical procedure for spinal tuberculosis. The areas under the receiver operating characteristic curve for a risk prediction model constructed based on the significant risk factors were 0.753 (95% CI: 0.693–0.813) and 0.779 (95% CI: 0.696–0.863) for the training and validation sets, respectively. Decision curve analysis demonstrated that the model yielded good clinical benefit. Finally, we applied the newly developed poor surgical site healing risk assessment score for the external prospective validation set; the area under the receiver operating characteristic curve for the poor surgical site healing risk assessment score was 0.846 (95% CI: 0.769–0.923) demonstrated that the model yielded better predictive effectiveness.
Conclusion:
The novel poor surgical site healing risk assessment score exhibits good discriminatory power and represents a beneficial predictive tool for facilitating suitable postoperative clinical management.
Spinal tuberculosis (STB) is a secondary infection that arises from the dissemination of Mycobacterium tuberculosis to the spinal column and represents the predominant form of extrapulmonary tuberculosis and is the underlying cause of 50%–70% of osteoarticular tuberculosis cases.1–4 Despite a notable reduction in mortality rates in patients with STB, the frequency of spinal infections has exhibited a consistent upwards trend over recent decades.5–7 Spinal infection poses a significant risk for poor surgical site healing (PSSH), a serious complication that often manifests within days to weeks after surgical procedure. The management of PSSH remains very challenging as prevention and treatment are not timely and may develop into surgical site infection (SSI) and even secondary sepsis and osteomyelitis.8,9 This complication can prolong hospitalization, impede patient recovery, and increase the likelihood of an unplanned return to the operating room.10–12 Previous studies have reported that early diagnosis and treatment can improve prognosis and reduce mortality. 13 Therefore, development of an early prediction tool is needed for poor surgical site healing (PSSH) in these patients.
A range of basic information and laboratory test results are available after admission, often before or soon after surgical procedure; therefore, it is reasonable to consider that earlier recognition models could be derived for predicting PSSH on the basis of data that are collected routinely. In clinical practice, clinical and laboratory variables are increasingly being used for patient monitoring. 6 The automated mining of these data provides us with an excellent opportunity to expedite clinical diagnoses and improve outcomes.14,15 Recently, Chen et al. 6 performed a single-center retrospective study and constructed a nomogram to predict the risk of postoperative SSI in patients with STB. In another study, Li et al. 16 built a model to predict the ability of technology to detect pathogens specific to STB infections, and effectively shorten diagnostic cycle. Subsequently, Hu et al. 13 built a disease prediction model with a nomogram to predict the occurrence of STB at an early stage; this provided a tool that can effectively guide doctors to systematically administer antituberculosis drugs at an early stage. All of these existing models provide an automated estimate of the risk of disease or complications according to daily that are collected on a daily basis. However, a predictive model for PSSH in patients undergoing surgical procedure for STB that can facilitate clinical management has yet to be developed.
In the present study, we aimed to develop and validate a predictive score for the differentiation of PSSH on the basis of routine variables that can be easily measured during clinical processes postadmission and before or during the early postoperative period. We followed a fully data-driven approach using the entire set of information collected from the patients undergoing surgical procedure for STB and then constructed a score that can be applied for the early prediction of PSSH. We hypothesized that the combination of clinical risk factors and biomarkers, compared with either alone, would provide a superior prediction model for identifying patients at a high risk of PSSH.
Patients and Methods
Patient enrollment
This study was conducted at the Affiliated Hospital of Guizhou Medical University, the Second Affiliated Hospital of Guizhou Medical University, Guizhou Provincial People’s Hospital, and Guizhou Provincial Orthopedic Hospital. Patients with STB were enrolled between January 2015 and October 2022 to allow us to develop a suitable model. A multi-center, prospective study was conducted at the Affiliated Hospital of Guizhou Medical University, Guizhou People’s Hospital, and Guizhou Orthopedic Hospital, from January 2023 to February 2024, to verify the predictive efficacy of the model. Patients with STB who met the following criteria were included in the study: (1) patients diagnosed with STB by clinicopathological imaging; (2) aged ≥18 years; and (3) the surgical methods involved open debridement and combined lateral debridement. Patients were excluded for the following reasons: (1) complicated by acute, urinary, or respiratory system infections; (2) the presence of tumors and a history of radiotherapy and chemotherapy in the spinal region; (3) multiple organ failure that made it difficult for the patient to tolerate surgical procedure; and (4) severe anemia or hypoproteinemia that could not be improved by preoperative treatment. Diagnostic criteria for PSSH were included SSI and PSSH in the study, and diagnosis was made on the basis of the presence of one of the following conditions: first, SSI—(1) redness, swelling, heat, pain, or purulent secretion on the surface of the incision; (2) presence of pus in the deep part of the incision (determined through drainage or puncture); (3) purulent secretion or fever >38°C in the cracked incision and local pain or tenderness in the incision; (4) deep incision abscess or other evidence of infection found by surgical exploration, histopathology or imaging examination; and (5) incisional or lacunar infections diagnosed by clinicians on the basis of positive bacterial culture of secretions after pathogen testing, and second, PSSH—In electronic medical cases, when the description of poor healing of the surgical site in the medical and nursing records shows significantly stagnant, delayed, or complex exudates in the incision healing process more than 7 days after the surgical procedure, leading to a long-term non-union state, hematoma at the incision site, and even incision cracking and persistent inflammation, it may be defined as PSSH.5,17,18 Basic features and clinical data were extracted from electronic medical records. All sensitive patient information was excluded from this study, which was approved by the Institutional Review Board of the Affiliated Hospital of Guizhou Medical University (approval number: 2023 Trial No. 894). Each patient, or their next-of-kin/family provided informed consent to participate.
Key variables
We collated a range of demographic data for the enrolled patients, including age, gender, body mass index (BMI), disease duration, duration of antituberculosis drug treatment, systolic blood pressure, and diastolic blood pressure. Surgical variables included the duration of surgical procedure, approach, requirement for a combined operation, operation site, number of operative segments, number of pedicle screws, incision length, intraoperative blood loss, blood transfusion requirement, volume of transfused blood, postoperative drainage volume, and the number of drainage tube roots. Laboratory variables included routine blood tests (white blood cell count, hemoglobin, hematocrit, platelet, neutrophil ratio, lymphocyte count, lymphocyte ratio, monocyte count, monocyte ratio, and neutrophil count), blood coagulation function, liver function tests, renal function tests, biochemical indicators, and blood gas analysis. All variables were recorded preoperatively and at 1–3 days post-surgical procedure. If multiple examinations were performed before or 1–3 days post-surgical procedure, the most recent examination was considered for analysis. Any predictor that was lacking >30% of the dataset was excluded. All missing data were imputed using a two-step approach; when a given variable was missing, we used the value for the day after the event where possible to impute the missing value. For all other cases, we performed imputation using mean values.
Statistical analysis
Continuous variables are reported as the mean and standard deviation and were compared with between patients with poor and good surgical site healing using the Student t or the Mann–Whitney U test. Categorical variables are presented as numbers and proportions, and differences between categorical variables were compared using the chi-squared test. The complete dataset was randomly divided (in a 7:3 ratio) into training and validation datasets. The training dataset included 294 (70.0%) patients and the remaining 126 (30.0%) patients were included in the validation dataset. Three steps were followed to develop a risk model and select the best predictors. First, we analyzed all of the potential predictors for PSSH by applying univariate logistic regression and selected significant candidate predictors (p < 0.05). To avoid introducing predictive optimism, least absolute shrinkage and selection operator (LASSO) techniques were used to select the best subset of features. This technique reduced the coefficient to zero by adjusting lambda. Similar to best subset selection, the LASSO method shrinks certain feature coefficients to zero when the lambda parameter is sufficiently large. 19 We then selected the maximum lambda value, for which the cross-validation error was within one standard error range of the minimum. The LASSO regression model provided the coefficients for each feature. Subsequently, a logistic regression model was constructed to convert the remaining predictors into PSSH prediction scores. Subsequently, we used the ‘rms’ and ‘regplot’ packages to build a nomogram and plot receiver operating characteristic (ROC) curves and calculate area under the ROC curve (AUC) values, and decision curve analysis (DCA) was used to evaluate clinical practicability. Then, the nomogram prediction model was applied to the patients in the test set and the verification set. The probability of each variable in the nomogram model was weighted, and the risk of PWH of patients in the test set was divided into four risk levels of low risk, medium risk and high risk according to the interquar method. A rating table for the PSSH risk assessment score (PSSHRS) in patients with STB, was constructed according to the assignment and risk of each predictor variable. On the basis of the absolute clinical PWH risk level from the PSSHRS, 110 patients with STB were further divided into low-, medium-, high-, and very high-risk groups to verify the predictive efficacy of the model. The incidence of PSSH in the externally validated set was then evaluated by AUC values. All statistical analyses were performed using R (version 4.1.3) and SPSS 25. p Value < 0.05 was considered statistically significant, and all statistical tests were two-sided.
Results
Characteristics of the study cohorts
A total of 744 patients with STB were included in this dataset 214 patients did not meet the inclusion criteria and were excluded. The specific details related to exclusion are presented in Supplementary Figure S1. Thus, 530 patients were included in the final analysis: 294 (70.0%) in the training dataset, 126 (30.0%) in the validation dataset, and 110 in the multicenter prospective external validation dataset. In the training dataset and validation dataset, 288 and 132 cases were in the good surgical site healing and PSSH group, respectively. In this cohort, 88 out of 132 patients (66.67%) with STB exhibited wound seepage. Upon reviewing the medical records of these 88 patients, it was found that bacterial cultures were not performed on the exudate of 21 patients due to insufficient exudate volume. For the remaining 67 patients with adequate exudate, bacterial cultures were conducted. The results indicated that Escherichia coli was present in 39 cases (58.21%), Staphylococcus aureus was identified in 21 cases (31.34%), and the cultures were negative in 7 cases (10.45%). Among the 132 patients diagnosed with PSSH, 60 exhibited infective exudation and 22 presented with redness, both indicative of SSIs. Consequently, 82 patients (82/132, 62.12%) were classified as having infections. Additionally, 7 patients (7/132, 5.30%) had non-infective exudates, 21 patients (21/132, 15.91%) displayed minor exudates without bacterial culture confirmation, and 19 patients (19/132, 14.39%) experienced bleeding. Furthermore, 2 patients (2/132, 1.52%) suffered from wound rupture, and 1 patient (1/132, 0.75%) exhibited wound liquefaction. In addition, the incidence of PSSH was 31.43% (132/420). Of the 420 patients, 120 (120/420,28.75%), 300 (300/420, 71.43%), 231 (231/420,55%), and 189 (189/420,45%) were >60 years-of-age, ≤60 years-of-age, males, and females, respectively. Within this cohort, 76 (76/420,18.1%) cases had an antituberculosis time >3 months; this compared with to 344 cases (344/420,81.9%) ≤3 months. In the surgical site group, 182 patients (182/420; 43.33%) underwent surgical procedure for lumbar tuberculosis; the incidence of PSSH was 30.77% (56/182). Furthermore, 224 cases (224/420; 53.33%) underwent surgical procedure for thoracic vertebral tuberculosis; the incidence of PSSH was 32.14% (72/224). Fourteen patients (14/420; 3.34%) underwent surgical procedure for cervical vertebral tuberculosis; the incidence of PSSH was 28.57% (4/14). The baseline patient data are shown in Table 1.
General Data on Poor Surgical Site Healing in Patients with Spinal Tuberculosis
BMI, body mass index.
Model and PSSHRS development
First, we used univariate analysis to screen variables from the training dataset and selected 16 predictors (p < 0.05) for subsequent investigation (Table 2). Moreover, for generalization in clinical practice, we used the LASSO technique to identify the variables most suitable for predicting PSSH. During LASSO analysis, the best λ parameter value is selected by a cross-validation method; lambda_1se (λ) was 0.05296478, thus indicating that the variable had strongest comprehensive predictive ability (Fig. 1). On the basis of further screening, seven variables were retained in the LASSO analysis: BMI, combined surgical procedure, 1–3 days postoperative drainage volume, intraoperative blood loss, preoperative albumin level, postoperative neutrophil count, and postoperative direct bilirubin level. Variables with statistical significance (p < 0.05) in the LASSO analysis were then considered as independent variables for multivariate logistic regression analysis; variables with or without PSSH were considered as dependent variables. Analysis identified several risk factors for postoperative PSSH in patients with STB (Table 3): BMI (odds ratio [OR]: 0.452 [0.259–0.787], p = 0.005), preoperative albumin (OR: 0.348 [0.177–0.686], p = 0.002), combined surgical procedure (OR: 2.317 [1.348–3.981], p = 0.002), intraoperative blood loss (OR: 1.887 [1.144–3.113], p = 0.013), 1–3 days postoperative neutrophil count (OR: 0.366 [0.196–0.684], p = 0.002), 1–3 days postoperative direct bilirubin level (OR: 2.010 [1.206–3.350], p = 0.007) and 1–3 days postoperative drainage volume (OR: 2.600 [1.613–4.189], p <0.001). The model was constructed using the seven variables that were statistically significant in the logistic regression analysis, as shown in Figure 2. All seven variables were obtained from routine laboratory measurements and by direct observation.

The potential risk factors selected by least absolute shrinkage and selection operator (LASSO) logistic regression. The maximum lambda parameter was selected using the LASSO model on the basis of the criterion of cross-validation error within one standard error range of the minimum. Different deviance (binomial deviance) values within the range of lambda are also shown.
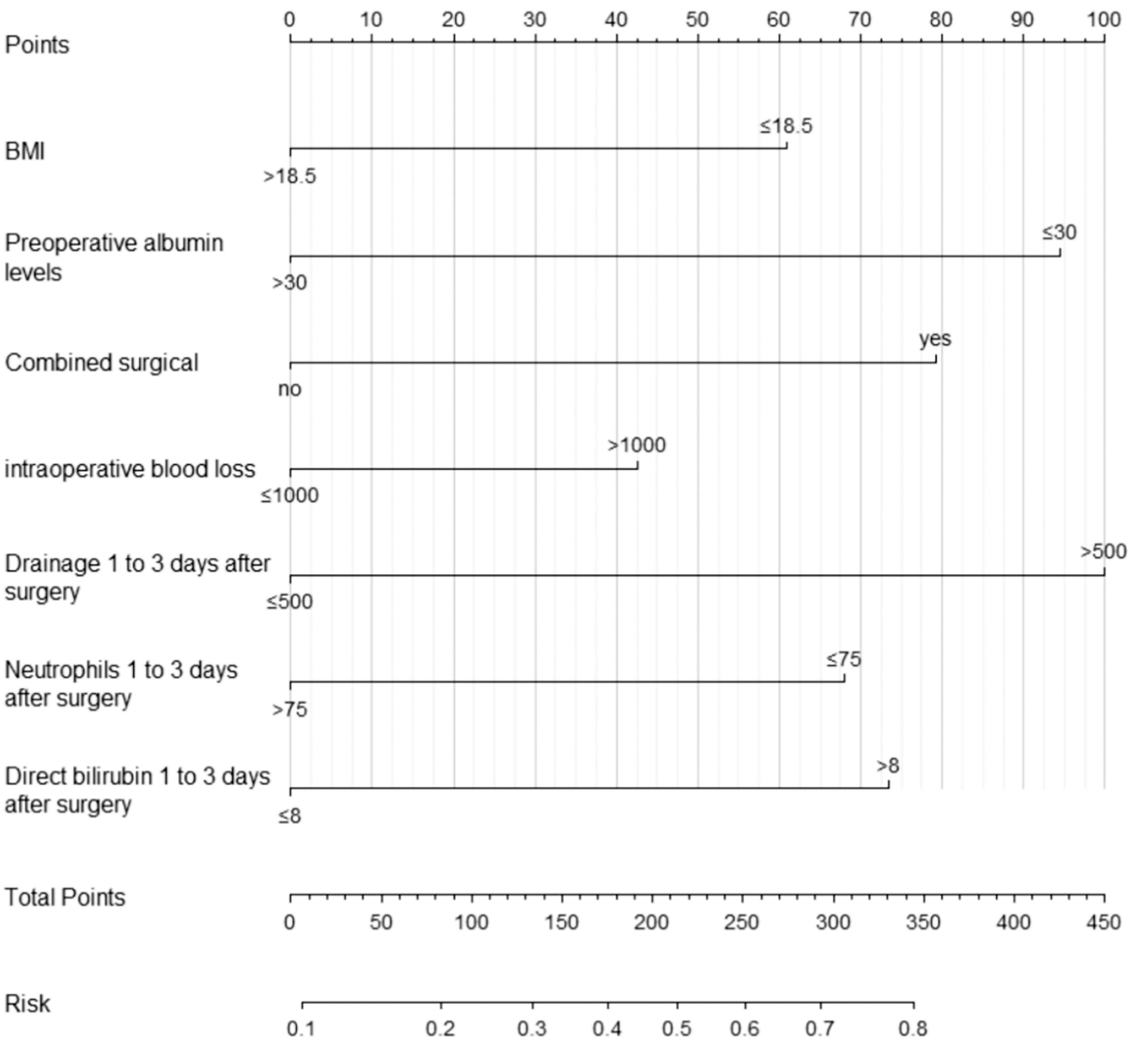
A predictive model for the risk of poor surgical site healing in patients with spinal tuberculosis, which we named the poor surgical site healing risk assessment score (PSSHRAS) for spinal tuberculosis.
Univariate Analysis of Poor Surgical Site Healing in Patients with Spinal Tuberculosis
BMI, body mass index.
Multivariate Logistic Regression Analysis of Poor Surgical Site Healing of Spinal Tuberculosis
Next, we further stratified the PSSHRS into four groups according to quartiles: low (score Q0–Q25), intermediate (score Q26–Q50), high (score Q51–Q75), and very high (score Q76–Q100). The detailed scoring criteria for the PSSHRS prediction model are presented in Table 4. Analysis showed that 119 patients were classified into the low-risk group, accounting for 28.33% (119/420) with a 10.08% (12/119) incidence of PSSH; 96 patients (96/420; 22.86%) were classified into the medium-risk group with a PSSH incidence of 21.88% (21/96). Furthermore, 106 (106/420,25.24%) cases were classified into the high-risk group with a PSSH incidence of 37.74% (40/106); finally, 99 (99/420, 23.57%) cases were classified into the very high-risk group with a PSSH incidence of 59.60% (59/99).
Prediction Model of the PSSH Scoring System
PSSHRS score: Low-risk: 0–2 points; Medium-risk: 3–5 points; High-risk: 6–8 points; Very high-risk: >9 points.
BMI, body mass index; PSSH, poor surgical site healing; PSSHRS, PSSH risk assessment score.
Validation of the PSSHRS
Validation analysis of the PSSHRS revealed that the AUC of the training set was 0.753 (95% CI: 0.693–0.813), with a sensitivity of 70.30% and a specificity of 68.50%; the AUC of the validation set was 0.779 (95% CI: 0.696–0.863) with a sensitivity of 87.80% and a specificity of 58.80%, thus showing good differentiation, as shown in Figure 3. The prediction efficiencies of AUC values for the single variables and the model are shown in Table 5. In the DCA, the X-axis represents the risk threshold for the disease, the Y-axis represents the net benefit, and Y = 0 represents no intervention for all patients. Most of the net benefit curves for the training and test sets were > Y = 0. The DCA of the validation set showed that the model had a better clinical benefit than Y = 0 or patient intervention, as shown in Figure 4. In the external validation set, 110 patients undergoing surgical procedure for STB were evaluated by the same trained investigator with regards to PSSH score and risk. Analysis showed that patients with low risk accounted for 25.45% (28/110) with a PSSH incidence of 14.29% (4/28), patients with high risk accounted for 43.64% (48/110) with a PSSH incidence of 43.75% (21/48), and patients with very high risk accounted for 30.91% (34/110) with a PSSH incidence of 58.82% (20/34). Figure 5 shows a comparison of the ROC curves for the training, test, and external validation sets.

Receiver operating characteristic (ROC) curves for the validation set of patients with spinal tuberculosis with regards to the poor surgical site healing risk assessment score (PSSHRAS).

Decision curve analysis (DCA) curve for the validation set of patients with spinal tuberculosis with regards to the poor surgical site healing risk assessment score (PSSHRAS).

Receiver operating characteristic (ROC) curves for poor surgical site healing in patients with spinal tuberculosis in the training, internal, and external validation sets.
Predicted probability of Single Variable, Training, Validation and External Validation
AUC, area under the receiver operating characteristic curve; BMI, body mass index.
Discussion
The risk of PSSH in patients with STB due to M. tuberculosis infection is known to be higher than in other surgical patients. 20 The poor healing of surgical wounds is associated with a certain degree of difficulty with regards to anti-infection treatments, including secondary sepsis, osteomyelitis, and neurological dysfunction. 8 Severe STB can lead to spinal deformities and even paraplegia. Early identification and diagnosis are critical if we are to reduce the disability and mortality associated with STB. 16 PSSH is the main cause of SSI; furthermore, if the prevention and treatment of PSSH are not carried out in a timely manner, this condition can develop into a SSI, thus delaying recovery and increasing disease burden. 5 Therefore, the establishment and verification of a predictive model for the identification of PSSH in patients with STB at admission and during the early postoperative stage is of great significance for preventing and treating PSSH. In the current study, we developed a novel predictive scoring system for PSSH on the basis of data that are routinely available. We used the LASSO technique to select the best variables for the prediction score. Then, we used logistic regression to further identify the best predictors for building and validating the model. The model was then validated externally using other datasets. We demonstrated that the discrimination and calibration of the new scoring system were satisfactory.
We selected seven predictors to build our model: BMI, preoperative albumin level, combined surgical procedure, intraoperative blood loss, postoperative drainage volume, postoperative direct bilirubin level, and neutrophil count. Each predictor can readily be obtained from routine laboratory indicators and by direct observation, thus representing a convenient method for medical staff to identify potentially high-risk patients with PWH in the early stages. A BMI ≤18.5 kg/m2 and a preoperative albumin level ≤30 g/L were previously reported to represent strong predictors for postoperative PSSH; 21 these findings concurred with those of the present study. Due to the chronic consumption of tuberculosis foci, inflammatory mediators can cause damage to liver cells and hepatic sinus endothelial cells, cause tissue and organ ischemia and hypoxia, liver tissue fibrosis, and reduce the synthesis of albumin, thus resulting in a reduction in BMI and patient resistance.22,23 Concurrent with these events, the colloid osmotic pressure decreases, tissues begin to ooze fluid, while wounds begin to swell and split readily. The increased exudation of tissue fluid at the surgical site increases the risk of pathogenic bacteria entering the skin surface around the wound and increases the risk of PSSH.5,24 A previous study showed that patients who underwent combined surgical procedure experienced a higher incidence of postoperative PSSH. 21 Combined surgical procedure is more likely to lead to increased intraoperative blood loss, a prolongation in operation time, and an increased probability of blood transfusion; furthermore, this can induce a higher state of metabolic stress in the body due to greater surgical trauma. 8 During surgical procedure, the operative area can be manipulated in an aggressive manner; this can damage the surrounding tissue and result in slower rates of wound healing.5,21
The findings of the present study indicate that a direct bilirubin level >8 µmol/L and a neutrophil count ≤75 × 109/L 1–3 days post-surgical procedure are key factors responsible for PSSH in patients with STB. Previous studies reported that bilirubin exerts an anti-inflammatory effect and is transformed into conjugated bilirubin, also known as direct bilirubin,25,26 by binding to glucuronic acid under the action of glucuronyltransferase. 27 Patients with STB are more susceptible to inflammatory cell infection following infection with M. tuberculosis and surgical trauma. This will cause the levels of bilirubin to increase continuously to resist the M. tuberculosis infection and inflammatory cell invasion; thus, these factors represent predictors for PSSH in patients with STB following surgical procedure. 26 Neutrophil count is traditional index that is widely used for the diagnosis of infection. 28 Previous studies have reported that neutrophil count is helpful for the predicting the orthopedic probability of postoperative SSI in a timely manner.28,29 Patients usually exhibit changes in inflammatory cells and after surgical procedure, notably a decline in B-cell-mediated, nonspecific, cellular immune function, thus compromising immune function within 3–4 days after surgical procedure. These events result in lower neutrophil counts that are not sufficient to resist inflammatory invasion, thus increasing the risk of infection and the incidence of PSSH.28,30 The induced flow of patients with STB at 1–3 days - procedure is ≥500 mL; this is likely to lead to increased blood loss, hypoproteinemia, an increased need for blood transfusion, and a number of postoperative complications, including severe electrolyte disturbance and anemia. 31 Impaired immunity and reduced immunity to residual M. tuberculosis can cause secondary destruction of the vertebral body, intervertebral disc, and surrounding tissues, thus causing further damage to the body and delaying tissue recovery.5,32 Furthermore, increased drainage and the prolonged insertion of a wound drainage tube, can increase the risk of infection at the surgical site; this represents a high-risk factor for PSSH.33,34
On the basis of these findings, we conclude that the seven clinical variables and biomarkers included in our prediction model are independent risk factors for PSSH in patients with STB. When these variables were integrated into a panel, their predictive ability was significantly improved. This confirms our hypothesis that although any single variable could be applied for the early prediction of the risk of PSSH in these patients, the discriminatory ability of a single variable is limited.
In clinical practice, the interpretability and practicality of predictive models are of utmost significance. The external validation outcomes of the PSSHRS in this study demonstrate its high accuracy, sensitivity, and specificity. The scoring system is designed to be straightforward and practical, facilitating healthcare professionals in the rapid identification of individuals at elevated risk for impaired wound healing following STB surgery. This capability allows for the timely implementation of intervention measures, thereby mitigating the risk of postoperative complications. Patients with a BMI of ≤18.5 kg/m2and a preoperative albumin level of ≤30 g/L should be identified as high-risk individuals and provided with enhanced nutritional support and perioperative management. Additionally, patients with a drainage volume of ≥500 mL within 1 to 3 days post-surgical procedure, a direct bilirubin level of >8 μmol/L, and a neutrophil count of ≤7.5 × 109/L require close monitoring. The prophylactic use of antibiotics and hemostatic drugs is recommended to mitigate the risk of infection and complications. For example, the BMI of STB patients was 18.5 kg/m2, the preoperative albumin level was 30 g/L, the operation method was combined surgical procedure, the intraoperative blood loss was 800 mL, the postoperative neutrophile granulocyte was 80 × 109/L, the direct bilirubin was 9 μmol/L, and the postoperative drainage volume was 400 mL. The predicted score for the occurrence of PSSH in this patient was 2 + 5 + 4 + 0 + 0 + 3 + 0 = 14. This patient is at a particularly high risk for PSSH, and medical staff should attach great importance to it and deal with it as soon as possible. In summary, the scoring system developed in this study provides healthcare workers with an efficient tool by integrating conventional laboratory indicators and clinical observation results, enabling them to identify high-risk individuals for PWH in STB patients after surgical procedure, optimize patient management strategies, and enhance the quality and efficiency of clinical decision-making.
This study had several advantages. First, we applied LASSO analysis and logistic regression to select the best predictors to construct a predictive model for PSSH in patients with STB. The AUC, sensitivity, and specificity of the model in the training set were 0.735, 0.703, and 0.685, respectively. The AUC, sensitivity, and specificity of the test set was 0.786, 0.878, and 0.588, respectively, thus indicating that the model had good discriminatory ability. Furthermore, the DCA curve demonstrated that the model has high clinical practicability. Second, we designed a new risk assessment tool (PSSHRS) to further develop a multicenter prospective validation model and then determined the predictive effect of the risk assessment tool for clinical scenarios. The AUC, sensitivity, and specificity of the external validation set were 0.846, 0.911, and 0.646, respectively. The prediction efficacy of the surface model was superior. Therefore, the predictive model developed in this study can provide healthcare professionals with a personalized clinical tool for the early identification of PSSH in patients with STB.
There are also some limitations to this study that need to be considered. First, our model was on the basis of retrospective analysis and cannot clearly determine specific intraoperative indicators, including complete abscess clearance. Furthermore, the sample size was limited and our analysis could have potentially included unconsidered risk factors. Second, the data in this study were collected from four hospitals, it is important to consider that there may have been differences between different surgeons and treatments, and the treatment plans of each group may not have been equivalent. In the future, homogenized longitudinal large-sample multi-center studies need to be carried out to provide a more precise reference for the further external verification of the clinical transformation and application effect of the model and exploration of intervention measures to promote wound healing.
Conclusions
In this study, we established a novel risk prediction model and assessment score for PSSH in patients with STB which exhibited good differentiation, calibration, and clinical practicability. In future, medical staff can quantitatively evaluate the risk of PSSH in patients with STB according to the actual clinical situation and utilize this model to provide effective prevention and treatment measures for high-risk patients in a timely manner. In addition, the model will enhance preoperative preparations, risk assessment and symptom management, operative precision, and provide early prevention post-surgical procedure. By using the new model, clinicians can formulate individualized treatment plans to prevent and treat PSSH at an early stage, thus reducing the risk of postoperative wound complications and improving the quality and safety of surgical procedure.
Footnotes
Acknowledgments
The authors are very grateful to the Department of Spine Orthopedic, the Second Affiliated Hospital of Guizhou Medical University for their help and support in this multi-center cohort study. The authors thank all the participants who participated in this study.
Authors’ Contributions
W.T. and G.X.P. contributed to project administration and article revision. Q.Y., Y.Z., and S.S.A. contributed to data curation. R.L. and Q.X. contributed to the investigation. J.L.W. wrote the original draft. All authors read and approved the final version of the article.
Ethics Approval and Consent to Participate
The study was conducted according to the guidelines of the Declaration of Helsinki and was achieved from the Institutional Review Board of the Affiliated Hospital of Guizhou Medical University, (Approval number: 2023 Trial No. 894), and each patient or their kin provided informed consent.
Consent for Publication
Each patient or their next-of-kin/family provided informed consent to participate.
Data Availability
All data generated or analyzed during this study are included in this published article. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This work is supported by Doctor Start-up Fund of Affiliated Hospital of Guizhou Medical University (gyfybskj-2023–07), Guizhou Provincial Science and Technology Projects (QKH-ZK[2024]222), the Science and Technology Fund of Guizhou Provincial Department of Health (GZWKJ2024-252, GZWKJ2024-158), and Nursing research project of Affiliated Hospital of Guizhou Medical University (gyfyhl-2023-A13) .
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.