
Abstract
Background:
Antibiotics within an hour of incision reduce the incidence of surgical site infection (SSI) in clean-contaminated abdominal surgery. However, patients undergoing emergency surgery for an intra-abdominal infectious process often receive treatment antibiotics and may not benefit from additional pre-incisional antibiotics (POA). We hypothesized that POA would not lead to a reduction in the occurrence of SSIs following emergency appendectomy.
Patients and Methods:
All patients at a single institution undergoing emergency appendectomies for acute appendicitis from 2013 to 2020 were included. Age, gender, perforation, body mass index (BMI), Elixhauser comorbidity index (ECI), surgical approach, emergency department antibiotics (EDA), EDA administration time, and pre-operative antibiotics were abstracted. Primary outcomes were superficial/deep and organ-space SSIs. Bi-variable logistic regression models assessed the independent impact of each tactic. Multi-variable models compared those receiving pre-incisional cefazolin with those receiving no POA.
Results:
Patients (n = 1380) had a mean age (standard deviation) of 39.5 (17.0) years, and 48.6% were female. Age, gender, perforated appendicitis, EDA, ECI, and BMI all were predictive of infection. POA were not predictive of SSI (p = 0.632). After adjustment for age, gender, perforation, EDA, EDA administration timing, ECI, and BMI, only perforation (odds ratio [OR]: 17.08, 95% confidence interval [CI] = 6.97–51.43) and male gender (OR: 2.75, 95% CI = 1.29–6.43) were associated with organ-space infection, whereas pre-incisional cefazolin was not (OR: 0.83, 95% CI = 0.38–1.97). Emergency department broad-spectrum antibiotics were associated with a lower incidence of superficial/deep infection (OR: 0.06, 95% CI = 0.00–0.68); however, pre-incisional cefazolin was not (OR: 0.71, 95% CI = 0.08–15.34).
Conclusion:
For patients undergoing emergency appendectomies who have received broad-spectrum antibiotic treatment, additional pre-incisional cefazolin does not reduce the incidence of superficial/deep or organ-space SSI.
Background
Pre-incisional antibiotic (POA) prophylaxis has been demonstrated in multiple randomized controlled trials and meta-analyses to reduce the risk of surgical site infections (SSIs) across different types of surgical procedures. 1 In addition to the burden placed on patients, SSIs burden the healthcare system through increased rates of readmissions and reoperations, increased cost of care, and overall increased morbidity and mortality. 2 Given that approximately 15% of all antibiotic agents in hospitals are prescribed for surgical prophylaxis,3,4 peri-operative antibiotic prescribing patterns can be a major contributor to antibiotic resistance, thereby further increasing healthcare costs. 5
In 2008, the World Health Organization Surgical Safety Checklist recommended administering pre-operative cefazolin within 60 min of surgical incision. 6 In 2013, joint guidelines for antibiotic prophylaxis in surgical procedures were revised and updated by the American Society of Health-System Pharmacists, Infectious Diseases Society of America, Surgical Infection Society, and Society for Healthcare Epidemiology of America 7 recommending prophylactic cefazolin for procedures involving entry into the lumen of gastrointestinal tract. 8 This was further supported by guidelines from the American College of Surgeons and Surgical Infections Society in 2016. 8 Although there are data suggesting the efficacy of certain antibiotics pre-incision, 9 current literature supporting cefazolin prophylaxis is limited in large part to obstetrics (cesarean section) and bariatric surgery.10,11 However, there have been no studies investigating cases of emergency surgery for intra-abdominal infectious processes, particularly where patients have already received broad-spectrum antibiotics for disease treatment.
Despite the lack of evidence for cefazolin’s efficacy as antibiotic prophylaxis for emergency appendectomy or colorectal surgical procedures, several studies have gone on to investigate the optimum timing of cefazolin prophylaxis. A study by Wu et al. concluded that the frequency of SSI after appendectomy was independent of the timing of administration of cefazolin and other antibiotics. 12 The authors did not, however, investigate the impact of foregoing additional antibiotics in the immediate peri-operative period. Institutional recommendations for surgical antibiotic prophylaxis for appendectomy are often based on recommendations created for elective colorectal surgery. To our knowledge, no study to date has examined the effect of pre-incisional cefazolin or pre-incision broad-spectrum antibiotics in addition to broad-spectrum antibiotics administered at presentation in the emergency department (ED) for an intra-abdominal infectious process on SSI.
In this retrospective study, the outcomes of patients who received pre-incisional cefazolin for emergency appendectomy compared with patients who did not receive POA were evaluated. The appendectomy procedure was chosen because of its high volume and relative homogeneity with respect to the disease process. Guidelines recommend a dose of cefazolin within 30 min of most elective abdominal surgeries.6,7,13 The effect of administering cefazolin within 30 min of incision on the rate of both superficial/deep and organ-space SSI was investigated. In our institution, a guideline recommending the addition of a pre-incisional dose of cefazolin for skin and gram-negative coverage in colon cases within an hour of surgery was implemented in early 2017. After this change, the use of pre-incisional cefazolin increased from just over half to nearly all appendectomies. The cefazolin dosing was based on weight. Any patient more than 40 kg was given 2 g, and if more than 120 kg, the dose was 3 g. For those less than 40 kg, dosing was by physician preference, either 1 or 2 g. It was hypothesized that POA would not lead to a reduction in the occurrence of SSIs following emergency appendectomy.
Patients and Methods
Study design
This is a retrospective cohort study using data from both campuses of a 1,541-bed quaternary care academic medical center between 2013 and 2020. Both campuses are staffed by the same group of surgeons. Data were abstracted from the electronic medical record. Institutional review board approval was obtained. This study is reported following the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 10 This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Inclusion and exclusion criteria
All patients undergoing emergency abdominal surgery, both open and laparoscopic, were identified by admission through the ED and underwent surgery within 24 h for a primary diagnosis of acute appendicitis. Uncomplicated appendicitis was defined as appendicitis without abscess or other clear evidence of perforation on imaging prior to operation. Patients were classified as having perforated appendicitis if this was described in the operative report or on pathologic examination of the specimen. Patients less than 18 years of age, those who died during the index hospitalization, and those patients who had their initial dose of antibiotics started within an hour of skin incision or who did not present for at least one outpatient follow-up visit were excluded from the study.
Extracted data points
Baseline parameters included demographics, comorbidities leading to the calculation of the Elixhauser comorbidity index (ECI, drug use, body mass index [BMI], obesity, weight loss, depression, arrhythmias, stroke, diabetes mellitus, hypertension, congestive heart failure, chronic pulmonary disease, cancer, renal failure, cirrhosis, and bleeding disorder), surgical indication, operative and pathologic findings, surgical technique (laparoscopic vs. open), and antibiotic coverage and administration timing. Patients were categorized based on when and where POA were administered. All antibiotic administration timing was calculated from the time of incision in minutes. POA were those given in the operating room within 30 min of skin incision. ED antibiotics (EDA) were those antibiotics given for treatment within 12 h of surgery but more than 60 min before skin incision. Antibiotics were further categorized into broad spectrum, narrow spectrum, and, in the case of POA, cefazolin only. Narrow-spectrum antibiotics were defined as single or combination antibiotics that did not cover gram-positive, gram-negative, and anaerobic bacteria. These included ciprofloxacin, ceftriaxone, cefazolin, metronidazole, gentamicin, clindamycin, vancomycin, ampicillin, cefuroxime, oxacillin, and ceftazidime. Broad-spectrum antibiotics were defined as single or combination antibiotics covering gram-negative, gram-positive, and anaerobic bacteria. These included piperacillin–tazobactam, ampicillin–sulbactam, cefoxitin, cefotetan, gentamicin–metronidazole, gentamicin–clindamycin, metronidazole–ciprofloxacin, metronidazole–cefazolin, metronidazole–clindamycin, and metronidazole–ceftriaxone. The primary outcome was SSI including superficial, deep, and organ-space SSIs as defined by the Center for Disease Control’s National Healthcare Safety Network. 14 Because of the infrequent nature of deep SSI, these were combined with superficial SSI.
Statistical analysis
The incidence of SSI in patients receiving pre-incisional cefazolin, pre-incisional broad-spectrum antibiotics, or no POA was compared. Bi-variable comparisons were made between each of the presumed SSI risk factors and the outcome using chi-square or Student’s t-test where appropriate. We also assessed the timing of EDA relative to the surgical incision. Multi-variable logistic regression models were created using these same risk factors to assess the independent impact of each antibiotic tactic. Our primary model assessed the impact of pre-incisional cefazolin compared with those receiving no POA. Continuous parameters are reported as medians and interquartile ranges, whereas categorical parameters are reported as percentages. All statistical analyses were carried out using R: A language and environment for statistical computing version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org/).
Results
After a review of the EMR, 1,380 patients were identified who underwent emergency surgical intervention for acute appendicitis. The mean age was 39.5 years, and 48.6% were female. All patients underwent attempted laparoscopic appendectomy, with 5.8% being converted to open. Most patients received broad-spectrum EDA and pre-operative cefazolin. Complete patient characteristics are presented in Table 1. Complete outcome data were available for 1,328 patients who followed up at least one time at seven days post-operatively or later (Fig. 1). Following a bi-variable comparison, age, gender, perforated appendicitis, EDA, ECI, and BMI were associated with infection (Table 2). POA and timing of EDA were not predictive of superficial/deep or organ-space SSI (p values of 0.632 and 0.193, respectively). After adjustment for confounders, only perforation (odds ratio [OR]: 17.08, 95% confidence interval [CI] = 6.97–51.43) and male gender (OR: 2.75, 95% CI = 1.29–6.43) were associated with organ-space infection (Table 3). Broad-spectrum EDA were associated with a lower incidence of superficial/deep infection (OR: 0.06, 95% CI = 0.00–0.68); however, pre-incisional cefazolin was not (OR: 0.71, 95% CI = 0.08–15.34). Although time from EDA administration to surgery was not found to be associated with infection, there was a trend with those patients experiencing superficial/deep infections having shorter times between administration and incision (Table 4).
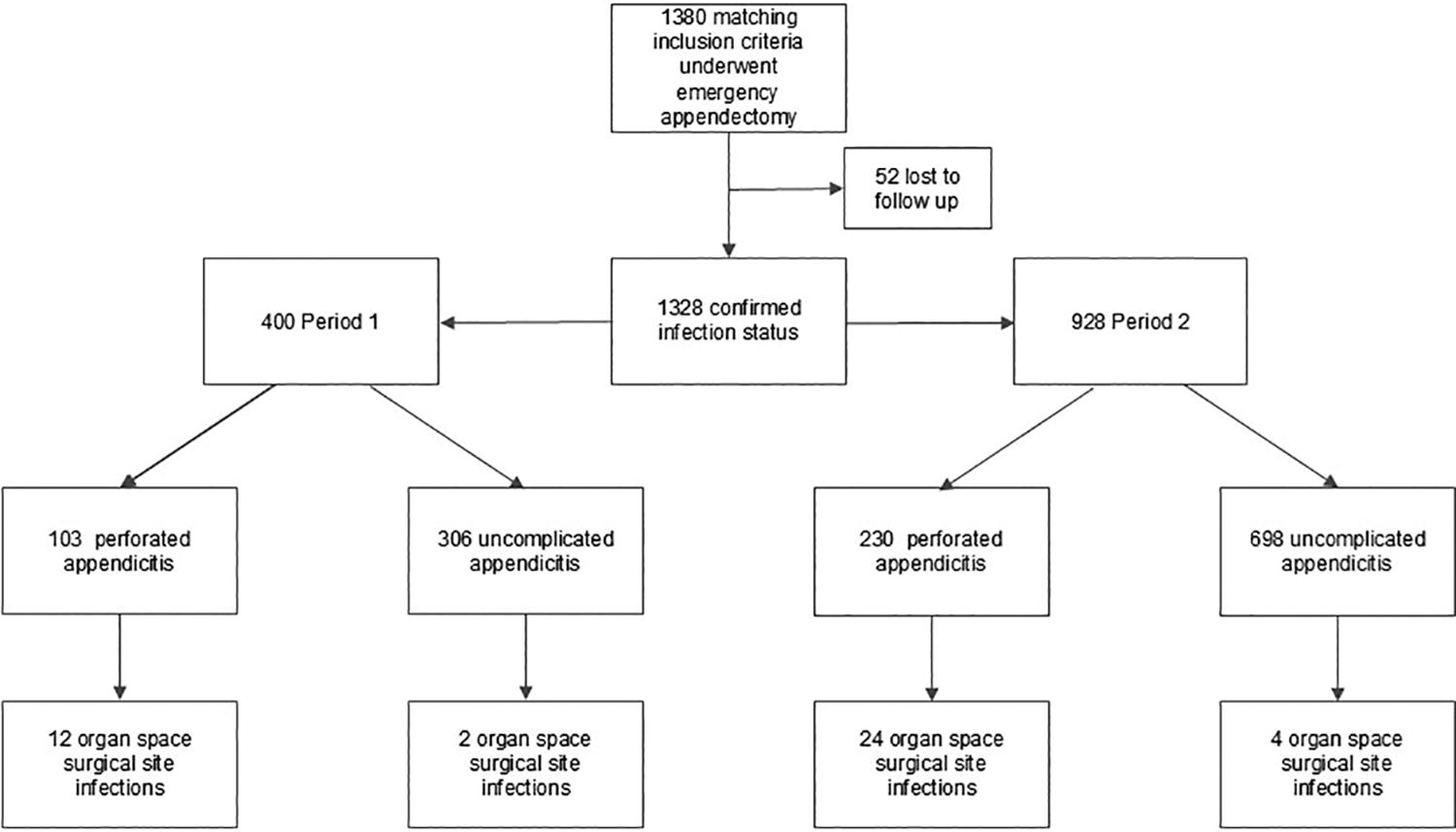
Patient flowchart. Period 1 was from February 2013 to December 2016. Period 2 was from January 2017 to December 2020.
Patient Characteristics
Patients who received other pre-incisional antibiotics in addition to cefazolin or instead of cefazolin are not included in the table.
ED = emergency department; SD = standard deviation; BMI = body mass index; COPD = chronic obstructive pulmonary disease.
Unadjusted Comparison of Baseline Parameters and Outcomes
SD = standard deviation; ED = emergency department.
Factors Associated with Organ-Space and Superficial/Deep Infection Using Multi-Variable Logistic Regression Analysis
CI = confidence interval; ECI = Elixhauser comorbidity index; BMI = body mass index; EDA = emergency department antibiotics.
Antibiotic Administration Timing in Minutes Prior to Incision
SSI = surgical site infection; EDA = emergency department antibiotics.
Discussion
Following a policy change recommending pre-incisional cefazolin for emergency abdominal surgery, we found no evidence that this additional dose of cefazolin reduces the risk of SSI in patients undergoing appendectomy for acute appendicitis. This was irrespective of the time between antibiotics received in the ED at the time of diagnosis and surgery and the antimicrobial coverage provided by those EDAs. We did demonstrate that antibiotics given in the ED were associated with a reduced risk for superficial SSI. However, the timing of broad-spectrum EDA administration was not found to be a significant predictor of SSI. Perforation was found to be the strongest predictor of SSI, which is expected given the resulting contamination of the abdominal cavity from intraluminal contents and demonstrated by multiple investigators.11,15,16
SSIs have profound implications for both patients and healthcare systems. They currently stand out as the most prevalent and economically burdensome among all hospital-acquired infections, constituting 20% of such cases. 8 Associated with a 2- to 11-fold increase in mortality risk, SSIs extend hospital stays by an average of 9.7 days, leading to additional expenses exceeding $20,000 per admission. 8 When extrapolated, the estimated annual occurrence of SSIs ranges from 160,000 to 300,000 in the United States, correlating with estimated annual costs ranging from $3.5 to $10 billion. 17 Given that a significant proportion of SSIs may be preventable through evidence-based measures, addressing SSI has emerged as a key target for research. One avenue of reducing SSI occurrence involves the use of prophylactic antibiotics. As described previously, cefazolin has proved to be effective antibiotic prophylaxis in bariatric surgery procedures, 18 cesarean section deliveries, 19 as well as lumbar fusions, 6 and specifically gastric bypass. 20 In the case of emergency intra-abdominal procedures, studies have examined the timing of cefazolin administration 12 as well as prophylactic parental antibiotic combinations. 21 Additional studies have concentrated on pinpointing a more accurate and optimal timeframe for prophylactic antibiotic administration. Unfortunately, the findings have been divergent. Although some advocate for particular administration windows,22,23 others demonstrate no statistically significant differences in SSIs with more precise timing. 14
Unlike elective surgery, no study has yet to examine pre-incisional cefazolin’s efficacy in the case of emergency intra-abdominal procedures, particularly in cases where broad-spectrum coverage was administered in the ED prior to surgery and within two to three half-lives, ensuring adequate circulating levels of the antibiotics. Despite this lack of evidence, institutions may recommend cefazolin use prior to emergency abdominal surgery based on the evidence from studies of elective surgery. The results from this study are significant as they provide evidence of cefazolin’s lack of efficacy for emergency appendectomy when the patient has received broad-spectrum antibiotics in the ED. By limiting usage of cefazolin in these patients, surgeons can support good antibiotic stewardship and potentially reduce antibiotic resistance. Other antibiotic complications, including Clostridium difficile infection, may also be reduced by eliminating additional POA. Additionally, foregoing pre-incisional cefazolin can contribute to decreasing healthcare costs. Although inexpensive at about US $7 per 2 g dose, given the volume of appendectomies in the United States, about 300,000 per year, this leads to a cost savings of about 2.1 million dollars annually. 24
The findings of this study are limited by its retrospective design; there may be a subgroup of patients who would benefit from the addition of pre-incisional cefazolin, but our data would be unable to identify these patients. Additionally, the association between EDA timing and SSI does not adjust for different antibiotic half-lives, as all EDA are grouped together, although the majority of EDA consisted of ceftriaxone and metronidazole. Because few patients received an anaerobic antibiotic POA, we cannot draw conclusions on this complete broad-spectrum approach. We also are limited by a lack of control of other factors including the time from ED presentation to the administration of ED antibiotics and post-operative treatment paradigms that were followed. Because the vast majority of patients were given broad-spectrum antibiotics at the time of diagnosis, we are also unable to draw any conclusions regarding those patients who fail to receive antibiotics in the ED. Collection of SSI data, particularly superficial SSI, may also be difficult retrospectively; however, we used well-established definitions for these when applied retrospectively. 25 Because of the retrospective nature of this study, a consistent, specific follow-up period was not possible; however, the majority of first post-op visits occurred between 1 and 3 weeks. Additionally, the per-protocol analysis introduces potential attrition bias. If patients followed up outside the health system, some infections may have been missed; however, it is unlikely that there would have been enough of these cases to have altered our findings. As the data collected for this study came from one institution, results may not be generalizable.
Conclusion
In conclusion, for patients undergoing emergency appendectomies who have received broad-spectrum antibiotic treatment in the ED, additional pre-incisional cefazolin is unlikely to reduce the incidence of superficial or organ-space SSI. Further studies in the form of randomized controlled trials are warranted to further scrutinize the efficacy of pre-incisional cefazolin in emergency appendectomy patients to not only allow for better care of this population but also to improve antibiotic stewardship practices and conservation of hospital resources.
Footnotes
Authors’ Contributions
A.H.: Methodology, validation, investigation, data curation, writing—original draft, writing—review and editing, and visualization. A.K.: Conceptualization, methodology, investigation, and writing—review and editing. A.A.M.: Conceptualization, methodology, validation, writing—review and editing, and supervision. B.B.: Conceptualization, methodology, validation, writing—review and editing, and supervision. K.A.D.: Conceptualization, methodology, validation, investigation, writing—original draft, writing—review and editing, and supervision. K.M.S.: Conceptualization, methodology, validation, investigation, data curation, writing—original draft, writing—review and editing, visualization, and supervision.
Funding Information
No funding was accepted for the study.
Author Disclosure Statement
The authors have no conflicts of interest to declare.