
Abstract
Background:
Surgical site infections (SSIs) have a significant health economic burden, accounting for more than US $3.3 billion in costs, and lead to increased microbial resistance, prolonged hospital stays, elevated 30-day mortality rates, greater incidences of reoperation, and decreased quality of life. Recently, evidence has emerged suggesting that prophylactic closed incision negative pressure wound therapy (ciNPWT) may substantially reduce the risk of post-operative wound complications, specifically SSIs. This study aimed to evaluate whether ciNPWT is cost-effective compared with routine incision care for the prevention of superficial SSIs.
Hypothesis:
We hypothesized that ciNPWT is cost-effective compared with routine incision care for the prevention of superficial SSIs.
Methods:
A cost-effectiveness decision analytic model was created comparing the use and non-use of ciNPWT. Superficial SSI probabilities, cost of care for patients with and without post-operative infection, and quality of life Short Form (SF)-36 survey data were obtained from a literature review. Cost of ciNPWT was obtained from health administrative data. A decision tree was constructed using TreeAge Software Pro Version 2020 (TreeAge Software, Inc., Williamstown, MA). Deterministic and probabilistic sensitivity analyses were performed to evaluate the robustness and reliability of the model.
Results:
One-way sensitivity analysis with a willingness-to-pay threshold of $5,000 demonstrated that above a baseline infection rate of approximately 6.4%, ciNPWT is cost-effective at reducing superficial SSI. Probabilistic sensitivity analysis indicated that even with uncertainty present in the parameters analyzed, the majority of simulations (95.4%) favored ciNPWT as the more effective tactic.
Conclusions:
Despite the added device cost, ciNPWT is cost-effective for superficial SSI prevention across a variety of surgical infection risk profiles.
Background
Surgical site infections (SSIs) have a significant health economic burden, accounting for more than US $3.3 billion in costs annually, and lead to prolonged hospital stays, elevated 30-day mortality rates, greater incidences of reoperation, and decreased quality of life. 1 In 2016, the World Health Organization (WHO) identified prevention of SSIs as an international high priority and published recommendations for a wide range of risk-reducing perioperative interventions. 2 Both the 2016 and 2018 editions of the WHO global guidelines conditionally recommended prophylactic use of closed incision negative pressure wound therapy (ciNPWT) for SSI prevention, despite noting overall low-quality evidence and lack of consensus with other national/specialty guidelines.3,4 At least tentative recommendations have similarly been made by the World Society of Emergency Surgery, the Japan Society for Surgical Infection, the American College of Surgeons, and a joint recommendation from the Society for Healthcare Epidemiology and the Infectious Diseases Society of America.5–8
Recently, ciNPWT has been the subject of multiple randomized controlled trials, systematic reviews, and meta-analyses with accumulating moderate-to-high certainty evidence for its efficacy in SSI prevention.9–13 The latest Cochrane Review shows a relative risk reduction in superficial SSI of 0.70 (95% confidence interval [CI]: 0.53–0.92) with prophylactic ciNPWT application compared with standard dressings. 14 Similar results were also reported by James et al. (2024), who found a statistically significant improvement in superficial SSI outcomes for patients receiving ciNPWT (odds ratio [OR]: 0.30; 95% CI: 0.17–0.53) in a recent large meta-analysis. 15 Despite this evidence for clinical benefit, routine use of ciNPWT is not standard practice for many surgeons. We believe that a lack of robust cost-efficacy data may contribute to inconsistent implementation.
Inherent cost differences between ciNPWT and standard surgical dressings, as well as risk-stratified variation in clinical effectiveness data, highlight a critical need to identify groups of patients in whom this intervention is cost-effective. Thus, the purpose of this study was to assess the cost-effectiveness of ciNPWT compared with standard dressings for SSI prevention across a range of baseline infection rates, using the most up-to-date meta-analytic data. We hypothesized that use of ciNPWT would reduce healthcare costs in patients with a high baseline risk of superficial SSI.
Methods
A cost-effectiveness model was created from the perspective of a healthcare administrator. The model evaluates the development of superficial SSI at 30 days for two clinical pathways as follows: (1) with ciNPWT and (2) without ciNPWT. The model also assumes that all incisions are closed primarily regardless of contamination even if ciNPWT is not used. Modeling ciNPWT compared with open wounds designed to close by secondary intent (regardless of augmentation by other forms of NPWT) is beyond the scope of this study.
All data included in the model are listed in Table 1. The model assumes a baseline superficial SSI rate of 15% with a range from 1% to 30%, reflecting a surgical cohort with wide range of superficial SSI risk. Modulating this baseline superficial SSI rate is the primary way that the model evaluates differing levels of infection “risk” with low-risk patients/wounds corresponding to low baseline infection rates (clean cases, etc.) and high-risk patients corresponding to greater baseline rates (dirty/infected wounds, etc.). We chose to model the risk of infection directly rather than using subjective wound classifications. The ORs reflecting the use of ciNPWT on 30-day superficial SSI were taken from the James et al. meta-analysis. 15 The probability of superficial SSI in patients with ciNPWT was modeled by converting baseline infection rates into odds, multiplying the resulting new odds by the ciNPWT OR, and then converting back to a probability. 16 Cost of ciNPWT was the acquisition cost for the ciNPWT system used at our institution (3M™ Prevena™ Incision Management System). The model assumes that the cost of a “standard” dressing is negligible. Costs of managing superficial SSI were taken from published literature and inflated to 2024 dollars.17,18 Considering that data on quality adjusted life years for superficial SSIs are limited, published data using the physical component of the SF-36 for patients with and without superficial SSI were used to model effectiveness. 19 For the purposes of the analysis, the authors calculated ranges of ±5% for the SF-36 values. Differences in the SF-36 of 4–7 points are considered a reasonable threshold for minimal clinically important difference. 20
Model Parameters
Range estimates are ±5%.
SSI = surgical site infection; ciNPWT = closed incision negative pressure wound therapy.
The model is illustrated in Figure 1. The model was constructed using TreeAge Software Pro Version 2020 (TreeAge Software, Inc., Williamstown, MA). Cost-effectiveness analysis was conducted, with one- and two-way sensitivity analyses performed on superficial SSI rate and the OR for ciNPWT. Probabilistic sensitivity analysis was conducted, and cost-effectiveness was assessed at $5,000 and $50,000 willingness-to-pay (WTP) thresholds. 16 Because of uncertainty related to scarcity of evidence for model inputs, all parameters in probabilistic sensitivity analyses were assumed to have a uniform underlying distribution, therefore making any value within the range as likely as any other. In addition, the model was created assuming that ciNPWT would not increase wound infection rates; therefore, the OR for ciNPWT was allowed to range from 0 to 1, but not above 1. This range is far outside of the bounds of ORs reported by the reference meta-analysis. 15 This choice allows us to determine the OR threshold below, which ciNPWT might be cost-effective, even if this threshold is outside of that reported in the literature.
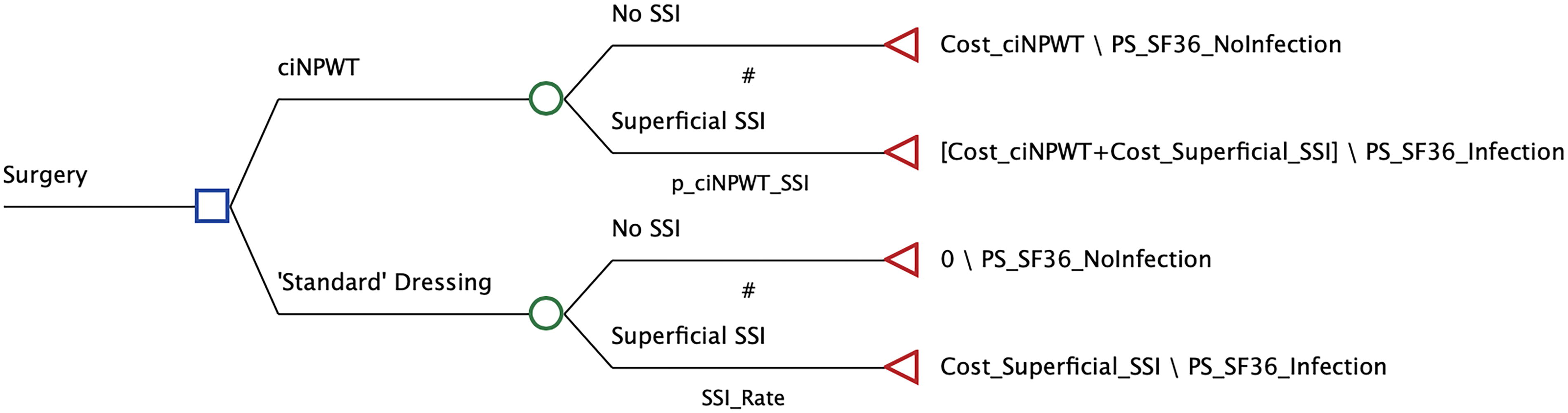
Cost-effectiveness model.
Results
Base case decision analysis identified ciNPWT as the optimal tactic. With an average cost of $1,532.29 and average SF-36 score of 46.81, ciNPWT was both less expensive and more effective than (“dominant” over) standard dressings ($2,930.49 and 46.40). Probabilistic sensitivity analysis of 100,000 iterations demonstrated that ciNPWT was the optimal tactic in 95.4% of cases at a WTP threshold of $5,000 and 99.7% at a WTP threshold of $50,000. A scatterplot of the incremental cost-effectiveness as calculated by probabilistic sensitivity analysis is included as Figure 2.

Incremental cost effectiveness scatterplot for ciNPWT versus “standard” dressing at WTP = $5,000. Points on scatterplot represent results from probabilistic sensitivity analysis for ciNPWT using “standard” dressing as the baseline. The ellipse represents the 95% confidence interval for the analysis. Dark gray = ciNPWT is the optimal tactic. Light gray = ciNPWT is not the optimal tactic. ciNPWT = closed incision negative pressure wound therapy; WTP = willingness to pay.
One-way sensitivity analysis of SSI rate demonstrated that ciNPWT was the most cost-effective option above an infection rate of 6.4% at a WTP threshold of $5,000 and 5.3% at a WTP threshold of $50,000 (Fig. 3 for WTP $5,000). One-way sensitivity analysis of the OR for SSI with ciNPWT demonstrated that ciNPWT was the more cost-effective option below ORs of 0.89 and 0.98 at WTP thresholds of $5,000 and $50,000, respectively (Fig. 4 for WTP $5,000). One-way sensitivity analyses conducted at the $50,000 threshold are shown in Supplementary Figures S1 and Figure S2.
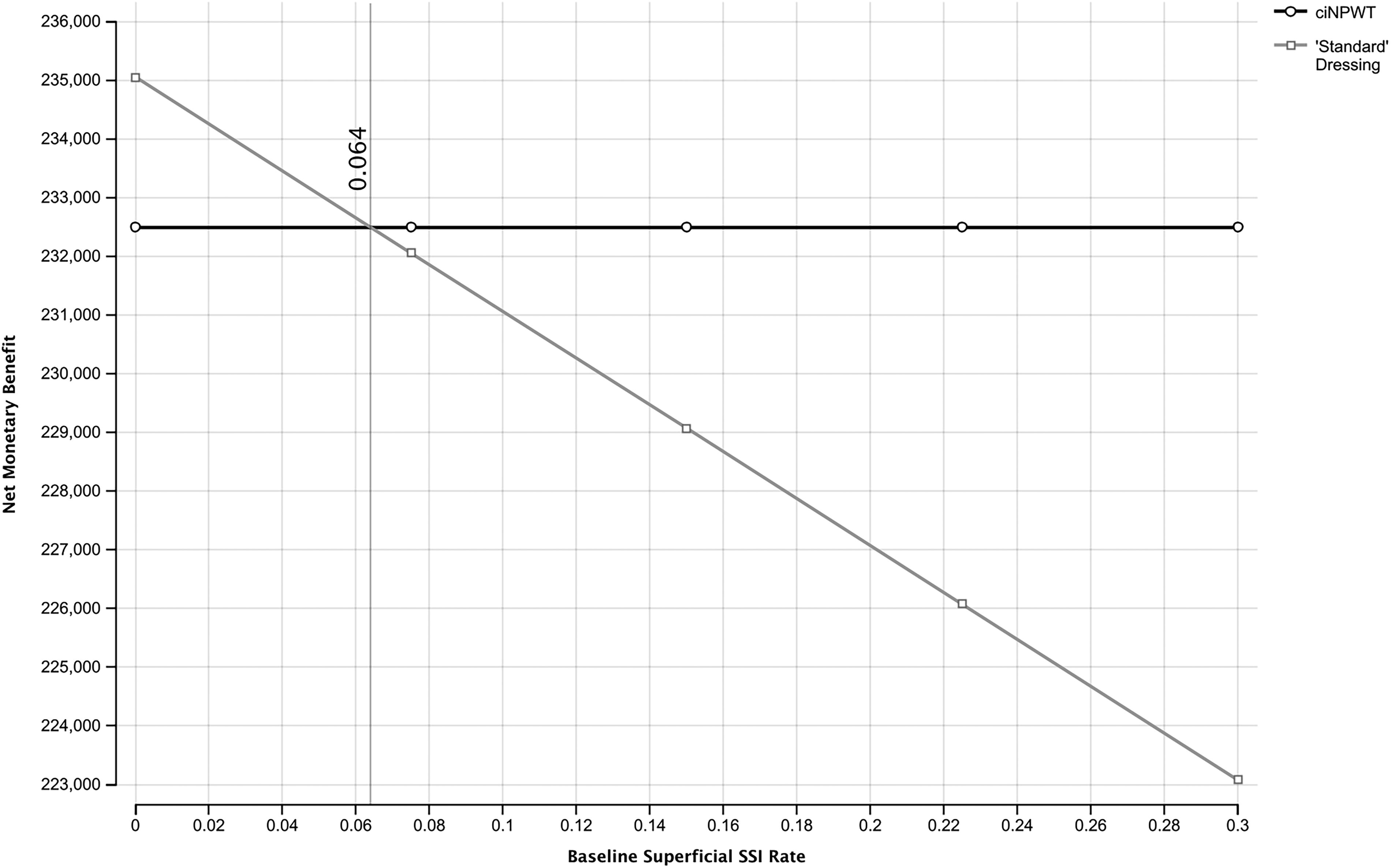
One-way sensitivity analysis for superficial SSI rate at WTP = $5,000. SSI = surgical site infection; WTP = willingness to pay.
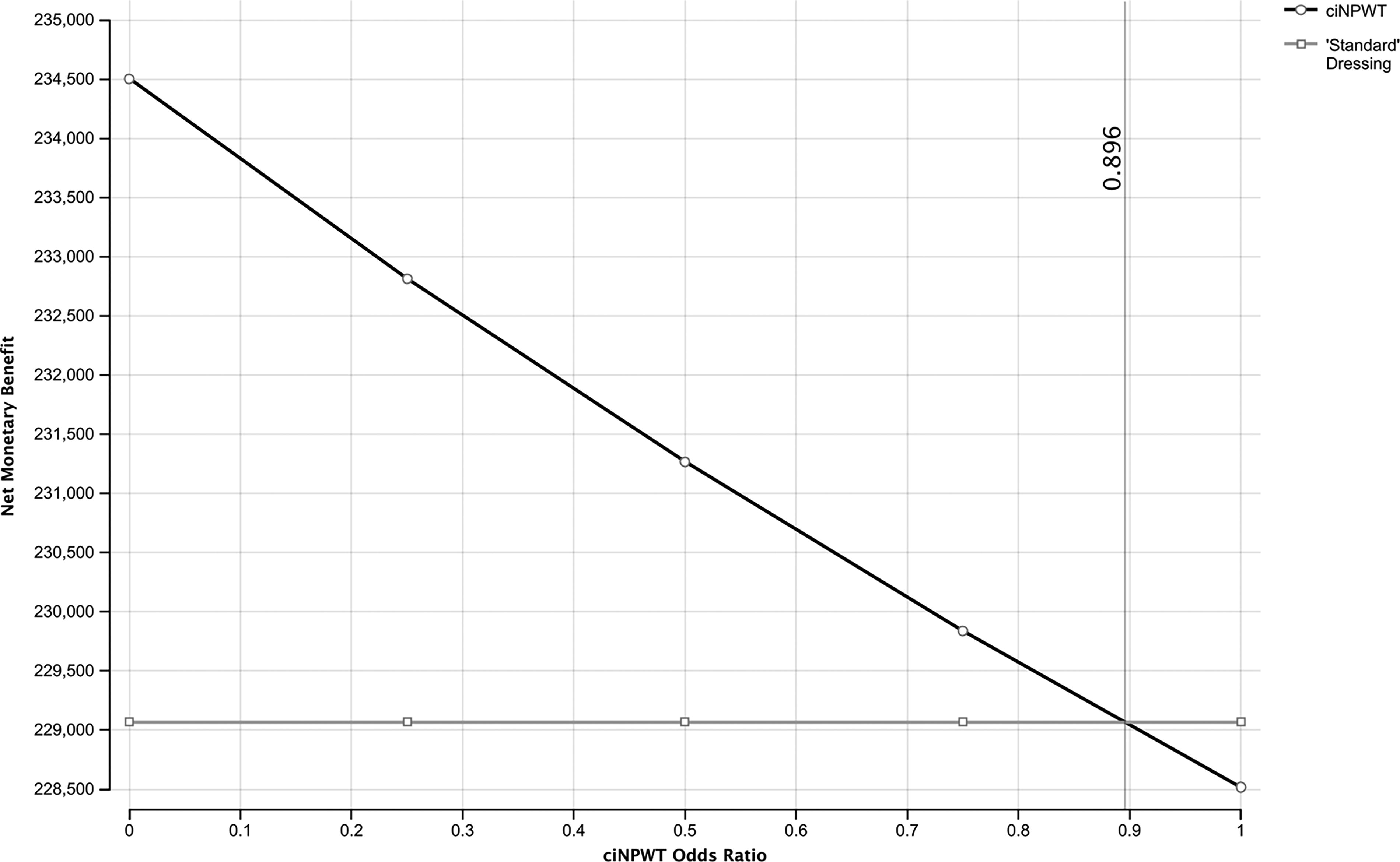
One-way sensitivity analysis for ciNPWT odds ratio at WTP = $5,000. ciNPWT = closed incision negative pressure wound therapy; WTP = willingness to pay.
The interaction between SSI rate and the OR for ciNPWT is illustrated in the two-way sensitivity analyses at the WTP thresholds of $5,000 and $50,000 (Fig. 5 for WTP $5,000). In both WTP scenarios, the likelihood of ciNPWT being the optimal tactic increases as baseline infection rate increases, even as the effectiveness of ciNPWT decreases, as described by an increasing OR. The two-way sensitivity analysis conducted at the $50,000 threshold is included in Supplementary Figure S3.

Two-way sensitivity analysis for baseline SSI rate and ciNPWT odds ratio at WTP = $5,000. SSI = surgical site infection; ciNPWT = closed incision negative pressure wound therapy; WTP = willingness to pay.
Discussion
The results of this study suggest that ciNPWT is a cost-effective tactic for reducing superficial SSIs across a wide range of baseline infection rates and, therefore, a wide range of surgical populations. Surprisingly, our model was not sensitive to changes in WTP, providing similar outcomes at both the $5,000 and $50,000 thresholds. According to our model, at a WTP threshold of $5,000, ciNPWT was the preferred option when the baseline rate of superficial SSI was above 6.4% and the OR of SSI for ciNPWT was below 0.89.
The purpose of cost-effectiveness analysis is to “determine if the value of an intervention justifies its cost.” 21 When an intervention both improves outcomes and results in lower overall costs than a comparator, the intervention is considered economically “dominant.” 22 In our model, ciNPWT improves outcomes by lowering superficial SSI rates. Although this improvement comes at an increased initial cost for the device itself, the resulting cost savings from reduced infection rates more than make up for the device cost, resulting in ciNPWT being the “dominant” tactic.
Sensitivity analysis in these models is a valuable tool for evaluating the intervention. Model parameters can be allowed to take on a wide range of values, allowing the intervention to be evaluated under a variety of potential cases and limiting the impact of uncertainty in the parameters being evaluated. Sensitivity analysis can also help to answer practical questions about how to apply the intervention. In our study, we use sensitivity analysis to answer two simple questions as follows: (1) above what baseline infection rate is it potentially beneficial to use ciNPWT? and (2) how poorly can ciNPWT function and still be of value? We, therefore, seek to define practical constraints/limitations on the baseline infection rate and OR for superficial SSI reduction.
Our model suggests that this intervention is cost-effective above a minimum baseline risk of superficial SSI (6.4% in our study). Hyldig et al. found ciNPWT to reduce SSI rates from 9.2% to 4.2% in a population of obese patients undergoing cesarean delivery. 11 Similarly, a recent meta-analysis of vascular groin wounds (baseline SSI rate 18%−42%) found ciNPWT to be effective at reducing SSI. 23 In operative groups with low baseline SSI risk, studies have not found ciNPWT to be cost-effective. Hawkins et al. found that ciNPWT was not cost-effective at reducing the rate of superficial SSI in cardiac operation for a population with a baseline infection rate of 0.9%. 24 Png et al. similarly found ciNPWT not cost-effective in an orthopedic surgical procedure setting. In their study, approximately 5.7% of the overall population was provided antibiotic agents for presumed SSI. 25 In contrast, Nherera et al. found ciNPWT cost-effective at a baseline complication rate of 4.8% 26 in their model, including all surgical site complications. However, costs and effectiveness in their model included downstream readmissions and mortality, which may account for the favorable profile. Because of the general consistency of results in the literature, we believe that the cost-effectiveness of this intervention is unlikely to vary widely across different types of operation for reasons unrelated to baseline variability in SSI rates. 27
Literature review of ciNPWT returns a fairly wide range of ORs for superficial SSI reduction with ciNPWT. 15 To account for this uncertainty in sensitivity analysis, we allowed our OR for superficial SSI reduction to range from 0 to 1 under an assumption that this therapy would not increase infection rates. We found that the upward constraint on the OR in our model is 0.89 at a WTP threshold of $5,000 and 0.98 at a $50,000 WTP threshold. This means that at the current acquisition cost, ciNPWT needs only slightly reduced SSI rates to still be cost-effective. These upward constraints are significantly greater than pooled estimates from the clinical literature. 15 Although exact thresholds will be expected to vary from model to model, our findings suggest that even if ciNPWT is somewhat less effective than pooled data would suggest, it is still likely to be of high economic value under typical thresholds for WTP.
The recent SUNRISE trial is a large multicenter randomized trial of ciNPWT in patients undergoing emergent laparotomies. The authors randomized 840 patients to either ciNPWT versus surgeon preference for wound dressing and found no difference in superficial SSI rate. 28 Although not directly reported in the article, infection rates for each wound classification are calculable based on the data provided. These overall rates were high ranging from 21.3% overall in clean cases to 41.6% overall in dirty/infected cases. 28 Although these rates are not that dissimilar from the 28.3% (clean) and 35.8% (dirty) SSI rates observed in the ROSSINI trial, they are significantly greater than observed infection rates in trauma and emergency general surgical procedure.29–31 These rates are also greater than the SSI rates observed in the STOP-IT trial, even after excluding patients who only underwent percutaneous intervention. 32 It remains to be seen if these results persist on repeat study. Including the SUNRISE trial in future meta-analyses will serve to increase the pooled OR. A benefit of our study is that the sensitivity analysis ranged up to 1 in anticipation of the true effect of ciNPWT being potentially worse than previously reported. Our study suggests that depending on the WTP, the true OR can range between 0.89 and 0.98 and still be cost-effective.
Leaving the skin open to heal by secondary intention has been a long-practiced method of minimizing infection risk for patients who are deemed to be either at high risk for infection (because of contamination, immunosuppression, or other factors) or inability to tolerate a future infection. Although the infection risk for a contaminated wound may be high, an infection does not develop in most patients.30,31 Wound healing by secondary intention may avoid the superficial SSI, but this practice comes at the cost of increased hospital length of stay, increased number of outpatient office visits, and a substantial negative patient experience.30,33 Recent interest in ciNPWT is one method of potentially increasing the number of patients whose skin can remain intact after operation. A recent survey of Surgical Infection Society members suggested that 30% of providers would still close the skin of a dirty/infected case with most of these surgeons choosing ciNPWT. 34 We do not suggest that all wounds should be closed. Physician judgment should continue to dictate whether it is safe to close a particular patient’s wound or not. However, if the surgeon believes that it is safe to close the wound, our study suggests that ciNPWT may be a reasonably cost-effective adjunct in many cases.
This study has several limitations. Probability parameters were based on meta-analyses, which suffer from the inherent limitation of pooling data gathered from sources with varied methodology. In addition, cost estimates were taken from acquisition costs from our institution, which may not be generalizable to other settings. Because our model assumes the perspective of a healthcare administrator, it incorporates and reflects hospital costs rather than patient charges. Finally, this model did not consider the effect of ciNPWT on complications other than superficial SSI. Although some studies have shown decreased rates of dehiscence, seroma, and hematoma with ciNPWT use compared with standard dressings, incorporating these outcomes was beyond the scope of this model. 35 However, ignoring these additional possible benefits only underestimates the cost-effectiveness of ciNPWT.
Conclusions
Despite the added cost of the device, ciNPWT is likely to be cost-effective and even cost saving for superficial SSI prevention across a variety of surgical infection risk rates. Our data suggest that ciNPWT should be considered for any closed wound with a baseline infection risk of greater than approximately 6%.
Footnotes
Authors’ Contributions
Conceptualization: C.A.G. Methodology: C.A.G., L.T.K., and K.A.V. Formal analysis: C.A.G., L.T.K., and K.A.V. Investigation: All authors. Writing: L.T.K. and C.A.G. Editing and review: All authors. Visualization: C.A.G.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. For the remaining authors, no conflicts of interest were declared.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.