
Abstract
Background:
Broad-spectrum antibiotic agents are utilized for complicated intra-abdominal infection (cIAI); however, the need for empiric methicillin-resistant Staphylococcus aureus (MRSA) coverage is not clear as the incidence of MRSA cIAI is rare.
Patients and Methods:
A single-center, retrospective, pre- and post-cohort study of adults admitted to the surgical intensive care unit (SICU) with cIAI between March 1, 2021, to May 1, 2023, was conducted. Historically, the SICU utilized vancomycin for all cIAI; however, in April 2022, the preferred regimen was changed to either piperacillin-tazobactam with vancomycin added for patients with MRSA risk factors or for Enterococcus spp. coverage in cefepime- or levofloxacin-based regimens for penicillin-allergic patients. The primary outcome was number of vancomycin days of therapy (DOT) per 1,000 patient days. Categoric and continuous variables were analyzed with chi-square and Fisher exact tests.
Results:
A total of 142 SICU encounters were included, 64 in the pre-cohort and 78 in the post-cohort. There was no difference in median vancomycin DOT per 1,000 patient days (14 days [interquartile range or IQR 5–21]; 16 days [IQR 8–17] p = 0.522) between the pre- and post-cohort. There was a significant reduction in the number of patients given vancomycin after the protocol change (90.6%; 76.9%, p = 0.042). A significant increase in piperacillin-tazobactam exposure was also observed (48.4%; 82.1%, p < 0.001) in the post-cohort aligning with our institutional practice change.
Conclusions:
In critically ill surgical patients with cIAI, the implementation of an antimicrobial stewardship guideline did not reduce vancomycin DOT per 1,000 patient days, however, it did result in a significant reduction in vancomycin exposure.
Background
Complicated intra-abdominal infections (cIAIs) represent the second-most common cause of infectious morbidity and mortality in the intensive care unit (ICU) and can be a surgical emergency. 1 These infections are associated with mortality rates ranging from 24% to 36%.2,3 cIAI is defined as an infection of the abdominal cavity that extends beyond the hollow viscus of origin into the peritoneal space and is associated with abscess formation or peritonitis.4–6 Standard treatment of cIAI is two-fold: early antimicrobial agent therapy and appropriate source control.4–7 Antimicrobial agent therapy should be broad, as cIAIs are often polymicrobial with specific organisms varying on the basis of the source of infection. Common isolates from cIAI include Escherichia coli (36.8%), Enterococcus spp. (25.9%), Staphylococcus aureus (3.2%), and anaerobes (11.7%).2,4,8
The 2024 Surgical Infection Society guidelines for the management of cIAI suggest against the use of vancomycin for empiric therapy, whereas the Infectious Disease Society of America (IDSA) and World Society of Emergency Surgery guidelines recommend vancomycin as an option for treatment of Enterococcus spp. or in patients at risk for methicillin-resistant S. aureus (MRSA) infection.4,5,9 However, most empiric regimens for cIAI cover Enterococcus spp. without the need for vancomycin, and the incidence of MRSA cIAI is rare (1%−3.1%).2,10,11 This begs the question as to whether empiric vancomycin should be used for cIAI.
In 2022, the surgical ICU (SICU) implemented a protocol change to limit the use of empiric vancomycin for cIAI to patients at high risk for MRSA infections or on a cefepime- or levofloxacin-based regimen for Enterococcus spp. coverage. Therefore, the aim of this study was to examine the use of vancomycin and other antibiotic agents for SICU patients before and after the protocol change. We hypothesized that this change would result in a decrease in vancomycin days of therapy (DOT) per 1,000 patient days.
Patients and Methods
We conducted a single-center, retrospective, pre- and post-cohort study at an 864-bed quaternary academic medical center and American College of Surgeons Level-1 Trauma Center. The study was approved by the Institutional Review Board. All adult patients admitted to the SICU with a cIAI between March 1, 2021, and May 1, 2023, were included. Patients with cIAI were identified by the International Classification of Diseases, Tenth Edition (ICD-10) and Current Procedural Terminology (CPT) codes associated with intra-abdominal procedures and peritonitis (Supplementary Table S1). The diagnosis of cIAI was confirmed through chart review. Patients were divided into two cohorts on the basis of their admission date to the SICU. The antimicrobial agent protocol to limit the use of vancomycin to high-risk patients was implemented on April 1, 2022. Patients admitted between March 1, 2021, and March 31, 2022, were in the pre-cohort and admissions between May 1, 2022, and May 1, 2023, were in the post-cohort. The month of April in 2022 was used as a washout period.
Historically, the SICU had utilized a rotation of empiric antibiotic agent regimens, including vancomycin and meropenem; vancomycin, cefepime, and metronidazole; or vancomycin, levofloxacin, and metronidazole for cIAI. Of note, linezolid was not routinely utilized in the SICU for cIAI. In April 2022, the SICU antimicrobial stewardship guideline updated the preferred antibiotic agent for cIAI to piperacillin-tazobactam monotherapy. Empiric vancomycin therapy would be considered if a patient had risk factors for MRSA, such as an immunocompromised state, previous culture with MRSA, or extensive healthcare exposure in the past 90 days.4,6 Empiric vancomycin could also be added for Enterococcus spp. coverage when using cefepime or levofloxacin with metronidazole for patients with severe penicillin allergies. Severe penicillin allergies were defined as history of anaphylaxis, disseminated hives, shortness of breath/wheezing/coughing, a history of Stevens–Johnson syndrome, toxic epidermal necrolysis, drug reaction with eosinophilia and systemic symptoms, or at the discretion of the treating provider.
Demographic data collected included age, gender, weight, race, and ethnicity. Additional data included active immunosuppression or chemotherapy and history of solid organ transplantation. Active chemotherapy and immunosuppression use was defined as administration within three months of SICU admission. The presence of septic shock (lactate >2 and requirement of a vasopressor) was determined by obtaining the highest lactate within 24 hours of admission to the SICU and vasopressor use within the same time frame. Nasal swab MRSA polymerase chain reaction (PCR) was encouraged to be obtained on SICU admission for all patients with a cIAI. Test results were collected for patients who were screened during the SICU admission. For patients who received empiric vancomycin therapy because of high risk for MRSA infection as well as MRSA nares PCR testing and had a negative test result, vancomycin was discontinued.
Each SICU admission for a cIAI was included as a separate encounter. Patients who were transferred out of the ICU and then transferred back during the same hospital stay and received antibiotic agents for a cIAI were included as two separate SICU admission encounters.
The primary outcome was the number of vancomycin DOT per 1,000 patient days present in the ICU comparing pre- and post-protocol change. For DOT per ordered course of vancomycin and DOT per 1,000 patient days, any one dose of vancomycin on any day after midnight was considered as one absolute day of therapy. Secondary outcomes include number of piperacillin-tazobactam, cefepime, metronidazole, and levofloxacin DOT per 1,000 patient days present comparing pre- and post-protocol change, incidence of MRSA cIAI defined as a cIAI culture with MRSA growth, and incidence of multi-drug-resistant organism (MDRO) growth on cIAI culture. MDRO was defined as bacteria resistant to three or more classes of antimicrobial agent drugs, which included extended-spectrum beta-lactamase, vancomycin-resistant enterococci, and carbapenem-resistant Enterobacteriaceae organisms. 12 Intra-abdominal cultures are not routinely obtained for secondary peritonitis in the SICU and are reserved for patients with drainable abscesses or failure to improve.
A subgroup analysis was conducted of patients who received more than five days of antibiotic agents to assess for secondary infections and source control. A secondary infection was defined as any infection after the initial cIAI requiring antibiotic agent therapy. A patient was determined to have source control if they had a source control procedure, completed the course of antibiotic agents for cIAI, and did not require further procedures. Patients were considered not to have source control if they were discharged on a prolonged antibiotic agent course for their cIAI, had documented lack of source control, or died before source control was obtained.
Descriptive statistics were calculated to describe the patient population using medians and interquartile ranges (IQRs). Data collection was performed using Microsoft Excel, and statistical analysis were performed utilizing Microsoft Excel and IBM SPSS Statistics Version 29. The Shapiro–Wilk test was used to determine normality of data. Chi-square and Fisher exact tests were used for categoric data and the Mann–Whitney U was used for continuous variables. For all analyses, p < 0.05 was considered statistically significant.
Results
Patient identification and characteristics
A total of 130 unique patients accounting for 142 SICU encounters were identified, all of whom were confirmed to have a cIAI. Of the 142 encounters, 64 encounters (58 patients) were included in the pre-cohort and 78 encounters (72 patients) were included in the post-cohort (Fig. 1). Multiple SICU admissions during a hospitalization was rare, with four patients in the pre-cohort and five patients in the post-cohort admitted twice and one patient in each cohort admitted three times.
Patient enrollment and treatment cohort. Patients were identified for inclusion by the International Classification of Diseases, Tenth Edition (ICD-10) and Current Procedural Terminology (CPT) codes associated with intra-abdominal procedures and peritonitis. The pre-cohort included patients who were admitted between March 1, 2021, and March 31, 2022, and the post-cohort included patients who were admitted between May 1, 2022, and May 1, 2023.
Baseline demographics for the 130 patients were similar between cohorts (Table 1). Patients were a median age of 64 years, 52% male, and were predominately Caucasian. The median SICU length of stay was six days (IQR 3–11) in the pre- and six days (IQR 4–11) in the post-cohort. Septic shock occurred in 60.3% (35/58) of patients in the pre-cohort and 51.4% (37/72) of patients in the post-cohort (p = 0.238), with a median lactate of 3.0 mmol/L in both cohorts. There were numerically more patients with recent chemotherapy or immunosuppression in the pre- compared with post-cohort, 32.8% (18/58) versus 22.2% (15/72), however, this was not statistically different (p = 0.334). A total of 13 patients had a history of solid organ transplantation (pre-cohort, 6 [10.2%], and post-cohort, 7 [9.7%, [p = 1.000]) with kidney transplantation being the most common.
Demographics and Baseline Characteristics
IQR = interquartile range; SICU = surgical intensive care unit.
Primary outcome
The median DOT per 1,000 patient days was not statistically significantly different between cohorts with a median of 14 [IQR 5–21] versus 16 days [IQR 8–17] (p = 0.522) (Fig. 2). However, there was a significant decrease in patients with vancomycin exposure; 90.6% of patients in the pre-cohort received vancomycin compared with 76.9% of patients in the post-cohort (p = 0.042).
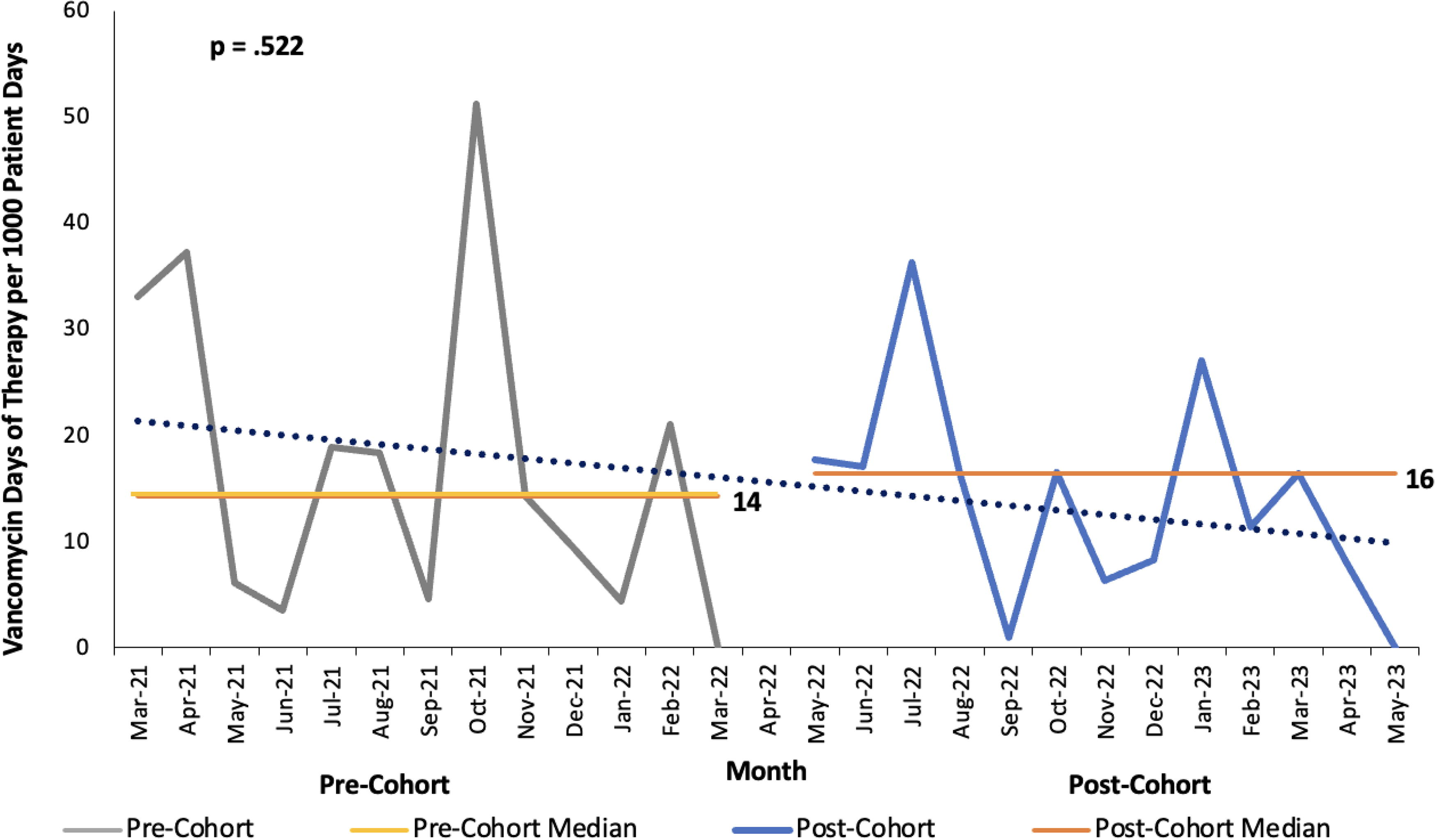
Vancomycin days of therapy (DOT) per 1,000 patient days. Statistical process chart to showcase change in vancomycin DOT per 1,000 patient days over time in months. Presented is the DOT per 1,000 patient days per month with the pre-cohort represented in gray and the post-cohort represented in blue as well as the median DOT per 1,000 patient days in yellow for the pre-cohort and orange for the post-cohort. The blue dotted line represents the overall trend of vancomycin DOT per 1,000 patient days.
Secondary outcomes
As described in Table 2, there were no statistically significant differences in median DOT per 1,000 patient days for any antimicrobial agent. A statistically significant increase in piperacillin-tazobactam usage was observed in the post-cohort, with 82.1% of patients receiving piperacillin-tazobactam compared with 48.4% of patients in the pre-cohort (p < 0.001). The overall median antibiotic agent duration in SICU was five [IQR 4–7] days in both cohorts.
Antimicrobial Agent Therapy and Microbiologic Results
MDRO = multi-drug-resistant organism defined as bacteria that are resistant to more than three classes of antimicrobial agents; ESBL = extended-spectrum beta-lactamase; VRE = vancomycin-resistant enterococci; CRE = carbapenem-resistant Enterobacteriaceae; MRSA = methicillin-resistant Staphylococcus aureus.
When examining absolute antimicrobial agent days, no statistically significant changes were seen between cohorts regarding vancomycin, cefepime, metronidazole, meropenem, and levofloxacin (Table 2). However, a statistically significant increase in absolute piperacillin-tazobactam use was seen with a median absolute day of therapy of 8 [IQR 3–24] days in the pre-cohort compared with 23 [IQR 14–33] days in the post-cohort (p = 0.038).
Empiric vancomycin was appropriately started in 41/64 (64.1%) of encounters in the pre-cohort and 36/78 (46.2%) of encounters in the post-cohort. Of those who received empiric vancomycin coverage, more encounters in the pre-cohort compared with those in the post-cohort received vancomycin for Enterococcus spp. coverage (40.6% vs. 30.8%) as well as for immunocompromised patients (23.4% vs. 15.3%). History of MRSA infection was rare, with just two patients in the post-cohort fitting this criterion (p = 0.501). When vancomycin was added for Enterococcus spp. coverage, 34 encounters (17 pre- and 17 post-cohort) utilized vancomycin plus cefepime, whereas 14 (nine pre- and five post-cohort) utilized vancomycin plus levofloxacin.
Microbiologic results
Microbiologic results are described in detail in Table 2. MRSA PCR nasal swab testing was more common in the post-cohort, with 61.1% (44/72) of patients receiving the test versus 32.8% (18/58) in the pre-cohort (p = 0.005). Of those screened, 11.1% (2/18) in the pre-cohort and 18.2% (8/44) in the post-cohort had positive MRSA nares tests. The incidence of positive MRSA nares and positive MRSA cIAI culture was observed in three patients—one patient in the pre-cohort and two patients in the post-cohort. No patients had positive MRSA cIAI culture with a negative nares result.
Infectious diseases (ID) consultations are not required for the management of cIAI at the institution; however, 42.2% (27/58) of patients in the pre-cohort and 46.2% (35/72) of patients in the post-cohort had an ID consultation (p = 0.735). Of those who received ID consultations, transplant ID as opposed to a general ID service was consulted in 11.1% (3/27) of patients in the pre-cohort and 13.9% (5/36) of patients in the post-cohort. Intra-abdominal cultures were collected in 44% (28/64) of patients in the pre-cohort and 49% (38/78) of patients in the post-cohort. Of patients who were cultured, positive intra-abdominal culture resulted in 79% (22/28) and 92% (35/38) of patients in each cohort. Of the patients with positive intra-abdominal cultures, 13 patients (5 in the pre-cohort and 8 in the post-cohort) had MRDO infections and 11 patients received ID consultations for management guidance. All three patients with MRSA isolated from their intra-abdominal culture had an ID consultation. For patients who received ID consultation, there was no difference in absolute antibiotic agent day between cohorts with 5 [IQR 4–6] days in the pre-cohort versus 5 [IQR 4–7] days in the post-cohort (p = 0.520).
Subgroup analysis
In the subgroup analysis of patients who received more than five days of antibiotic agents, a total of 40 patients accounting for 45 unique SICU encounters received prolonged vancomycin courses and a total of 23 patients (24 unique SICU encounters) received prolonged piperacillin-tazobactam courses (Table 3).
Subgroup Analysis of Patients Receiving Prolonged Vancomycin or Piperacillin-Tazobactam
Prolonged vancomycin courses were attributed to secondary infections in 52.5% of encounters in the pre-cohort and 68.8% in the post-cohort (p = 0.379). Source control was achieved for 72.4% and 75.0% of these encounters (p = 0.853). Of the encounters who received prolonged vancomycin courses, source control was not achieved in eight encounters in the pre-cohort and four encounters in the post-cohort.
Patients receiving prolonged piperacillin-tazobactam courses had secondary infections in 100.0% of patients in the pre-cohort and 66.7% of patients in the post-cohort (p = 0.401), whereas source control was achieved in 66.7% and 33.3%, respectively (p = 0.401). Of the patients who received prolonged piperacillin-tazobactam courses, source control was not achieved in one encounter in the pre-cohort and 14 encounters in the post-cohort.
When excluding patients who did not have source control, no difference in vancomycin use was seen with median DOT per 1,000 patient days of 9 days [IQR 5–19] in the pre-cohort and 8 days [IQR 7–16] in the post-cohort (p = 1.000). When examining piperacillin-tazobactam, a significant increase in use was seen with median DOT per 1,000 patient days of 7 days [IQR 3–14] in the pre-cohort and 13 days [IQR 4–18] in the post-cohort (p = 0.223).
Discussion
In this retrospective, pre- and post-cohort study of critically ill surgical patients with cIAI, an antimicrobial stewardship guideline did not impact vancomycin DOT per 1,000 patient days, however, a significant reduction in vancomycin exposure was observed.
Although the lack of a difference in the primary outcome seems counterintuitive, a few nuances of the post-cohort may explain this finding. First, two patients in the post-cohort with no history of MRSA presented in septic shock with active MRSA infections and subsequently accounted for 19 days of vancomycin use throughout their prolonged SICU admission. The post-cohort included two additional patients with a history of MRSA in the 90 days leading up to admission therefore warranting empiric vancomycin for cIAI and accounting for 10 days of vancomycin therapy. Finally, more patients in the post-cohort had a positive MRSA nasal swab thus limiting de-escalation or prompting inappropriate antibiotic agent escalation. This was associated with 31 days of vancomycin compared with 12 days of vancomycin in the pre-cohort.
In addition, it is important to note that many patients who received prolonged vancomycin courses did not have source control or had a secondary infection, such as pneumonia or bacteremia. This highlights the complexity of the patient population and the difficulty to examine a single type of infection in patients who are at high risk for infectious complications throughout admission. As such, these patients are more likely to receive prolonged antibiotic agent courses and therefore drive up the overall antibiotic agent usage and DOT.
The patient population described in this study is all-encompassing, including 18.1% of patients who were classified as immunocompromised and those without source control. This patient population is rarely included in studies examining cIAI and when included often represent a small subset of patients. In the STOP-IT trial, only 11% of included patients had a malignant disease. Furthermore, the STOP-IT trial had a mean APACHE II score of 10 with no documentation of ICU admissions and patients were believed to have had source control for inclusion. In the DURAPOP trial, patients who were neutropenic, immunosuppressed, or receiving chronic corticosteroid therapy were excluded.13,14 In addition, both the STOP-IT and DURAPOP trials excluded patients who did not have source control. Through robust inclusion criteria, this study examined a broader patient population often neglected in studies allowing for a real-world example of what is happening in critically ill surgical patients.
Positive organism detection on IAI culture was observed in 86.4% of patients, with 5.3% of positive cultures having MRSA. This overall culture positive rate is higher than that described in the DURAPOP study, reporting positive IAI cultures in 20.4% of patients; however, the authors described the incidence of MRSA as 13.6% of patients with positive samples, which is much higher than what was found in this study. 13 A previous study conducted in the SICU at this institution also demonstrated a low incidence of MRSA cIAI at a rate of 2.6%. 15 Furthermore, a post hoc analysis of the STOP-IT trial conducted by Sanders et al. isolated MRSA in 2.3% of patients and found low utility for empiric vancomycin administration. 16 As such, this study supports the restricted use of empiric vancomycin for MRSA coverage in cIAI within this antimicrobial stewardship protocol.
Several strengths of this trial should be noted, including the broad patient population and the primary outcome of DOT per 1,000 patient days. DOT per 1,000 patient days is an antimicrobial stewardship metric conducted at the population level and is considered an ideal measure for antimicrobial stewardship. It comprised an aggregate sum of days for which any amount of antimicrobial agent was administered to individual patients divided by total patient days. 17 This metric is supported by the Joint Commission and the IDSA.
There are several limitations to this study. This was a retrospective, single-center study with data limited by what was documented in the electronic health record. Because of the retrospective study design, it was not feasible to collect the date source control obtained, as this is a subjective decision made by the surgery team. Most of the patients in the SICU require multiple procedures to obtain source control making it difficult to retrospectively define the date of source control and assess appropriate duration of antibiotic agents; however, this was often able to be inferred on the basis of the date of their last procedure. Furthermore, patient inclusion was reliant on admission to the SICU, use of antibiotic agents for cIAI, and a pre-defined list of ICD-10 and CPT codes. This may have introduced selection bias toward the critically ill and not captured our full cohort of patients with intra-abdominal infections. In addition, patient’s allergy history was not able to be fully elucidated by chart review therefore potentially exposing more patients to vancomycin for enterococcal coverage because of documented severe penicillin allergies.
Conclusion
In critically ill surgical patients with cIAI, a practice management change to limit the use of empiric vancomycin did not reduce the median vancomycin DOT per 1,000 patient days but did reduce overall vancomycin exposure. Because of the low incidence of MRSA cIAI, there is an opportunity for antimicrobial stewardship, and practitioners should limit the use of antibiotic agents that cover MRSA to patients at high risk for MRSA infections.
Footnotes
Authors’ Contributions
M.E.P. designed the study, collected and interpreted the data, and drafted the article. K.R., J.F., and M.C.S. contributed to the interpretation of data and critically revised the article for important intellectual content. All authors approved the final version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors have reviewed and approved this article before submission for publication.
Author Disclosure Statement
This study did not receive any funding and no competing financial interests exist. The authors declare no competing interests. M.E.P., J.F., K.R., and M.C.S. all contributed equally to the article writing.
Funding Information
No funding was received for this article.