
Abstract

To the Editor:
We have read the recent article published in Surgical Infections by Houston et al., 1 which provides a notable update on the management of intra-abdominal infections (IAIs) in 2017.
Current guidelines categorize IAI patients on the basis of broad indicators, such as comorbidities and the presence of organ dysfunction. 1 However, this may overlook the pathophysiologic mechanisms driving the infection and lead to the overuse of antibiotic agents and undertreatment of certain infections where specific interventions could be more beneficial. Thus, a cause-based treatment could provide a more precise therapeutic approach. IAIs are acute conditions in which physical, biologic (including immunologic), and chemical factors (including nutritional) play the major role in their pathogenesis. 2 Genetic, environmental, and sociopsychologic elements, on the other hand, serve minor roles. Therefore, we propose a new treatment paradigm that emphasizes the physics, biology, and chemistry (P-B-C) aspects of infection to better individualize therapy.
The proposed P-B-C model categorizes IAIs on the basis of the etiology of the infection, under three aspects as follows: physics, biology, and chemistry. The physical aspect mainly relies on imaging for evaluation, whereas biology and chemistry aspects are investigated through biochemical tests. The physics aspect encompasses structural and mechanical causes of IAIs. For instance, in perforated diverticulitis, the primary cause of the infection is mechanical, and the mainstay of treatment should involve resolving the structural defect, such as surgical repair, whereas antimicrobial therapy plays a supportive role. 3 The biology aspect focuses on the biologic agents responsible for the infection. For example, in polymicrobial infections, the identification of specific pathogens and their virulence factors can lead to more precise antimicrobial therapy. 4 Instead of using a one-size-fits-all antibiotic regimen, therapy could be adjusted on the basis of the bacterial species involved, their resistance profiles, and the patient’s immune response. The chemistry aspect refers to the biochemical environment that may exacerbate or contribute to the infection. An example would be post-pancreatectomy pancreatic fistula, where leakage of pancreatic fluid into the peritoneal cavity causes chemical destruction of surrounding tissues, which predisposes to and exacerbates intra-abdominal infections. In such cases, removing the fluid by drainage or peritoneal lavage could improve patient outcomes by addressing both the infection and the inflammatory environment it propagates. 5 By dividing the causes of IAIs into physics, biology, and chemistry, we can individualize treatments on the basis of the specific mechanisms involved.
Furthermore, the P-B-C model provides an additional layer to improve prognostic accuracy in IAIs. Although existing scoring systems emphasize risk factors derived from test results, a scoring system on the basis of the P-B-C model could be developed by assessing the severity of each P-B-C dimension (Fig. 1). For example, a high score in physics may indicate substantial structural damage requiring prompt surgical intervention, whereas a high score in biology might suggest a compromised immune status that demands aggressive antimicrobial therapy. Similarly, a high score in chemistry might indicate the presence of enzymatic degradation that, if managed early, could substantially improve the prognosis.
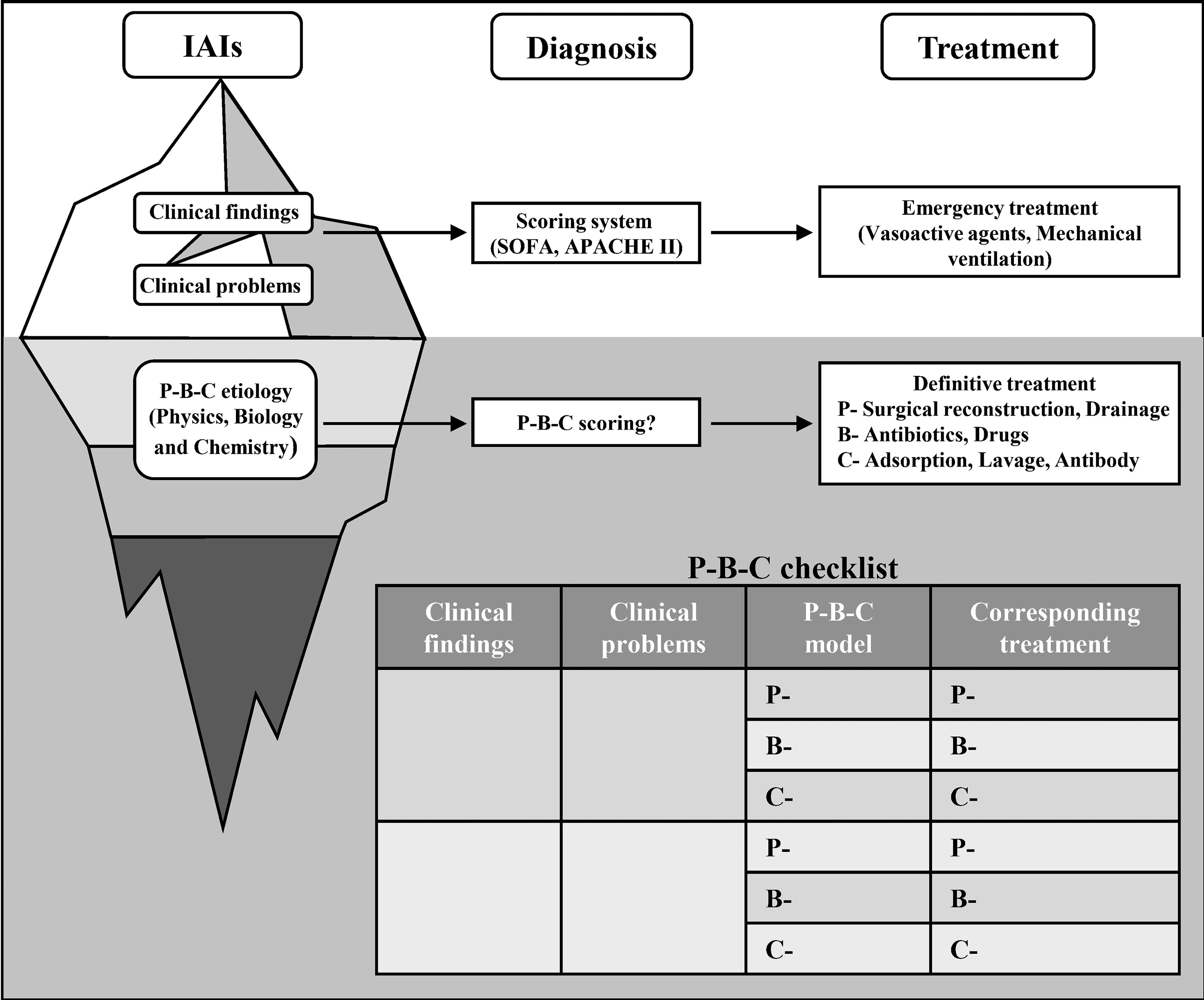
The iceberg model of intra-abdominal infections (IAIs) treatment framework, highlighting the P-B-C (physics–biology–chemistry) approach concerning current diagnostic and treatment systems. The visible portion of the iceberg represents clinical findings and clinical problems, typically the focus of current diagnostic and scoring systems, such as SOFA and APACHE II. These systems guide initial emergency treatments such as vasopressors or mechanical ventilation. However, the submerged portion of the iceberg illustrates the deeper mechanisms such as physics, biology, and chemistry that may drive the infection, but are often less emphasized in traditional scoring models. The P-B-C model incorporates these underlying causes to guide more specific radical treatments. The P-B-C scoring system could complement existing scoring systems, offering a more comprehensive approach by addressing both visible symptoms and the underlying causes of infection. The checklist at the bottom outlines potential clinical findings, corresponding clinical problems, and the P-B-C model’s alignment with targeted treatments, which may be adopted in the clinic.
The P-B-C model aims to improve the current guidelines by incorporating the pathophysiology of IAIs into consideration. This could help clinicians make more individualized treatment following initial empiric therapy. It is especially valuable in the context of decreasing antimicrobial resistance and personalized medicine.
Footnotes
Authors’ Contributions
F.Z.: Wrote the first and final drafts of the article and critically reviewed and revised the article. X.Z.: Drew the figure. C.L.: Critically reviewed and revised the article. J.Z.: Designed the topic of the article and critically reviewed and revised the article. All authors read and approved the final article.
Funding Information
This project was funded by the National Natural Science Foundation of China (No. 82472191).
Author Disclosure Statement
The authors declare no competing interests.