
Abstract
Background:
Post-operative urinary tract infections (UTIs) are a notable complication of radical prostatectomy, contributing to prolonged hospital stays, increased healthcare costs, and diminished patient quality of life. Despite international guideline recommendations of European Association of Urology and the French Society of Anesthesia and Intensive Care Medicine regarding the use of pre-operative urine cultures and antibiotic prophylaxis (AP) before radical prostatectomy, the role of pre-operative urine cultures in mitigating UTI risk remains uncertain.
Methods:
This multi-center prospective cohort study analyzed data from six French urology departments. Patients who underwent radical prostatectomy between January 2019 and June 2023, with variable inclusion periods across centers, were included if pre-operative urine cultures were performed. Patients were stratified into subgroups based on the occurrence of post-operative UTIs. Uni-variable and multi-variable logistic regressions, as well as receiver-operating characteristic (ROC) curve analysis, were used.
Results:
A total of 467 patients were analyzed, among whom post-operative UTIs developed in 30 patients. Among peri-operative factors, only the ASA (American Society of Anesthesiologists) score (p = 0.014) and the duration of post-operative catheterization (p = 0.001) were significantly associated with UTI occurrence in uni-variable analyses. Multi-variable logistic regression confirmed both factors as independent predictors of post-operative infections, with a model area under the ROC curve for catheterization duration of 0.789. A seven-day threshold for catheterization duration was identified as the optimal cutoff for predicting infection risk. Notably, neither pre-operative urine bacterial cultures nor AP reduced the incidence of post-operative UTIs.
Conclusion:
This study demonstrates that pre-operative urine cultures and prophylactic antibiotic agents do not mitigate UTI risk following radical prostatectomy, underscoring the need for optimized infection prevention tactics. The findings challenge the clinical utility of routine pre-operative urine cultures and highlight the critical roles of ASA score and post-operative catheterization duration in predicting infections.
Prostate cancer remains a notable concern for men worldwide, and prostatectomy stands out as a crucial therapeutic approach. Among the various complications associated with prostate surgical procedure, post-operative urinary tract infections (UTIs) pose a notable challenge. The incidence of UTIs after prostatectomy can lead to prolonged hospital stays, increased healthcare costs, and a decline in the overall quality of life for patients.
An aspect deserving particular attention is the role of pre-operative urine culture in predicting and mitigating the risk of UTIs after prostatectomy. Although the importance of pre-operative assessments is widely recognized, the specific impact of routine urine cultures in this context remains an active area of research. This French multi-center study aims to delve into the existing literature, examining the relation between pre-operative urine cultures and the subsequent risk of UTIs in patients undergoing prostatectomy.
Understanding the microbial landscape of the urinary tract before operation could offer valuable insights into the patient’s susceptibility to post-operative infections. By identifying potential pathogens and their antibiotic susceptibility profiles through urine cultures, clinicians can tailor prophylactic antibiotic regimens, enhancing the efficacy of preventive measures. In addition, the exploration of patient-specific risk factors contributing to UTIs post-prostatectomy will further inform targeted interventions, potentially reducing the incidence of these infections.
UTI stands as one of the most prevalent infections, with approximately one-fifth of reported cases occurring in males. The reported incidence of UTIs in males aged 65–74 years is 0.05 per person-year. 1 The mortality rate associated with urosepsis increases significantly with age, ranging from 20% to 40%. 2 UTIs contribute substantially to nosocomial infections, accounting for about 36%, affecting mortality rates and incurring social and medical costs. 3
The incidence and risk factors associated with UTIs after prostate cancer (PCa) treatment remain unclear. In the realm of prostatectomy, related infectious complications have been relatively underlooked.
It remains unclear whether antibiotic prophylaxis (AP) should be recommended or discouraged in robot-assisted laparoscopic radical prostatectomy (RALP) for PCa. The development of microbial resistance and side effects are risks of antibiotic use. We hypothesize that pre-operative urine cultures may help identify patients at risk of post-operative UTI, thereby informing targeted prophylactic tactics.
The aim of the study is to evaluate whether pre-operative urine cultures predict and mitigate post-operative UTI risk after prostatectomy, using a French multi-center cohort.
Patients and Methods
Study design
We asked six departments to share their prospective database on patients who underwent a radical prostatectomy from January 2019 to June 2023 with variable periods of inclusion between participating centers. Inclusion criteria were patients undergoing laparoscopic or robotic radical prostatectomy and pre-operative urine culture. Patients operated by open approach were excluded. This study received a waiver of informed consent from the Institutional Review Board of CHRU Tours, as it involved secondary use of anonymized data collected during routine clinical practice.
Post-operative UTI was defined as febrile urinary infection with irritative urinary symptoms and documented with one or both, urine/blood cultures in the 30 days period following surgical procedure.
Statistical analysis
Students’ and chi-square tests were used for quantitative and qualitative variables, respectively. The significance level was set at 0.05 for all statistical tests, and p-values were two sided.
The Kolmogorov–Smirnov test was used to assess normality of continuous variables, including age, body mass index (BMI), prostate volume, operative time, blood loss, and catheterization duration. Non-parametric tests were used when appropriate.
Uni-variable and multi-variable logistic regression was performed to investigate risk factors associated with the occurrence of post-operative UTI episodes. Receiver-operating characteristic (ROC) curves were used to evaluate the diagnostic accuracy of the duration of catheterization for UTI after radical prostatectomy. The Youden index (J), defined as the maximum vertical distance between the ROC curve and the diagonal line, serves as another global measure of overall diagnostic accuracy and can be used to choose the optimal cutoff point. 4 Finally, cutoff value of continuous parameters selected from logistic regression was calculated by ROC curve. p < 0.05 was considered significant for all tests. Patients with missing data were excluded from the analysis. Statistical analysis was performed with R software® version 2021.09.0 (R Foundation for Statistical Computing, Vienna, Austria).
Multiple patient- and procedure-related parameters potentially implicated in these episodes were included as follows: age, BMI, history of UTI in the year preceding operation, smoking, diabetes mellitus, type of surgical procedure (laparoscopic- or robotic-assisted), pre-operative urine culture, pyuria, type of bacteria, fluoroquinolone resistance, pre-operative antibiotic, AP, type of antiseptic scrub, American Society of Anesthesiologists (ASA) score, operative time, prostate volume, blood loss, lymph node dissection, drain, hospital stay, post-operative febrile UTI, and other complications. We focused on fluoroquinolones because they are the most common prophylactic agents.
Results
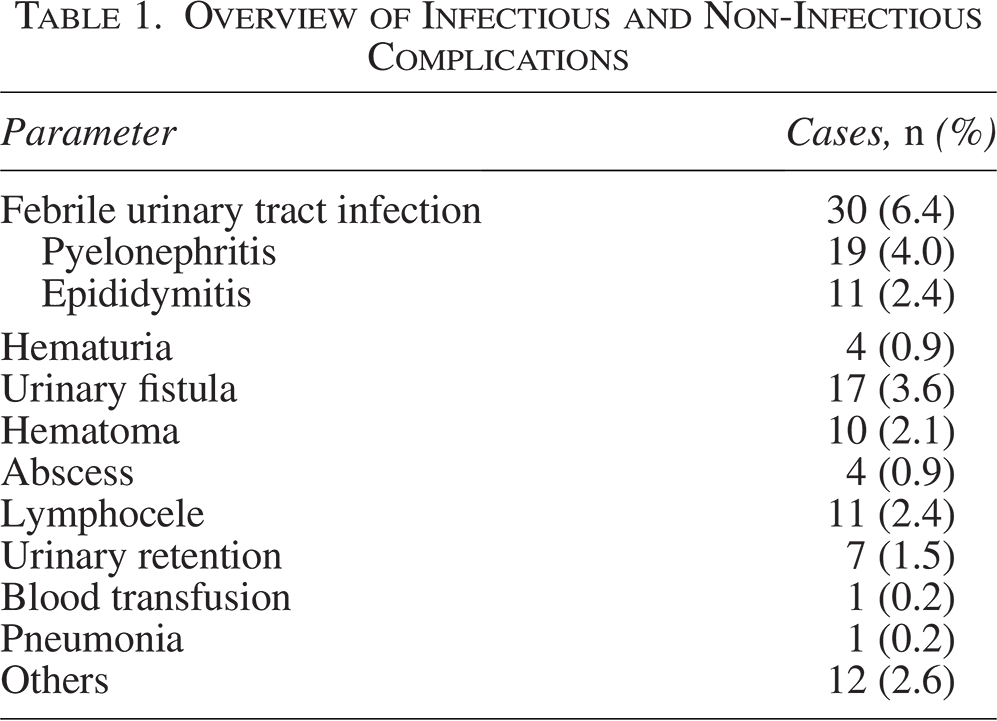
A total of 467patients have been enrolled in the study from six French centers. All patients were followed up, at least one month, to identify several UTIs post-radical prostatectomy. Schematic representation of post-operative UTI incidence according to multiple pre- and operative parameters are shown in Figures 1–3. Thirty febrile infections were identified with 11 epididymitis and 19 pyelonephritis. No cases of cystitis or orchitis were observed in our cohort. Non-infectious complications were observed, including lymphocele in 11 patients, urinary fistula in 17 patients, and others as shown in Table 1. No surgical site infections (SSIs) were recorded.
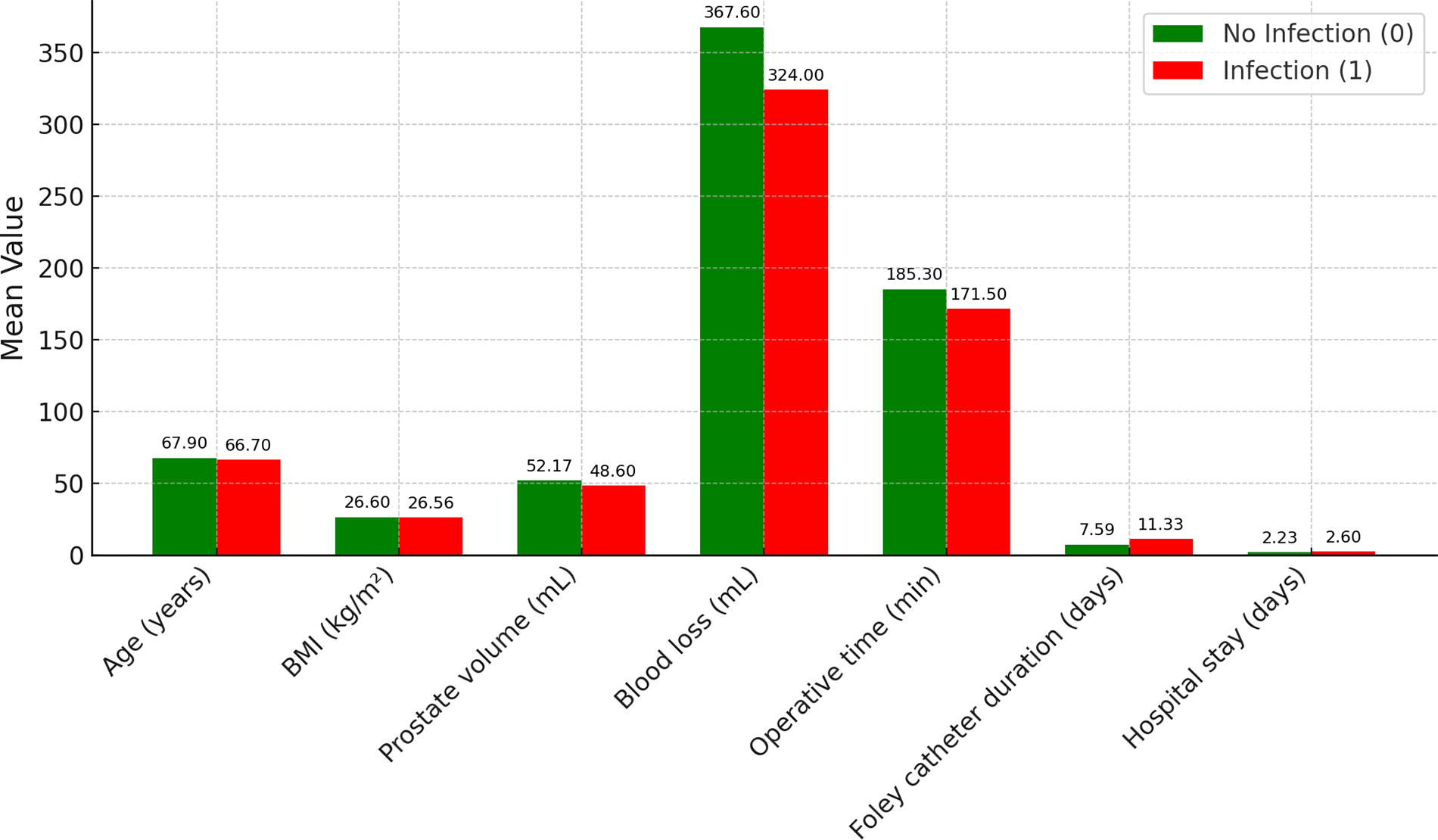
Post-operative UTI incidence using multiple continuous parameters (1 referred to infection, 0 to absence of infection). UTI = urinary tract infection.

Post-operative UTI incidence depending on pre-operative urine culture results and antibiotic prophylaxis. UTI = urinary tract infection.
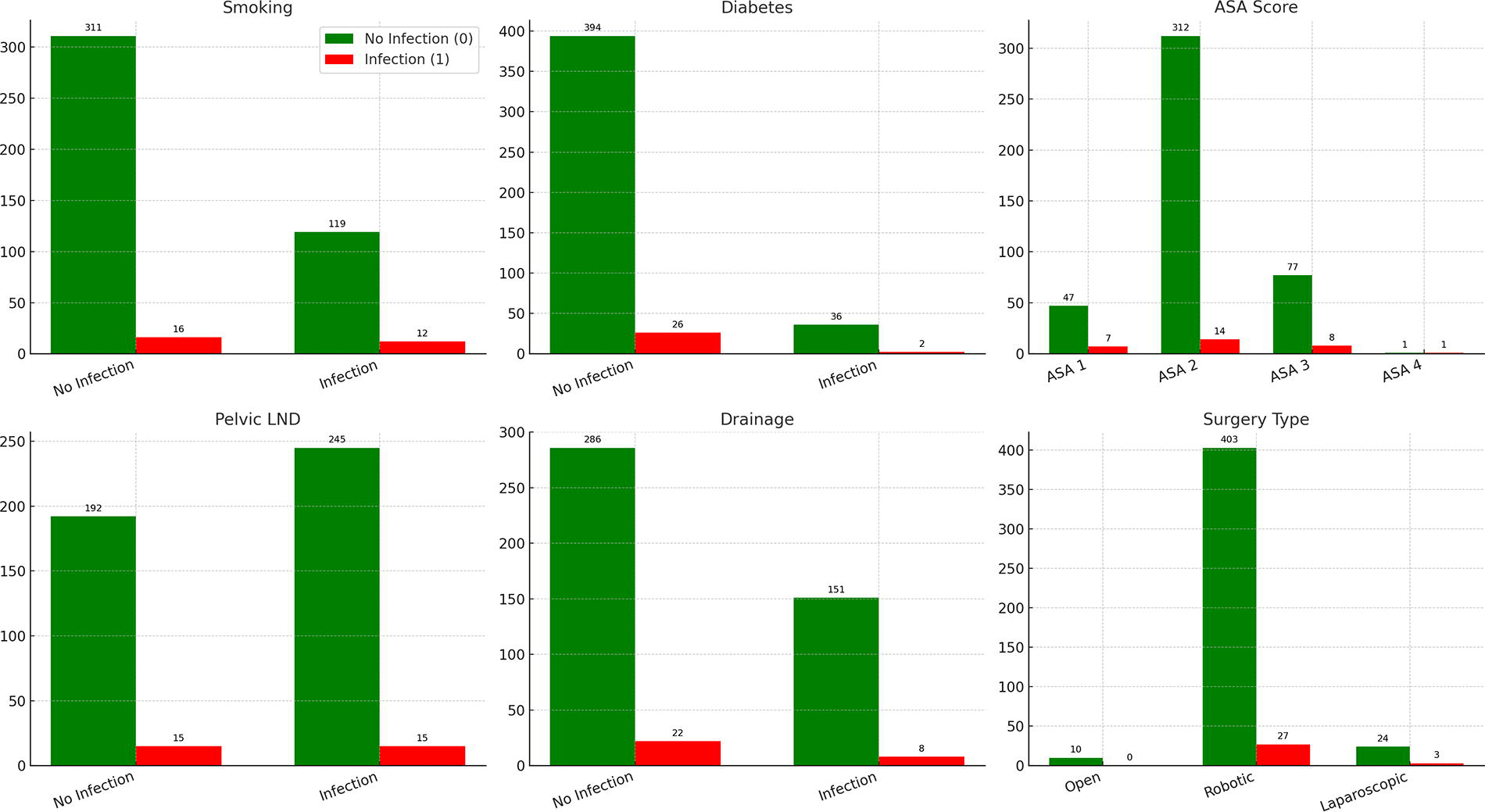
Post-operative UTI incidence using multiple peri-operative ordinal parameters. UTI = urinary tract infection.
Overview of Infectious and Non-Infectious Complications
Clinical and Peri-Operative Characteristics of Patients and Uni-Variable Associations with Post-Operative Urinary Tract Infection After Radical Prostatectomy

All values are expressed as mean (±SD) or n (%).
Bold and * = statistically significant.
SD = standard deviation; BMI = body mass index; ASA = American Society of Anesthesiologists; UTI = urinary tract infection.
Multi-Variable Analysis to Predict Urinary Tract Infection After Radical Prostatectomy
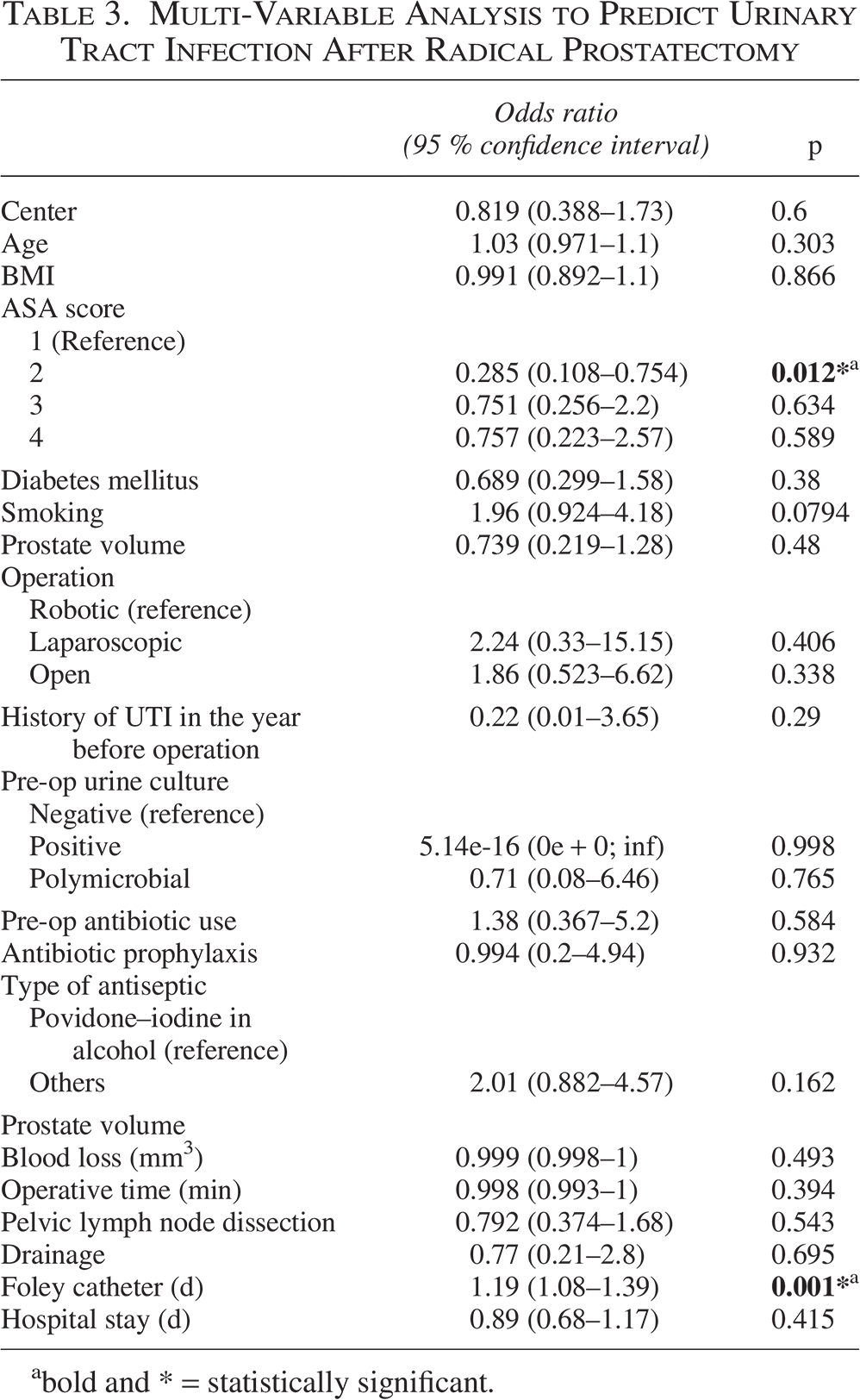
bold and * = statistically significant.
Of the 30 infected patients, 29 had negative pre-operative culture and 1 had a positive polymicrobial urine culture. Polymicrobial culture was not sufficient to define infection, unless associated with clinical symptoms and positive post-operative cultures.
Regarding prophylactic antibiotic use, 27 patients (5.8%) received peri-operative antibiotic prophylaxis, despite national recommendations advising against it in this context. Among them, post-operative UTIs developed in two patients, suggesting limited protective effect. Escherichia coli was the predominant bacterial species in 7 of 30 patients, followed by Enterococcus faecalis in 4 patients and Klebsiella pneumoniae in 3 patients. Other species included Morganella morganii, Citrobacter koseri, Staphylococcus aureus, and Streptococcus agalactiae. Profile of resistance was recorded in 21 out of 30 patients with only 5 having penicillinases; no extended-spectrum beta-lactamase or multi-drug-resistant organism species were recorded.
The mean duration of catheterization was 11.33 ± 12.35 days in the infection group compared with 7.59 ± 2.87 days in the non-infection group. This difference was statistically significant (p = 0.001). Patients were stratified into two subgroups according to the occurrence of post-operative UTIs. Uni-variable analysis showed that an ASA score of 2 was associated with a lower risk of post-operative UTI (p = 0.014), whereas prolonged post-operative catheterization was associated with a greater risk (p = 0.001) Table 2.
Multi-variable logistic regression analysis identified two independent factors associated with the occurrence of post-operative UTIs (Table 3). An ASA score of 2 was significantly associated with a reduced risk of UTI (adjusted odds ratio [OR]: 0.35, 95% confidence interval [CI]: 0.15–0.82, p = 0.016), indicating a protective effect. In contrast, prolonged post-operative catheterization was associated with an increased risk of UTI. When analyzed as a continuous variable, each additional day of catheterization increased the odds of post-operative UTI by 11% (adjusted OR: 1.11, 95% CI: 1.05–1.17, p < 0.001). In addition, ROC curve analysis for catheterization duration identified a seven-day threshold as the optimal cutoff for predicting infection risk, with an area under the curve of 0.789. These findings emphasize both the protective effect of better pre-operative health status (ASA score 2) and the negative impact of longer catheterization on infection risk.
Discussion
The European Association of Urology states in their guidelines that antibiotic prophylaxis should be used before radical prostatectomy; however, they also note that there is no high-level evidence supporting this practice. In addition, as the susceptibility of bacterial pathogens and antibiotic availability vary worldwide, any use of prophylactic antibiotic agents should adhere to local guidelines. 5
Meanwhile, the French Society of Anesthesia and Intensive Care Medicine, in association with the French Association of Urology, states that there is no evidence to support the use of any antibiotic prophylaxis before radical prostatectomy. 6 Similarly, the American Urological Association guidelines classify surgical procedures based on the risk of SSIs into low-, intermediate-, and high-risk categories. Radical prostatectomy is categorized as an intermediate-risk procedure, for which antimicrobial prophylaxis may be recommended depending on patient comorbidities and local resistance patterns. For example, simple cystoscopy in healthy patients is considered low risk and does not require prophylaxis, whereas transurethral prostate procedures carry a high risk and necessitate antibiotic prophylaxis because of a greater rate of infectious complications if antibiotic agents are not administered. This procedural stratification provides a framework for rational antibiotic use and supports individualized decision-making based on surgical and patient-related factors. 7
A recent systematic review examined the evidence supporting AP in RALP and concluded that there is no evidence indicating a difference in the rate or severity of infective complications within 30 days post-operation among various prophylactic protocols. The overall incidence of post-operative infectious complications ranged from 0.6% to 6.6% among patients who received AP, with SSI rates ranging from 0.46% to 1.12%. 8
Our findings highlight two important independent factors influencing the risk of post-operative UTIs following radical prostatectomy. First, an ASA score of 2 was protective against infection, consistent with previous studies identifying better pre-operative health status as a determinant of surgical outcomes. Second, prolonged catheterization emerged as a significant risk factor. Importantly, our analysis showed that each additional day of catheterization increased the odds of UTI by 11%, reinforcing the clinical importance of minimizing catheter duration whenever feasible. Although a seven-day threshold was identified as an optimal cutoff point, the continuous relation between catheterization duration and infection risk underscores that even small extensions in catheter time may negatively affect outcomes. These results provide a strong rationale for early catheter removal protocols and suggest that individualized catheter management tactics could help reduce post-operative infectious complications.
The occurrence of UTI following either radiation therapy (RT) or radical prostatectomy (RP) remains somewhat ambiguous. In a prospective study involving approximately 425 patients treated with robot-assisted RP, the UTI rate was found to be 6.1% within 30 days post-operation. 9 Treatment-induced anatomic or histologic changes may elevate the occurrence of UTIs, as bacteria can ascend through the urethra into the bladder. Radical prostatectomy can compromise the natural defense mechanisms in males with an elongated urethra. 9 UTI rates also vary across different RP methods.10,11
Robot-assisted RP is associated with fewer post-operative complications and a greater urinary continence rate compared with laparoscopic RP. 10 These advantages may contribute to a reduced likelihood of UTIs. In addition, post-operative UTIs could be linked to changes in bladder microbiome composition resulting from incontinence operation. 12
Hyun et al. 11 recently published a population-based study assessing trends in UTIs and the prognosis of patients with PCa after RP and RT. They showed that the robot-assisted RP group had a lower risk of UTIs compared with the open/laparoscopic RP group in both the early (adjusted HR: 0.77; 95% CI: 0.77–0.78; p < 0.001) and late (adjusted Hazard ratio [HR]: 0.90; 95% CI: 0.89–0.91; p < 0.001) follow-up periods. In patients in whom a UTI developed, factors such as Charlson Comorbidity Index score, primary treatment type, age at UTI diagnosis, type of UTI, hospitalization, and sepsis from UTI were associated with overall survival.
The ASA score is widely recognized as a strong independent predictor of post-operative medical complications and death across various surgical procedures. 13 Although our study included a sizable cohort and a certain degree of uniformity in pre-operative and peri-operative antibiotic practices across centers, it still carries the inherent limitations of a retrospective analysis, particularly given that post-operative UTI incidence remains relatively low.
This study has several limitations. First, although data collection was prospective at the center level, the analysis was retrospective, introducing potential biases. Second, the relatively low incidence of post-operative UTIs may reduce the statistical power to detect associations with less common risk factors, such as ASA scores of 3 or 4, potentially resulting in a Type II error. Third, some clinically relevant parameters, such as the presence of obstructive uropathy or detailed comorbidity indices, were not consistently available across centers, limiting our ability to fully explore their impact. In addition, the generalizability of our findings may be influenced by the uniform healthcare setting in France and the predominance of robot-assisted surgical procedures in our cohort.
Future prospective studies with standardized definitions, broader geographic representation, and longer follow-up are needed to validate our findings. In particular, the adoption of consistent and uniform criteria for assessing infectious complications could improve data reliability. Importantly, such findings could contribute to upcoming modifications in national guidelines, including the possible elimination of mandatory pre-operative urinary bladder cultures in the era of robotic radical prostatectomy.
Conclusion
Our study confirms for the first time that neither the pre-operative urine bacterial culture nor antibiotic prophylaxis reduces the risk of infection following radical prostatectomy despite international guidelines discrepancy. These findings along with other future studies should lead the way toward a change in recommendations, with an aim of reducing both antibiotic consumption and probably also antibiotic resistance.
Authors’ Contributions
A.B.: Conceptualization, data collection, and writing—original draft. M.T.: Statistical analysis, data interpretation, and writing—review and editing. A.V.: Supervision and project administration. S.K.: Methodology and data curation. R.H.: Visualization and data validation. M.F.: Resources and investigation. J.R.: Supervision and validation of the final draft. O.K.: Software and formal analysis. M.V.: Data interpretation and critical revision. F.B.: Funding acquisition and overall supervision.
Footnotes
Acknowledgments
The authors wish to thank the participating centers for their valuable contributions and the staff involved in data collection and patient care.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no specific funding.