
Abstract
Background:
Wound complications in gynecologic oncology, especially among patients with overweight and obesity, can significantly impact post-operative recovery and delay the initiation of adjuvant treatment. Although staples are commonly used for vertical incisions, sutures may offer clinical advantages; however, direct comparative data remain limited. This study aimed to compare post-operative wound complication rates between staples and non-absorbable sutures in patients with gynecologic cancer with a body mass index ≥25 kg/m2 and undergoing a vertical incision surgical procedure.
Patients and Methods:
A retrospective review was conducted at a gynecologic oncology center between January 2022 and September 2023. Patients who underwent midline laparotomy with either staples or 3-0 non-absorbable monofilament sutures for skin closure were included. Patients with prior chemotherapy, benign pathology, or age <18 were excluded. Wound complications—including seroma, hematoma, dehiscence (superficial and fascial), and infection—were recorded within eight weeks postoperatively.
Results:
Of 72 patients, 29 received staples and 43 received sutures. Wound complications occurred in 41% of the staple group and 21% of the suture group (p = 0.061). Fascial dehiscence was observed in four cases (two in each group). Although rates of dehiscence and infection were higher with staples, differences were not statistically significant. Hospital stay was significantly longer in the staple group (p = 0.045).
Conclusion:
Although not statistically significant, suture closure was associated with fewer wound complications and a shorter hospital stay, suggesting potential advantages in wound healing. These findings may inform future recommendations, and further prospective studies are warranted.
Post-operative wound site complications are a multi-factorial problem because of the local and systemic factors. 1 Increased body mass index (BMI), prior abdominal operations, comorbidities, and the duration of operation have all been associated with a higher risk of wound complications. Common wound complications include seromas, hematomas, surgical site infections (SSIs), and dehiscence, which is usually superficial but can occasionally involve fascial separation. 2 Superficial wound dehiscence may result in prolonged hospital stays for surgical patients. 3
Among women undergoing a surgical procedure for gynecologic cancer, SSIs are common and can lead to delays in discharge and adjuvant treatment. 4 In oncology patients, wound complications may potentially delay adjuvant treatment and could negatively impact cancer-specific survival. The incidence of wound complications following a gynecologic cancer operation can be as high as 37%. 5
Stainless steel staples have been used to close skin incisions in gynecologic oncology patients, particularly midline vertical incisions.5,6 However, the obstetric literature suggests that sutures may reduce wound complications, but limited research is available in gynecology.7,8 Although some studies have indicated that the use of staples instead of sutures does not significantly affect the rate of SSIs in gynecologic surgery, others have found an association between the use of staples and an increased risk of infection.4,9
The aim of this study was to evaluate the effect of staples versus sutures on wound complications in patients with vertical incisions who have undergone a gynecologic oncology operation.
Patients and Methods
The study was conducted retrospectively at a university-based tertiary gynecologic oncology surgical center. Patients who underwent a surgical procedure with a vertical incision between January 2022 and September 2023 were reviewed retrospectively. The study included patients who received a diagnosis of gynecologic cancer and were operated on with a vertical incision and had their surgical wounds closed with either a stainless-steel stapler or non-absorbable 3-0 monofilament suture. All patients in the suture group received closure with a vertical mattress technique using Prolene (non-absorbable monofilament 3
Wound complications were defined as seroma, hematoma, wound dehiscence (including both superficial and fascial separation), and SSI requiring additional medical or surgical intervention. Complications were identified within eight weeks after surgery using inpatient records and outpatient follow-up documentation. These data were obtained through review of the hospital’s electronic medical record system, including operative notes, post-operative progress notes, and outpatient visit summaries. Prophylactic antibiotic agents were administered to all patients before skin incision, in accordance with institutional protocol. Patients were evaluated for SSI, wound dehiscence, and prolonged hospital stay.
The study was approved by the Institutional Review Board of Akdeniz University (KBAEK-26). The requirement for patient consent was waived because of the retrospective nature of the study and the absence of any interventions.
Statistical analyses were performed using IBM SPSS version 23 (SPSS/IBM, Chicago, IL, USA) software. Data were tested for normal distribution using the Shapiro–Wilk test. Qualitative data were represented as frequencies and relative percentages. The chi-square test and Fisher exact test were used to calculate differences between qualitative variables as indicated. Quantitative data were expressed as mean ± standard deviation for parametric and median and range for non-parametric data. Independent t-tests and Mann–Whitney tests were used to calculate differences between quantitative variables in two groups for parametric and non-parametric variables, respectively. Cases with a type 1 error level (p value) of <5% were interpreted as being statistically significant. Risk ratio (RR) and the corresponding 95% confidence interval (CI) values were used to evaluate the power of the relationship and statistical significance.
Results
A total of 72 patients who met the inclusion criteria were enrolled in the study. The study compared patient outcomes between those who underwent operation with staples (n = 29) and those with sutures (n = 43) as closure methods.
Patient demographics and clinical characteristics are presented in Table 1. The mean age of the stapler group was 61.6 ± 8.2 years, whereas the suture group was slightly younger at 56.7 ± 13.8 years; however, this difference was not statistically significant (p = 0.069). BMI and weight were similar between the two groups, and no statistically significant differences were observed (p = 0.157 and p = 0.361, respectively). There were no significant differences between the groups in terms of previous abdominal operation, tobacco use, diabetes, pulmonary disease, or cardiovascular disease (p > 0.05). However, the distribution of the American Society of Anesthesiologists (ASA) classification showed a statistically significant difference, with patients in the stapler group having higher ASA scores (p = 0.015).
Patient Demographics and Clinical Characteristics
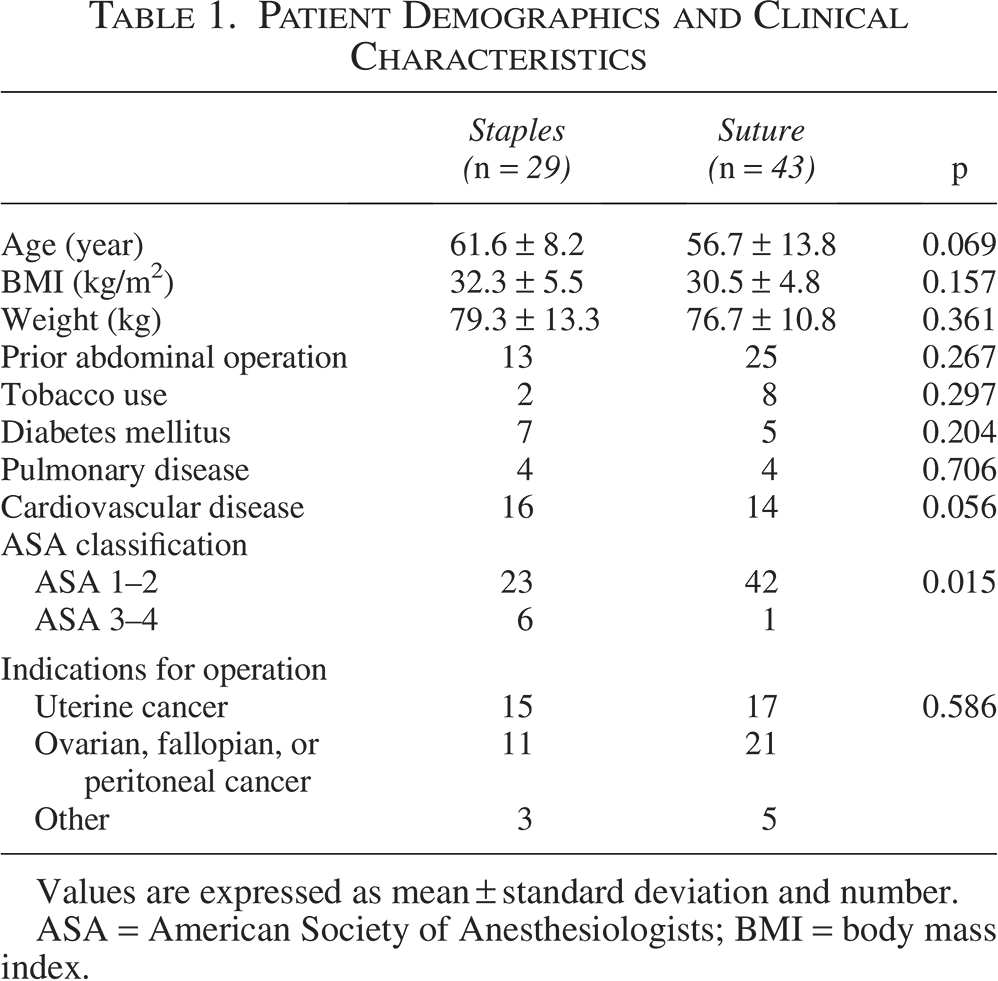
Values are expressed as mean ± standard deviation and number.
ASA = American Society of Anesthesiologists; BMI = body mass index.
Operation characteristics are shown in Table 2. Hemoglobin, hematocrit, serum glucose, and serum albumin concentrations were also compared, and a notable difference was observed in serum albumin concentrations (stapler: 34.0 ± 4.3 g/L, suture: 39.3 ± 4.6 g/L, p = 0.001). Surgical characteristics such as operative time and estimated blood loss were similar between the two groups (p > 0.05).
Operation Characteristics
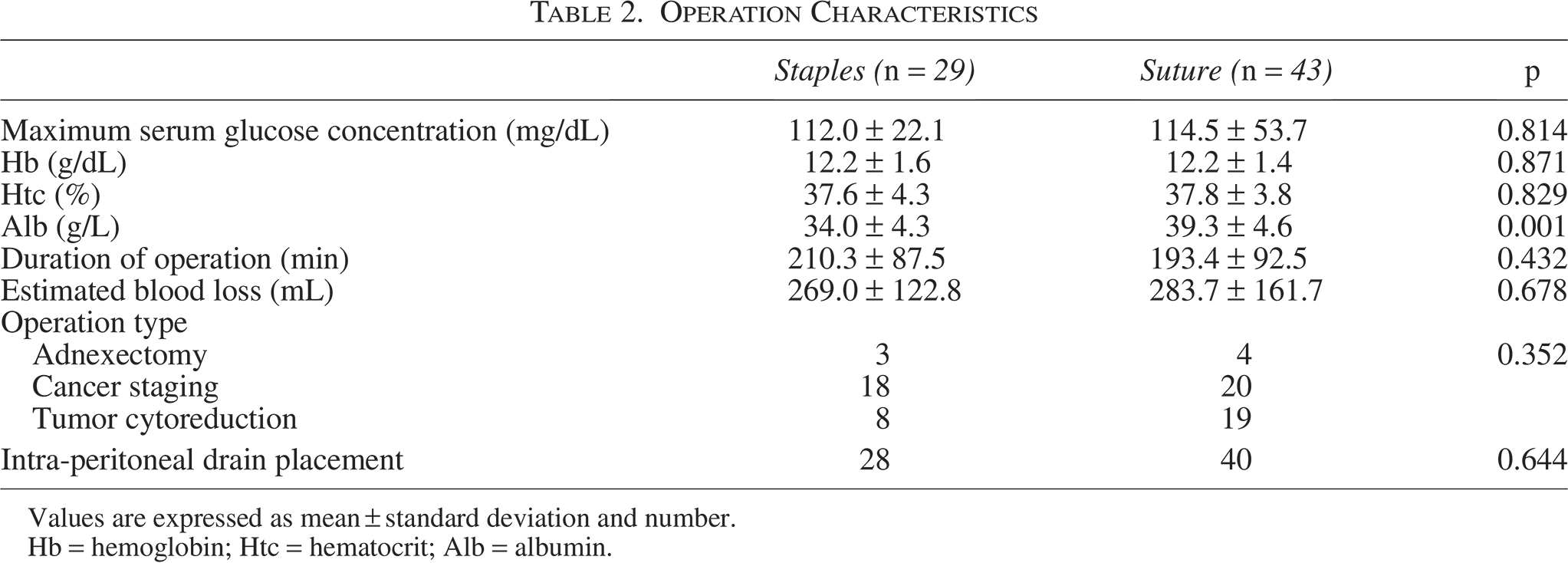
Values are expressed as mean ± standard deviation and number.
Hb = hemoglobin; Htc = hematocrit; Alb = albumin.
The comparison of post-operative outcomes between staple and suture closure revealed notable differences. Table 3 summarizes these findings. Wound complications occurred in 12 patients (41%) in the staple group and in nine patients (21%) in the suture group, indicating a trend favoring sutures, although the difference was not statistically significant (p = 0.061, RR = 1.98, 95% CI: 0.96–4.08).
Post-Operative Outcomes

Values are expressed as number and percentage.
RR = risk ratio; CI = confidence interval.
Wound dehiscence was also more frequent in the staple group, occurring in 24% of patients compared with 12% in the suture group (p = 0.204, RR = 2.08, 95% CI: 0.73–5.91). Among the 12 cases of dehiscence, 4 were identified as fascial dehiscence, with 2 cases observed in each group (p = 0.683).
Wound infections were infrequent and did not differ significantly between the two groups (p = 0.561, RR = 2.97, 95% CI: 0.28–31.22). In contrast, the risk of prolonged hospitalization was significantly higher in the staple group, with an approximately three-fold increase compared with the suture group (RR = 2.97, 95% CI: 1.13–7.78).
Discussion
This study compared post-operative wound complications in patients with overweight, obesity, and gynecologic cancer who underwent a vertical incision surgical procedure with skin closure using either staples or non-absorbable sutures.
The BMI cutoff of 25 kg/m2 was selected because wound complication rates begin to increase, even in individuals with overweight, as demonstrated by Nugent et al. Including patients with both overweight and obesity helped to ensure an adequate sample size and capture a broader at-risk population. 10
Several studies have associated factors such as BMI, diabetes mellitus history, previous abdominal operation, and operative time with wound dehiscence.9,10 Among these, an increased BMI is the most strongly associated with wound dehiscence. In our study, the BMI of patients ranged from 25.0 to 47.3 kg/m2, with an average of 31.2 ± 5.1 kg/m2. Among this population of patients with overweight and obesity, the wound complication rate (including seroma, hematoma, dehiscence, or infection requiring additional medical or surgical treatment) was 29.2%, whereas the rate of SSI was 4.2%. Nugent et al. found that wound complications began to increase at a BMI of 25 kg/m2, with patients with morbid obesity (BMI 40–49 kg/m2) being 10 times more likely to experience complications compared with those of normal weight (BMI 18.5–24.9 kg/m2). 10
Various strategies, such as placing subcutaneous drains and using subcuticular sutures, have been used to prevent wound dehiscence. For example, placing a pelvic drain has been associated with a lower risk of wound complications. Another study demonstrated that prophylactic subcutaneous retention sutures in patients undergoing gynecologic cancer operations with a vertical incision reduced wound complications and shortened hospital stays. 11 However, no patients in our study had subcutaneous drains inserted.
Few studies compare staples with non-absorbable sutures. One study, involving non-gynecologic patients with clean wounds, found no significant difference between the two closure methods. However, in the infected/contaminated wound group, the use of staples had a positive effect on outcomes. Conversely, tight application of sutures was found to increase the risk of wound complications in patients with infected/contaminated wounds. 12 The recently published “Preventing Surgical Site Infection After Colorectal Surgery” consensus concluded that there was insufficient evidence to recommend either staples or subcuticular sutures for wound closure. 13 A randomized controlled trial on wound closure after a hepatobiliary surgical procedure found that subcuticular sutures might reduce SSIs compared with staples, although the difference was not statistically significant. 14
Studies have also compared staples and sutures in an obstetric surgical procedure. Two meta-analyses of randomized controlled trials demonstrated a two-fold increase in wound complications with staple closure in cesarean deliveries. Tuuli et al. reported a wound complication rate of 13.4% (107 of 803) with staples, compared with 6.6% (45 of 684) with sutures. 7 Similarly, Clay et al. reported wound complication rates of 13.0% (50 of 385) with staples versus 5.7% (28 of 492) with sutures, with a pooled odds ratio of 2.11 (95% CI: 1.29–3.48). 8 However, a Cochrane review of these studies concluded that there is no definitive evidence on the best method of skin closure after cesarean section. 15
Malnutrition, particularly hypoalbuminemia, has been extensively studied as a predictor of post-operative complications, including SSI. Previous research has established that low serum albumin concentrations increase the risk of SSI and other infections, particularly in major surgical procedures such as gynecologic cancer and non-gynecologic surgical procedures.16,17 In line with these findings, low serum albumin concentrations were found to be a significant risk factor for deep or organ space SSI.18,19 Our study similarly found that serum albumin concentrations were significantly lower in the staples group (34.0 g/L vs. 39.3 g/L, p = 0.001), which may have contributed to poorer wound healing and the increased risk of complications associated with staples.
In a study of gynecologic oncology patients, it was observed that SSI prolonged hospital stays, and in a quarter of these patients, adjuvant treatment was either delayed or canceled. 4 This UK-based study identified BMI as the most significant risk factor for SSI, consistent with previous studies. Staples used for wound closure also emerged as a risk factor. 4 In our study, hospital stays were significantly longer in the staples group, although no statistically significant difference was found regarding wound SSI rates.
A recent review suggested that evidence on the optimal skin closure technique in gynecologic oncologic operations remains unclear, although it recommends avoiding staples for skin closure. 20
Our findings should be interpreted with caution because of several methodologic limitations. One of the primary limitations was the relatively small sample size, which may have reduced the ability to detect moderate differences between groups. Although the observed trends appeared clinically relevant, they did not consistently reach statistical significance. This underlines the importance of future studies with larger and statistically powered cohorts.
Benign cases were intentionally excluded to reduce clinical heterogeneity, as oncologic surgical procedures are typically more extensive and require timely initiation of adjuvant therapy. Furthermore, benign gynecologic conditions are more often managed with minimally invasive approaches, making them fundamentally different in surgical scope and recovery.
To our knowledge, only a few studies have directly compared staples and non-absorbable sutures in the context of gynecologic oncology. By focusing on this specific population, our study addresses an important gap in the existing literature.
Lastly, because of the retrospective design of the study, we were unable to evaluate cosmetic outcomes or post-operative pain related to wound closure methods. These parameters represent valuable areas for future research.
Future larger scale studies with standardized closure techniques and long-term follow-up are needed to clarify the role of wound closure methods in gynecologic oncology patients.
Conclusion
In this retrospective study of patients with overweight, obesity, and gynecologic cancer undergoing vertical incision surgery, staple closure was associated with a higher rate of wound complications and a significantly longer hospital stay compared with suture closure. Although not all differences reached statistical significance, the clinical trends observed suggest that suture closure may be preferable in this patient population.
Given the limited number of studies comparing these two methods in gynecologic oncology, our findings contribute to the growing body of evidence on optimal wound management strategies.
This study may serve as a preliminary step for future guideline development on wound closure techniques in gynecologic oncology.
Authors’ Contributions
Concept: F.C.G., E.I., and T.Ş. Design: F.C.G. and E.I. Data collection or processing: F.C.G. and E.I. Analysis or interpretation: F.C.G., E.I., S.D., H.A.T., and T.Ş. Literature search: F.C.G., E.I., S.D., H.A.T., and T.Ş. Writing: F.C.G. and E.I. Critical review: S.D., H.A.T., and T.Ş.
Footnotes
Acknowledgments
The authors acknowledge all the healthcare professionals who have contributed to the care of their patients.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors declared that this study received no financial support.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Committee Approval
The study was approved by the Committee of Ethics of Akdeniz University Faculty of Medicine (KBAEK-26).