
Abstract
Background and Objectives:
Historically, a triple-antibiotic (TA) regimen (ampicillin, gentamicin, metronidazole) has been used for children with complicated appendicitis (CA) at our institution. We implemented a double-antibiotic (DA) regimen (ceftriaxone, metronidazole) in November 2018. The aim of this study was to compare the post-operative outcomes between the two groups.
Patients and Methods:
Clinical and laboratory data were collected from the medical records of children who underwent laparoscopic appendicectomy (LA) for CA between November 2017 and 2019. Data, reported as number of cases (%) and median with interquartile range or 95% confidence interval (CI), were analyzed with Fisher exact test and Mann-Whitney U test; p values <0.05 were considered significant.
Results:
One hundred and ninety-seven patients were identified; 99 treated with the TA regimen and 98 with the DA regimen. The groups had similar demographics. Post-operative complications were similar between the two groups: intra-abdominal abscess (IAA) 12 (12.1%) in TA versus 10 (10.2%) in DA (p = 0.82); surgical site infections 1 (1.0%) in TA versus 2 (2.2%) in DA (p = 0.62). Time to defervescence in the first 5 post-operative days was substantially longer in the TA group: 72 (95% CI 72–96) versus 48 (95% CI 48–72) hours (p = 0.003). Among patients without post-operative IAA, the DA group had a shorter post-operative hospital stay (5 [5–6] vs. 5.5 [5–6] days; p = 0.04). The cost of DA regimen was substantially lower (p < 0.0001).
Conclusions:
The DA regimen provided better post-operative temperature control and a quicker overall recovery, without increasing the incidence of IAA and surgical site infection in children following LA for CA.
Acute appendicitis is one of the most common surgical emergencies worldwide, with an estimated lifetime risk reported to be 7%–8%. 1
From a clinical perspective, acute appendicitis can be categorized as simple appendicitis (SA) or complicated appendicitis (CA); the latter is defined if one or more of the following intra-operative features are present: macroscopic perforation or four quadrant pus or intra-abdominal mass/abscess or free fecalith.2,3
Post-operative intra-abdominal abscess (IAA) remains an important complication in children with CA, developing in as high as 20% of cases, a much greater risk when compared with patients with SA. 3
Therefore, patients with CA often require a prolonged course of antibiotics to control infectious complications after appendicectomy. Different regimes of antibiotics are advocated in CA compared with SA and depend on a number of factors including local hospital guidelines.4,5 Traditionally, the “triple antibiotic” (TA) regimen, consisting of ampicillin, gentamicin, and metronidazole (or clindamycin), has been administered to patients with CA for as long as 10 days and continues to be the “gold standard” antibiotic tactic in many institutions. 6 The TA regimen requires administration of each antibiotic dose several times a day; in addition, the aminoglycoside gentamicin is known to have relatively narrow therapeutic ranges and associated problems of ototoxicity and nephrotoxicity. 7 Consequently, the use of gentamicin is coupled with tight serial blood sampling for measurement of serum concentration in order to maintain safe, non-toxic, and therapeutic windows. The dosing schedule and the gentamicin toxicity, with need for monitoring of therapeutic concentrations, have led to shifts away from this traditional TA regimen.7–11 The use of monotherapy with piperacillin–tazobactam has been recently proven to reduce the risk of post-operative IAA when compared with double therapy with ceftriaxone and metronidazole in children with CA. 12
Undeniably, substantial discrepancies exist in many aspects of care provided by practicing pediatric surgeons regarding the choice of antibiotics regimen.4,5 This can also be explained by the difference in local practice guidelines and constantly evolving strains and emergence of bacterial resistance to the antimicrobial therapy instituted.
At our institution, there was a shift from TA to a “double antibiotic” (DA) regimen in November 2018 for children with CA; the shift was driven by the concerns related to the ototoxicity and nephrotoxicity with the use of gentamicin.
The aim of this article was to evaluate if the DA regimen is an effective therapy for prevention of post-operative infectious complications when compared with the TA regimen in children undergoing laparoscopic appendicectomy (LA) for CA.
Patients and Methods
After obtaining institutional review board approval (RES-19-0000-797Q), the records of all pediatric patients below 18 years of age who underwent LA for CA (defined in the presence of macroscopic perforation and/or four quadrant pus and/or intra-abdominal mass/abscess or free fecalith) between November 2017 and November 2019 were reviewed. In November 2018, our institution implemented a change in antibiotics regimen from a TA regimen (ampicillin, gentamicin, metronidazole) to a DA regimen (ceftriaxone, metronidazole).
Laparoscopic standard technique (1 × 10 mm port at the umbilicus, 2 × 5 mm ports in suprapubic region and left iliac fossa) was utilized; after dissection, the appendix base was ligated with Endoloop® PDS® II (Ethicon, Somerville, NJ, USA), resected and removed in an EndocatchTM bag (Medtronic, Minneapolis, MN, USA) in all cases. Fecal material and purulent fluid were aspirated and the abdomen washed out with up to 2,000 mL of physiologic saline. Intraperitoneal fluid microscopy and culture were not routinely taken.
All patients received intravenous antibiotics before starting the procedure and post-operatively for 5 days according to the following doses and schedule: patients receiving the TA regimen were administered ampicillin (50 mg/kg/dose, every 6 h), gentamicin (6–7.5 mg/kg/dose, daily), and metronidazole (7.5 mg/kg/dose, every 8 h); patients receiving the DA regimen were administered once daily dosing of ceftriaxone (50 mg/kg) and thrice daily dosing of metronidazole (15 mg/kg/dose, every 8 h). The TA group had serum gentamicin concentration checked after the third dose, and the doses titrated accordingly to a safe pre-dose (trough) concentration of <1 mg/L.
Patients with immunosuppression or history of serious allergy to study drugs and therefore subject to a different antibiotic regimen were excluded from the study. Patients were discharged home after 5 days of post-operative intravenous antibiotics if they were apyrexial for 48 hours, tolerating oral intake and managing pain with oral paracetamol only.
Data obtained included baseline patients’ demographics (age, gender, and weight), clinical data on admission including duration of symptoms and fever, blood results including full blood count and C-reactive protein, post-operative gentamicin serum concentrations, complications including IAA and surgical site infection, length of hospital stay, readmission, reoperation, and return to emergency department within 60 days of operation.
Data are reported as number of cases (%), median with interquartile range, or 95% confidence interval (95% CI) for continuous variables. Normality was confirmed using D’Agostino-Pearson test. Fisher exact test and Mann-Whitney U test were performed as appropriate with p value <0.05 considered statistically significant. All statistical analyses were conducted using GraphPad Prism 9 (GraphPad Software, La Jolla, CA, USA).
Results
A total of 569 patients underwent LA for acute appendicitis during the study period; 291 patients were admitted from November 2017 to October 2018, whereas 278 patients were admitted from November 2018 to November 2019. After exclusion of SA, the final cohort with CA contained 99/291 (31%) patients in the TA group and 98/278 (35%) patients in the DA group. Baseline demographic, clinical, and biochemical characteristics of patients are presented in Table 1. Operative data are presented in Table 2. All patients in both groups underwent LA without needing conversion to laparotomy. There were no statistically significant differences in regard to the presence of frank pus, perforation, or the distribution of purulent fluid intra-abdominally. The median duration of post-operative intravenous antibiotic therapy was similar between the two groups: 5 (5–6) days in the TA group and 5 (5–6) days in the DA group; p = 0.66. The incidence of post-operative infections was similar between the groups and is presented in Table 3.
Baseline Demographic and Clinical Characteristics of Patients on the Day of Admission: Number of Case (%), Median, and Interquartile Range
DA = double-antibiotic regime; TA = triple-antibiotic regimen.
Intraoperative Data: Number of Cases (%)
DA = double-antibiotic regime; TA = triple-antibiotic regimen.
Post-Operative Clinical Outcomes: Number of Cases (%)
DA = double-antibiotic regime; TA = triple-antibiotic regimen.
IAA was diagnosed in 22 (11%) children. Of those who developed IAA, 50% from both groups were diagnosed and treated prior to discharge. There were no differences in the management of IAA between the two groups (Table 4).
Patients with Post-Operative Intra-Abdominal Collection: Number of Case (%), Median, and Interquartile Range
DA = double-antibiotic regime; IAA = intrabdominal abscess; IAC = intrabdominal collection; TA = triple-antibiotic regimen.
Among patients without post-operative IAA, in the TA group there was a slightly longer post-operative stay (TA 5.5 [5–6] vs. DA 5 [5–6] days; p = 0.04).
Ten patients (10.1%) in the TA group and 8 patients (8.2%) in the DA group represented to the emergency department within 30 days post-discharge (p = 0.81): 6 patients from the TA group and 5 patients from the DA group were re-admitted with diagnosis of IAA; other reasons for representation included: fever (no cause identified TA n = 1); fever secondary to rhinovirus infection (TA n = 1); recurrent abdominal pain (TA n = 2, DA n = 2). One patient in the DA group was readmitted with adhesion obstruction that was conservatively managed.
One patient in the TA group, with persisting post-operative diarrhea during the hospital admission, was diagnosed with Clostridium difficile infection from the stool specimen.
Time to defervescence in the first 5 post-operative days was substantially longer in the TA group (72 h, 95% CI 72–96) compared with to the DA group (48 h, 95% CI: 48–72); p = 0.003 (Fig. 1).
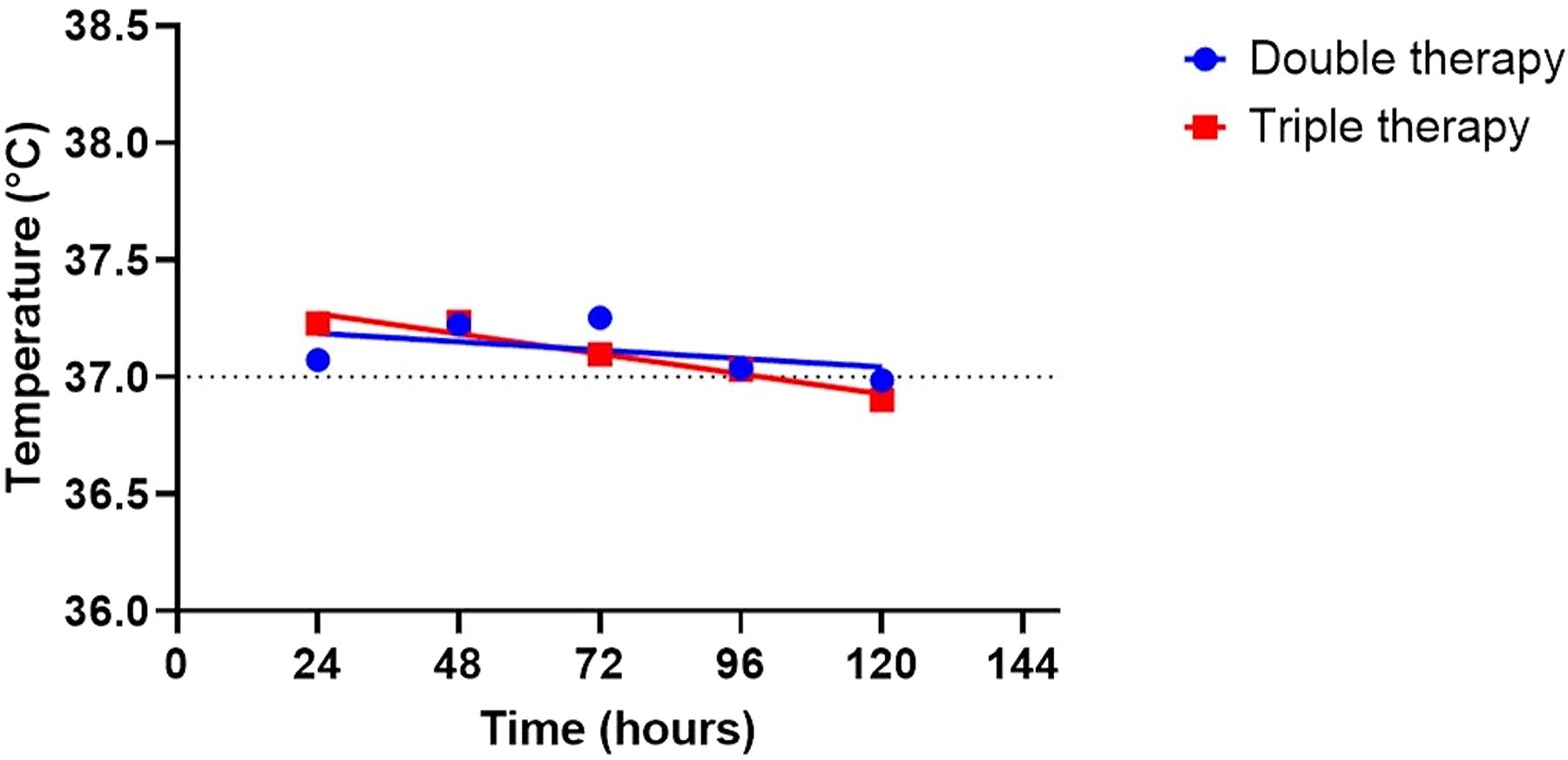
Mean maximum daily temperature regimen in each of the first 5 post-operative days.
Regarding the serum gentamicin concentration analysis, a total of 151 blood draws were required for the 99 patients in the TA group; no clinically useful gentamicin concentrations were found in 16 patients (16.2%) because of insufficient specimen collection. Thirty-nine patients (39.4%) receiving gentamicin were found to have a safe and therapeutic level from the outset, whereas the remainder spent a portion of their hospital stay at below the therapeutic level (19 patients [19.2%]), above the therapeutic level (13 patients [13.1%]), or both above and below therapeutic levels (12 patients [12.1%]). No patients in either group developed acute kidney injury, rash, or other known adverse reactions to the antibiotics.
Throughout the admission, the median cost of the antibiotic treatment alone per patient in the TA regimen was AUD 49.56 (33.30–77.22), being substantially more expensive than in the DA regimen of AUD 23.15 (14.49–31.13) (p < 0.0001).
Discussion
Our study has shown that the DA regimen is as effective as the TA in preventing IAA and surgical site infection following LA for CA in children. Although our study was a retrospective case–control study, it focuses on a large population of children; another strength of our study includes the equivalence between the two groups in terms of demographics and clinical presentation with the exception of a slightly greater median temperature in the TA group at presentation. Furthermore, all patients received a standardized LA and 5-day course of intravenous antibiotics.
Similar to our findings, in their randomized controlled trial of 100 patients, St Peter et al. found that DA with ceftriaxone and metronidazole was equally effective as their TA regimen of ampicillin, gentamicin, and clindamycin in preventing post-operative IAA and surgical site infection. 11 More recently, the same group reported the results of a randomized controlled trial in children undergoing LA for CA using monotherapy with piperacillin-tazobactam that has proven to substantially reduce the risk of post-operative IAA when compared with to double therapy with ceftriaxone and metronidazole (6.1% vs. 23.8%, odds ratio 4.80, p < 0.002). 12 At present, in our institution, based on directives from the infection disease team, in order to reduce the incidence of antibiotic resistance, the use of piperacillin–tazobactam is considered a second-line therapy, reserved for patients who develop post-operative IAA while on ceftriaxone and metronidazole.
Interestingly, the incidence of IAA in our study (11%) is lower than other studies with reported rates greater than 20% (7–12). The high rate of post-operative IAA (16% in TA regimen and 20% in DA regimen) reported by St Peter et al. could be attributed to the median longer duration of symptoms (3.0 d in the TA regimen and 3.2 d in the DA regimen) at presentation compared with our cohort (2 d in the TA regimen and 3 d in the DA regimen) and their use of once-daily dosing of metronidazole compared with thrice-daily dosing of metronidazole in our study. 11 However, an in vitro study examining once-daily dosing of metronidazole compared with thrice-daily dosing regimen demonstrated that they were equally bactericidal against strains of Bacteroides fragilis. 13
Dreznik et al. also found that the DA regimen with ceftriaxone and metronidazole was as clinically effective as the TA regimen (ampicillin, gentamicin, metronidazole) in children with CA after appendicectomy in preventing IAA and surgical site infections (9). However, it should be noted that in this study all patients underwent open appendicectomy, meaning their results are not necessarily comparable with our cohort of patients undergoing LA.
We found a low rate of surgical site infections in both groups (1%–2.2%) when compared with other studies such as those from Dalgic et al. and Dreznik et al., which showed rates of up to 5%–6%.8,9 The greater rate of surgical site infections could be associated with the use of open appendicectomy in these studies. In addition, we always retrieve the appendix using the Endocatch bag (Medtronic), which might also contribute to the low incidence of surgical site infections in our cohort. Indeed, St Peter et al., in patients undergoing LA, reported an equally low rate of surgical site infections as our study (of up to 2%). 11 This is further supported by the lower rate of surgical site infections observed after LA in both children and in adults, when compared with open appendicectomy, based on a systematic review of 85 trials. 14
Time to defervescence is often used as a surrogate of formation of post-operative IAA, as longer periods of fever are associated with greater rates of abscess formation. 15 Although differences in IAA were not found between the TA and the DA groups in our study, time to defervescence was substantially shorter in the DA group. Similarly, St Peter et al. and Hurst et al. found their DA regimen with ceftriaxone and metronidazole was able to achieve quicker defervescence from post-operative day 1 onward when compared with the TA regimen.10,16 However, in St Peter et al.’s study, there was a greater number of patients in the DA regimen group undergoing LA than in the TA regimen where there were more patients undergoing open appendicectomy. In our study, the quicker defervescence could be explained by the substantial portion (31%) of patients in the TA regimen group having subtherapeutic doses of gentamicin, during part or whole of their index admission. Difficulty in achieving uniformly therapeutic levels of gentamicin was not only encountered in the TA group in our study but also is a well-known phenomenon in literature. 11 Substantial discrepancies also exist in different pediatric units on gentamicin dosing policy and therapeutic drug monitoring. 17 Over half of our patients required at least one change in dose of gentamicin because of it being in either supratherapeutic or subtherapeutic level. The randomized controlled trial by St Peter et al. did not identify a difference in defervescence rate. 11
The potential nephrotoxic and ototoxic nature of gentamicin are recognized causes of concern. In pediatric patients, the rate of aminoglycoside-related ototoxicity is reported to be 2.0%–2.3%. 18 In our cohort, no concern was raised on hearing malfunction while the patients were inpatient or on follow-up visits.
Aminoglycoside-induced nephrotoxicity is also a well-known side effect associated with increased hospital stay and hospital costs, and its true incidence may be underrepresented.19–21 In our cohort, only 55% patients from the TA regimen and 47% patients from the DA regimen had serial measurement of their renal function at various time point intervals from admission, none of which showed acute kidney injury. Furthermore, in 16% of patients of the TA regimen, we encountered errors in collecting enough serum specimen for accurate measurement of gentamicin levels, highlighting the issue of practicality and non-adherence with gentamicin administration.
Our study also identified, in patients without post-operative complications, a slightly longer post-operative hospital stay in the TA regimen group compared with the DA regimen group; this could be explained by the earlier defervescence in patients in the DA regimen group because patients were discharged when apyrexial for 48 hours. We also identified a reduced cost per patient for the antibiotics with the use of the DA regimen. The shorter hospital stay could portend savings on the healthcare system, although we were not able to explore this in the details owing to the retrospective nature of our study.
There are several limitations of this study. Owing to the retrospective nature of our study, the rate of aminoglycoside-related ototoxicity was not actively sought out or screened at follow-up; thus, subtle hearing dysfunction could have been under-appreciated. In addition, we were not able to detail the use of antipyretics in our patients, which could potentially serve as an important confounding parameter.
A further limitation of our study is a 10%–12% loss of patients to follow-up that could compound on the true incidence of complications, but the rate of patients lost to follow-up was similar in both groups (p = 0.63). Considering the geographical distribution of hospitals with pediatric surgery units in our state, we can safely assume that patients with IAA would have represented to our hospital.
In conclusion, our study confirms that DA regimen with ceftriaxone and metronidazole, when used in children following LA for CA, provides similar outcomes to the TA regimen. By offering simpler dosing schedule and negating the need for regular serum monitoring of gentamicin level, the DA regimen lessens the expense, and reduces demands on patient, nursing staff and pharmacy staff. These advantages will result in greater satisfaction among patients and nursing staff over time.
Further randomized controlled studies of suitable antibiotic regimens investigating not only their clinical effectiveness but also their cost-effectiveness, patient-reported outcomes, and profile of microbial resistance are required to continually inform the local health policies on the optimal antibiotic regimen for complicated appendicitis in the pediatric population.
Footnotes
Authors’ Contributions
Study concepts and design: M.P. Data acquisition: K.-Z.L. Quality control of data and algorithms: K.-Z.L., R.M.N., and M.P. Data analysis and interpretation: K.-Z.L. and M.P. Statistical analysis: K.-Z.L. and M.P. Manuscript preparation: K.-Z.L. Manuscript editing: K.-Z.L., R.M.N., and M.P. Manuscript review: K.-Z.L., R.M.N., and M.P.
Author Disclosure Statement
The authors have no personal or financial conflict of interest to disclose.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.