
Abstract
Introduction:
Peritoneal carcinomatosis (PC) patients undergoing cytoreductive surgery (CRS) combined with hyperthermic intraperitoneal chemotherapy (HIPEC) face a high risk of morbidity. Surgical site infections (SSIs) are among the main contributors to this issue. This relation is influenced not only by the effects of major surgical resections but also by the hemodynamic changes induced by HIPEC. Although elevated lactate levels (LL) have been associated with greater complication rates in CRS-HIPEC patients, their direct association with the development of SSIs has not been thoroughly investigated.
Methods:
Patients who underwent CRS + HIPEC were retrospectively reviewed. Pre-operative demographic data, hemodynamic parameters and records, transfusion records, and all post-operative follow-up and treatment records were analyzed. Patients were categorized into SSI+ and SSI−. Factors contributing to SSI development were examined using regression analysis.
Results:
A total of 110 patients who underwent CRS + HIPEC between January 2018 and December 2021 were included in the study. LL obtained at intensive care unit (ICU) admission were greater in patients who developed SSIs (p = 0.020). Cutoff point for ICU admission LL in diagnosing SSI was ≥6 mmol/L (area under the curve: 0.640 [0.526–0.753], p = 0.020). SSI development (23% vs. 50%, p = 0.003) was more prevalent in patients with lactate values ≥6 mmol/L. In multi-variable analysis, LL ≥6 mmol/L (odds ratio [OR]: 4.614, p = 0.005) and clean-contaminated wounds (OR: 27.677, p = 0.002) were related with increased SSI development.
Conclusion:
In patients with PC, LL of 6 mmol/L or greater during the ICU stay have been associated with SSI development. For this high-risk patient subgroup, a readily available peri-operative parameter such as lactate may guide prophylactic antibiotic selection. However, despite its high specificity, the low sensitivity of our findings should be carefully considered before clinical decision-making. Further studies analyzing larger, more homogeneous cohorts are needed to better clarify the relation between LL, SSI development, and prophylactic antibiotic use.
Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) are an effective treatment choice for several advanced oncologic conditions. However, the potential for incomplete resection and post-operative toxicity risk limit its use to carefully selected cases. 1 Post-operative complications can delay adjuvant therapy. 2 Surgical site infections (SSIs) are a leading cause among these complications, often cause for relaparotomy, prolonged hospitalization, and greater mortality rates. 3
Factors such as transfusion or prolonged operation can affect hemodynamic stability and perfusion during this complex protocol. Notably, patients undergoing CRS demonstrate greater increases in lactate levels (LL) compared with those undergoing other major oncologic surgical procedures; these effects being further intensified by the addition of HIPEC. 4
Among studies related to CRS + HIPEC in peritoneal carcinomatosis (PC), hypothermia, prolonged hospitalization, extended surgery duration, prolonged drainage, catheter use, extended post-operative intubation, the immunosuppressive effects of HIPEC, and prevalent malnutrition have been shown to contribute to SSIs.5,6 In a similar study, LL ≥2.5 mmol/L were found to increase early complications in intensive care units (ICUs). Elevated LL are indicative of tissue hypoperfusion, which compromises immune function and increases susceptibility to infections, including SSIs. 7 Therefore, monitoring LL may help predict the risk of SSIs.
Currently, no studies have evaluated the relation between LL and the development of SSIs in CRS + HIPEC procedures. This study aims to examine the association between pre-operative and post-operative LL and the incidence of SSIs in patients treated with CRS + HIPEC.
Patients and Methods
Study design
The approval gained from the Ethics Committee of Kosuyolu High Specialization Training and Research Hospital was dated August 09, 2022 and numbered 2022/11/618. Records of patients who underwent CRS + HIPEC procedure at the same center’s Department of Gastrointestinal Surgery between January 01, 2018 and December 31, 2021 were reviewed. Patients who underwent elective curative operations for histologically confirmed gastric, ovarian, or colorectal malignant diseases, malignant mesothelioma, and Pseudomyxoma Peritonei (PP) were retrospectively analyzed. Because of the study’s retrospective nature, informed consent was not obtained.
Patient selection
Patients with a history of palliative surgical procedure, inadequate cytoreduction, insufficient follow-up data on surgical, laboratory, and clinical outcomes, those with evidence of hemolysis, pancytopenia, or missing culture results, patients with an Eastern Cooperative Oncology Group performance status score 8 of ≥3, Peritoneal Cancer Index (PCI) >18 for colon cancer, PCI >10 for gastric cancer, or sarcomatoid malignant mesothelioma were excluded, as well as those with extra-abdominal metastasis, centralization, or mesenteric root involvement.
Patients with hemoglobin ≤8 gm/dL without cardiovascular disease or ≤10 gm/dL with cardiovascular comorbidities received blood transfusions before operation. The Prognostic Nutritional Index was used to assess nutritional status. 9 Patients with PC who met our inclusion criteria were initially evaluated for CRS/HIPEC. However, patients who developed sustained MAP <65 mm Hg for more than one hour and experienced major vascular injury, prolonged hypothermia, or hemodynamic instability during cytoreduction were excluded from receiving HIPEC to prevent additional morbidity and therefore excluded from the study. Similarly, patients who underwent HIPEC but subsequently developed these complications requiring modification of the planned surgical procedure were also excluded from analysis to prevent bias in lactate measurements between groups, as these conditions could independently impact both LL and the standard surgical approach and affect post-operative outcomes.10–15
To avoid bias in SSI development or lactate evaluation, patients with intra-abdominal abscesses, tumor perforation, or hemodynamic instability during operation were excluded. In addition, patients with severe cardiac arrhythmias, heart failure, chronic obstructive pulmonary disease, asthma, or chronic kidney/liver disease were excluded, as they were not candidates for CRS + HIPEC. Surgical procedures intended for prophylactic HIPEC candidates were also excluded.
Patient preparation and evaluation
The comorbidities, surgical history, nutritional status, and surgical risk scores of all patients were systematically extracted from medical records, including pre-operative consultant notes. All operations were managed by a single anesthesia team. Central catheterization and pre-operative lactate assessments were conducted during the pre-operative period. Epidural catheterization was used for post-operative analgesia in patients without contraindications. For eligible patients, an epidural analgesic solution of 20 cc fentanyl and 5 cc Marcaine diluted in 100 cc of 5% NaCl was administered at 2 cc/h/kg. This regimen was maintained for three days unless contraindicated, after which epidural catheters were removed. Intravenous cefazolin prophylaxis (2 grams) was administered 60 minutes before surgical procedure and repeated every three hours. Patients undergoing or planned for colectomy also received 500 mg metronidazole and repeated every seven hours. Post-operatively, prophylactic ceftriaxone and metronidazole were continued until the third post-operative day in patients without allergies. In addition, mechanical bowel preparation, consisting of two rectal enemas and oral laxatives, was performed for all patients regardless of diagnosis. Intravenous fluid replacements were provided pre-operatively to prevent fluid loss.
Surgical procedure and post-operative follow-up
Drug dosages were determined on the basis of Peritoneal Surface Oncology Group International recommendations.11–13,15,16 For colorectal and appendiceal cancers, intravenous 5-fluorouracil (400 mg/m2) and intraperitoneal oxaliplatin (360 mg/m2) were administered over 30–60 minutes. For ovarian cancers, cisplatin (80 mg/m2) was given over 60 minutes. For gastric cancers and mesotheliomas, cisplatin (50 mg/m2) and doxorubicin (15 mg/m2) were administered over 60 minutes. Patients who had previously received chemotherapy underwent operation at least 30 days after their last session, extended to 6 weeks for those treated with bevacizumab.
The CRS + HIPEC procedures followed the open technique by Sugarbaker et al. 17 Patients were mobilized on the first post-operative day when feasible, and respiratory physiotherapy started immediately after extubation. Urinary catheters were removed upon ward admission if monitoring was unnecessary, and central venous catheters were removed post-oral intake if peripheral access was established. Drains were removed as clinically appropriate. Culture samples from blood, urine, percutaneous drainage, and wound were obtained on the basis of clinical presentations. Infectious disease specialists were managing treatment and adjusting antibiotic agents on the basis of culture results. Peri-operative vital signs, urine output, serum glucose concentrations, and fluid balances were recorded from anesthesia documents. Arterial blood gas tests were routinely performed peri-operatively, at operation onset, every 90 minutes, and during HIPEC, with LL recorded. Data collection continued during post-operative ICU admission.
Measurements
The recorded data included operation duration, types and amounts of intravenous fluids and transfusions, occurrences of hypothermia or hyperthermia, estimated blood loss, intraoperative body temperatures, fluid balance, medications and dosages during HIPEC, PCI scores, Completeness of Cytoreduction Scores, 18 and LL measurements at baseline, 3rd, and 6th hours, during HIPEC, upon ICU admission, and at 3rd, 6th, 9th, and 12th hours in the ICU. SSIs were classified on the basis of the Centers for Disease Control and Prevention’s 1999 guidelines and its 2017 update into Superficial Incisional SSI (SiSSI), Deep Incisional SSI (DiSSI), and Organ/Space SSI (OsSSI).19,20 Patients were categorized as SSI+ if an infection was present and SSI− if absent. Demographic and clinical data, diagnoses, intraoperative measurements, peri-operative and post-operative LL, post-operative complications, and length of hospital stay were compared between the groups. Post-operative complications were graded using the Clavien–Dindo system, with grades ≥3 classified as major and grades ≤2 as minor. 21
Statistical analyses
Statistical analyses were performed using SPSS 27.0 (SPSS Inc., Chicago, IL). The Kolmogorov–Smirnov test assessed normality for quantitative variables. The Mann–Whitney U test was used for non-normally distributed variables, whereas chi-square analysis evaluated associations between qualitative variables. ROC analysis determined the optimal LL cutoff at ICU admission for predicting SSI risk, reporting sensitivity and specificity. Non-normally distributed quantitative variables are presented as median (25th–75th percentile) and qualitative variables as frequencies (%). LL, PCI, wound classification (which is known to be associated with SSI), age, history of diabetes mellitus or smoking, the presence of colon resection, anastomosis, and ASA scores were included in the regression analysis. p-Value <0.05 was considered statistically significant.
Results
A total of 110 patients had undergone CRS + HIPEC. Fifty-one patients underwent surgical procedure for colorectal cancer, 20 for PP, 12 for gastric cancer, 18 for ovarian cancer, and 9 for mesothelioma, all undergoing CRS + HIPEC. The SSI− group comprised 76 patients, whereas the SSI+ group included 34 patients. Among the SSI+ group, SiSSI was observed in 26 patients, DiSSI in 11 patients, and OsSSI in 11 patients.
Culture samples were collected from 47 patients with SiSSI or DiSSI, yielding pathogen growth in 24 cases. Pathogen growth was observed in 10 of 20 drainage catheter cultures, 1 of 11 central catheter cultures, 6 of 23 blood cultures, and 9 of 31 urine cultures. Among the patients with SiSSI or DiSSI, 22 cases required local wound exploration and follow-up in addition to antibiotic therapy. Vacuum-assisted closure was used in 4 patients, whereas wound debridement and primary skin closure were performed in 9 patients because of the occurrence of evisceration (Table 1).
The Pathogens Isolated from Surgical Sites and Other Infections in Patients Who Developed Infections Include
SiSSI = superficial incisional surgical site infection; DiSSI = deep incisional surgical site infection; OsSSI = organ/space surgical site infection.
In the pre-operative analysis, Class II wounds (64.5% vs. 97.1%) and PCI of ≥8 were substantially more common in SSI+ patients (58.8% vs. 38.1%; p = 0.044). Major complications were more frequent in the SSI+ group (61.7% vs. 13.1%; p < 0.001). Although no 30-day mortality occurred in the SSI− group, two deaths were reported in the SSI+ group (0% vs. 5.8%; p = 0.033). Gastrointestinal anastomosis rates were similar between groups (73.6% vs. 76.4%; p = 0.757). Reoperation rates were greater in SSI+ patients (23.5% vs. 6.6%; p = 0.011), as were enterocutaneous fistulas (11.7% vs. 0%; p = 0.002) and pancreatic fistulas (20.5% vs. 2.6%; p < 0.001). Additional complications such as nephrotoxicity (29.4% vs. 6.5%; p = 0.001), pneumonia (23.5% vs. 3.9%; p = 0.002), and pleural effusion (29.4% vs. 7.8%; p = 0.003) were also more frequent in SSI+ patients. Reoperations in the SSI− group included cases of bleeding (n = 3) and visceral evisceration (n = 2), whereas the SSI+ group included anastomotic leaks (n = 2), enteroatmospheric fistulas (n = 2), uncontrolled bleeding (n = 2), ileostomy necrosis (n = 1), and visceral evisceration (n = 1). ICU stays were longer in SSI+ patients (2 [1–3] vs. 1 [1–2]; p = 0.006), as were hospital stays (16 [12–28.25] vs. 8 [7–12]; p < 0.001). LL at ICU admission were greater in SSI+ patients (5.05 mmol/L [4.00–6.50] vs. 4.45 mmol/L [3.70–5.00]; p = 0.020). Other demographic, surgical, and post-operative characteristics were comparable (p > 0.05) (Table 2).
Descriptive Statistics and Comparison Results of Qualitative and Quantitative Demographic and Surgery-Related Risk Factors
Only female patients included. Among these patients, 27 with TAH + BSO history excluded (n = 35).
14 total gastrectomy patients excluded (n = 96).
Patients excluded without a gastrointestinal system anastomosis (n = 82).
Colostomy and Ileostomy patients included (n = 43).
Only female patients included (n = 62).
Significant values are shown in bold. Significance levels: *p < 0.050, **p < 0.010, ***p < 0.001.
SSI = surgical site infection; HIPEC = hyperthermic intraperitoneal chemotherapy; ASA = American Society of Anesthesiology; Oxaliplatin + 5Flu-Leu = Oxaliplatin + 5-Fluorouracil + Leucovorin; CVC = central venous catheter; CCS = complete cytoreduction score; PCI = Peritoneal Cancer Index; GIS = gastrointestinal system; ICU = intensive care unit; TAH+BSO = total abdominal hysterectomy + bilateral salpingo-oophorectomy; BMI = body mass index; χ^2 = Chi-square test statistic; Z = Mann–Whitney U test statistic; † = Chi-square analysis; ‡ = Mann–Whitney U test. Descriptive statistics are presented as frequency (percentage) or median (25th–75th percentile).
ROC analysis findings for the ICU admission lactate parameter in predicting SSI are provided. Accordingly, the cutoff point for ICU admission LL in diagnosing SSI is ≥6 mmol/L (p = 0.020). The sensitivity of this cutoff point in correctly identifying true SSI cases is 47.06%, whereas the specificity in correctly identifying true healthy cases is 81.58%. The area under the curve (AUC) value is 0.640 (Fig. 1) (Table 3).
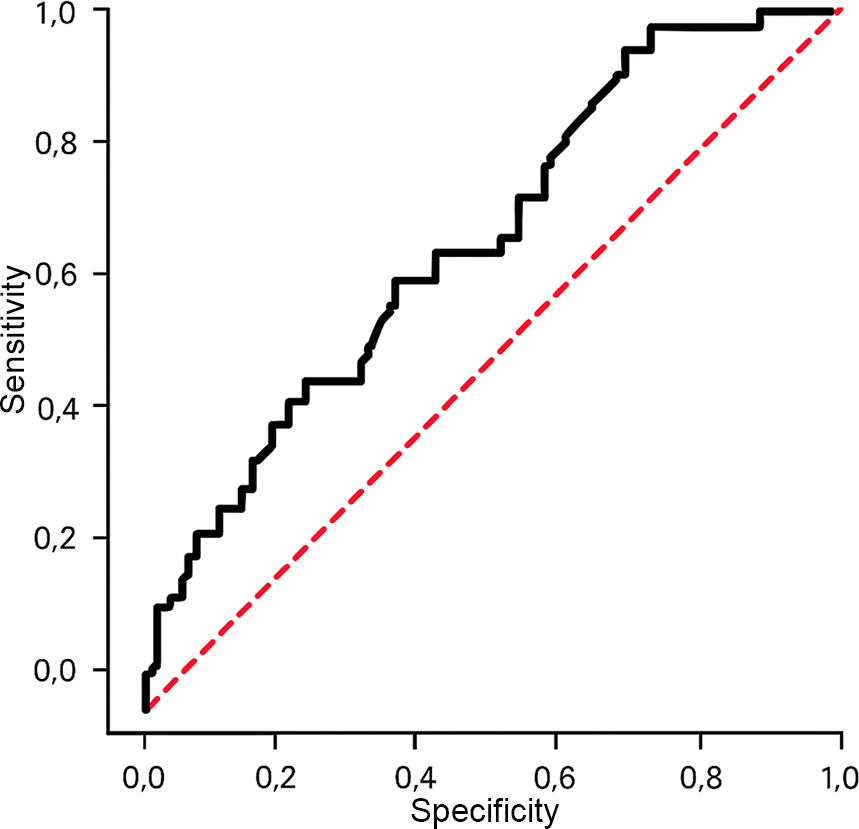
ROC curve illustrating the diagnostic performance of lactate levels in predicting surgical site infections following cytoreductive surgery with HIPEC. AUC = 0.640, p = 0.020. HIPEC = hyperthermic intraperitoneal chemotherapy; AUC = area under the curve.
Surgical Site İnfection Prediction with Intensive Care Unit Admission Lactate Variable and Applied ROC Analysis Findings
AUC = area under the curve; CI = confidence interval; SEAUC = standard error of the AUC.
Using the cutoff value of ≥6 mmol/L derived from the ROC analysis, ICU admission LL were categorized into two groups as follows: 78 patients with LL <6 mmol/L and 32 patients with ≥6 mmol/L. SSIs were substantially more common in patients with ≥6 mmol/L (50% vs. 23%, p = 0.003), as were SiSSIs (40.6% vs. 16.6%, p = 0.007). In addition, nephrotoxicity (28.2% vs. 10.2%, p = 0.019) and pancreatic fistulas (6.2% vs. 2.5%, p = 0.011) were more prevalent in this group. Patients with a PCI score of ≥8 were more frequently observed in the high-lactate group (62.5% vs. 27.1%, p = 0.015). Greater LL were associated with oxaliplatin-based regimens (81.2% vs. 57.6%), whereas cisplatin-based regimens were linked to lower LL (18.7% vs. 42.3%; p = 0.019). The high-lactate group also had shorter HIPEC durations (30 [30–30] vs. 60 [30–60] min, p < 0.001) and lower HIPEC body temperatures (37.22 [37–37.8] vs. 37.73 [38–38.5] °C; p = 0.038). Conversely, this group showed greater HIPEC serum glucose concentrations (411.82 [355–459] vs. 329.06 [280–392] mg/dL; p = 0.019), HIPEC LL (6.19 [4.9–7.2] vs. 4.38 [3.9–4.7] mmol/L; p < 0.001), and ICU LL at 6 h (4.65 [3.25–4.73] vs. 3.35 [2.1–4.889] mmol/L; p = 0.008), 9 h (3.5 [2.23–5.03] vs. 2.4 [1.78–3.7] mmol/L; p = 0.010), and 12 h (3.1 [2.1–4.05] vs. 2.1 [1.5–3.15] mmol/L; p = 0.003). No differences were found in other parameters (p > 0.05) (Table 4).
Descriptive Statistics and Comparison Results for Hypoperfusion Variables on the Basis of Intensive Care Unit Admission Lactate Groups
Patients excluded without a gastrointestinal system anastomosis (n = 82).
Colostomy and Ileostomy patients included (n = 43).
14 total gastrectomy patients excluded (n = 96).
Only female patients included (n = 62).
*: p < 0.050, **: p < 0.010, ***: p < 0.001.
SSI = surgical site infection; SiSSI = superficial incisional surgical site infection; DiSSI = deep incisional surgical site infection; OsSSI = organ/space surgical site infection; PCI = Peritoneal Cancer Index; HIPEC = hyperthermic intraperitoneal chemotherapy; ICU = intensive care unit; CCS = complete cytoreduction score; pRBC = packed red blood cells; FFP = fresh frozen plasma; † = chi-square analysis; s = independent samples t-test; ‡ = Mann–Whitney U test; χ^2 = chi-square test statistic; Z = Mann–Whitney U test statistic. Descriptive statistics are presented as frequency (percentage) or median (25th–75th percentile).
Factors influencing SSI development, including LL, PCI, wound classification (which is known to be associated with SSI), age, history of diabetes mellitus or smoking, the presence of colon resection, anastomosis, and ASA scores, were included in the regression analysis. In the uni-variable analysis, LL of ≥6 mmol/L (OR: 3.33; p = 0.007), a PCI of ≥8 (OR: 2.315; p = 0.046), and Class II wounds (OR: 27.667; p = 0.002) were identified as significant risk factors for SSI development. When these significant parameters were subjected for multi-variable analysis, only parameters found to increase SSI risk were lactate ≥6 mmol/L (OR: 4.614; p = 0.005) and Class II wounds (OR: 27.677, p = 0.002) (Table 5).
The Findings of Uni-variable and Multi-variable Logistic Regression Analysis Obtained on the Impact of Surgical Site Infection
PCI = Peritoneal Cancer Index; ASA = American Society of Anesthesiology; OR = Odds Ratio; 95% CI = 95% confidence interval.
Discussion
This study investigated the relation between LL and SSI development after CRS + HIPEC. ICU admission LL, major complications, and prolonged hospital stay were found to influence SSI development. As SSI is linked to complications and extended hospital stays, LL have been shown to be a reliable predictor of SSI in PC patients post-operatively.
Aggressive procedures involving multi-organ resections, such as peritonectomy, pre-operative urinary tract stenting for pelvic involvement, and colon or gastric resection, heighten the risk of contamination. Additional factors increasing SSI risk include neutrophilia after HIPEC and splenectomy-induced immunosuppression. 3 Changes in LL are influenced by many factors beyond hypoperfusion, including shock, sepsis, severe hypoxia, anemia, drug use history, and chronic liver disease. 22 To assess these influences, replacement products, serum glucose, pulse values, operation durations, and drug regimens during operation were evaluated.
As changes in LL are multifactorial, their evaluation in critically ill patient populations remains debated. Several systematic reviews suggest its use in risk-stratification, but more homogeneous and lactate-focused studies are needed.23,24 Another study on elective debulking operation involving 51 patients showed that greater PCI and prolonged surgical duration increased LL. 25 In contrast, our study found no association between PCI or transfusion with LL.
A study on elective colorectal cancer cases assessed the impact of post-operative venous LL and 48-hour CRP concentrations on 30-day morbidity. LL significantly predicted OsSSI (p = 0.046, AUC: 0.707), although sensitivity decreased after logistic regression, indicating a twofold increase in OsSSI risk. Combining LL and CRP improved prognostic accuracy. The study linked elevated venous lactate to oxidative stress and prolonged hypotension during operation, increasing OsSSI risk, whereas technical issues such as anastomotic leakage explained the low predictive value of lactate. 26 Another study on pancreatectomies found greater lactate concentrations, base excess, and ICU stays in SSI cases, with LL >3.250 mmol/L yielding 90% sensitivity and 83.87% specificity (AUC: 0.895). Although our study showed lower sensitivity, specificity was comparable. 27
A similar pilot study included 68 oncology patients divided into three groups as follows: primary oncologic resection, CRS, and CRS + HIPEC. Analysis of surgical processes in quartiles showed that CRS increased LL at all periodic intervals, with an even greater increase, during HIPEC. Using baseline LL as a cutoff, major complications were more frequent in all patients and in the CRS + HIPEC group, although this was not statistically significant. 4 In contrast, our study found both complication development and SSI occurrence to be significant at a greater lactate cutoff value than the baseline concentration.
Hervás et al. demonstrated that patients with LL >2.5 mmol/L upon ICU admission after PC surgical procedure experienced more post-operative complications and longer ICU stays, with a substantial association for Grade II complications above this threshold. 7 Similarly, our study found a substantial association between LL ≥6 mmol/L at ICU admission and increased SSI, major complications, and prolonged hospitalization. The greater lactate cutoff in our study may be because of the absence of prophylactic HIPEC in our cohort, restrictive fluid management practices at our center, and differences in patient selection, as patients with CCR2 and above were excluded. Furthermore, our study included a larger cohort and utilized logistic regression analyses to evaluate the relation between SSI and other factors, offering a broader perspective for comparison.
Chichura et al. evaluated the effects of pre-operative factors on CRS + HIPEC outcomes in gynecologic origin PC. They observed increased complication rates, from prolonged intubation to bleeding, with lower pH concentrations. It was suggested that patients with high LL might maintain acid–base balance via compensation mechanisms, recommending the inclusion of hypoperfusion indicators such as pH in such studies. The study found that high LL combined with acidosis increased SSI risk. The frequency of SSI among patients with high post-operative LL in the ICU was comparable to our results; however, no relation was found between peri-operative LL and SSI development in our study. Although the inclusion of only gynecologic-origin patients in their study created a more homogeneous cohort, in contrast, our study minimized variations in LL by excluding patients with chronic kidney failure or CCR2. 28
Finally, Smibert et al. evaluated SSI factors in 43 CRS + HIPEC patients, reporting a median arterial lactate of 2.2, with no association between LL and SSI. In our study, median LL were greater, with 49 patients having a PCI >8 compared with their median PCI of 5. Their median surgical duration of three hours was also shorter than in our study, likely accounting for the greater values observed in our results. 29
The retrospective design of this study is a key limitation. Although the heterogeneity arising from PC etiologies was noted, our analysis indicated that diagnosis did not impact SSI development in this cohort. To reduce bias, numerous parameters were analyzed, and patients with potential confounding factors were excluded. The greater lactate cutoff in our study compared with others may be attributed to restrictive fluid management aimed at minimizing post-operative complications. Moreover, the majority of our study period took place before the publication of PRODIGE-7. The PRODIGE-7 trial demonstrated an increase in grade 3–4 complications in patients undergoing CRS/HIPEC, and subsequent studies have recommended the use of mitomycin C instead of oxaliplatin-based regimens, particularly in colorectal cancer cases. Although no substantial difference was observed in SSI development between patients receiving oxaliplatin-based regimens in our cohort, we found that LL were greater in these patients compared with those receiving cisplatin-based regimens. Had the use of mitomycin C been feasible during our study period, both the lactate cutoff values and the complication rates in the oxaliplatin group might have been lower. Prophylactic HIPEC cases were excluded to standardize surgical durations and disease severity, which resulted in a smaller patient volume. Although the low sensitivity of lactate (47%) may limit its stand-alone clinical utility, lactate measurement is readily accessible via routine post-operative arterial blood gas monitoring. This standard practice provides LL without additional costs, making its use as an SSI predictor feasible and practical.
Conclusion
This study demonstrates that post-operative SSI susceptibility in PC patients undergoing CRS + HIPEC can be effectively evaluated through LL monitoring. Arterial lactate concentrations at ICU admission may provide critical insights into hypoperfusion susceptibility and its role in SSI development, particularly in highly immunosuppressed and vulnerable populations. Routine lactate monitoring, already a standard part of post-operative ICU care, serves as a practical tool for early intervention. Future prospective studies with larger randomized cohorts are needed to validate these findings and explore the efficacy of intensified prophylactic measures, including even enhanced antifungal regimens. Such tactics may not only reduce SSI risk but also address related complications, such as post-HIPEC neutropenia, ultimately improving outcomes in this fragile patient population.
Footnotes
Authors’ Contributions
Conceptualization: İ.C.A., A.O.S., S.A., and E.P. Methodology: İ.C.A., A.O.S., S.A., and E.P. Investigation: İ.C.A., A.O.S., and S.A. Data Curation: İ.C.A., A.O.S., S.A., Ö.Ö., U.D., S.G., and M.D. Original draft preparation: İ.C.A., A.O.S., S.A., and E.P. Review and editing supervision: İ.C.A. and E.P.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and received ethical approval from the Koşuyolu Yüksek İhtisas Training and Research Hospital Research Ethics Committee (approval no. 2023/06/679) on August 09, 2022, with the need for written informed consent waived.
Data Availability Statement
The data supporting this study are available upon reasonable request from the authors, with permission from the University of Health Sciences Koşuyolu Yuksek Ihtisas Training and Research Hospital, in compliance with institutional guidelines.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.