
Abstract
Background:
Abdominal operation is common as are surgical site infections (SSIs). Triclosan (polychlorophenoxyphenol) is an antimicrobial antiseptic used in a variety of consumer products, including suture. The Surgical Infection Society’s Therapeutics and Guidelines Committee convened to perform a systematic review and develop pragmatic recommendations for use of triclosan-coated suture in prevention of SSI after an abdominal surgical procedure.
Methods:
A research librarian designed and performed searches of three bibliographic databases: PubMed, Embase, and Web of Science. Methodology for this practice management guideline conformed to Reporting Items for practice Guidelines in HealThcare Working Group standards. Covidence was used for study selection and quality and certainty of published evidence was evaluated using GRADE. The clinical question assessed was: “For adult patients undergoing abdominal surgery, does triclosan-coated suture vs. non-triclosan-coated suture reduce the risk of post-operative SSI?”
Results:
A total of 3,616 studies were identified, with 30 studies involving 97,807 patients informing the clinical question response. Among included studies, 13 (43%) were randomized controlled trials (RCTs) and 17 (57%) were meta-analyses. Seventeen (57%) studies comprising 67,445 (69%) patients demonstrated reduction in SSI, with 13 (43%) studies comprising 30,362 (31%) patients demonstrating no benefit. Estimated cumulative adjusted absolute risk reduction associated with triclosan-coated sutures, among studies demonstrating benefit, was 3.2% (standard deviation ±6.2%). Overall quality of evidence was high. We recommend triclosan-coated suture for incision closure after an abdominal operation to reduce risk of SSI (Grade 1A).
Conclusions:
Higher-level evidence suggests a small but significant benefit for triclosan-coated suture in reducing SSI risk following an abdominal surgical procedure.
An abdominal operation is common, with 2–4 million laparotomies and more than 3 million laparoscopies or thoracoscopies performed annually in the United States.1,2 Surgical site infections (SSIs) are similarly prevalent and costly, with more than 195,000 SSIs occurring annually in the United States alone, with an estimated cost of USD 5.5 billion. 3 Frequency of SSI after laparotomy is dependent upon underlying abdominal pathology, degree of contamination during the operation (by intestinal contents in particular), patient comorbidities, and the surgical setting.4,5 Tactics to mitigate SSI risk are numerous, including timing and choice of pre-operative antibiotic agents, skin preparation, management of hair removal, instrument and room management, and peri-operative temperature and glycemic control, among others.6,7
One therapy included occasionally in SSI prevention bundles is use of triclosan-coated suture material. Sutures are a foreign body that may serve as a nidus for bacterial colonization, predisposing to development of an SSI. Triclosan (polychlorophenoxyphenol) is an antimicrobial antiseptic used in a wide variety of consumer products, including soap, hand sanitizer, toothpaste, and mouthwash, with 10.5 million pounds of triclosan manufactured annually. 8 Triclosan is used to treat a range of suture material, including braided polyglactin 910, poliglecaprone 25, and polydioxanone. Use of triclosan-coated suture is hypothesized to reduce risk of biofilm formation and subsequent infection and may elute an antibacterial zone of inhibition into tissue fluid at the site of an incision. The Surgical Infection Society’s (SIS) Therapeutics and Guidelines Committee convened to perform a systematic review of current literature and develop pragmatic recommendations for use of triclosan-coated suture in prevention of SSI after an abdominal operation.
Level of Evidence: Level IV, therapeutic/care management
Objective
Clinical question
For adult patients undergoing an abdominal operation, does use of triclosan-coated suture versus non-triclosan-coated suture reduce the risk of post-operative SSI?
Methods
Methodology for this practice management guideline was based on the framework described by Arksey and O’Malley 9 and conforms to multi-disciplinary international Reporting Items for practice Guidelines in HealThcare (RIGHT) Working Group standards (Supplementary Data S1). 10 A guidelines team with experience in surgical infectious diseases, epidemiology, and systematic reviews for guidelines was established to determine the clinical question and study protocol. Review consisted of five phases: establishment of clinical question and outcomes, identification of relevant studies, study selection, data abstraction, and collation and summary of results.
On August 2, 2023, a research librarian designed and performed searches of three bibliographic databases: PubMed® (National Library of Medicine, National Institutes of Health, Bethesda, MD), Embase (Elsevier, Amsterdam, The Netherlands), and Web of Science (Clarivate Analytics, Philadelphia, PA) (Supplementary Data S2). This search was repeated on September 4, 2024, to capture recent articles not identified originally. Only English-language articles or articles that could be translated into English were reviewed. Studies published in the year 2003 or later were included to maximize capture of relevant studies. Inclusion criteria included randomized controlled trials (RCTs) or meta-analyses that evaluated use of triclosan-coated suture for an abdominal operation. Meta-analysis without subgroup analysis of an abdominal operation in isolation was not included. Systematic reviews, commentaries, operative technique descriptions, active clinical trials, and animal studies were excluded. Pediatric patients were defined as patients <18 years of age. Studies with a majority (≥50%) of pediatric patients in their study population were excluded. Wound contamination was defined by the existing Centers for Disease Control and Prevention definitions. 6 Income status by country (locales conducting the studies) was defined according to the World Bank (2024–2025). Unless otherwise stated by authors, studies assessing colorectal procedures were assumed to include clean-contaminated and contaminated cases. Conflicts of interest (COI) and funding sources were identified for each study.
Database results were uploaded into Covidence (Melbourne, Australia), a Cochrane-sanctioned, web-based application. Upon completion of the electronic literature search, titles and abstracts from citation lists were reviewed by two of five committee members to identify potentially relevant studies. Any disagreement about study inclusion was resolved by consensus with a third reviewer. Full-text review and data abstraction were performed by five committee members.
Quality and certainty of published evidence were evaluated using Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) definitions using high (A), moderate (B), or weak (C) nomenclature.11,12 Strength of the recommendation was graded as strong (1) or weak (2).13,14 Missing data were sought from corresponding authors. Degree of bias and certainty were reported after group consensus. Absolute risk reduction for studies showing statistical benefit was reported. Estimated cumulative adjusted absolute risk reduction was calculated using studies showing benefit of triclosan-coated suture. Study quality was not included in the cumulative adjusted absolute risk reduction estimate. When calculating cumulative adjusted risk reduction, only subgroups where benefit was demonstrated were included. Microsoft Excel 2019 (Redmond, WA) was used for statistical analysis.
Using iterative consensus, all committee members voted to accept or reject the recommendation. If abdominal operation analysis was performed as a subgroup analysis for either an RCT or meta-analyses, this was considered to decrease study quality. The intended primary guideline users include surgeons, operating room leadership, infection preventionists, and hospital administrators. The guideline is intended for both outpatient and inpatient settings. This study was exempt by the institutional review board as all articles are publicly available.
Results
Qualitative synthesis
In total, 3,616 studies were identified, with 30 studies involving 97,807 patients used to inform responses to the clinical question (Fig. 1). Included studies were published between 2009 and 2024 (Table 1). Among the 30 included studies, 13 (43%) were RCTs and 17 (57%) were meta-analyses. Seven (54%) RCTs were single-center. Eighteen studies were multi-national with 12 involving healthcare center(s) in a single country with ten countries represented (Japan [two studies], Spain [two studies], Croatia, Egypt, Germany, Hungary, Italy, Korea, Thailand, and Turkey). Among the RCTs, six were multi-institutional and seven were single institution. The abdominal operation was evaluated as a subgroup analysis in seven studies. Most (n = 26, 87%) studies did not report COI or and only one study reported industry funding. No studies included had more than 50% pediatric patients.
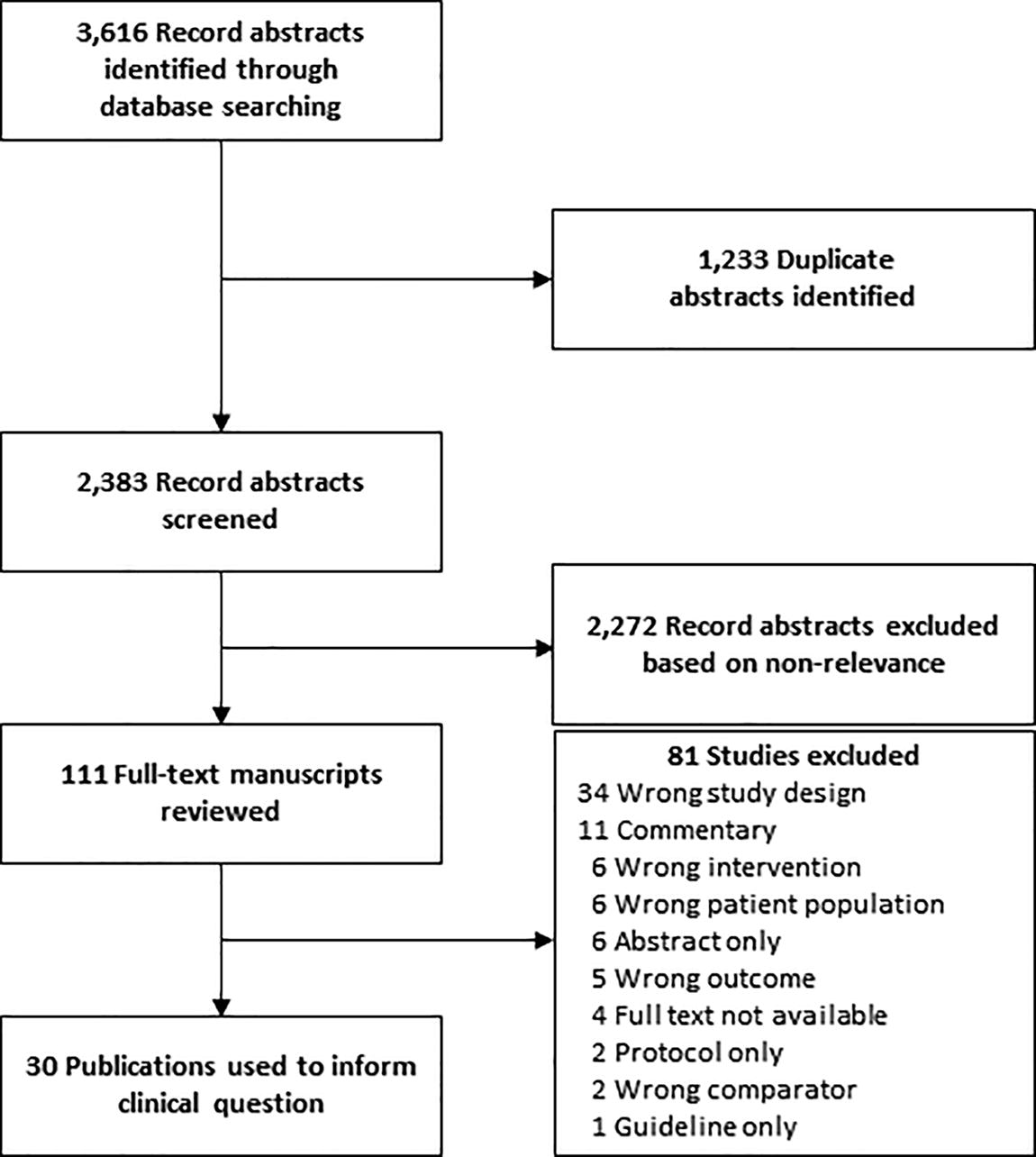
Flow diagram showing selection process for included articles.
Articles Identified Through Search, Reviewed for Clinical Question
Altemeier/US Centers for Disease Control and Prevention Classification System. Class I (I) (clean): Uninfected incision in which no inflammation is encountered. Alimentary, genitourinary, or respiratory tracts not entered. Clean incisions are closed primarily and if necessary, drained with a closed system. Incisions made to manage blunt trauma are included if criteria are met. Class II (II) (clean-contaminated): Incisions where the alimentary, genitourinary, or respiratory tracts are entered under controlled conditions and without overt contamination. Operations involving the appendix, biliary tract, and vagina are included absent evidence of infection or a major break in technique. Class III (III) (contaminated): Open, fresh traumatic wounds. Operative incisions with a major break in sterile technique (e.g., open cardiac massage) or overt “spillage” from the alimentary tract. Incisions in which acute, non-purulent inflammation is encountered. Class IV (IV) (dirty-infected): Old traumatic wounds with retained, devitalized tissue. Incisions made to control active purulent infection, with bacterial pathogens present in the field before incision (e.g., perforated viscus).
RR = relative risk; RCT = randomized controlled trial; COI = conflict of interest; T = triclosan; N/A = not applicable; PDS = polydioxanone suture; NR = not reported; CRS = colorectal surgical procedure; CI = confidence interval; OR = odds ratio; SSI = surgical site infection.
Seventeen (57%) studies comprising 67,445 (69%) patients demonstrated reduction in SSI with 13 (43%) studies comprising 30,362 (31%) patients demonstrating no benefit. Of the studies showing benefit, 12 (71%) were meta-analysis and five (29%) were RCTs, compared with seven (54%) meta-analyses and six (46%) RCTs demonstrating no benefit. Of the RCTs showing benefit, one (20%) was performed in an low- and middle-income country (LMIC). By contrast, of the six RCTs showing no benefit, three (50%) were performed in LMICs. Among the 14 studies with adequate information available to enable combinatorial analysis, the estimated cumulative adjusted absolute risk reduction associated with triclosan-coated sutures was 3.2% (standard deviation [SD] ± 6.2%) (Fig. 2). Each study is described individually below, with studies showing benefit described first, followed by studies showing no benefit, in chronologic order.

Cumulative adjusted risk reduction for studies showing benefit of triclosan-coated suture. Light gray = studies showing benefit of triclosan-coated suture. Dark gray = studies showing no benefit of triclosan-coated suture.
Studies supporting triclosan-coated suture
In 2011, Rasic et al. published a single-center, RCT in Croatia examining the use of triclosan-coated polyglactin 910 versus non-coated polyglactin for abdominal wall (peritoneum, muscle, fascia) closure among patients undergoing an elective colorectal surgical procedure for colorectal cancer. 17 Skin closure was performed with polyamide. Among 184 patients included in the study, the authors noted a 9% absolute risk reduction. 17 Only uni-variable analysis was performed (p = 0.035.) 17 Risk of bias accrued owing to the absence of multi-variable comparison for the primary outcome. This was followed by Nakamura et al. in 2013, who published a single-center RCT in Japan comparing triclosan-coated polyglactin 910 versus non-coated polyglactin for abdominal wall closure. 18 Among 410 patients, a 5% absolute risk reduction was identified (p = 0.047.) 18 Risk of bias included lack of data on skin closure technique and absence of multi-variable comparison for the primary outcome. Also in 2013, Wang et al. performed a meta-analysis comparing triclosan-coated suture with non-triclosan-coated suture across a range of surgical procedures. 19 In the abdominal surgical procedure subgroup that comprised 1,562 patients, a 2% absolute risk reduction was identified (relative risk 0.69 [0.50–0.97], p = 0.030, P for Q test 0.169, I2 34%.). 19 Risk of bias included dependence upon subgroup analysis.
In 2015, Apisarnthanarak et al. published a meta-analysis comparing triclosan-coated sutures with non-triclosan-coated sutures across a range of surgical procedures. 22 In the abdominal surgical procedure subgroup that comprised 6,315 patients, a 5% absolute risk reduction was identified (fixed-effects model relative risk 0.59 [0.50–0.69], random-effects relative risk [0.56 (0.41–0.77]). 22 Within the colorectal operation subgroup of 1,364 patients, no risk reduction was identified (fixed-effects model relative risk 0.77 [0.56–1.06], random-effects model relative risk 0.73 [0.46–1.17]). 22 When calculating cumulative adjusted risk reduction, only the abdominal operation subgroup was included. Other risk of bias included dependence upon subgroup analyses and COI reported by authors.
Also in 2015, Ruiz-Tovar et al. reported a multi-center RCT in Spain comparing triclosan-coated sutures versus non-triclosan-coated sutures in patients undergoing abdominal fascial closure after a dirty or infected operation. 24 Among the 101 patients enrolled, an absolute risk reduction of 25% was identified (odds ratio [OR] = 0.204; 95% confidence interval [CI] 0.069–0.605, p = 0.004). 24 Risk of bias included the randomization process. This was followed in 2016 by Guo et al. who performed a meta-analysis of triclosan-coated sutures versus non-triclosan-coated sutures for patients undergoing a range of surgical procedures. 25 On subgroup analysis of 3,020 patients undergoing abdominal operation, a 3% absolute risk reduction was identified (risk ratio 0.70 [95% CI 0.50–0.99], p = 0.04). 25 Risk of bias included subgroup analysis and absence of specification of skin closure technique.
In 2017, Henriksen et al. published a meta-analysis evaluating use of triclosan-coated suture to non-triclosan-coated suture in patients undergoing a range of abdominal procedures. 28 Among 3,502 patients, an absolute risk reduction of 4% (OR 0.67, 95% CI 0.46–0.98, p = 0.04) was identified. 28 Risk of bias was low. Similarly in 2017, Konstantelias et al. published a meta-analysis comparing triclosan-coated suture with non-triclosan-coated suture for patients undergoing a broad selection of surgical procedures. 29 By subgroup analysis of 2,410 patients undergoing colorectal surgical procedures, a risk ratio of 0.58 (95% CI 0.37–0.91) was identified suggesting benefit, although absolute risk reduction was not reported. 29 Risk of bias included failure to report complete outcomes data and dependence upon subgroup analysis for colorectal operation cases. In 2018, Uchino et al. performed a meta-analysis for patients undergoing digestive tract operation, comparing patients receiving wound closure with triclosan-coated suture with those without. 31 Among the 3,488 patients included, a 3% absolute risk reduction was identified (risk ratio 0.67, 95% CI 0.48–0.94, p = 0.02). 31 Risk of bias was low.
In 2019, Olmez et al. published a single-center RCT from Turkey comparing triclosan-coated polydioxanone suture (PDS) with non-triclosan-coated PDS for fascial closure in patients undergoing elective or emergency laparotomies. 33 Among 890 patients a 7% absolute risk reduction (p = 0.0.16) was identified and no multi-variable comparison was performed. 33 Risk of bias included absence of multi-variable analysis and paucity of randomization technique information. In 2020, Ruiz-Tovar et al. performed a second multi-center RCT comparing triclosan-coated, barbed suture with triclosan-coated looped PDS versus non-coated looped PDS in patients undergoing emergency abdominal operations with contaminated, dirty, or infected wounds. 35 Among the 150 patients randomized, a 15% absolute risk reduction was identified on patients undergoing closure with any triclosan-coated suture, whether barbed or looped (p = 0.009 on pairwise analysis). 35 Risk of bias included low patient accrual in each study arm.
In 2023, Miyoshi et al. performed a meta-analysis comparing triclosan-coated suture with non-triclosan-coated suture, evaluating studies where any abdominal operation was performed with fascial closure. 38 Among the 9,588 patients identified, a 1% absolute risk reduction was identified (OR 0.7; 95% CI 0.68–0.88). 38 Risk of bias was low. Also in 2023, Otto-Lambertz et al. performed a meta-analysis of a range of surgical procedures comparing triclosan-coated suture with non-triclosan-coated suture. 39 In the abdominal surgical procedure subgroup analysis, a risk ratio of 0.75 (95% CI 0.61–0.91, p = 0.009) was identified although no absolute risk reduction was reported. 39 Risks of bias included absence of outcome data for subgroup analysis and dependence upon subgroup analysis.
In 2024, Depuydt et al. published a meta-analysis comparing triclosan-coated suture with non-triclosan-coated suture among studies where any abdominal fascial closure was performed. 40 Among the 10,234 patients included, an absolute risk reduction of 3% was seen (OR 0.84, 95%CI 0.75–0.93, p = 0.001.) 40 Conflicts of interest were identified as a risk of bias. Also in 2024, Erfan et al. published a single-center RCT in Egypt comparing patients undergoing port-site closure after laparoscopic cholecystectomy, laparoscopic sleeve gastrectomy, or laparoscopic appendectomy evaluating outcomes of triclosan-coated polyglactin 910 versus non-coated polyglactin 910. 41 Among 480 randomized patients, absolute risk reductions of 6% (p < 0.001) and 4% (p = 0.015) were seen in patients undergoing laparoscopic cholecystectomy and laparoscopic appendectomy, respectively. 41 Risk of bias included failure to include ORs in outcome reporting and inability to delineate port-site-specific risk reduction. Kouzu et al., in 2024, published a meta-analysis comparing triclosan-coated suture with non-triclosan-coated suture for patients undergoing fascial closure after abdominal operation. 42 Among 4,309 patients, an absolute risk reduction of 4% was identified (relative risk 0.79, 95% CI 0.64–0.98). 42 Risk of bias was low. Finally, in 2024, Suleiman et al. published a second-order meta-analysis comparing triclosan-coated suture with non-triclosan-coated suture across a range of surgical procedures. 43 Abdominal operation and colorectal operation subgroup analyses were performed. Among the 11,270 patients included in the abdominal operation subgroup, an absolute risk reduction of 3% (relative risk 0.64, 95% CI 0.51–0.82) was seen. 43 No benefit was observed for the colorectal operation subgroup. 43 Risk of bias included reliance upon subgroup analysis.
Studies not supporting triclosan-coated suture
In 2009, Mingmalairak et al. performed a single-center RCT comparing triclosan-coated polyglactin 910 with non-triclosan-coated polyglactin 910 suture in patients aged 15–60 years undergoing open appendectomy. 15 No difference in SSI rate was identified by uni-variable analysis (p = 0.7). 15 This study was started as a pilot and failed to enroll sufficient patients to meet the pre-determined power calculation. Risk of bias was identified in deviations from the intended intervention as most operations were performed by second-year residents as opposed to attending surgeons, and out-of-hospital outcomes were not reported. In 2011, Baracs et al. performed a multi-center RCT in Hungary comparing triclosan-coated running looped PDS with non-coated running looped PDS for fascial closure in elective benign or malignant colon or rectal operations. 16 Among 385 patients, rates of infection were comparable between groups (p > 0.05). 16 However, among a small subgroup of 85 rectal operations, an absolute risk difference of 8% was identified (p = 0.033). 16 Risk of bias was low.
In 2014, Daoud et al. performed a meta-analysis comparing triclosan-coated sutures versus non-triclosan-coated sutures for a range of surgical procedures. 20 Upon subgroup analysis of patients undergoing appendectomy or colorectal operation, the pooled relative risk was 0.698 (95% CI 0.476–1.002, p = 0.0536). 20 Risk of bias included dependency on subgroup analysis. Also in 2014, Diener et al. published a multi-center RCT in Germany comparing triclosan-coated PDS with non-triclosan-coated PDS for adult patients requiring closure of a midline laparotomy. 21 Among 1,185 patients an OR of 0.91 (95% CI 0.66–1.25) was observed. 21 Risk of bias included industry funding and COIs listed for authors for the same industry partner. In 2015, Mattavelli et al. published a multi-center RCT from Italy comparing triclosan-coated polyglactin 910 suture with non-triclosan-coated polyglactin 910 among patients undergoing colorectal operation in a clean-contaminated field. 23 Among 281 patients an OR of 1.24 (95% CI 0.60–2.57) was observed showing an increase in infections in the triclosan-coated suture group. 23 Risk of bias was identified owing to deviations from the intended intervention, as any patient who developed a leak or required a reoperation was dropped from the study. In 2016, Sandini et al published a meta-analysis evaluating patients undergoing an elective colorectal surgical procedure, comparing triclosan-coated sutures with non-triclosan-coated sutures. 26 Among the 2,168 patients included, no difference was noted, with an OR of 0.81 (95% CI 0.58–1.13.) 26 Risk of bias was low. In 2017, Elsolh et al. performed a meta-analysis of 3,117 patients undergoing an abdominal operation, comparing triclosan-coated sutures with non-triclosan-coated sutures. 27 The OR was 0.79 (95% CI 0.57–1.09) and risk of bias was low. 27 This was followed in 2018 by Ichida et al. who published a single-center, RCT comparing triclosan-coated polyglactin 910 with non-triclosan-coated polyglactin 910 in 1,013 patients undergoing a gastrointestinal operation requiring abdominal fascial closure. 30 Only a uni-variable analysis was performed, with no difference noted between suture types (p = 0.61). 30 Risk of bias was low but a large range of gastrointestinal procedures were enrolled.
In 2019, Hunger et al. published a meta-analysis comparing triclosan-coated sutures with000 non-triclosan sutures for patients requiring abdominal closure after a colorectal operation. 32 Among 2,957 patients, an OR of 0.62 (95% CI 0.29–1.31) was identified. 32 Risk of bias was identified owing to 50% of included studies not containing RCTs and COI with industry reported by the authors. 32 Also in 2019, Zucker et al published a meta-analysis comparing 10 suture types (with subgroup analysis of each suture type compared with each other.) 34 Whereas triclosan-coated sutures were not compared with as a group against non-triclosan-coated sutures, neither triclosan-coated polyglactin 910 nor triclosan-coated PDS was found to be superior against any other suture type. 34 Risk of bias was identified owing to the number of subgroup analyses.
In 2021, Ademuyiwa et al. published a multi-center multi-national RCT in LMICs comparing triclosan-coated suture with non-triclosan-coated suture among 3,051 patients undergoing abdominal surgical procedures with incisions ≥5 cm requiring closure. 5 There was no difference between suture types in either the clean-contaminated stratum nor the dirty stratum. 5 Risk of bias was present owing to subgroup analysis. In 2022, a global surgery research consortium followed this multi-center RCT with a meta-analysis comparing triclosan-coated suture with non-triclosan-coated suture in 8,619 patients undergoing abdominal operation. 36 There was no difference between suture types (OR 0.90, 95% CI [0.74–1.09]). 36 Risk of bias was present owing to subgroup analyses. Finally, Kang et al. in 2023 published a single-center RCT comparing triclosan-coated polyglactin 910 with non-triclosan-coated polyglactin 910 in patients undergoing open or laparoscopic colorectal procedures. 37 No difference was noted (p = 0.98). 37 Risk of bias was noted as the colorectal procedures were misclassified as clean.
Recommendation
A systematic review of current literature has addressed the risk of SSI after an abdominal operation utilizing triclosan-coated suture. Overall quality of the body of evidence was rated as high. Some concerns over risk of bias were identified for 22 studies, although this was due most commonly to the presence of subgroup analyses informing study interpretation.
We recommend triclosan-coated suture for incision closure after an abdominal operation to reduce risk of SSI (Grade 1A).
Discussion
Using this guideline in clinical practice
Comparing recent studies evaluating use of triclosan-coated suture for abdominal wall closure, we observed a 3.2% absolute risk reduction in SSI. Applied to approximately seven million abdominal operations performed annually in the United States alone, a risk reduction of this magnitude may prevent up to 224,000 SSIs.1,2
No harm from triclosan-coated suture was identified although no studies addressed antimicrobial agent susceptibility to triclosan. Considering this favorable risk–benefit profile, there is little downside to incorporating triclosan-coated sutures in settings with robust SSI prevention bundles, other than the incremental acquisition costs. On the basis of data from the UK National Health Service, the average cost of an SSI was USD 3,767–6,289 with a cost of USD 13 per suture used. 39 Similarly, Singh et al showed that triclosan-coated sutures saved USD 4,109–13,975 (hospital perspective), USD 4,133–14,297 (third-party payer perspective), and USD 40,127–53,244 (societal perspective) in surgical procedures with a 15% risk of SSI. 44 However, the authors noted that when SSI risk is no more than 5% and efficacy in preventing SSIs is <10% (an absolute risk reduction of 3.2% was found across studies in this guideline), the extra expenditure for hospitals and third-party payers ranged from USD 1,626 to 1,071 for each preventable SSI. 44
Existing cost–benefit analyses are largely built within higher income settings. As such, this clear cost advantage may not be reproducible in all contexts, particularly in resource-constrained environments.5,36 In these settings, cost–benefit ratios may not favor non-triclosan-coated suture. One possible explanation is that the “full benefit” (i.e., no SSI) of triclosan-coated suture may require concurrent implementation of a bundle of other interventions that synergistically act to reduce SSIs such as the presence of sterile processing, skin preparation, and maintenance of patient homeostasis (e.g., normothermia, euglycemia) among others.4,6,7,45 When core components of infection prevention bundles are not present or are present in a variable manner, the effect of triclosan-coated sutures in reducing the risk of SSI may be less evident.
Limitations
There are several limitations to this clinical guideline. First, given the range of interventions and outcomes, combinatorial analysis of all studies was not possible. For example, abdominal operations were inconsistently defined across all studies. Some studies included operations on the small and large intestine, whereas others excluded these operative conditions. Second, the type of triclosan-coated suture used was not uniform. Third, publication bias was presumed. Fourth, cost and resource analyses were not ubiquitously included in all studies across all practice settings. This limited our ability to perform a cost–benefit analysis. Fifth, subgroup analysis describing degree of contamination was not performed by all studies limiting direct comparisons across all studies. Sixth, standard pre- and peri-operative management was not defined across all studies (e.g., antimicrobial prophylaxis). Seventh, our cumulative adjusted absolute risk reduction calculation did not take study quality into consideration. Notably, the two studies by Ruiz-Tovar et al. that evaluated only dirty or contaminated cases may have had an outsized impact on the final estimate of benefit. In addition, given that many meta-analyses included patients from the same foundational RCTs, there is potential for additive bias. Eighth, the CI for the estimated cumulative adjusted absolute risk reduction was 6.2%, nearly double the estimated risk reduction effect. This underscores the importance of applying these guidelines to local contexts and to cost–benefit analyses, as the magnitude of the effect may not be realized in all settings. Finally, not all studies evaluated only abdominal operations, and frequently abdominal operations were only identified independently on subgroup analysis, limiting the power to assess infection risk in this patient population in several articles.
Conclusions
Current evidence suggests a small, but significant benefit to the use of triclosan-coated suture to prevent SSI following an abdominal operation. There was no clinical harm identified as a result of triclosan-coated suture use. However, this favorable benefit may not be achievable in all practice settings. For surgeons, infection preventionists, and healthcare systems, use of triclosan-coated suture may depend on a local cost–benefit analysis. Ultimately, the decision to use triclosan-coated suture to prevent SSI should be made in the context of suture cost, the cost of an SSI, anticipated infection rates for a procedure, and local availability.
Footnotes
Authors’ Contributions
A.S.—Study design, literature search, data collection, and critical review. N.P.—Literature search, data collection, and critical review. N.F.—Literature search, data collection, and critical review. J.H.—Study design, literature search, data collection, data analysis, data interpretation, and critical review. J.D.F.—Study design, literature search, data collection, data analysis, data interpretation, writing, and critical revision. P.B.—Data analysis and critical revision.
Funding Information
No funding was received for this work.
Author Disclosure Statement
No conflicts of interest were reported for any author for this work product. Other disclosures: J.D.F.—unrestricted research funding from Varian and Pacira for an investigator-initiated trial, funding from Eclipse Regenysis for industry-sponsored clinical trial, consultant—Costa Surgical, Inc.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.