
Abstract
Background:
This study sought to determine key risk factors for post-operative pulmonary infections (PPIs) in traumatic intra-cranial hematoma (TICH) patients and to develop a nomogram for evaluating infection risk.
Methods:
A retrospective analysis was performed on TICH patients at a single-center hospital between October 2014 and September 2023. Key risk factors for PPI were identified using multi-variable logistic regression analysis, which were subsequently incorporated into a nomogram. Internal validation of the model was performed to assess its reliability and accuracy.
Results:
This study included 252 TICH patients, identifying significant risk factors for PPI such as age ≥60 years (odds ratio [OR]: 3.45, 95% confidence interval [CI]: 1.89–6.78, p < 0.001), smoking history (OR: 2.95, 95% CI: 1.56–5.24, p < 0.001), Glasgow Coma Scale [GCS] score <8 (OR: 4.10, 95% CI: 2.22–8.35, p < 0.001), mechanical ventilation for more than 3 days (OR: 6.25, 95% CI: 3.35–11.75, p < 0.001), and chest injury (OR: 4.75, 95% CI: 2.49–9.16, p < 0.001). A predictive nomogram based on these factors demonstrated good discriminative power upon internal validation.
Conclusion:
Age, smoking history, GCS score, duration of mechanical ventilation, and chest injury are independent risk factors for PPI in TICH patients. The developed nomogram is a valuable tool for clinicians in predicting infection risk and guiding post-operative management.
Introduction
Traumatic intra-cranial hematoma (TICH) is a serious complication of traumatic brain injury (TBI), one of the leading causes of disability and mortality worldwide. 1 TBI accounts for a substantial portion of injury-related deaths and long-term disabilities, with intra-cranial hemorrhage often representing the most life-threatening aspect of the condition. 2 TICH can present as epidural hematoma (EDH), subdural hematoma (SDH), or intra-parenchymal hematoma, each carrying varying degrees of risk depending on the size and location of the hemorrhage. 3 In patients undergoing surgical intervention for TICH, post-operative complications such as pulmonary infections are frequent and can exacerbate outcomes. Pulmonary infections in TICH patients are associated with prolonged hospital stays, increased healthcare costs, greater rates of intensive care unit admission, and elevated mortality rates. 4
Post-operative pulmonary infections, particularly pneumonia, are a substantial concern in patients who need extended mechanical ventilation, chest trauma, or exhibit impaired consciousness following severe TBI. In fact, studies have shown that infection rates in mechanically ventilated TBI patients can be as high as 40%, with ventilator-associated pneumonia (VAP) being the most common complication. 5 These infections not only complicate the recovery process but also lead to a greater likelihood of adverse outcomes such as sepsis, multi-organ failure, and prolonged rehabilitation. 6 Several clinical studies have consistently identified factors such as advanced age, low Glasgow Coma Scale (GCS) scores, the need for mechanical ventilation, and the presence of chest injuries as substantial contributors to the risk of pulmonary infection in these patients.7–9
Although previous studies have highlighted individual risk factors associated with PPI in TBI or TICH patients, there remains a need for a comprehensive predictive model that incorporates multiple parameters to provide a more accurate risk assessment.10,11 A nomogram—a statistical tool that integrates various risk factors into a user-friendly predictive model—has proved to be effective in other clinical settings for individual patient risk stratification. However, a nomogram specifically designed to predict PPI in TICH patients has not been developed.
The objective of this study was to identify the key clinical factors associated with the development of PPI in TICH patients and to develop a nomogram that can predict infection risk using readily available clinical data. This predictive model is intended to assist clinicians in identifying high-risk patients early, allowing for the execution of specialized interventions designed to lower the incidence of pulmonary infections and optimize clinical results in this susceptible population.
Patients and Methods
Study design and participants
This was a retrospective single-center study conducted at the People’s Hospital of Wuyuan County from October 2014 to September 2023. The hospital serves a population of approximately 370,000. Patients with a diagnosis of TICH confirmed by head computed tomography (CT) scans and who underwent operation were included. Inclusion criteria were as follows: (1) age ≥18 years, (2) confirmed TICH based on head CT scans, (3) complete clinical data, and (4) post-operation hospitalization. Patients with incomplete data, systemic diseases, or concurrent infections unrelated to TICH were excluded.
Data collection
Clinical data for each patient were collected from medical records, including gender, age, body mass index (BMI), hypertension, diabetes mellitus, GCS score, smoking history, systolic blood pressure, diastolic blood pressure, serum albumin concentrations, mechanical ventilation duration, chest injury, hematoma volume, cerebrospinal fluid leak, and occurrence of PPI. The hematoma location was classified into four types as follows: EDH, SDH, intra-cerebral hematoma, and others.
Definitions and grouping
Participants were classified into two distinct groups as follows: those in whom PPIs developed and those who did not experience any infections. Pulmonary infection was diagnosed based on clinical signs (fever, purulent sputum), chest imaging, and microbiologic findings. 12 BMI was calculated as weight (kg)/height (m2), and serum albumin concentrations <35 g/L were categorized as hypoalbuminemia.13,14 Patients requiring mechanical ventilation for more than three days were identified as at greater risk of infection.
Statistical analyses
Statistical analyses were conducted with R software (version 4.1.2, R Foundation for Statistical Computing). Categorical parameters were presented as counts and percentages, whereas continuous parameters were shown as mean ± standard deviation. Uni-variable analyses applied chi-square tests for categoric data and t-tests for continuous data. Parameters with p-values <0.05 were included in a multi-variable logistic regression model to find independent risk factors for PPI. Odds ratios (ORs) and 95% confidence intervals (CIs) quantified the associations. A predictive nomogram was created using the “rms” package based on these risk factors. The model’s predictive accuracy was assessed through the area under the receiver operating characteristic curve (AUC) and the concordance index (C-index). Internal validation was done with 1,000 bootstrap resamples, and calibration was evaluated using calibration curves.
Ethical considerations
The Institutional Review Board of The People’s Hospital of Wuyuan County approved the study. Written informed consent was waived owing to the study’s retrospective nature.
Results
Patient characteristics
In this retrospective study, data were collected from 252 patients who underwent surgical intervention for TICH between October 2014 and September 2023. The final analysis included 70 patients with PPIs and 182 patients without infections (Table 1). No significant difference was found between the lung infection and no-infection groups regarding gender distribution (p = 0.707), BMI (p = 0.260), hypertension (p = 0.658), or diabetes mellitus prevalence (p = 0.275). However, age ≥60 years, smoking history, GCS score <8, serum albumin <35 g/L, mechanical ventilation duration >3 days, chest injury, and cerebrospinal fluid leak were significantly associated with lung infection risk. Notably, patients with lung infections had a greater prevalence of age ≥60 years (74.3% vs. 29.6%, p < 0.001), smoking history (54.3% vs. 28.6%, p < 0.001), GCS score <8 (57.1% vs. 23.1%, p < 0.001), and mechanical ventilation >3 days (71.4% vs. 17.6%, p < 0.001). Cerebrospinal fluid leaks were also more common in the lung infection group (p = 0.024), whereas no significant difference was found in hematoma volume (p = 0.122), traumatic coagulation abnormalities (p = 0.396), gastrointestinal bleeding (p = 0.925), or deep vein thrombosis (0.534).
Patients’ Characteristics

PPI = post-operative pulmonary infection; BMI = body mass index; GCS = Glasgow Coma Scale; SBP = systolic blood pressure; DBP = diastolic blood pressure; EDH = epidural hematoma; SDH = subdural hematoma; ICH = intra-cerebral hematoma; TCA = traumatic coagulopathy.
Multi-variable logistic regression analysis
Multi-variable analysis identified age ≥60 years (OR: 3.45, 95% CI: 1.89–6.78, p < 0.001), smoking history (OR: 2.95, 95% CI: 1.56–5.24, p < 0.001), GCS score <8 (OR: 4.10, 95% CI: 2.22–8.35, p < 0.001), mechanical ventilation >3 days (OR: 6.25, 95% CI: 3.35–11.75, p < 0.001), and chest injury (OR: 4.75, 95% CI: 2.49–9.16, p < 0.001) as independent risk factors for PPI (Table 2).
Multi-Variable Logistic Regression Analysis for Predicting Risk of Post-Operative Pulmonary Infection
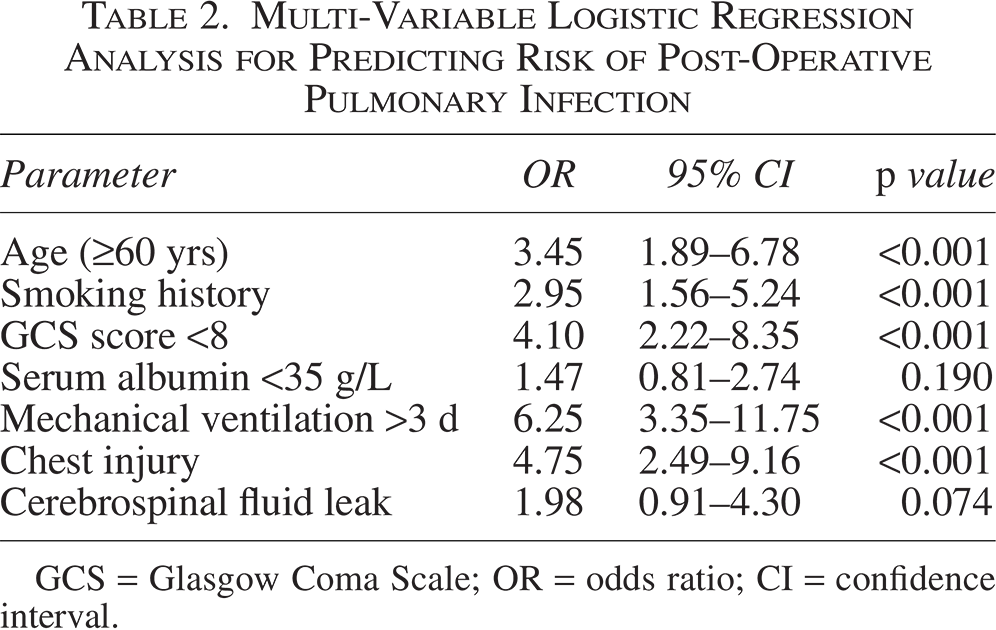
GCS = Glasgow Coma Scale; OR = odds ratio; CI = confidence interval.
Establishment of the nomogram model
On the basis of the independent risk factors found in the multi-variable logistic regression analysis, a nomogram was developed (Fig. 1). These included age, smoking history, pre-operative GCS score, mechanical ventilation duration exceeding three days, and the presence of chest injury. Each factor was assigned a corresponding number of points, as shown in Table 3. For example, a patient aged 65 years, with a smoking history, a pre-operative GCS score of 7, requiring mechanical ventilation for more than 3 days, and with chest injury would accumulate a total of 291 points. On the basis of the nomogram, this score correlates with a greater probability of developing a PPI.
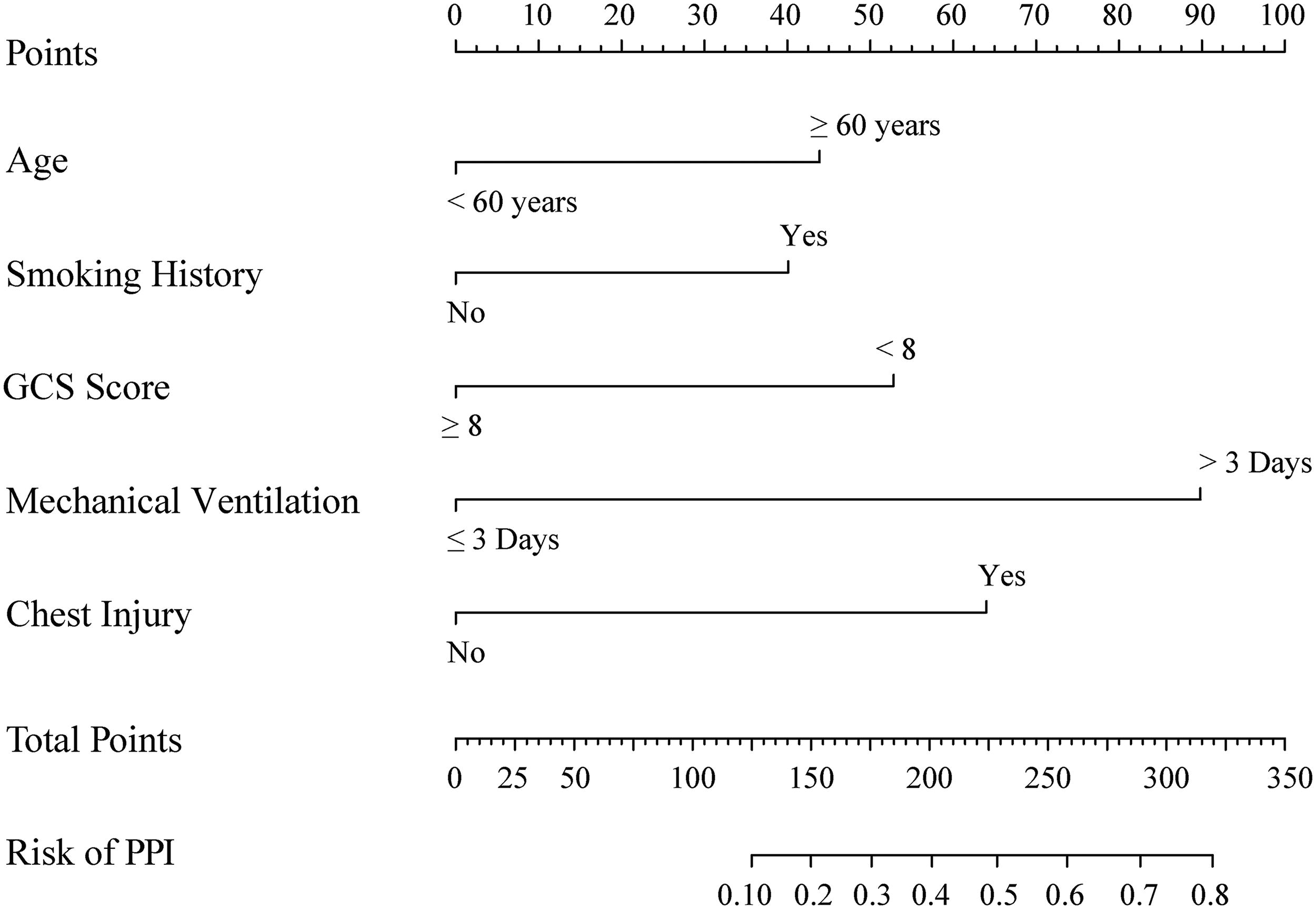
Nomogram predicting the probability of post-operative pulmonary infection in patients with TICH based on age, smoking history, pre-operative GCS score, duration of mechanical ventilation, and chest injury. TICH = traumatic intra-cranial hematoma; GCS = Glasgow Coma Scale.
A Scoring System for Predicting Post-Operative Pulmonary Infection Risk in Traumatic Intra-Cranial Hematoma Patients
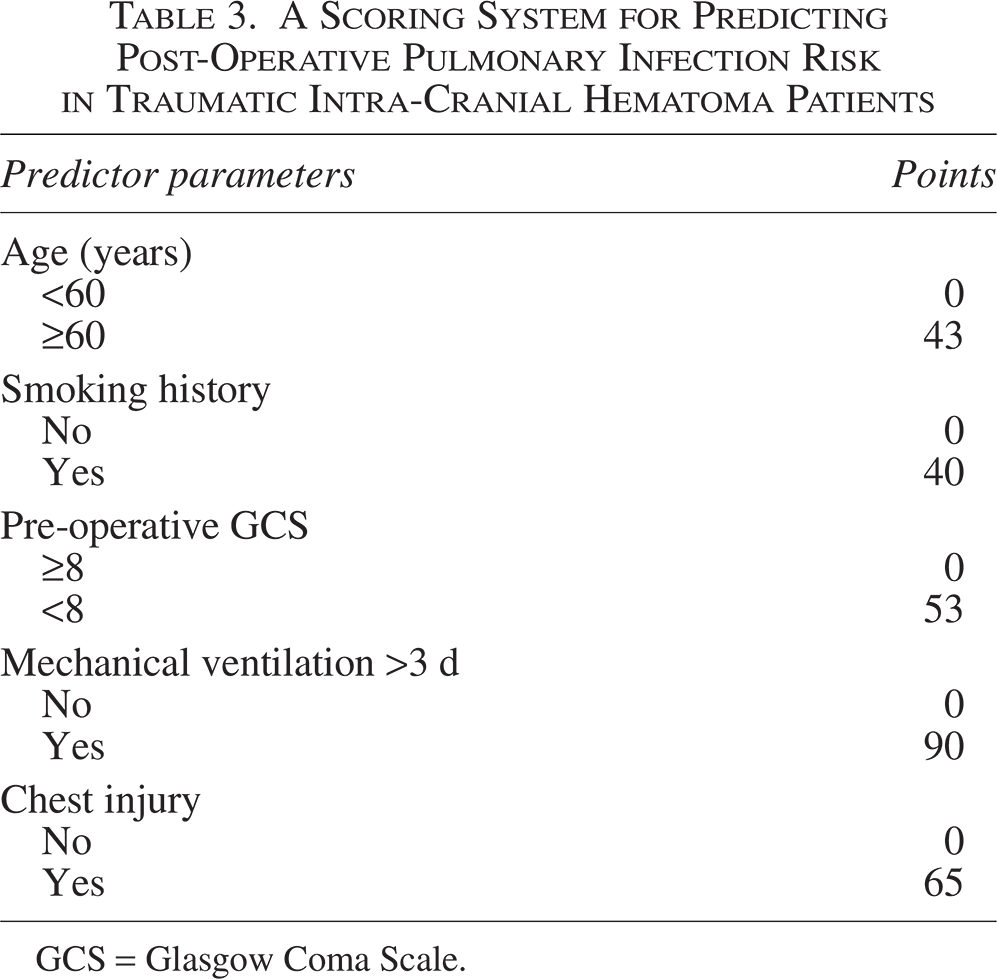
GCS = Glasgow Coma Scale.
Validation of the nomogram model
The nomogram’s performance was evaluated through internal validation using 1,000 bootstrap resamples. The model’s discriminative ability was evaluated using the C-index and the AUC. The calibrated C-index was 0.801, demonstrating strong predictive accuracy. The AUC was 0.801 (95% CI: 0.681–0.919) (Fig. 2A), showing that the model has a strong ability to identify patients in whom PPIs are likely to develop versus those in whom it will not.

In addition, a calibration curve was generated to assess the model’s accuracy in predicting PPI (Fig. 2B). The calibration curve showed minimal deviation from the ideal 45-degree line, confirming that the predicted probabilities were in agreement with the observed outcomes, further supporting the robustness and reliability of the nomogram. This tool can serve as a valuable asset for clinicians to recognize high-risk patients promptly and implement focused interventions to lower the incidence of PPIs in patients with TICH.
Discussion
In this study, we aimed to develop and validate a predictive nomogram for assessing the risk of PPI in patients with TICH following surgical intervention. Pulmonary infections remain one of the most common and challenging complications in TICH patients, often prolonging hospital stays and increasing the risk of mortality. Our study identified several independent risk factors for PPI, including age ≥60 years, smoking history, GCS score <8, mechanical ventilation duration >3 days, and chest injury. A nomogram was constructed to estimate the risk of infection, allowing for early identification of high-risk patients and the implementation of targeted preventive strategies.
Our findings demonstrated that advanced age, particularly ≥60 years, was a significant predictor of PPI in TICH patients. This observation aligns with prior studies that have found that age is a crucial determinant of infection risk in trauma patients. The immunosenescence associated with aging leads to a decline in immune function, making older individuals more susceptible to infections.15,16 In addition, older patients often have comorbidities and decreased physiologic reserves, which further increase the risk of post-operative complications, including infections. 17
Smoking history emerged as another critical factor, with a nearly three-fold increase in the odds of PPI. Smoking is widely acknowledged as a key risk factor for pulmonary infections, primarily because of its detrimental effects on mucociliary clearance, immune response, and lung function. 18 The prevalence of smoking in TICH patients, combined with the presence of underlying trauma, exacerbates the risk of lung infections post-operation. These findings underscore the need for smoking cessation programs in patients with TBI as part of pre-operative management.
The GCS score is widely used as a clinical tool to assess the severity of TBI. In our study, a pre-operative GCS score of <8 was strongly associated with the development of PPIs. This finding aligns with previous research that indicates that lower GCS scores, indicative of more severe brain injury and impaired consciousness, are linked to a greater risk of respiratory complications. 19 Patients with severe brain injury often require prolonged mechanical ventilation and are at increased risk for VAP, which is a well-known contributor to PPIs. 7
Mechanical ventilation for more than 3 days was identified as the most significant risk factor in our study, with OR of 6.25. The longer duration of ventilation increases the likelihood of VAP, which is a major cause of hospital-acquired infections among critically ill patients. 20 Prolonged mechanical ventilation predisposes patients to aspiration, bacterial colonization of the lower respiratory tract, and impaired clearance of secretions, all of which contribute to infection risk.8,21 Early extubation and strict adherence to ventilator care protocols are crucial in minimizing this risk.
Chest injury was another independent predictor of PPI. Trauma to the chest can result in rib fractures, lung contusions, and hemopneumothorax, all of which compromise pulmonary function and increase the risk of infection. 22 In TICH patients, chest trauma often necessitates mechanical ventilation and impairs the ability to clear secretions, further predisposing these patients to pulmonary infections. Our findings are consistent with studies that highlight the increased incidence of respiratory complications in trauma patients with concurrent chest injuries.23,24
The nomogram developed in this study integrates five independent risk factors—age, smoking history, GCS score, mechanical ventilation duration, and chest injury—into a user-friendly tool for predicting the risk of PPI. The calibration curve demonstrated that the nomogram’s predicted probabilities closely aligned with the actual observed outcomes, confirming its reliability and accuracy. The AUC was 0.801, indicating good discriminative ability. Internal validation using bootstrap resampling further reinforced the robustness of the model, making it a practical tool for clinicians.
In clinical practice, the nomogram can be used to stratify patients based on the risk of PPI developing in them. For high-risk patients, preventive measures such as early mobilization, chest physiotherapy, and the use of noninvasive ventilation should be prioritized to reduce the incidence of infection. In addition, targeted antibiotic prophylaxis and strict infection control protocols should be implemented to mitigate the risk of pulmonary complications in vulnerable patients.
Despite the strengths of this study, including the use of a large well-defined cohort and robust statistical methods, there are several limitations. First, this study was carried out at a single center, which may restrict the applicability of the findings to other populations or healthcare settings. Second, although internal validation was performed, external validation using data from multiple centers would further enhance the reliability of the nomogram. Third, some potential confounding factors, such as the use of corticosteroids or immunosuppressive therapy, were not included in the analysis and may have influenced the results. Future studies should aim to validate the nomogram in different clinical settings and explore the incorporation of additional parameters, such as inflammatory biomarkers and comorbidities, into the model. In addition, the role of early intervention strategies based on risk stratification should be investigated to determine their impact on reducing the incidence of PPI in TICH patients.
Conclusion
In conclusion, this study identifies age ≥60 years, smoking history, GCS score <8, mechanical ventilation duration >3 days, and chest injury as independent risk factors for PPI in patients with TICH. The nomogram developed from these factors provides an effective tool for predicting infection risk and can guide clinicians in implementing preventive measures for high-risk patients. The model demonstrated strong predictive accuracy and reliability, with potential for improving patient outcomes through early intervention.
Authors’ Contributions
Conceptualization: J.-R.Y., H.H., H.L., Z.Y., J.-T.T., and Q.Z. Methodology: J.-R.Y., H.H., Z.Y., J.-T.T., and Q.Z. Software: J.-R.Y. and J.-T.T. Validation: J.-R.Y. and H.L. Formal analysis: Z.Y. and J.-T.T. Investigation: J.-R.Y., H.H., and H.L. Data curation: H.L. Writing—original draft: J.-R.Y., H.H., Z.Y., J.-T.T., and Q.Z. Writing—review and editing: J.-R.Y. and H.L. Visualization: J.-R.Y. and H.L. Resources: J.-T.T. and Q.Z. Supervision: J.-T.T. and Q.Z.
Footnotes
Acknowledgments
The authors would like to express their deepest gratitude to all the patients who participated in this study.
Author Disclosure Statement
The authors report no conflicts of interest.
Funding Information
No funding was received for this article.