
Abstract
Abstract
The objective of this study was to modify titanium nonwoven fabrics (Ti) with a hydroxyapatite (HA)–like coating and fibroblast growth factor (FGF)-2 combination, and evaluate the bone regeneration potential of the modified Ti. Biodegradable gelatin hydrogel microspheres (GM) were prepared as a carrier matrix for the controlled release of FGF-2. Ti, HA-coated Ti (Ti-HA), and Ti-HA incorporating GM (Ti-HA-GM) infused FGF-2 were applied to skull defects of rabbits. Then osteointegration in the Ti was evaluated by alkaline phosphatase activity, Ca2+ content, and histological observation, and the hemoglobin content was assessed for angiogenic measurement. Ti-HA-GM promoted bone regeneration to a significantly greater extent than Ti, Ti-HA, or mixed Ti-HA and free FGF-2 6 weeks after application, and it also enhanced the hemoglobin content. It is concluded that the combination of HA-like coating and FGF-2 release promotes Ti induction of bone regeneration.
Introduction
It has been reported that fibroblast growth factor (FGF)-2 can stimulate bone formation.8–10 However, when used in the free form, FGF-2 does not exhibit the expected in vivo biological activity because of its short half-life in vivo. As a practical method to overcome this problem, a biodegradable hydrogel of acidic gelatin was examined, and it enabled FGF-2 to achieve controlled release at the site of action, 11 resulting in enhancement of FGF-2–induced bone regeneration. In this release system, FGF-2 is immobilized in the hydrogel mainly through the ionic interaction between it and gelatin molecules. The FGF-2 immobilized is released from the hydrogel matrix only when the hydrogel is degraded to generate water-soluble gelatin fragments. The time profile of FGF-2 release can be regulated by changing that of hydrogel degradation. We have demonstrated that the controlled release of FGF-2 from gelatin hydrogel promotes biological activity to induce bone regeneration.12,13
In this study, the FGF-2 release system was combined with HA-like coated Ti to provide them with osteointegrative activity. After the fabrics combined with gelatin hydrogel microspheres incorporating FGF-2 were applied to rabbit skull defects, the bone regeneration at the defects was assessed and compared with that of the fabrics with or without free FGF-2. We also evaluated the in vivo profile of FGF-2 release from the Ti combined with gelatin microspheres incorporating FGF-2 and free FGF-2.
Materials and Methods
Preparation of HA-like coated Ti and those combined with gelatin microspheres incorporating FGF-2
Ti (fiber diameter, 50 μm; 87 v/v% porosity; average pore size, 200 μm) were kindly supplied by HI-LEX Corporation, Takarazuka, Japan. The fabrics were cut into a round shape (diameter, 4 mm; thickness, 1.5 mm). All samples were ultrasonically cleaned with 70 v/v% ethanol and distilled water for 15 min. A fivefold-concentrated simulated body fluid (5SBF) was prepared according to the methods described previously.14,15 The chemical compositions of human blood plasma and 5SBF are summarized in Table 1. Briefly, 5SBF was prepared by dissolving 19.99 g of NaCl, 0.875 g of NaHCO3, 0.560 g of KCl, 0.570 g of K2HPO4-3H2O, 0.358 g of MgCl2, 0.695 g of CaCl2, and 0.180 g of Na2SO4 in 500 mL of demineralized water in which CO2 gas was bubbled. All materials were of special reagent grade and were used without further purification (Nacalai Tesque, Kyoto, Japan). Ti was immersed in 50 mL of 5SBF at 37°C for 3 days to obtain HA-coated Ti (Ti-HA). The Ti-HA thus prepared was observed using a scanning electron microscope (SEM, S2380N; HITACHI, Tokyo, Japan). X-ray diffraction (XRD) analysis was carried out as reported previously, 16 using a microbeam XRD system (M18XHF22-SR, Mac Science). Cu-Kα radiation was generated at a tube voltage of 40 kV and a tube current of 90 mA. A titanium nonwoven fabric was swung and rotated in the appropriate range of Eular angles to obtain sufficient diffraction intensity. The scattered diffraction was registered using a curved position-sensitive proportional X-ray counter.
Gelatin hydrogel microspheres (GM) were prepared for the controlled release of FGF-2 according to the method reported previously. 17 An FGF-2-free GM suspension in distilled water was inoculated into Ti-HA using a 1 mL syringe (TERUMO, Tokyo, Japan); the GM were trapped inside the Ti-HA, followed by freeze-drying to obtain Ti-HA incorporating GM (Ti-HA-GM). All the fabrics prepared were sterilized with ethylene oxide gas for the following in vivo experiments. FGF-2 solution 20 μL (2.5 mg/mL), kindly supplied by Kaken Pharmaceutical (Tokyo, Japan), was dropped onto the freeze-dried Ti-HA-GM, after which it was left at 37°C for 60 min to obtain Ti-HA-GM containing 50 μg of FGF-2. As a control, 20 μL of FGF-2 solution was similarly dropped onto the Ti and Ti-HA to prepare the respective samples containing 50 μg of FGF-2.
Implantation of Ti combined with gelatin microspheres incorporating FGF-2 into rabbit skull defects
In vivo bone regeneration of bone defects in rabbit skulls was evaluated according to a surgical procedure reported elsewhere.13,18 For implantation, six healthy skeletally mature Japanese white rabbits weighing 2.5–3.0 kg were used. They were anesthetized by intramuscular administration of ketaral and pentobarbital. The skin of the rabbit head was cut to expose the skull, and after incision of the pericranium, six defects 4 mm in diameter per head were carefully prepared using a surgical microdrill without injuring the underlying dura mater. Following the application of Ti, Ti-HA, or Ti-HA-GM combined with or without 50 μg of FGF-2 (a total of 36 implants) into the defects, the pericranium and skin were carefully sutured a with 4-0 nylon monofilament. All the animal experiments were performed according to the Institutional Guidance of Kyoto University on Animal Experimentation. Three defects randomly selected from different rabbits were used for each fabric at different sampling time points. The animals were euthanized 3 and 6 weeks after the procedure, and the skull bone was removed and prepared for the following biochemical and histological analyses.
Biochemical and histological evaluation of bone formation
Bone regeneration at the defect was assessed by alkaline phosphatase (ALP) activity, Ca content, and histological examinations 3 and 6 weeks after application. Hemoglobin content was measured to assess the neovascularization in or around the Ti. Each specimen collected (n = 3) was immediately frozen and preserved in a freezer at −30°C until the examinations. For the measurement of ALP activity and hemoglobin content, they were mixed in 1 mL of 0.2 w/v% IGEPAL (Sigma, St. Louis, MO) containing 10 mM Tris-HCL and 1 mM MgCl2 (pH 7.5), and stored for 3 days in a refrigerator at 4°C.
The ALP activity was assayed using a commercial kit (alkaline phosphor B-test, Wako #TQ717; Wako Pure Chemical, Osaka, Japan) based on the absorbance measurement of a p-nitrophenol product generated by ALP digestion. Briefly, 80 μL of the tissue sample prepared by the method described above was mixed with 100 μL of 6.7 mM p-nitrophenyl phosphate aqueous solution, followed by standing at 37°C for 15 min. After mixing with 1 mL of 20 mM NaOH aqueous solution, the absorbance of the solution was measured at 405 nm with a spectrophotometer (VersaMax™; Molecular Devices, Tokyo, Japan) to assess the ALP activity.
The tissue sample was incubated in 1 mL of 1 M HCl solution by shaking for 24 h at 4°C. The amount of Ca2+ in the HCl solution obtained was determined using a commercial kit (Calcium C-test, Wako #TH994; Wako Pure Chemical, Osaka, Japan). Briefly, 10 μL of the sample solution in HCl was mixed with 1 mL of 0.88 M monoethanolamine aqueous solution. After mixing with 100 μL of aqueous solution containing 69 mM 8-hydroxyquinoline and 0.63 mM o-cresolphtalein, the solution was allowed to stand at room temperature for 5 min. The absorbance of the solution was measured at 570 nm by spectrophotometry to assess the amount of Ca2+.
The hemoglobin content was determined using a hemoglobin assay kit (Wako Pure Chemicals, Kyoto, Japan) based on a calibration curve obtained using hemoglobin standard solutions.
For histological examination, the specimens were fixed with 10 w/v% neutral phosphate-buffered formaldehyde solution, dehydrated in a graded series of ethanol, and embedded in polyester resin (Rigolac 2004; SHOWA HIGH POLYMER, Isesaki, Japan). Following polymerization reaction, cross sections were prepared on a microtome (Crystal Cutter, MC-415Y; MARUTO INSTRUMENT, Tokyo, Japan). 19 All the sections were conventionally stained with Cole's H-E stain, and viewed by light microscopy for bone formation (ECLIPSE E800; Nikon, Tokyo, Japan). Image analysis was performed to evaluate the ingrowth and newly formed bone area at the inner surface of the fabric. The histological sections were digitalized at low magnification, and the bone tissue and titanium were detected using Image J software (NIH). Newly formed bone was measured and the area calculated.18,20
Estimation of in vivo FGF-2 release of titanium nonwoven fabrics combined with gelatin microspheres incorporating FGF-2 or free FGF-2
FGF-2 was radioiodinated according to the conventional chloramine-T method.11,21 125I-labeled FGF-2 solution (20 μL) was impregnated into Ti, Ti-HA, and Ti-HA-GM to prepare the respective titanium samples incorporating 125I-labeled FGF-2. The fabric samples combined with 125I-labeled FGF-2 were implanted into the back subcutis in ddY mice (three mice per group, 6–7 weeks old). At 1, 3, 5, and 7 days after implantation, the fabric was taken out, and the tissues around it carefully removed. In addition, the mouse back skin around the implantation site was removed and the corresponding facial area was thoroughly wiped off with filter paper. The radioactivity of the explanted fabric, the skin strip, and the filter paper was measured to evaluate the time profile of FGF-2 remaining around the implanted fabric. Each group at every sampling time was composed of three mice.
Statistical analysis
All the data were evaluated using ANOVA followed by the Tukey–Kramer multiple comparison test. Experimental results were expressed as the mean ± standard error.
Results
Characterization of apatite-like coated Ti combined with gelatin microspheres
Figure 1 shows the scanning electron micrographs of titanium nonwoven fabric with or without apatite-like coating, and the XRD pattern of the apatite-like coated fabric. After immersion in 5SBF, an apatite-like structure of needle-like crystallites was coated on the nonwoven titanium fabric. In the pattern of XRD, (002) diffraction at 25.9°, an envelope of (211) (112) (300) diffractions at around 32°, and (310) diffraction at 39.8° are characteristic of bone-like apatite. The Ca/P ratio of the apatite-like coating was determined to be 1.506 by energy dispersive spectroscopy analysis (data not shown). The Ca2+ content of the apatite-like coating on Ti was 3.62 ± 0.91 μg per 1 mg of Ti.
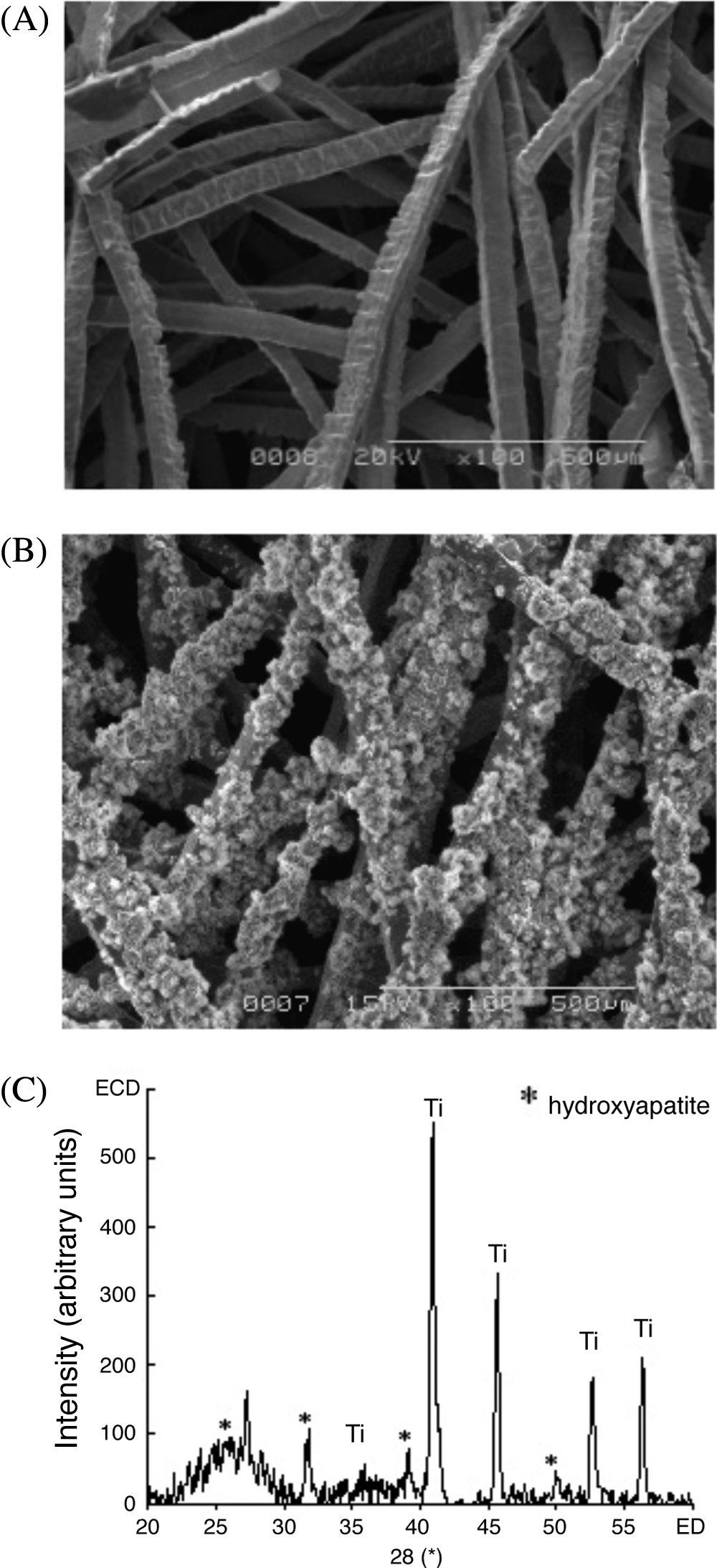
Scanning electron micrographs of a titanium nonwoven fabric (
The gelatin content was 1.11 ± 0.29 mg/sample of Ti-HA-GM.
Biochemical evaluation of bone regeneration by Ti combined with gelatin microspheres incorporating FGF-2 or free FGF-2
Figure 2 shows the ALP activities at the skull defects 3 weeks after application of various titanium nonwoven fabrics. The highest ALP activity was that of Ti-HA-GM (FGF+), 64.6 ± 15.9 IU/mg tissue. The second highest ALP activity was that of Ti-HA, 48.6 ± 18.2 IU/mg tissue. The lowest ALP activity was that of Ti-HA combined with free FGF-2 (26.2 ± 10.1 IU/mg tissue), which was similar to that of FGF-2-free Ti (36.1 ± 12.5 IU/mg tissue). The ALP activity of the HA-Ti-GM (FGF+) was significantly greater than those of Ti, Ti-HA-GM (31.0 ± 12.1 IU/mg tissue), Ti (FGF+) (35.2 ± 2.46 IU/mg tissue), and Ti-HA (FGF+).
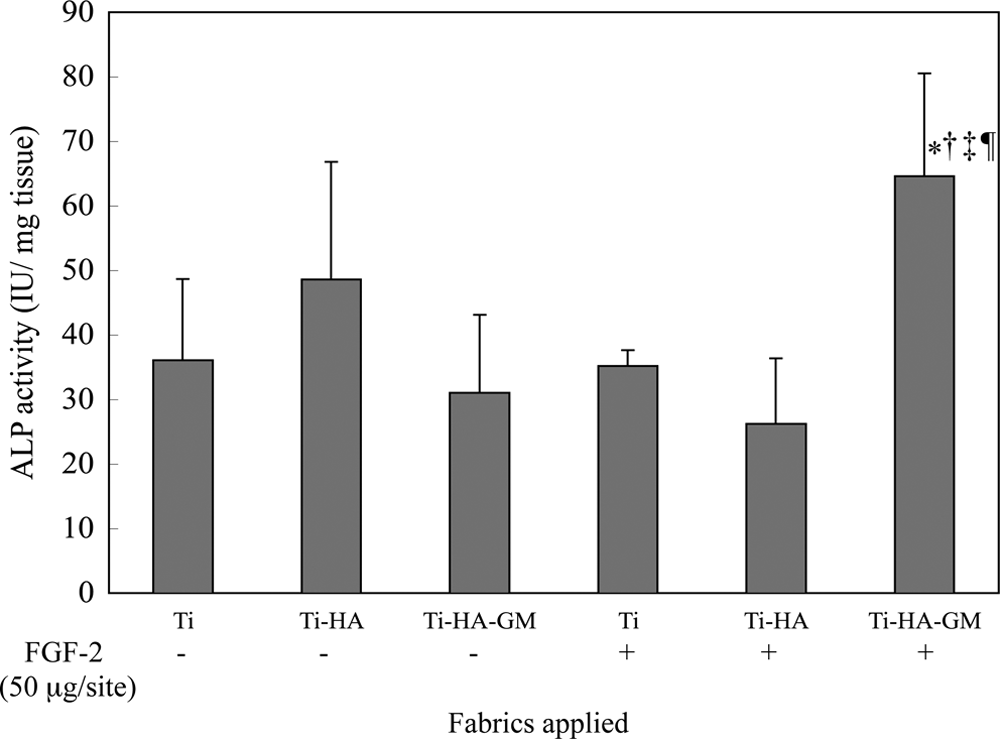
ALP activities at the skull defects of rabbits 3 weeks after treatment with various titanium nonwoven fabrics. *p < 0.05: significant difference from the ALP activity of the Ti (FGF-) group. †p < 0.05: significant difference from the ALP activity of the Ti-HA-GM (FGF-) group. ‡p < 0.05: significant difference from the ALP activity of the Ti (FGF+) group. ¶p < 0.05: significant different from the ALP activity of the Ti-HA (FGF+) group.
Figure 3 shows the Ca2+ contents at the skull defects 3 and 6 weeks after application of the fabrics. At 3 weeks, the highest Ca2+ content was observed for Ti-HA-GM (FGF+), 39.3 ± 6.6 μg/mg tissue. This was significantly greater than those of Ti (17.8 ± 5.3 μg/mg tissue), Ti-HA (13.3 ± 3.9 μg/mg tissue), and Ti (FGF+) (15.1 ± 3.4 μg/mg tissue). The second highest Ca2+ content, 38.8 ± 16.8 μg/mg tissue, was observed for Ti-HA (FGF+). This was significantly greater than those for Ti and Ti-HA. This implied that Ti-HA infused with FGF-2 increased the mineral supply until 3 weeks after treatment, but that the effects did not continue after that. At 6 weeks, the highest Ca2+ content was found with Ti-HA-GM (FGF+) (178.0 ± 23.4 μg/mg tissue), which was significantly different from those of other groups. Similar to the ALP activity, Ti-HA-GM (FGF+) was significantly effective in enhancing the Ca2+ content, in marked contrast to the other fabrics.

Ca2+ content at the bone defect 3 weeks (white bar) and 6 weeks (gray bar) after treatment. *p < 0.05: significantly different from the Ca2+ content of the Ti (FGF-) group 3 weeks after treatment. †p < 0.05: significantly different from the Ca2+ content of the Ti-HA (FGF-) group 3 weeks after treatment. ‡p < 0.05: significantly different from the Ca2+ content of the Ti (FGF+) group 3 weeks after treatment. §p < 0.05: significantly higher for the Ti-HA-GM (FGF+) group than for the other groups 6 weeks after treatment.
Angiogenesis by titanium nonwoven fabrics combined with gelatin microspheres incorporating FGF-2 or free FGF-2
Figure 4 shows the hemoglobin contents at the skull defects with various titanium nonwoven fabrics after 3 weeks. The highest hemoglobin content was found with Ti-HA-GM (FGF+), 3.8 ± 0.6 μg/mg tissue, which was significantly greater than those for Ti-HA (2.1 ± 0.4 μg/mg tissue), Ti (FGF+) (1.7 ± 0.7 μg/mg tissue), and Ti-HA (FGF+) (1.9 ± 0.3 μg/mg tissue). The second highest hemoglobin content, 3.2 ± 0.5 μg/mg tissue, was found with Ti-HA-GM, followed by 2.6 ± 0.7 μg/mg tissue for Ti. The contents of these two samples were not significantly different from those of the other samples. Ti-HA-GM (FGF+) significantly enhanced angiogenesis, whereas Ti-HA combined with free FGF-2 did not exhibit any angiogenic effects, like FGF-2 free Ti and Ti-HA.
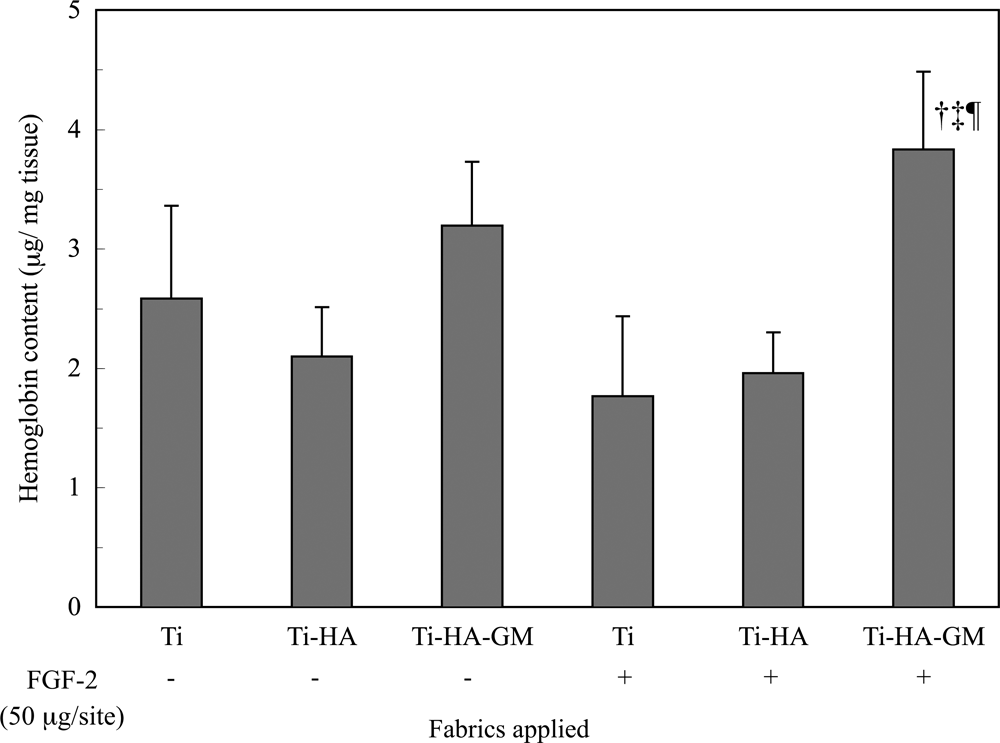
Hemoglobin (Hb) content at the skull defects of rabbits 3 weeks after treatment with various titanium nonwoven fabrics. †p < 0.05: significantly different from the Hb content of the Ti-HA (FGF-) group ‡p < 0.05: significantly different from the Hb content of the Ti (FGF+) groups. ¶p < 0.05: significantly different from the ALP activity of the Ti-HA (FGF+) group.
Histological evaluation of bone regeneration by titanium nonwoven fabrics combined with gelatin microspheres incorporating FGF-2 or free FGF-2
Figure 5 shows histological sections from around the skull defects of rabbits 6 weeks after application of the various fabrics at low magnification. Table 2 shows the new bone areas calculated by histological analysis of the skull defects. The largest bone area was for Ti-HA-GM (FGF+), and it was significantly greater those for Ti-HA-GM (FGF-) and Ti-HA (FGF+). This was similar to the findings for Ca2+ content determined by biochemical evaluation. The second largest bone area was found with Ti-HA. Similarly, this was significantly greater than for Ti-HA-GM (FGF-) and Ti-HA (FGF+). Figure 6 shows histological sections at the inner surfaces of the fabrics in high magnification to observe the histological differences and cell types. When the rabbit skull defect was treated with Ti (Fig. 6A), infiltration of inflammatory cells and blood corpuscles was seen, while osteoid formation occurred around the Ti. At the skull defect with Ti-HA (Fig. 6B), there was significant regeneration of bone tissue with bone marrow structure as well as osteoid and lamellar structures, though there were few blood corpuscles, fibrous tissues, and osteoblasts. In addition, mineral deposition was significant due to the osteoconduction of the apatite-like material. When Ti and Ti-HA combined with free FGF-2 (Fig. 6D, E) or Ti-HA-GM (Fig. 6C) were applied, no significant bone regeneration was observed but ingrowth of soft connective tissues into the fabrics was detected. The combination with FGF-2 or GM alone could induce proliferation of fibroblasts and soft connective tissues, but could not accelerate the osteoinduction of the fabrics. In contrast, Ti-HA-GM incorporating FGF-2 (Fig. 6F) significantly induced bone regeneration accompanied by osteoblasts, blood corpuscles, fibrous tissue, and bone marrow–like structures, which is the typical process of membranous ossification. Thus, Ti-HA-GM incorporating FGF-2 could accelerate wound healing and bone induction.
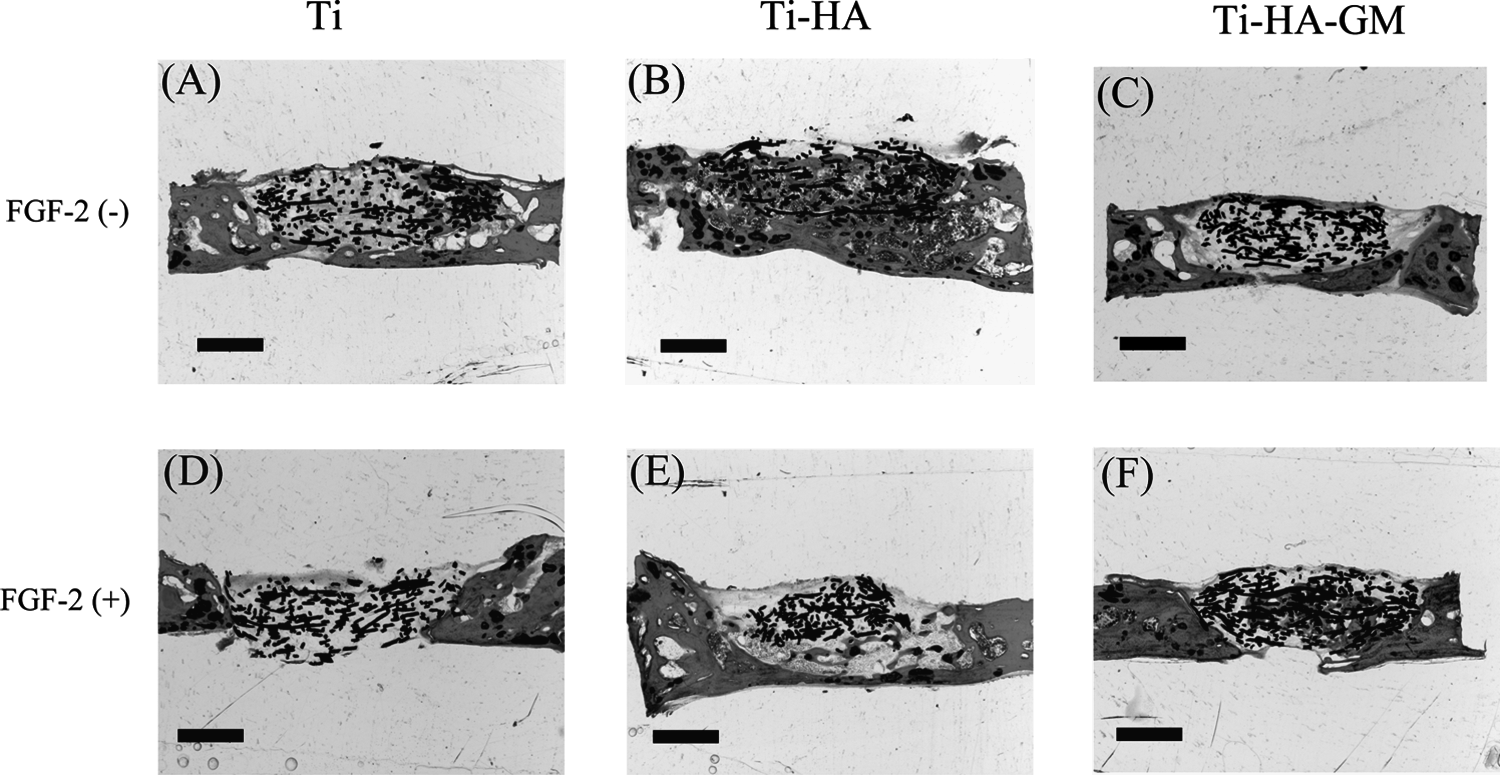
Histological cross sections from around the skull defects of rabbits 6 weeks after application of FGF-2-free Ti (
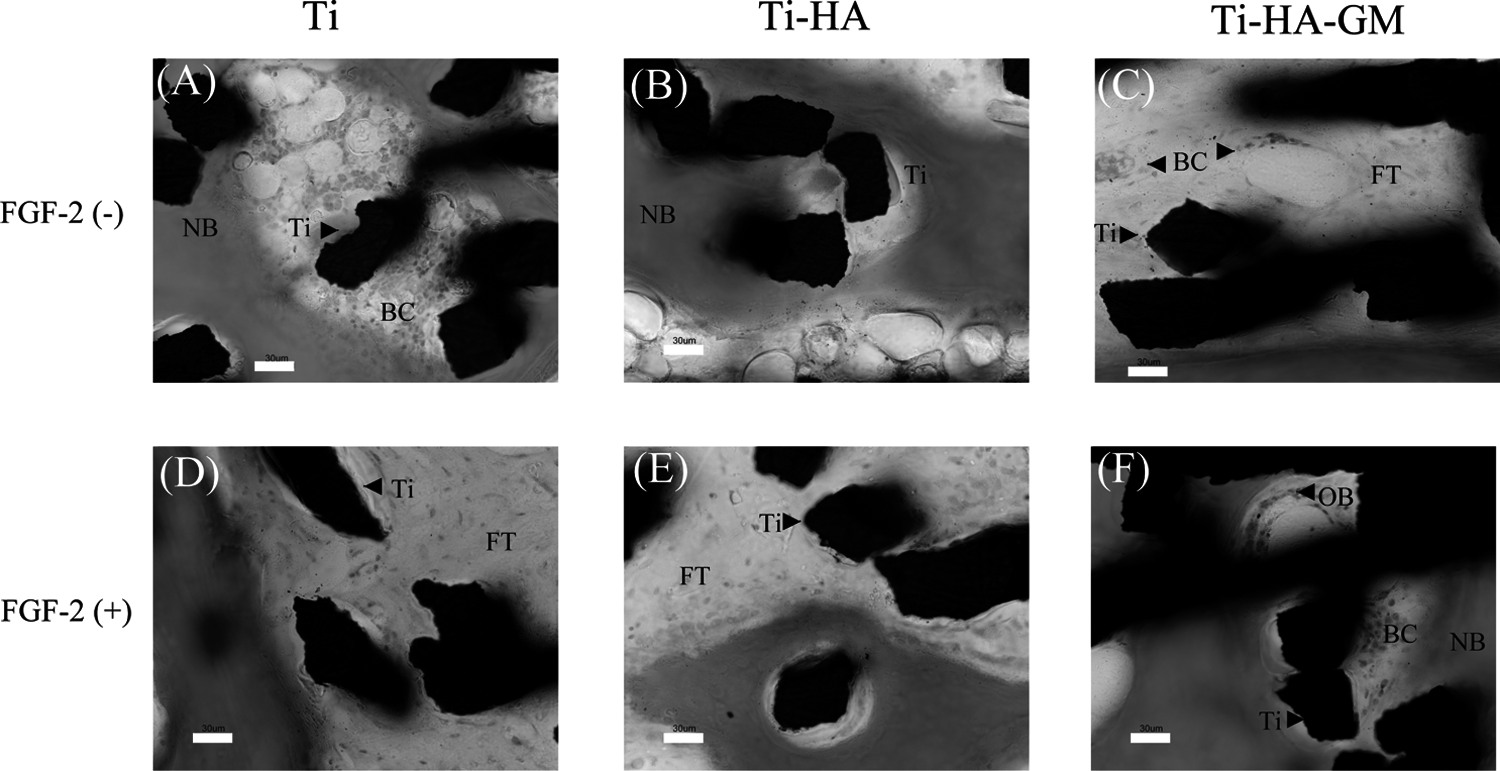
Histological cross-sections from the inner surfaces of the fabrics in the skull defects of rabbits 6 weeks after application of FGF-2-free Ti (
ap < 0.05: significant against the bone area of Ti-HA-GM (FGF−) group.
bp < 0.05: significant against the bone area of Ti-HA (FGF+) group.
In vivo time course of FGF-2 release
Figure 7 shows the time courses of radioactivity remaining after subcutaneous implantation of Ti, Ti-HA, and Ti-HA-GM combined with free 125I-labeled FGF-2 into the mouse back. Irrespective of the fabric type, the residual radioactivity of FGF-2 decreased with implantation time. The residual radioactivity levels of Ti and Ti-HA rapidly decreased to 25% within 3 days after implantation. However, for Ti-HA-GM, more FGF-2 remained for a longer time than with the other fabrics.
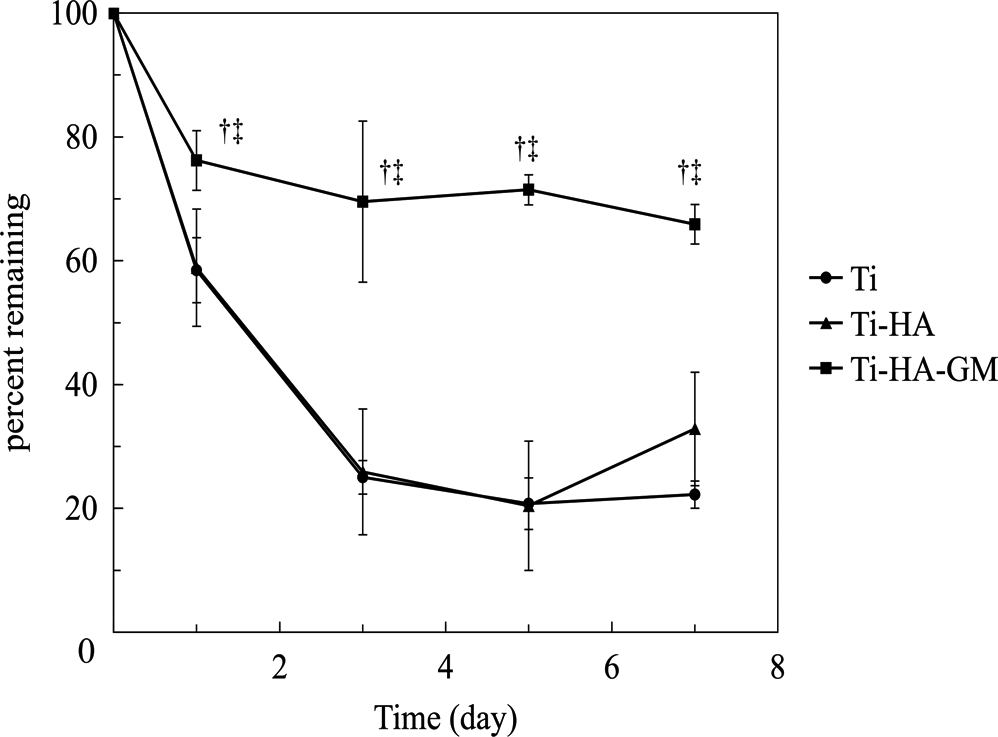
The time courses of remaining radioactivity of various titanium nonwoven fabrics incorporating 125I-labeled bFGF after implantation into the back subcutis in mice: Ti (●), Ti-HA (▴), and Ti-HA-GM (▪). †p < 0.05: significantly different from the percent remaining in the Ti group at the corresponding time. ‡p < 0.05: significantly different from the percent remaining in the Ti-HA group at the corresponding time.
Discussion
The present study demonstrated that combination with an FGF-2 release system significantly enhanced the bone regeneration potential of HA-coated titanium nonwoven fabrics upon application to skull defects of rabbits. The biochemical parameters and histology were clearly enhanced by the application of the system to Ti-HA-GM. This enhanced potential can be explained in terms of FGF-2 activity promoting the process of bone regeneration. The gelatin microspheres enabled FGF-2 not only to enhance the local concentration at the bone defect, but also to prolong the enhanced concentration, resulting in the promotion of the biological activity of bone regeneration. Simple combination with free FGF-2 did not enhance the Ti-HA bone regeneration potential. This is because with Ti-HA the controlled release of FGF-2 did not occur, in marked contrast to Ti-HA-GM.
It is recognized that HA coating gives titanium fiber implants an osteoinductive nature, and it has been reported that HA accelerates osteodifferentiation in vitro. 22 In addition, many researchers have demonstrated that ceramic implants induce bone formation more strongly than titanium implants.23–26 Despite the biological advantages of HA, its poor mechanical properties and resorbability remain as problems for clinical application. In this study, there was no significant difference in the biological parameters between Ti and Ti-HA. However, the bone surface area was higher for Ti-HA than for Ti. Thus, the coating procedure with HA is promising to simply make titanium nonwoven fabrics osteoinductive, and it resolves the mechanical problem of HA.
FGF-2 facilitates the proliferation of osteoblasts and periosteal cells in vitro27–29 and plays an important role in stimulating bone formation during the early stage of fracture healing of rat long bones. 30 In addition, it is a key factor in inducing neovascularization.31,32 From the viewpoint of bone regeneration, it is undoubtedly important to maintain good blood circulation around the bone graft.33–35 Ti-HA-GM enhanced the hemoglobin content to a significantly great extent compared with the other fabrics. It is likely that good blood circulation promotes the supply of oxygen, minerals, and nutrients to the defect to be regenerated. It is also thought that various humoral factors and key cells necessary for bone regeneration are provided through the blood vessels, resulting in acceleration of the regeneration process.
Wipperman et al. 36 and Wang and Aspenberg 37 demonstrated that FGF-2 increased bone ingrowth in porous HA implants in tibia defects. Schnettler et al. revealed that an HA ceramic coated with FGF-2 increased angiogenesis and bone ingrowth in pig femur defects. 38 However, the results of the present study were different from their results. Ti and Ti-HA combined with free FGF-2 did not contribute to the enhancement of osteoinduction. This can be explained in terms of FGF-2 release. FGF-2 release was observed from Ti and Ti-HA, but the amounts released and the periods of release were not as therapeutically effective as for Ti-HA-GM incorporating FGF-2. Following implantation into the rabbit skull defect, 36.5 μg of FGF-2 was rapidly released from Ti and Ti-HA within 3 days, whereas 2.4 μg of FGF-2 per day was released from Ti-HA-GM. It is likely that better FGF-2 release induces more effective biological activity, resulting in promotion of bone regeneration. FGF-2 is only absorbed on the HA surface of Ti-HA and the titanium surface of Ti. It is highly conceivable that the absorbed FGF-2 is readily detached by the host's body fluid in vivo because of the interchange of serum proteins. However, it is possible that the release mechanism of detachment does not always allow FGF-2 to sufficiently induce bone regeneration because of the amount and period of action. This is because the absorption site is so small that FGF-2 is rapidly detached. In our preliminary experiment, we studied the osteodifferentiation of rat mesenchymal stem cells in Ti, Ti-HA, and Ti-HA-GM with and without FGF-2 in vitro. Ti and Ti-HA with FGF-2 suppressed the osteodifferentiation of mesenchymal stem cells, whereas Ti-HA (FGF-) and Ti-HA-GM with FGF-2 accelerated it in vitro (data not shown). These results suggested that the FGF-2 detached from Ti and Ti-HA might be denatured and not exhibit complete biological activity. On the other hand, when the GM were loaded into Ti-HA, FGF-2 could not be easily washed away by the host's body fluid. In the in vitro experiment examining 125I-labeled FGF-2 release in phosphate-buffered saline solution, we confirmed that the 125I-labeled FGF-2 was mainly adsorbed to the gelatin microspheres in Ti-HA-GM. Inflammatory cells infiltrated into the fabric, secreted protease, and gelatin hydrogels were degraded. The FGF-2 released from the GM interacted with heparan sulfate proteoglycan in the ECM or the surface of the cells induced into the Ti-HA, resulted in acceleration of the regeneration process. It has been demonstrated that gelatin hydrogel microspheres can release FGF-2 with biological activity for a prolonged time period.
In the histological analysis, different healing processes were observed depending on the type of Ti implant. When Ti was applied to the defects, hematoma, organization, and wound healing of the bone fracture were observed. When Ti-HA was applied, bone ingrowth around the titanium fiber was promoted through its excellent osteoconductivity. However, when FGF-2 was incorporated into Ti and Ti-HA, it was just detached and released, and the consequent burst caused infiltration of inflammatory cells and soft connective tissues into the fabrics. On the other hand, when there is no FGF-2 release, the surrounding cells will not be activated to promote osteodifferentiation. When Ti-HA-GM (FGF-) was applied, inflammatory cells infiltrated the fabric. Although gelatin induced weak inflammation, the gelatin hydrogel alone could not promote bone regeneration. In contrast, when FGF-2 was sorbed into the GM of Ti-HA-GM and applied, significant promotion of bone regeneration was observed. This was because FGF-2 was released from the GM in Ti-HA-GM to enhance osteoinductive activity.
Our final goal of bone engineering is to reconstruct large bone defects of human patients. Such defects are often caused by trauma, tumors, or infection. For tissue engineering of such large defects, there will be vascularity problems during the process of bone regeneration. It is well known that after ablative surgery for malignancies, the surrounding soft tissue is heavily damaged by surgical procedures and radiation therapy.39,40 Undoubtedly, such tissue damage reduces the osteoinductive potential of the tissue. To deal with the reduced potential, tissue-engineered bone constructs should be well vascularized. FGF-2 is an angiogenic growth factor and can be used clinically at present. However, for patients with malignant tumors, FGF-2 should be employed with care, even if the tumor is surgically resected. This is because we cannot completely deny the possibility of tumor recurrence. The application of other growth factors may be one possible way to minimize this risk. For successful bone regeneration, it is practically necessary to design a biomaterial scaffold for osteoinduction with growth factors.
Conclusion
The combination of HA-coated Ti and hydrogel for controlled release of FGF-2 is promising to accelerate both bone regeneration and angiogenesis, resulting in enhanced osteointegration.
Footnotes
Acknowledgments
We thank Dr. Takayoshi Nakano and Mr. Ayumu Fujitani of the Department of Material Science and Engineering, Graduate School of Engineering, Osaka University, for their great assistance with XRD analysis. We also thank Dr. Tomoko Sonoda of the Department of Public Health, Graduate School of Medicine, Sapporo Medical University, for her great assistance with statistical analysis.