
Abstract
Three commercially available porcine-derived biologic meshes were implanted in an Old World primate abdominal wall resection repair model to compare biological outcome as a predictor of clinical efficacy. Tissues were explanted over a 6-month period and evaluated for gross pathology, wound healing strength, mesenchymal cellular repopulation, vascularity, and immune response. In vivo functional outcomes were correlated with in vitro profile for each material. Small intestinal submucosa-based implants demonstrated scar tissue formation and contraction, coincident with mesh pleating, and were characterized by immediate and significant cellular and humoral inflammatory responses. Porcine dermal-based grafts demonstrated significant graft pleating, minimal integration, and an absence of cellular repopulation and vascularization. However, a significant cellular immune response surrounded the grafts, coincident with poor initial wound healing strengths. In vivo observations for the three porcine-derived mesh products correlated with individual in vitro profiles, indicating an absence of characteristic biochemical markers and structural integrity. This correlation suggests that in vivo results observed for these mesh products are a direct consequence of specific manufacturing processes that yield modified collagen matrices. The resulting loss of biological and structural integrity elicits a foreign body response while hindering normal healing and tissue integration.
Introduction
To promote graft acceptance and prevent rejection, removal of cellular material is critical. 12 This is particularly important in non-human-derived matrices. Xenogeneic cells express numerous epitopes that hinder successful organ transplantation. However, most of these non-gal epitopes have not been well characterized or identified as a predominant impetus for eliciting a xenogenic response.13–16 As much of these epitopes may be cell associated, the majority may be removed during processing to remove cells from tissue matrices. However, non-cell-associated galactose α-(1,3)-galactose terminal carbohydrate epitopes (α-gal) may remain within the tissue matrix on n-linked glycoproteins even following decellularization processing. These epitopes have been shown to bind to naturally occurring α-gal antibodies in humans and Old World monkeys, 17 eliciting a rapid, complement-driven, hyperacute rejection response to porcine organs transplanted into primates.17–20 Although not participating in the classical hypercacute rejection pathway, acellular xenogeneic tissues have previously been shown to elicit a diminished inflammatory response associated with implantation in primates following α-gal removal. 21 Likewise, the interaction of naturally occurring anti-α-gal antibody in humans with α-galactosyl epitopes on animal-derived organs has been a major obstacle for clinical xenotransplantation. Thus, the α-gal epitope has become a major focus for acellular tissue xenotransplantation.
Distinct clinical outcomes are likely for individual biologic mesh products, based on the variety of tissue origins as well as distinct processing and sterilization procedures. Thus far, no single study has compared the clinical outcomes among G-PDM, SIS, and EO-PDM in a clinically immunologically relevant model. Such a comparison would aid surgeons to make informed choices regarding biologic repair matrix selection for their patients.
In an attempt to address this shortcoming, a recent study compared the host-tissue morphologic response to five different biologic scaffolds typically used in orthopedic applications (GraftJacket, acellular human dermal matrix; Restore, porcine small intestinal submucosa; CuffPatch, acellular porcine small intestinal submucosa; TissueMend, acellular fetal bovine dermis; and G-PDM) in a rodent body-wall repair model. 22 However, as rodents are immunologically dissimilar to humans, the host response in this study may not be predictive of the clinical response.
To support the hypothesis that matrix structure and biologic property preservation during the manufacturing process are critical for the coordinated sequence of biological events that allow for graft integration and acceptance following implantation, we have compared the in vitro attributes (biochemistry and histology) of three biologic matrices commonly used for abdominal wall repair (G-PDM, SIS, and EO-PDM) and have correlated these to host-tissue morphologic and immunologic responses over time in a previously described Old World primate model (Caribbean vervet) of abdominal wall resection repair. 23 Caribbean vervets (Cercopithecus aethiops) have been used extensively in biomedical research to understand the etiology, biology, and development of numerous human disorders because of similarities to human anatomy, physiology, immunology, and metabolism. 24 The rationale for use of the African Green monkey model in this study is its similarity to the human immune system in terms of the absence of both cell-associated and non-cell-associated xenogeneic epitopes (including α-gal epitopes), its consequential presence of anti-xenogenic antibodies (including anti-α-gal) in the serum, and its ability to mount a normal foreign body response. The African Green monkey, therefore, appears to be a relevant model to study clinical immune response to implanted biologic materials.
Materials and Methods
Biomaterials
The biomaterials in this study are commercial products manufactured by the following: Surgisis Gold (SIS), Cook Biotech, West Lafayette, Indiana; Permacol (G-PDM), Tissue Science Laboratories, Andover, Massachusetts; and CollaMend (EO-PDM), Davol, Cranston, Rhode Island. Biomaterials were prepared according to product package inserts.
In vitro analyses
In vitro analyses of biomaterials were performed prior to implant to determine structural and biochemical content and integrity as well as biophysical (thermodynamic) properties. A determination of the integrity of these matrices was made based on the outcomes of these tests, and an effort was made to correlate these results, namely, the presence of degraded or crosslinked matrix species, to in vivo outcomes. Analyses included routine histological staining with hematoxylin and eosin (H&E) to evaluate graft structural integrity, sodium dodecyl sulfate polyacrylamide gel electrophoresis (SDS)-PAGE to evaluate collagens for relative solubility and crosslinking, cellulose acetate electrophoresis for the presence of glycosaminoglycans (GAGs) (hyaluronic acid [HA] and chondroitin sulfate [CS]), which are labile and may be lost through processing, and differential scanning calorimetry (DSC) for thermal transition profiles as a measure of collagen denaturation and crosslinking. Finally, histological sections were assessed for α-gal epitope expression to correlate with in vivo function.
Biomaterial matrix structure and α-gal expression
Both H&E and anti-α-gal immunohistochemical stainings were performed on unimplanted graft materials to determine the structural integrity and presence of α-gal epitopes prior to implant for eventual correlation with in vivo outcomes. Unimplanted samples were processed for routine histology, stained with H&E, and assessed with the entire specimen being evaluated at 40 ×, 100 ×, and 200 × magnifications to give a representative description of each material. All histological findings were recorded on data sheets.
Frozen sections were produced from each biomaterial and were incubated with biotinylated Grffonia (Bandeiraea) Simplicifolia Lectin I Isolectin B4 (Vector Laboratory, Burlingame, CA) for 1 h at room temperature followed by incubation with HRP-conjugated streptavidin (Zymed/Invitrogen, Carlsbad, CA) for 30 min. The sections were then developed for α-gal expression and assessed as above.
Collagen analysis
Biomaterials were rinsed, lyophilized, micronized, and extracted with 4 M guanidine, followed by digestion with pepsin, using a method previously described. 25 Human placental type I and type III collagens were run alongside graft samples on polyacrylamide gels. Gel loading was normalized for total collagen content by a spectrophotometric assay for hydroxyproline, as previously described. 26 Gels were stained with Coomassie brilliant blue for collagen detection.
GAG analysis by cellulose acetate electrophoresis
Samples were digested and applied to cellulose acetate membranes based on a previously described method 27 along with HA/CS mixed standards. Electrophoresis was performed at 34 V for 3 h on ice and the membrane stained with 0.02% Alcian blue for GAG detection. Since GAGs are present in native skin, but can be lost during processing, 28 their presence in a biologic graft is one measure of retention of matrix integrity.
Differential scanning calorimetry
Samples were washed with saline and analyzed using a Differential Scanning Calorimeter (DSC-Q100; TA Instruments, New Castle, DE). Samples (15–20 mg) were hermetically sealed in aluminum crucibles, heated at 3°C/min from 2°C to 95°C, and dried in a vacuum oven (100–110°C) for 15 h to determine dry weight. TA Universal Analysis software was used to calculate melting onset temperature and transition enthalpy for each sample, normalized by dry weight. DSC yields an indirect measure of collagen thermal stability and may be able to detect tissue modification due to dehydration and different crosslinking chemistries. 29
Creation and repair of abdominal wall resection in a primate model
Procurement and handling of 33 adult (3–6 kg) Caribbean vervets (C. aethiops) as well as abdominal wall resection, repair and sacrifice procedures at 1, 3, and 6 months postoperatively were performed as previously described. 23 Briefly, animals were anesthetized by intramuscular injection with ketamine HCl (10 mg/kg) and xylazine (1 mg/kg). A longitudinal midabdominal incision was made to expose an area of the abdominal muscle wall, and a bilateral longitudinal full-thickness defect (3 × 7 cm) was created by removal of fascia, rectus muscle, and peritoneum. Defects were repaired with test articles (G-PDM, n = 15; SIS, n = 9; EO-PDM, n = 9) in a manner that imparted a uniform tension across the graft to close the defect. Implants were approximated to the edges of the defect with continuous 3-0 Prolene sutures (Ethicon, Somerville, NJ) that incorporated 3–5 mm of adjacent rectus abdominal muscle and fascia. Skin was closed with continuous 2-0 polydioxanone resorbable sutures (Ethicon). Following surgery, animals were monitored daily and wounds examined for inflammation, including redness, heat, and swelling.
Gross analysis of implanted biomaterials
Grafts were explanted as previously described. 23 Briefly, animals were euthanized by intravenous injection of pentobarbital solution at 1, 3, and 6 months following implantation. The repair site was exposed, and the graft and surrounding host tissues excised by making an incision 2.5 cm to the outside circumference of the implant. Grafts were evaluated through visual and tactile observations in situ for defects (holes or tears) as well as herniation, or protrusion of abdominal tissues through such a defect. The presence of scar tissue was inferred by tactile assessment of a change in graft properties to that of a generally tougher, harder material than what had originally been implanted. Graft pleating was determined visually and was noted where there were obvious undulations in the graft interrupting the normal smooth plane of the surgical site. Length and width of each graft was measured using permanent sutures to delineate graft edges and determine extent of graft contraction. Calculated percent contraction (percentage reduction in initial graft area upon explantation) was analyzed using analysis of variance (ANOVA), and Tukey's test was used for comparison among the three biomaterials and different time points. Statistical analysis was not conducted for observational data.
Cross sections of the explanted grafts were made and extent of integration into the surrounding host tissue determined by visual and tactile evaluation of graft and native tissue incorporation at the surgical interface (suture line). Tissues at the suture line were examined for existing clear visual demarcation between graft and host tissue and were palpated to determine whether the graft and host tissues appeared to remain separate as they had been at implantation or if the two materials had healed into one continuous entity. Observational data were captured photographically and all gross observations recorded on explant data forms. Statistical analysis was determined to be inappropriate and was not conducted for observational data.
Biomechanical testing
Biomechanics of the healing abdominal wall were assessed at the graft–host interface. Strips of tissue (15-mm wide), inclusive of the implanted graft, two suture lines, and adjacent host tissue on each side, were tensile tested to failure as described previously, 23 with the expectation of failure at the weaker of the two suture lines. To determine host primary healing strength, a single 2-cm-long sham incision was made in the abdominal wall superior to the implant along the linea alba in the same animals receiving biologic grafts (n = 30) and closed with a continuous suture pattern prior to routine closure of the skin. Upon explant, a 15-mm-wide strip spanning the primary closure was excised and tensile tested as for the explanted grafts. Permanent sutures were removed from both the primary closures and graft–host tissue interfaces prior to tensile testing. Healing strength was analyzed using ANOVA, and Tukey's test was used for comparison among the three biomaterials and different time points.
Histological and immunohistochemical analyses
Explant sections, including the graft–host interface and graft midportion, were stained with H&E to determine extent of cellular infiltration, vascularity, and immune response. The entire area of each of two biopsies was assessed blindly from each explant at each of three magnifications (40 ×, 100 ×, and 200 ×), giving a full, representative evaluation of each biopsy collected. A thorough description of each slide was recorded. Likewise, biopsy sections were also examined for the presence of T-lymphocytes, B-lymphocytes, and macrophages to determine the extent of immune response to the material and scored as previously described. 23
Briefly, the sections were incubated with antibody to human CD3 (MCA1477; Serotec, Oxford, UK), CD20 (N1520; DakoCytomation, Copenhagen, Denmark), and CD68 (08-0125; Zymed/Invitrogen). Antigen retrieval, antibody binding, and detection were done per supplier recommendation. Cross-reactivity of anti-human antibodies with Vervet monkeys was confirmed using sections of monkey spleen as a positive control. To exclude the possibility of nonspecific binding, each section was incubated with isotype controls or secondary antibody only. Briefly, integral score values ranging from 0 to 3 were assigned to each biopsy by a blinded reviewer with 0 equal to no staining and 3 equal to most staining. For each cell type (B-cells, T-cells, and macrophages), scores were compared across material types and over time using the nonparametric Krushal–Willis test method.
Serum antibody determination
Blood samples were withdrawn from animals at 0, 7, 14, 21, 35, 49, 70, 98, 120, 150, and 180 days postimplantation, and erial dilutions of serum samples were examined for elevated antibodies (immunoglobulin G [IgG], immunoglobulin M [IgM], and anti-α-gal) to tissue antigens by ELISA, as previously described. 23
Briefly, preimplant samples were washed free of cryoprotectant and then lyophilized and micronized using a freezer mill. Micronized tissue was suspended in PBS (0.5 mg dry weight/mL), aliquots (50 μL) inoculated into Immulon 96-well polystyrene microtiter plates and allowed to air-dry overnight. Serum samples were serially diluted in 1% bovine serum albumin (BSA) and aliquots (50 μL) incubated in microtiter wells for 2 h. Plates were washed and incubated for 1 h with goat anti-human IgG conjugated to alkaline phosphatase. Reaction product was measured at 405 nm in a microwell plate spectrophotometer and absorbance values used to generate a curve. Serial dilution curves were analyzed and fold increase in antibody titer plotted versus time.
Anti-α-gal antibody titer in the serum of the implanted monkeys was assessed by ELISA using synthetic α-galactosyl epitopes coupled to BSA (α-gal-BSA) (NGP0334; V-Labs, Covington, LO) as previously described. 21
Results
In vitro graft analysis
Histology
Preimplant H&E staining of SIS (Fig. 1) revealed a condensed, diffuse collagen fiber appearance, lacking in fibrillar structure. Uniaxial orientation of collagen fibers could also be observed in SIS, due to lamination of multiple submucosa layers during the manufacturing process. In addition, cellular material and cell nuclei were observed as previously reported, 30 while the other mesh products were acellular. H&E staining revealed a structural similarity between G-PDM matrix and native porcine skin (unpublished observations), while EO-PDM biologic grafts appeared to vary between condensed and fibrillar collagen, with large, nonstaining spaces in the matrix.
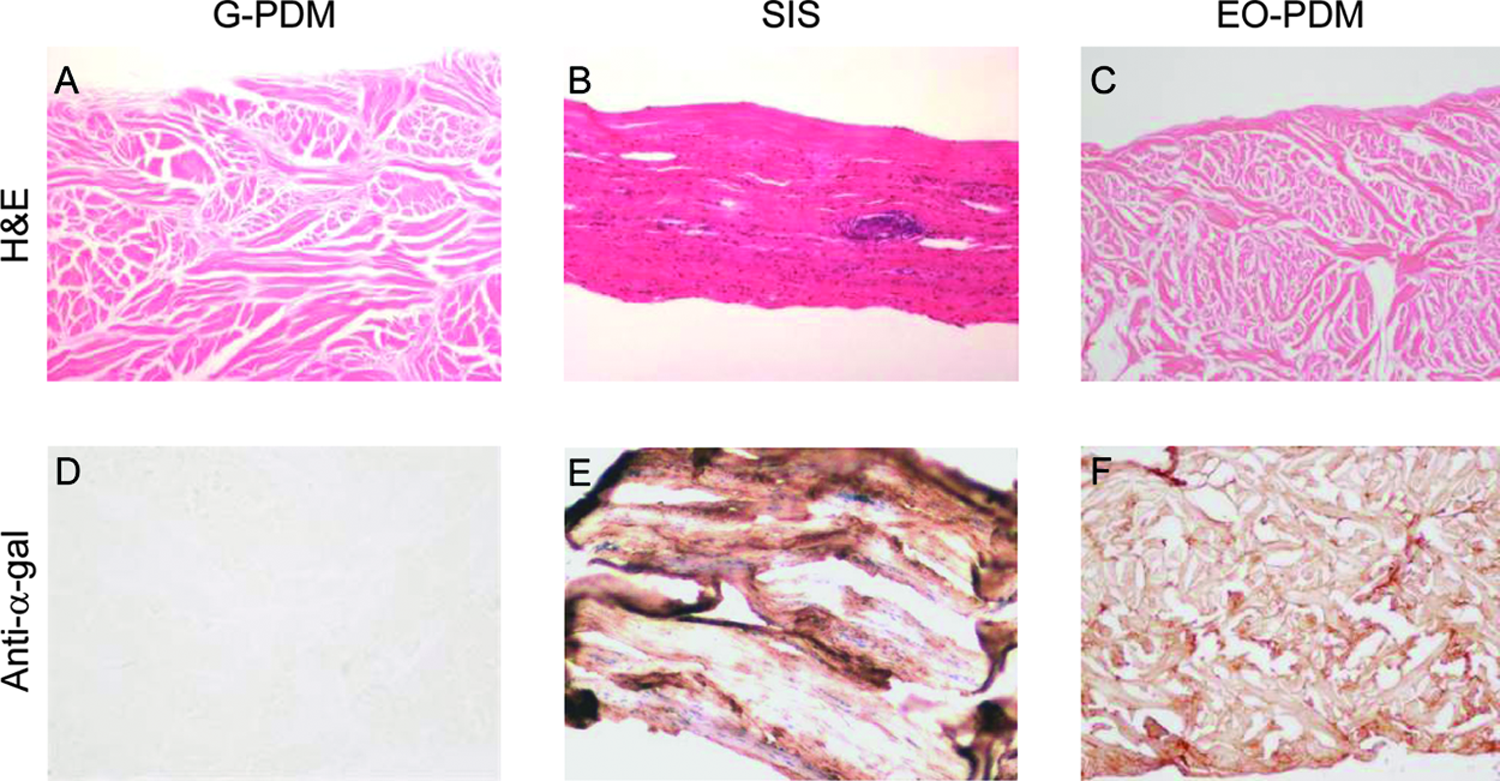
Representative histological staining of biologic graft materials prior to implant. H&E staining (100 ×): (
SIS and EO-PDM demonstrated widespread α-gal antigen staining throughout their matrices (Fig. 1), while G-PDM did not stain for α-gal.
Collagen analysis
Neither G-PDM nor EO-PDM grafts demonstrated any observable collagen bands by SDS-PAGE, while SIS demonstrated very light band intensity. Acid hydrolysis of graft collagen and spectrophotometric analysis of graft hydroxyproline content revealed >50% of graft collagen in these meshes to be pepsin insoluble (data not shown).
GAG analysis
Cellulose acetate electrophoresis revealed the presence of HA and CS in SIS, similar to native porcine skin. GAG was not able to be extracted from G-PDM or EO-PDM samples and could not be detected.
Differential scanning calorimetry
Subjecting EO-PDM samples to a linear heating program by DSC yielded a single elevated melting onset temperature (Tm) of 66.8 ± 0.7°C in comparison to that of native porcine dermal collagen (63.2 ± 0.7°C) (Table 1). SIS yielded a native collagen melting peak of 62.0 ± 0.9°C, along with two additional melting peaks (23.5 ± 2.0°C and 78.2 ± 2.9°C), comprising 32.5%, 17.4%, and 50.2% respectively, of the collagen participating in the melt. The native collagen species comprised 32.5%. Percentage of each species participating in the melt was determined by the fraction of total enthalpy contributed by the individual melting peak of that species. G-PDM yielded a single Tm of 60.1 ± 0.3, similar to that observed for native porcine collagen. However, the extent of crosslinking of this material is not evident by DSC, as the method of chemical crosslinking does not lead to collagen dehydration or consequential increase in Tm or enthalpy. 29
G-PDM and EO-PDM melted at significantly reduced enthalpy (12.1 ± 0.2 J/g and 14.5 ± 1.7 J/g, respectively) as compared to fresh unprocessed porcine skin (64.0 ± 2.6 J/g). This indicates that a significant portion of collagen matrix does not participate in the melting event and is consistent with extensive collagen degradation.
Postoperative observations
Explant graft examination revealed no defects or herniation in any animals implanted with SIS. Changes leading to physical defects occurred at the surgical sites of two animals receiving G-PDM grafts. In one animal, rupture of the host fascia adjacent to the implant–fascia interface led to evisceration of the stomach and portion of the colon from the surgical site at 53 days postoperative. Gross evaluation for this animal is included with the 3-month group in Table 2. In another animal, a tear was observed in G-PDM at explant that had not resulted in further complications. Graft failure, as defined by rupture at the graft midportion and separation into multiple pieces, was also evident for two animals receiving EO-PDM. In both EO-PDM cases, the resulting graft pieces were retained within the surgical site by significant overgrowth of host scar tissue and fibrous capsule.
Summary of in vivo graft morphology and immunology staining scores for T-cells, B-cells, and macrophages in biologic graft materials following implantation in abdominal wall resection repair model for 1, 3, and 6 months. Higher immunology staining scores correlate with greater migration of cells into the surgical site.
ANOVA-showed percent contraction data were not statistically different for SIS and EO-PDM, although contraction of both SIS and EO-PDM was statistically greater than that of G-PDM (p < 0.05). Change in graft size between 1 and 6 months was not statistically significant for any of the materials tested.
Perceived integration believed to be due to significant scar tissue.
Not determined.
Nonparametric analysis of G-PDM–implanted animals demonstrated a trend for increased macrophage presence at later time points (p < 0.05).
EO-PDM, G-PDM, and SIS grafts all showed considerable contraction as compared to implanted graft dimensions, with coincident persistent pleating, bulging, and graft hardening observed for EO-PDM and G-PDM grafts (Table 2, Fig. 2). Similar pleated morphology was observed for SIS but resolved over the 6-month implantation. SIS and EO-PDM grafts had contracted significantly more than G-PDM (p < 0.05) during the course of implantation. There was no statistically significant size difference between SIS and EO-PDM grafts. The change in graft size over the course of 1–6 months was not statistically significant for any of the materials tested.
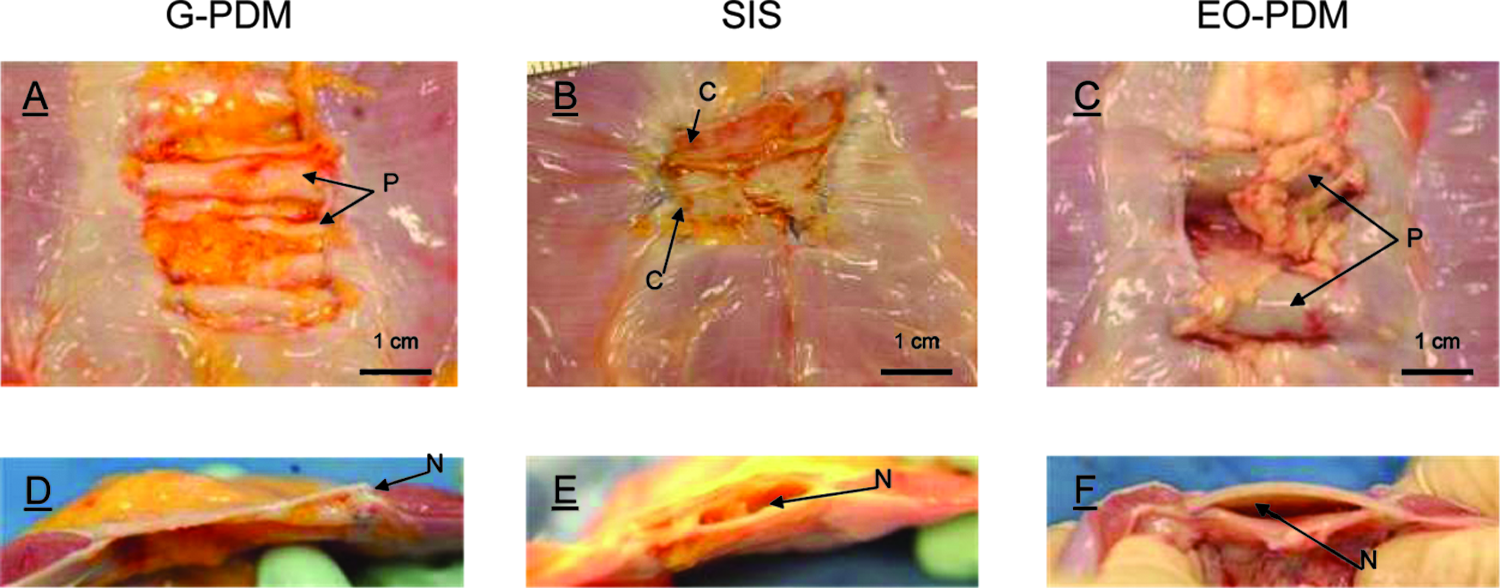
Representative graft morphology following implantation in abdominal wall resection repair model. Photos were chosen which best represented the results for the majority of animals receiving each graft type. Viscera-facing surface: (
Tissue integration was evaluated at the time of explantation by tactile palpation of the implant–native tissue interface. SIS and EO-PDM grafts were poorly incorporated into host tissue at the early time points, but appeared to become better integrated with time, possibly due to significant scar tissue formation (Table 2, Fig. 2). G-PDM grafts also displayed an initial lack of incorporation into host tissue but showed no improvement over the 6-month implant period.
Histology
No fibroblasts could be detected within the predominantly acellular G-PDM over the entire course of implant (Fig. 3). Nor was formation of blood vessels evident within the matrix at any time point. SIS was devoid of vasculature at 1 month but began to exhibit sparse vessels associated with inflammation by 3 months of implantation. EO-PDM, while predominantly acellular for the duration of the study, revealed few fibroblast-like cells and small-diameter blood vessels within the collagen fiber interstices by 1 month following implantation. These cells could not be clearly distinguished from myofibroblasts by H&E staining alone. Specific staining of serial tissue sections for von Willebrand factor to detect vascular structures was performed and confirmed results observed by H&E (data not shown).
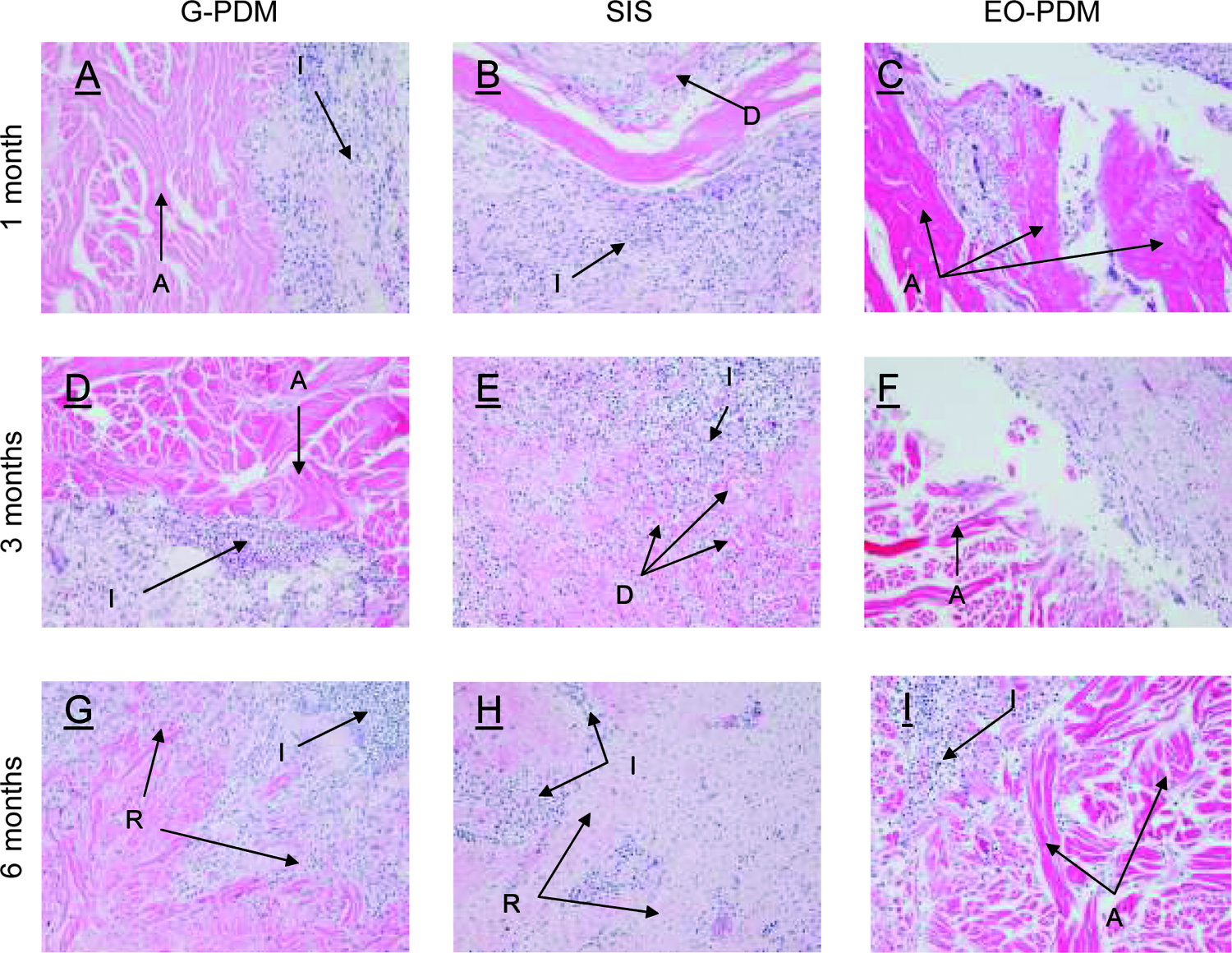
Representative histologic staining (H&E, 100 × ) of biologic graft materials following 1, 3, and 6 months of implantation in abdominal wall resection repair model. One month: (
Substantial inflammation was evident at the initial 1-month time point and persisted to the final 6-month time point for G-PDM, SIS, and EO-PDM meshes (Fig. 3). SIS appeared fully infiltrated with a mixed inflammatory response, consisting of polymorphonuclear (PMN), mononuclear cells, and foreign body giant cells. Delamination of the mesh was also apparent. A similar mix of inflammatory cells surrounded the perimeter of G-PDM and EO-PDM matrices by 3 months of implantation with no evidence of matrix penetration. By 6 months, a range of histological outcomes was observed for G-PDM, with two grafts remaining nearly acellular, one being partially penetrated by inflammatory cells, and one appearing fully engulfed by inflammatory cells with only sporadic, partially digested collagen fibers visible at the implant site. In the case of EO-PDM, few PMNs and macrophages were observed within the matrix, with a majority of the inflammatory response remaining along the graft perimeter even at 6 months of implantation.
Immunohistochemical evaluation
T-cell presence at the surgical site did not appear to increase with time for G-PDM or EO-PDM, while SIS grafts demonstrated a trend toward increased T-cell presence over the course of implantation (Table 2) and tended to have elevated inflammatory responses over the other graft materials. B-cell staining was also most prevalent in SIS for the duration of the implant study, with a trend toward an increase in B-cell presence between 1 and 3 months of implantation.
Macrophage presence was greatest for SIS at 1 and 3 months postoperative and for G-PDM at 6 months postoperative. Macrophage migration to the implant site remained relatively steady throughout the study for SIS and EO-PDM, while G-PDM–implanted animals demonstrated a trend for increased macrophage presence at later time points (p < 0.05).
Biomechanical healing strength
The healing strength of SIS (30.6 ± 5.3 N) at 1-month implantation was significantly higher (p < 0.05) than that of G-PDM (7.1 ± 2.0 N) or EO-PDM (6.5 ± 1.1 N) and reached a similar level to that of primary wound closures (24.4 ± 11.1 N) (Fig. 4). G-PDM and EO-PDM healing strengths at 1-month implantation were equivalent and considerably lower than that of primary wound healing. The 3-month and 6-month primary healing strength values (27.5 ± 12.9 N and 21.4 ± 4.9 N, respectively) were equivalent to the 1-month value, indicating that maximal healing had been reached by 1 month. No statistical difference in healing strength was observed among the biomaterials at the 3-month or 6-month time points. It was noted that healing strength values for SIS grafts continued to increase up to the 6-month time point and exhibited large variation among individual grafts (46.2 ± 26.3 N), which may indicate scarring. Healing strength data appeared to correlate with gross and histologic observations. Healing strength data for EO-PDM implanted for 6 months were not able to be collected due to test method failure.
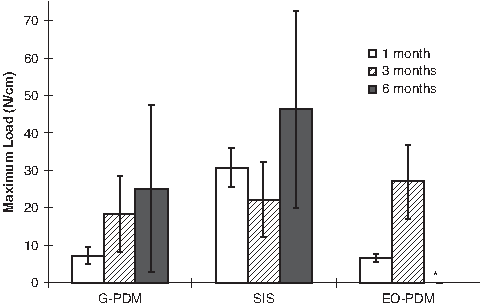
Healing strength at the graft–host tissue interface for biologic graft materials implanted for 1, 3, and 6 months. Strength is reported in Newtons/width (1 cm). White bars: 1 month of implantation; hatched bars: 3 months of implantation; black bars: 6 months of implantation. Healing strength of SIS at 1 month was significantly higher than G-PDM and EO-PDM at 1 month (p < 0.05). Asterisk (*)—no mechanical data were collected for CollaMend grafts implanted for 6 months due to test method failure.
It should be noted that healing strength measurement in this model does not take into account host tissue overgrowth on the subcutaneous surface of the grafts, which was significant for many animals in this study and may make the tensile strength of nonintegrated grafts appear artifactually high. This excess tissue was not removed from the specimens prior to testing due to the presence of scar tissue in many of the samples, a resulting difficult dissection, and the likelihood of imposing artifactual damage. Therefore, mechanical testing of the host–graft interface may be a better indicator of healing mode rather than true healing strength.
Humoral response (IgG/IgM)
A majority of SIS, G-PDM, and EO-PDM–implanted animals demonstrated significant humoral responses to the implanted material. Representative IgG titer time course data for animals surviving to 6 months are shown in Figure 5. Serum IgM was also measured for each animal and was detected at low levels (two- to fourfold) over the course of implant, independent of material (data not shown).
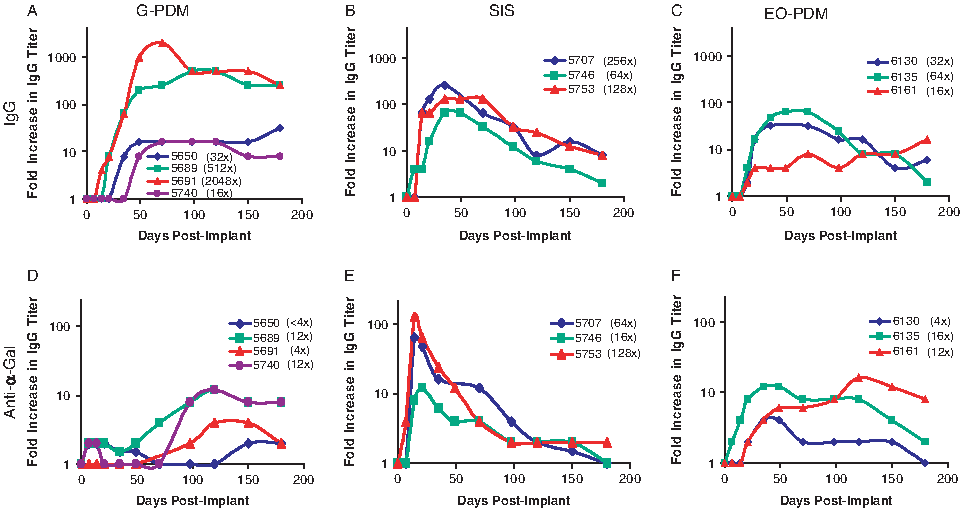
Representative fold increase in serum antibody titer over 6 months of implantation of biologic graft materials. Data are plotted as fold increase versus time on a semi-log scale and peak increase in titer for each animal is presented in parentheses. IgG response against implants: (
The majority of the G-PDM–implanted animals yielded an increase in IgG, ranging from a low 4- to 64-fold titer increase in 7 of 14 animals to a high 256- to 2048-fold titer increase in 6 of 14 animals. Of the G-PDM–implanted animals surviving to 6 months, none resolved the IgG response over the implantation time course but displayed an unresolved, sustained humoral immune response for the 6-month duration. One animal implanted with G-PDM did not yield any increase in IgG titer.
Eight of the nine animals implanted with SIS elicited a measurable immune response yielding a 32- to 256-fold increase in IgG. This humoral response to SIS peaked between 35 and 49 days postimplantation and came close to returning to baseline IgG levels during the 4- to 6-month time frame. The remaining animal implanted with SIS did not yield a significant increase in IgG titer.
All of the EO-PDM–implanted animals yielded an increase in IgG, ranging from a low 4- to 64-fold titer increase in six animals to a higher increase of up to 128-fold in the remaining three animals. This humoral response for six of the EO-PDM–implanted animals peaked between 35 and 70 days postimplantation and began to return to baseline IgG levels by 6 months. The remaining three animals displayed an unresolved, sustained humoral immune response for the 6-month duration.
Humoral response (α-gal)
Representative anti-α-gal IgG titer time course data for animals surviving to 6 months are shown in Figure 5. SIS-implanted animals demonstrated an early increase (16- to 128-fold) in anti-α-gal titer that peaked between 14 and 21 days and returned to baseline levels by 180 days postimplant.
In contrast, 6 of 14 G-PDM animals exhibited small (four- to eightfold) increases in anti-α-gal titer, while the remaining animals (8 of 14) yielded an insignificant response. Of the G-PDM animals implanted for 6 months, three out of four animals demonstrated a delayed (120 days), low-level (4- to 12-fold) increase in anti-α-gal titer that was still somewhat elevated at study conclusion.
In general, a low-level anti-α-gal response was observed for EO-PDM animals. Seven of nine animals exhibited a 2- to 16-fold increase that peaked between 14 and 120 days, while the remaining two animals demonstrated no response. The anti-α-gal response remained elevated for a majority of the animals receiving EO-PDM over the course of the experiment, indicating a sustained, though low-level response to this material. Anti-α-gal IgG titers returned close to baseline levels for two of the animals at the final 6-month time point.
Discussion
With the variety of surgical meshes commercially available, clinicians must be well informed to choose products that will provide a clinically advantageous outcome. There are numerous studies examining the biological efficacy of individual meshes,31–35 but these have been performed in various small animal models, making comparisons across studies difficult. Additionally, a recent study made direct comparisons of several biological scaffolds in a rodent model 22 whose immunology is dissimilar to the human immune system. Extrapolation of these results as predictive of the response in humans may be of limited value.
This study compares the mechanism of graft integration and functional outcome for three commercially available biologic meshes in an Old World primate abdominal wall resection repair model that is immunologically similar to humans. This model has been found appropriate for the preclinical study of biologic repair meshes as it most closely models the human biological response to implanted graft materials. 23
The meshes examined in this study, G-PDM, SIS, and EO-PDM, were assessed for in vivo functional outcomes and out-of-the-package biologic and physical properties that appear to correlate with those outcomes. Matrix properties for each mesh were evaluated through a series of structural, biochemical, and biophysical in vitro assays. This evaluation revealed that each has undergone significant matrix modification and differs considerably from native tissue possibly as a result of processing or sterilization procedures.
In vitro analysis revealed that G-PDM and EO-PDM meshes may be significantly crosslinked, a property that is believed to lead to resistance to degradation by matrix metallo-proteases (MMPs), 36 a process that is essential for subsequent cell migration, angiogenesis,37–39 and overall normal remodeling. In addition, crosslinking was not found to inhibit inflammatory or foreign body responses in vivo, in agreement with the literature. 40 Crosslinking and loss of noncollagenous proteins from these matrices were suggested by the lack of extractable native collagens and GAGs, the low enthalpy of melting, and significantly higher melting onset temperature by DSC. The lack of extractable collagens may indicate either that these graft components have undergone substantial degradation, yielding low-molecular-weight collagen, or that a majority of the collagen has undergone significant modifications, yielding pepsin-insoluble protein. Elevated melting temperatures by DSC are consistent with crosslinking of the major collagen species of the graft, while a depressed melting temperature may be indicative of collagen denaturation.
We hypothesize that extensive crosslinking of native matrix components results in tissue damage and the loss of biological signals that promote remodeling. This signaling deficiency may lead to inhibition of host fibroblast infiltration into and angiogenesis within the matrix 41 and may explain the lack of recelluarization of EO-PDM and G-PDM matrices up to 6 months in the present study as well as similar results observed in the literature.40,42,43 Lack of host cell infiltration and remodeling likely resulted in poor functional outcomes for G-PDM and EO-PDM, primarily the absence of normal healing, resulting in a lack of integration into host tissue and low healing strengths at the initial 1-month time point. In vitro mechanical failure of the entire explant, inclusive of two wound margins, generally occurred at the weaker of the two suture lines. Breaking (healing) strength at a single explant suture line was compared to healing strength of a single sham incision created within the same group of animals.
Integration and healing strength increased over time, but this is most likely due to the scar tissue observed grossly at explant, not regenerative repair. Related outcomes in the current study, and others, included severe graft pleating 40 coincident with hardening and nonincorporation into host tissue, and three individual cases of graft failure (one for G-PDM and two for EO-PDM), where grafts that did not remodel or become integrated into host tissue underwent physical graft breakdown.
Chemical crosslinking of G-PDM and EO-PDM is not only believed to lead to nonincorporation and graft failure, but also the preclusion of immune cell penetration41,43 making these grafts unable to participate in normal remodeling. Instead, immune cells rapidly encapsulated the grafts, consistent with a foreign body response. This histologic finding is consistent with the delayed antibody response observed for many G-PDM and EO-PDM grafts whose antigenic epitopes were believed to be initially masked and unavailable to elicit an immune response due to extensive crosslinking. This is particularly evident for G-PDM, where α-gal epitopes could not be detected by immunohistochemical methods in the preimplant material, possibly indicating that either the α-gal epitopes were inaccessible or α-gal–containing glycoproteins had been lost during the manufacturing process. With time, however, it is hypothesized that these epitopes became exposed through surface degradation of the mesh, resulting in a significantly increased antibody titer at later time points. EO-PDM, which elicited an IgG response more quickly than G-PDM, may be less extensively crosslinked, requiring less surface degradation for antigen exposure. In addition, EO-PDM may have greater initial exposure of α-gal epitopes than G-PDM as evident by immunohistochemical detection prior to implantation.
In vitro results suggest a different mechanism of action for SIS, whose matrix appeared degraded prior to implantation, and is believed to be responsible for significant inflammation, early resorption, and scar tissue formation in vivo. Scar tissue formation as a cause for graft contraction may be further supported by histological evaluation for myofibroblasts via α-smooth muscle cell actin staining and may be performed in future studies. In vitro assessment demonstrated minimal intact collagens and an overall low enthalpy of melting, distributed across three individual melting transitions. In addition to the normal onset of melting temperature for type I collagen, these transitions occurred at both significantly lower and significantly higher temperatures, which may indicate a mixed population of denatured and crosslinked collagens. Histologic evaluation revealed cellular material, the presence of α-gal epitopes, and multiple laminated layers of condensed collagen, suggesting modification of the matrix.
Unlike G-PDM and EO-PDM meshes, SIS is not intentionally crosslinked, and neither the antigenic cellular remnants nor the α-gal epitopes appear to be masked from the host immune system. Rather, they appear to be available and immediately recognized, eliciting an extensive immune response within the matrix by 1-month implantation that may have led to mesh resorption by 6 months. It is believed that the foreign body response may have resulted in the observed functional outcomes, including graft contraction and pleating, lack of early integration into the surrounding host tissue, and scar tissue formation that may be due to early degradation and resorption of the graft. In addition, antibody formation against SIS and α-gal, in particular, was evident by the 14-day time point, in agreement with histological observations. Alternatively, it has been reported in the literature that the inflammatory response elicited by SIS in a rat model may actually consist of macrophages of the M2 phenotype, which may promote angiogenesis and remodeling. 44
In vivo results for the modified matrices in this study are in contrast to a previous study where AlloDerm human acellular dermal matrix (HADM) (LifeCell, Branchburg, NJ) was implanted in the Old World primate abdominal wall resection repair model. 23 HADM, which is produced through a series of nondenaturing steps, has been shown previously to retain the native structural, biomechanical, and signaling properties of human dermis, maintaining the hallmarks of regenerative tissue matrix. 45 Unlike the porcine materials evaluated in this study, HADM has been shown to retain GAGs, native collagens, and the histologic structure of the native dermis from which it is derived (unpublished observations). When implanted in the abdominal wall of Old World primates, HADM rapidly became homogeneously infiltrated with vascular channels and fibroblasts and demonstrated a mixed inflammatory response consistent with normal wound healing and a minimal humoral immune response. 23 These results suggest a mechanism by which HADM meshes were able to integrate well into the surrounding host primate tissue, producing healing strengths greater than that of primary repair, without scar tissue formation. In addition, no physical graft defects, herniation, or pleating was observed.
While the products in these two studies generate a wide range of clinical outcomes and are derived from a variety of different biologic source materials, it appears that the manufacturing process for each mesh is more critical to product function than the source and species from which the tissue is procured. In fact, given the low anti-α-gal titers and unavailability of α-gal matrix epitopes in crosslinked grafts, very little of the in vivo response could be attributed to a xenogeneic reaction. Rather, poor outcomes for the xenogeneic meshes in this study are believed to be due to specific tissue processing techniques that damage the biochemical matrix components and may prevent a fully biologic repair. Preservation of these components, as observed for HADM, is believed to contribute to thorough remodeling and integration as well as overall host acceptance. 23 This point is further illustrated by the fact that the three grafts implanted in this study are each derived from porcine tissue but each demonstrated very distinct in vitro attributes and functional outcomes following implantation. The differences are believed to be due to variations in the individual tissue-processing regimens.
It should be noted that in the clinical setting, biologic implants are often selected over synthetic materials for patients at high risk of infection and with multiple comorbidities. In the above model, we studied the outcomes of biologic implants in young, healthy primates placed in a sterile environment. In the presence of bacteria, we believe that the ability of the implant to become rapidly incorporated and revascularized with minimal inflammation is even more important.
Footnotes
Acknowledgments
The authors wish to thank Dr. Wendell Sun for his invaluable expertise and assistance with statistical analysis of the data presented in this manuscript.
All animal care (boarding, implantation, sacrifice, and necropsy) was performed at Behavioral Sciences Foundation, Estridge Estate, St. Kitts, EC. Data collection and analysis following graft explantation were performed at LifeCell Corporation, One Millennium Way, Branchburg, New Jersey.