
Abstract
The objective of the current study was to determine the suitability of cell-laden and cell-free alginate–gelatin biopolymer hydrogel for osteochondral restoration in a sheep model (n = 12). Four femoral defects per animal were filled with hydrogel (cHG) plus autologous chondrocytes (cHG + C) or periosteal cells (cHG + P) or gel only (cHG) or were left untreated (E). In situ solidification enabled instantaneous implant fixation. Sixteen weeks postoperatively, defect sites were processed for light microscopy and immunofluorescence. A modified Mankin and a semi-quantitative immunoreactivity score were used to evaluate histology and immunofluorescence, respectively. Defects after cHG + C were restored with smooth, hyaline-like neo-cartilage and trabecular subchondral bone. cHG + P and cHG treatments revealed slightly inferior regenerate morphology. Undifferentiated tissue was found in E. The histological score showed significant (p < 0.05) differences between all treatment groups. In conclusion, cHG induces satisfactory defect regeneration. Complete filling of the cavity in one step and subsequent rapid in situ solidification was feasible and facilitated graft fixation. Cell implantation might be beneficial, because cells seem to play a key role in histological outcome. Still, their contribution to the repair process remains unresolved because host cell influx takes place. The combination of alginate and gelatin, however, creates an environment capable of serving implanted and host cells for osteo-chondrogenic tissue regeneration.
Introduction
Recent ACT generation had aimed to overcome these difficulties by improving cell and graft retention and environmental conditions. Cells are therefore being combined with biocompatible and biodegradable scaffolds, which can be fabricated using semi-synthetic polymers such as polylactin/polyglactin 10 or biopolymers such as collagen and hyaluronan. 9 Naturally derived materials might be preferable because of their ability to elicit biological repair responses. 1 They can function as natural substrates, cell adhesion sites, and conductive structures for tissue engineering. Their gelatinous consistency enables “anchorage independent” three-dimensional cell immobilization, which facilitates subsequent cell and tissue differentiation. 11 Ideally, they allow for complete filling of geometrically complex lesions followed by instantaneous solidification.
In this context, alginates are potentially suitable polysaccharide-based biopolymers, which can be solidified in the presence of multivalent cations. They are thoroughly characterized12,13 and have been shown to provide a chondrogenic environment for chondrocytes,14–16 bone marrow–derived mesenchymal stem cells (MSCs), 17 and periosteum.18,19 There is, however, still room for improvement in using alginates for osteochondral defect repair.20,21 Problems stem from inferior immunological properties, biomechanics, and degradation kinetics in terms of gradual softening and disintegration.17,20,22–24 Alginates are, moreover, devoid of bioactive ligands for interactions with mammalian cells. 25 A composite containing alginate alongside with a more vigorous material could theoretically improve the profile of alginates.
Gelatin is one potential candidate. The rationale lies in the fact that gelatin is a protein-based biopolymer and thus a cell adhesive of biologic origin that has inherent properties conducive to cell activity.1,26 Gelatin scaffolds have been shown to enable chondrogenic differentiation of adipose-derived stem cells 24 and bone marrow–derived MSCs in vitro. 27 When coalesced with poly(L-lactic acid), gelatin was capable of enhancing chondrocyte adhesion, proliferation, and function. 28 Variants such as thermoresponsive, poly(N-isopropylacrylamide)-grafted gelatin, 26 chitosan–gelatin hydrogels, 29 and gelatin–chondroitin sulfate–hyaluronan tri-copolymers 30 have been applied for in vitro chondrogenesis, thereby indicating that gelatin can be combined with other chondrogenically compatible materials.
Our earlier experiments demonstrated chondrogenic potential for an alginate–gelatin composite hydrogel (cHG) in an in vitro setting. 31 The present study was consequently designed to determine the suitability of cHG for cell-laden and cell-free treatment of osteochondral defects in situ. In contrast to standard ACT, chondrocytes and periosteal cells were separately implanted to obtain a sense of their individual contribution to the healing process. However, based on the experimental design, we did not intend to conclude that a particular treatment was superior. We rather hypothesized that our approach using a biopolymeric hydrogel for osteochondral restoration might generally improve common problems associated with repair techniques, namely lateral host–graft integration (scaffold-based techniques) and graft hypertrophy (first-generation ACT).
Methods
Experimental design
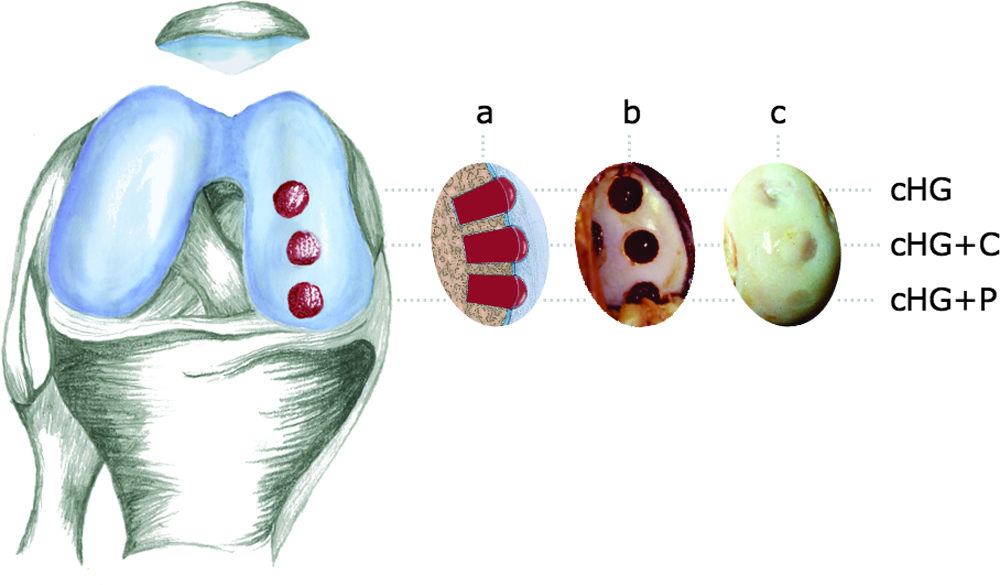
Skeletally mature house-bred merino sheep (n = 12; aged 4–6 years; weight 75–85 kg) underwent two separate knee surgeries approved by the Regierungspräsidium Freiburg, Germany (AZ 35-9185.81/1/390). One osteochondral cylinder (left knee, medial femoral condyle) each was explanted in a first surgery. These untreated defects served later as controls (E). Periosteum was harvested during the same session. Harvested cartilage and periosteum were separately processed for in vitro cell amplification. After 3 weeks, the sheep underwent a second surgery. Three osteochondral defects (right knee, medial femoral condyle) each were created to be filled with composite hydrogel (cHG), composite hydrogel plus autologous chondrocytes (cHG + C), or composite hydrogel plus periosteal cells (cHG + P) consistently from proximal to distal (Fig. 1). Defect sites and controls were analyzed 16 weeks post-treatment.
Three osteochondral defects were placed into the weight bearing area of medial femoral condyles of each of the animals' right knees. Distance between defects was consistently 5 mm to avoid communication between cavities and to assure joint stability (
First surgery and initial biopsies
Surgeries were conducted under general anesthesia and sterile conditions. Left knee joints were opened with a ventromedial arthrotomy and careful lateral subluxation of the patella. Each osteochondral cylinder was explanted with a core cutter (ø 6 mm × 12 mm depth, Aesculap, Tuttlingen, Germany) from a central weight-bearing area of the medial femoral condyle. These defects were left empty to serve as controls (E). The patella was put back in place and checked for correct patellar tracking. Joints were closed in layers. Periosteum was harvested from the medial aspect of the left tibial head during the same session. A 2-cm2 periosteal flap including cambium and fibrous layer was carefully elevated using a raspatory. Osteochondral and periosteal biopsies were stored in 0.9% sodium chloride containing 50 μg/mL of gentamicin (Gibco, Paisley, Scotland, UK) until further processing. Free range of motion was allowed postoperatively.
In vitro cell amplification
Cartilage was separated from subchondral bone. Cartilage and periosteum were separately cut into small pieces and rinsed with Ham's F-12 medium (Biochrom, Berlin, Germany). Pieces were digested in sterile 0.2% collagenase type CLS II (Biochrom) containing 50 μg/mL of gentamicin in an incubator for 15 h. Resultant cell suspensions were diluted with Ham's F-12 medium, filtered with 70-μm and 40-μm cell strainers (Falcon, Franklin Lakes, NJ), centrifuged 3 × at 1200 g and 20°C for 10 min and resuspended after each cycle. Isolated cells were seeded into 75-cm2 polystyrene cell culture flasks (Corning Corp., Corning, NY) at an initial density of 1 × 104 cells/cm2 with 10 mL Ham's F-12 medium, 10% heat-inactivated fetal calf serum, 1% penicillin/streptomycin, and 1% minimum essential medium vitamins (Biochrom, changed every third day) and cultured at 37°C, 5% carbon dioxide, and 100% humidity. Cultures were regularly examined under a microscope (Axiovert 25, Zeiss, Oberkochen, Germany) for growth characteristics. At confluence, cells were enzymatically detached with 0.25% trypsin–ethylenediaminetetraacetic acid solution (Sigma, St. Louis, MO). Their viability was tested using the trypan blue exclusion test. Cells were reseeded as described above. Required numbers of chondrocytes and periosteal cells (>4 × 106 cells/animal each, passage 3) were obtained after 3 weeks. Generally, no cell pooling occurred to truly ensure autologous cell implantation into the original host.
Biopolymer composite hydrogel
Hydrogel consisted of 5% (w/v) low-viscosity sodium alginic acid (Fluka, Buchs, Switzerland), 5% type I collagen–based pharma gelatin type B (Merck, Darmstadt, Germany), and 0.2% 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid buffer in distilled water. All components were sterilized separately and stirred together for 12 h at 30°C. Physiological pH value was achieved by buffering (0.1 M sodium hydroxide). Reconstituted hydrogel was stored at 3°C.
Second surgery
Surgeries, anesthesia, and postoperative management were carried out under identical conditions to those described for the first surgeries. Three osteochondral defects each were placed into the weight-bearing area of the medial femoral condyle of the right knee (Fig. 1). The distance between the defects was consistently 5 mm to avoid communication between cavities and to assure joint stability (Fig. 1a). No articulation of the proximal defect with the patella was observed in hyperflexion of the knees. Meanwhile, hydrogel was warmed to 30°C. Three different gel injections were prepared in 1-mL syringes containing 8 × 106 chondrocytes or periosteal cells/mL or cell-free cHG. Osteochondral defects were completely filled with cHG, cHG + C, and cHG + P consistently from proximal to distal (Fig. 1b). For instantaneous gel solidification (cross-linking of alginic acid chains), joints were rinsed with 102 mM calcium chloride solution for 5 min, followed by lavage with 0.9% sodium chloride. No implant shrinkage was observed before joint closure. Free range of motion was allowed postoperatively.
Final biopsies
Sixteen weeks after hydrogel injections (19 weeks after E), animals were sacrificed using intravenous barbiturate (100 mg/kg Trapanal; Byk Gulden, Konstanz, Germany) and potassium (2 mM/kg, 7.45% potassium chloride; Braun, Melsungen, Germany). Both knee joints were exposed and inspected macroscopically (Fig. 1c). Full-depth cores were harvested from treated sites, E, and native articular cartilage (AC; contralateral to treated defects) using a surgical saw. Cores were cut into halves. One half was stored in 4% formaldehyde for 5 days at 3°C for standard histology; the other was separated from subchondral bone and stored in Ham's F-12 medium at 3°C for immunofluorescence.
Histology and light microscopy
Fixed specimens were processed in graded ethanol, xylol, and paraffin. Decalcified sections 3 μm thick were cut with a RM 2165 (Leica, Bensheim, Germany) and stained with routine Saf-O protocols. For digital microphotography, SMZ 800 and Eclipse E 400 microscopes (both Nikon, Düsseldorf, Germany) were used with 2.5×, 10×, and 20× objectives.
Immunofluorescence
Unfixed neo-cartilage was processed in 5%, 10%, and 15% sucrose (Merck) for 30 min each and in tissue-freezing medium (Tissue-Tek; Leica) for 90 min at room temperature to prevent crystal formation, embedded in fresh freezing medium, and flash frozen over liquid nitrogen. Unfixed cryosections 20 μm thick were cut on a cryotome (CM 3000; Leica) at −19°C. Sections were preincubated with 1% bovine serum albumin (BSA) for 60 min in a humidified chamber at room temperature. Sections were then incubated with rabbit anti-bovine collagen type I (COL1) and type II (COL2) polyclonal (1:50, AB 749 P, AB 746 P) and adult mouse anti-human cartilage proteoglycan (PG) monoclonal (1:400, MAB 2015; all Chemicon, Hofheim, Germany) primary antibodies and subsequently with Cy3-conjugated goat anti-rabbit and goat anti-mouse (1:200; Dianova, Hamburg, Germany) secondary antibodies under identical conditions. Cell nuclei were stained with bisBenzimide (Sigma) for 1 min. Antibodies and DNA dyes were diluted in 1% BSA. Slides were rinsed with 1x PBS between each of the incubation steps. Slides were embedded with Mowiol (Hoechst, Frankfurt, Germany) under coverslips. No primary and no secondary antibody controls were performed. We relied on the same immunohistochemical protocol as for our previously described sheep model. 32 In addition, we expected no cross-reactivity of applied anti-COL1 antibodies with gelatin based on our previous in vitro study on the identical hydrogel; 31 no COL1 immunoreactivity of the primary hydrogel matrix could be detected after 2 weeks and later on. Specimens were examined using an epifluorescence photomicroscope Axioskop (Zeiss) equipped with a filter unit BP 510–560/FT 580/LP 590 for red fluorescence (Cy3) and ultarviolet excitation for bisBenzimide (blue) visualization. PlanNeofluar 10× and 40× objectives were used for microphotography.
Evaluation and statistics
Two blinded observers analyzed Saf-O histology of different regenerates and AC using a modified 19-point Mankin score, 33 including surface shape and structure, bonding, cartilage morphology, bone regeneration, and defect filling.
Randomly chosen cryosections of each animal were used to semiquantify immunofluorescence signal intensities of COL2, COL1, and PG in different neo-cartilages and AC. Three blinded observers assessed discrete (1), increased (2), intensive (3), and no (0) signal intensities. Cell densities (bisBenzimide-positive cells) were acquired from optical fields (340 × 230 × 5 μm) at 400 magnification applied on four different randomly chosen sections per animal. Both analyses were stratified into intermediate and deep zones.
Single-factor analysis of variance (ANOVA), Friedman-test (two-way ANOVA), and Wilcoxon's matched-pair, signed-rank test were performed where applicable. Data are presented as means ± standard deviations. Level of significance was set at p < 0.05 unless otherwise specified.
Results
Postoperative period
Free range of motion was allowed postoperatively. The individual recovery pattern was as follows. Animals were observed to have minimal weight bearing on their operated limbs in the first postoperative week but increased their knee range of motion and weight bearing gradually thereafter. No postoperative complications or infections were observed. This postoperative recovery pattern was similar for both surgeries.
Monolayer cell amplification
Chondrocytes and periosteal cells attached to polystyrene culture flasks within 24 h while developing a fibroblast-like phenotype. Both cultures revealed similar gross morphology and growth characteristics. After 3 weeks, initial cell numbers (mean) had increased 3.63 times for chondrocytes and 5.13 times for periosteal cells. Viability of more than 90% (trypan exclusion test) was determined for both cell lines.
Macroscopic appearance
Explored joints revealed no macroscopic graft-related signs of synovitis or inflammation. Treated defect sites and empty control sites could be clearly identified. Defects after cHG, cHG + C, and cHG + P were smoothly resurfaced with well-bonded neo-tissue and were primarily level with adjacent cartilage or slightly indented (Fig. 1c). There was no evidence of hydrogel remnants within the joint cavities. Untreated controls were incompletely filled with fragmented tissue (not shown). Macroscopically, surrounding cartilage in the different sites had no evident degenerative changes.
Morphology and histological score
Defects treated with cHG + C had neo-tissue growth up to the level of the surrounding cartilage, with tight bonding to adjacent tissue (Fig. 2a and 3a). The surface was smooth, and curvature was regained. Neo-cartilage was of hyaline-like morphology (Fig. 3b). Flat cells parallel to the surface were found in the superficial zone, with bigger cells partially arranged in cell columns in deeper zones. The osseous defect was restored with trabecular bone (Fig. 2a). Defects treated with cHG + P appeared to be smooth but slightly concave (Fig. 2b). Neo-cartilage was of variable thickness and of hyaline-like morphology partially. Cells were predominantly arranged in small cell clusters. Trabecular bone regeneration was incomplete. Cyst formation occurred in one animal. Incomplete, indented defect filling was found in the cHG treatment group. Neo-cartilage, which was covered with a fibrous layer, contained islands of hyaline-like characteristics (Fig. 2c). Cells were homogenously distributed, with no evident cell clusters. The osseous defect was restored with dense and partially trabecular bone. Bonding of neo-tissue after cHG + P and cHG treatment was firm. Saf-O intensity of neo-tissue after hydrogel treatments appeared similar to surrounding native tissue. Empty controls were irregularly restored (incomplete and excessive filling above the surface level), with undifferentiated osseous and fibrous tissue (Fig. 2d).

Representative Saf-O histology of regenerates in differently treated defects. (
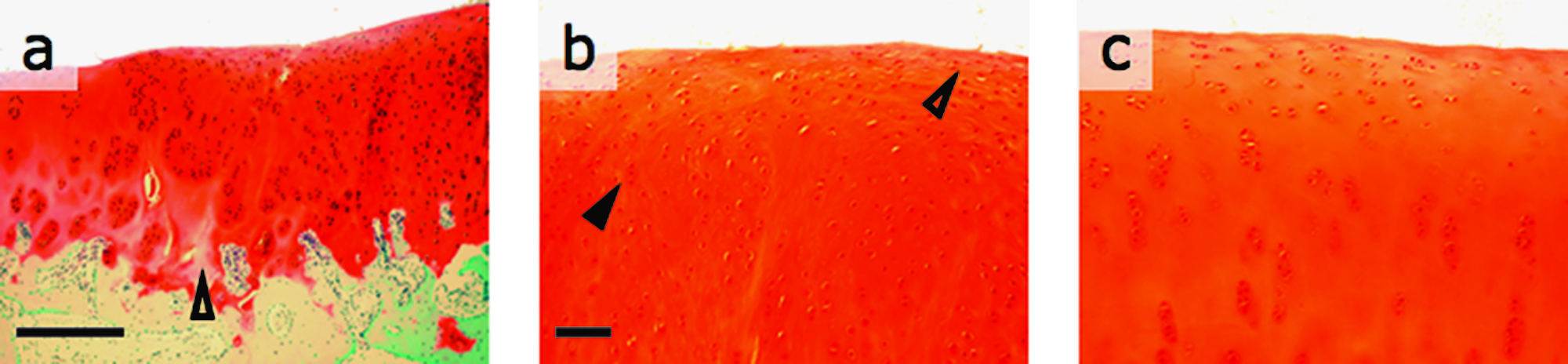
Saf-O histology of regenerates in defects after a cHG + C treatment (
The histological score revealed overall significant differences between all treatment groups and E (Fig. 4). Highest scores were determined for cHG + C treatments, followed by cHG + P and cHG, lowest for E. This grading was also observed when stratified into different score criteria (not shown), which was significant for E.
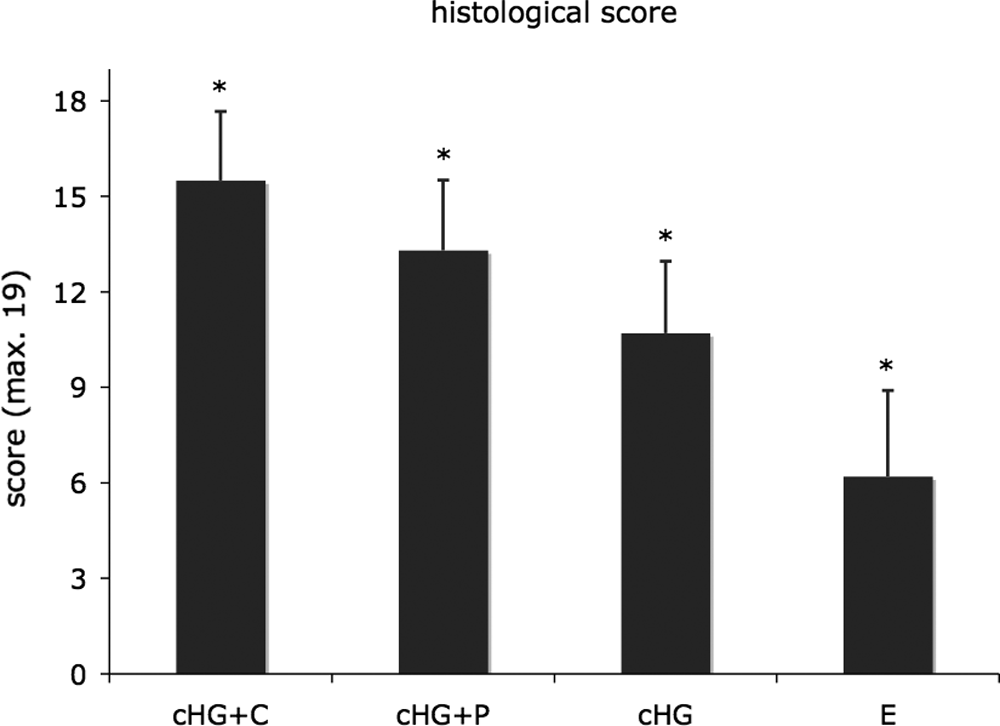
Histological evaluation of regenerates in differently treated defects using a modified Mankin score (maximum 19; overall means, standard deviation error bars). Significant differences (*p < 0.05) were found between all four regenerates.
Immunoreactivity and cell density
Signal intensities of COL2, COL1, and PG in neo-cartilage after cHG + C and cHG + P treatment resembled AC pattern, with high COL2 and PG and low COL1 yields found (Fig. 5). Even results for all matrix components could be observed after cHG treatment. Differences between cHG + C, cHG + P, and cHG were not significant. In contrast, regenerates in E showed significantly higher COL1 (p < 0.005) and lower COL2 (p < 0.001) intensities than AC. Generally, no significant differences in PG intensities could be found between the intermediate and deep zones of different neo-cartilages (not shown).

Semi-quantitative assessment of immunofluorescence signal intensities (overall means, standard deviation error bars) for type II collagen (COL2), type I collagen (COL1), and proteoglycan (PG) in neo-cartilages and native articular cartilage (AC). Intensities after cHG + C and cHG + P treatments resembled AC pattern. In untreated defects, intensities for COL2 were significantly lower (*p < 0.001) and for COL1 significantly higher (**p < 0.005) than AC. For PG intensities, neither significant differences between the four different regenerates nor between cHG + C and AC were found.
Mean cell numbers similar to those in AC were counted in neo-cartilage after cHG + P and cHG treatments (Fig. 6). Significantly lower numbers were found after cHG + C treatment and significantly higher numbers in E. Identical patterns could be seen when stratified into intermediate and deep zones. Neo-cartilage after cHG + C, cHG + P, and cHG treatments and AC contained significantly higher cell numbers in the intermediate zone than in the deep zone. This was not evident for E.
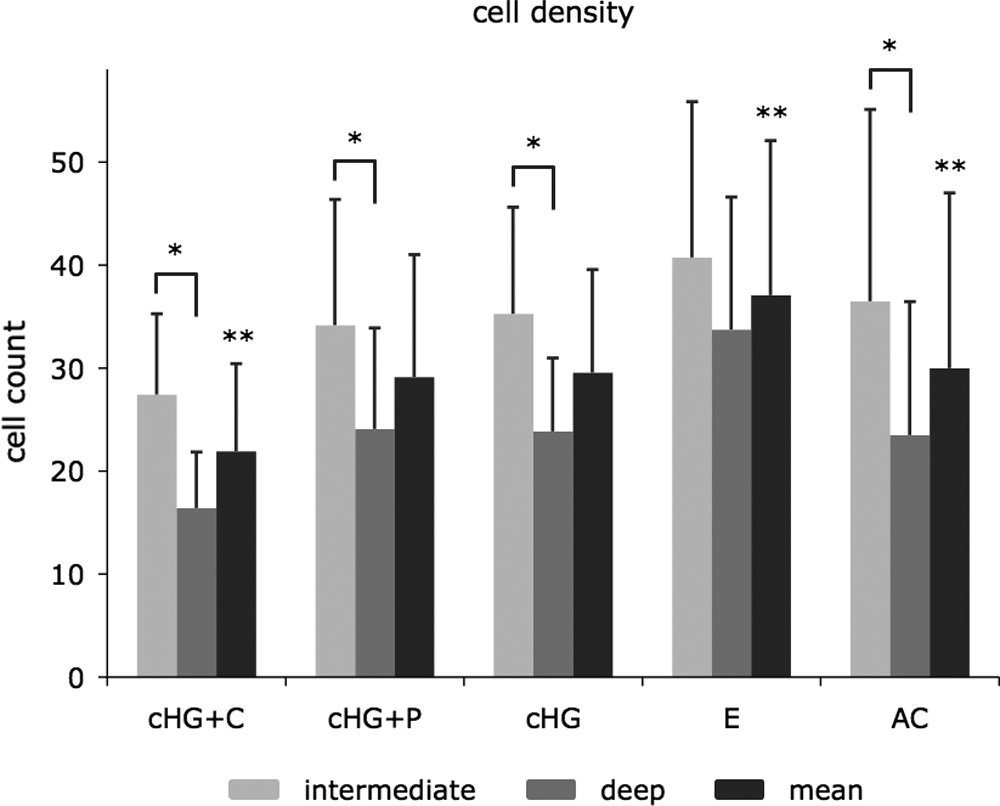
Zonal and overall cell numbers (overall means, standard deviation error bars). Note similar overall numbers as native articular cartilage (AC) in neo-cartilages after cHG + P and cHG treatments. Significantly lower numbers were detected for cHG + C than for AC and significantly higher numbers for untreated defects (**p < 0.05). Neo-cartilage after cHG + C, cHG + P and cHG, and AC contained significantly higher cell numbers in intermediate than in deep zones (*p < 0.05). This was not evident in untreated defects.
Discussion
To the best of our knowledge, this is the first description of an alginate–gelatin biopolymer hydrogel for cell-based treatment of osteochondral defects. The concept of injectable cell delivery via cHG was technically feasible, and it is conceivable that it might be performed arthroscopically. Filling of the entire lesion in one step and subsequent instantaneous in situ solidification made graft implantation easier than with ACT, which requires additional grafting for deeper lesions. 5 No graft hypertrophy was observed in any treatment group, and cyst formation was found in only one cHG + P treatment. Absence of synovitis or inflammatory infiltrations indicated good biocompatibility. Moreover, we observed no fissures, fragmentation, or bulk indentations, suggesting adequate durability and degradation kinetics of the implant. 31 This was unexpected, because gels are known to be poorly capable of withstanding biomechanical forces.11,12,34 The composition of the applied gel is likely to contribute to satisfactory mechanical resistance because gelatin allows for cell–graft interactions, which can result in cell-mediated packing and contraction.24,27
At harvest, red (Saf-O) stain for gel residues was scarcely detectable in former osseous defects, and the red (Saf-O) intensity of neo-cartilage after cHG containing treatments appeared similar to surrounding AC. Although being aware of cross-reactivity between Saf-O and potentially remaining alginates, we concluded that the implant was mainly replaced by neo-tissue, as previously described for pure alginates.22,35 High PG immunoreactivity supported this conclusion. Defect sites treated with cell-laden or cell-free cHG were thus restored with well-integrated neo-cartilage of partly hyaline-like characteristics and trabecular bone. As discussed in our previous ACT study, mature neo-cartilage seems to have cellularity that is lower than or similar to that of AC, 32 whereas fibrocartilage was associated with higher yield. Cellularities of the current study support these findings. We counted similar cell numbers after cHG + P and cHG treatments, and in AC, and lower after cHG + C treatments. However, similar histology was described for a rabbit model using chondrocytes in pure alginate suspension, 20 yet fibrocartilaginous repair tissue was found after cell-free treatment. This contradicts our findings that cell-free cHG promoted zonal cell distribution and sporadically hyaline-like islands. One reason could be that bioactive gelatin might have provided cHG with better chondrogenic properties than sole alginate.
Cellularity in cell-free cHG indicates, moreover, that host cells that probably came from the bone marrow, because a fresh bleeding osteochondral defect was created, invaded the gel. This has also been described to occur in other alginate models,17,20,21 which is worth discussing because the implanted cells' contribution to the repair process is generally being questioned. Select studies showed that 8% to 33%36,37 of the repair tissue's cell population arose from the implant itself. Mierisch et al. treated lesions with labeled chondrocytes in alginate beads and found them neither to form repair tissue nor to migrate into the adjacent host. 21 Breinan et al. corroborated these results. 38 Thus, literature supports a role for bone marrow–derived stem cells being prime contributors to tissue regeneration, also because of their ability to form cartilage and bone. Our study was not intended to determine whether it was redundant to implant cells because cell labeling was not performed. Moreover, the experimental design does not allow for conclusions regarding the different cell types' individual contribution. Nonetheless, the histological score revealed significant differences between cell-laden and cell-free cHG treatments and even between cHG + C and cHG + P. This suggests that certain cell types—in our case chondrocytes might be favorable for defect regeneration, although this could also be due to varying biomechanical effect on the differently located but consistently treated defects and their potential effect on each other. In a broader sense, the defect sites' different environmental conditions have to be seen as critical. However, we may still presume that the initial presence of implanted cells makes a difference, which select studies support; Diduch et al. embedded marrow stromal cells in alginate beads for osteochondral restoration and found lower proteoglycan yield in cell-free treatment controls. 17 Brittberg et al. postulated that chondrocytes are decisive for chondrocyte-augmented periosteal grafting compared with periosteum alone. 39 Besides, our cHG + C treatment promoted greater trabecular bone regeneration than cHG + P or cHG, although periosteal cells and MSCs are known to exhibited osteo-chondrogenic potential.4,40–43 Mechanical impact alone cannot explain these findings. They correspond to the work published by Tallheden et al. that articular cartilage seems to contain a cell population of phenotypic plasticity, which is comparable with that of MSCs when kept under appropriate conditions. 44 In fact, our biopolymer seemed to provide environmental conditions, which allow the implanted and invaded cells for differentiated neo-tissue formation. The underlying regulative factors and multifactorial processes1,39 remain yet unresolved.
In conclusion, the repair tissue's true origin, the role and fate of the implanted cells remain unanswered. However, we successfully demonstrated the principle of osteochondral restoration using an injectable alginate–gelatin hydrogel. The composite created a propitious environment for differentiated tissue formation. Lateral graft bonding was excellent, and graft hypertrophy was prevented. We believe that cell implantation is beneficial, and host cell influx must also be taken into account. Treatment randomization and cell labeling should be performed in the future, together with biomechanical tests, for valid graft and neo-tissue characterization. An additional cHG + C + P group would further increase the power of this study.
Footnotes
Acknowledgments
We are grateful to Dr. R. Landers (Institute of Macromolecular Chemistry) for contributions in biomaterial development; G. Menzel, E. Gimbel, and F. Moos for excellent technical assistance; Prof. Dr. J. Haberstroh and Dr. B. Eissner for animal care and anesthesia; Prof. Dr. J. Schulte-Mönting for statistical advice; and Prof. Dr. E. Schäfer for using core facilities at the Institute of Pathology (all University of Freiburg, Germany). We thank R. Rademacher (![]() ) for artwork contributions.
) for artwork contributions.
This article was previously published as an abstract as follows: ICRS & ETES/TESI 04.
This work was conducted at the University Hospital of Freiburg, Germany.