
Abstract
Delayed or absence of vascularization is one of the major reasons for skin engraftment failure in patients with extensive burns. For such trauma victims, the best alternative to a split-thickness graft would be wound coverage with an autologous in vitro reconstructed skin (RS) combining dermis and epidermis with an appropriate microvascularization. We have developed an endothelialized RS based on our self-assembly approach, which is generated from autologous cultured cells without any exogenous angiogenic growth factor or scaffold. After transplantation in athymic mice, an early inosculation between the graft and host vasculatures occurred within 4 days. We also concurrently detected an active invasion of the dermis by host capillaries sprouting from the wound bed. Thus, the microvascular network constructed in vitro within our three-dimensional skin substitute did not only develop functional anastomoses with the host's blood vessels but also promoted a rapid, complete, and optimal vascularization of the implanted tissues by exerting an angiogenic effect compared with control RS. Our model may bring about interesting possibilities for regenerative medicine by leading to faster vascularization in clinical applications. In addition, the endothelialized RS can be a useful in vitro angiogenesis model.
Introduction
When the dermal layer has been destroyed, the application of an epidermal substitute is not enough to ensure optimal healing. In such a case, the development of a bilayered substitute of adequate thickness is preferred. The epidermal layer is essential to restore control of fluid loss, body temperature, and protection against bacteria, whereas the dermal layer gives the skin its elasticity and strength. Currently, numerous products are commercially available for wound treatment. Some of them are tissue-engineered products, with or without living cells. 1 An important limitation during treatment with large three-dimensional (3D) skin substitutes for extensive permanent wound coverage is whether they will rapidly become vascularized, thus preventing necrosis and the ensuing loss of the protective epithelial barrier. Indeed, cells require oxygen and nutrients for their survival and are, therefore, located within 100–200 μm of blood vessels, which is the diffusion limit for oxygen. 2 Long-term survival and function of such 3D substitutes depend on rapid development of new blood vessels that will provide nutrients and oxygen to the cells, not only at the margin but also in the center of the tissue grafts.
Thus, premicrovascularization of skin substitutes will significantly enhance the efficacy and quality of wound healing. Different approaches are currently used to improve vascularization of skin substitutes before or after transplantation.3–6 The use of growth factors via absorption or incorporation into natural or synthetic scaffolds triggers their localized and sustained delivery and, thus, promotes vascularization (for review see ref. 7 ). A sustained release of vascular endothelial growth factor was observed for over 70 days from copolymers of lactic and glycolic acid sponges. 8 Basic fibroblast growth factor enhances the vascularization into a poly(vinyl alcohol) porous sponge 9 or in porous alginate scaffolds. 10 Transplanted cells can also be genetically modified to produce angiogenic proteins that promote better and faster vascularization. For example, Boyce and coworkers, built skin substitutes with keratinocytes that were genetically modified to overexpress platelet-derived growth factor 11 or vascular endothelial growth factor.12–14 Another approach is to modify endothelial cells with a caspase-resistant Bcl-2 protein to enhance their survival.15,16 Although angiogenic growth factor release seems safer and more clinically applicable than the use of genetically modified cells, tissue constructs that comprise synthetic or xenogenic components are liable to initiate adverse immune reaction.
Experimental results previously published by our laboratory indicate that endothelial cells can spontaneously assemble into capillary-like structures (CLS) and microvascular networks when cocultured with fibroblasts in skin substitutes produced in vitro with biological biomaterials. 17 We have also shown that after grafting such substitutes on nude mice, this network will inosculate with the host's own vascular system within 4 days instead of the 14 days needed for complete vascularization with nonvascularized skin substitutes. 18 In this study, we present a new model of endothelialized reconstructed skin (ERS) in which the angiogenic process takes place without the addition of any exogenous modulator-like growth factors, except those present in the commercially available culture media we used and without any exogenous scaffold. We describe here the in vivo remodeling of a tissue-engineered microvascular network within a human skin substitute, which was grown in vitro and transplanted onto nude mice.
Materials and Methods
Human cell isolation
Human keratinocytes and fibroblasts were isolated from human skin biopsies after breast reductive surgeries, as previously described.19,20 Human microvascular endothelial cells (HMVECs) were purified from the foreskin of a healthy baby using Dynabeads CD31 (Dynal Biotech); human umbilical vein endothelial cells (HUVECs) were obtained from the umbilical cord of healthy newborns by enzymatic digestion, as previously described. 21 These two types of endothelial cells were transduced by lentiviral vectors to provide stable luciferase and green fluorescent protein (GFP) expression.22,23 Transductions were graciously performed in Dr. J.A. Medin's laboratory (Ontario Cancer Institute, Toronto, Canada).
Reconstructed skin and ERS preparation
The self-assembly approach.24,25 was used to produce two different tissues: the control, RS and the ERS. Schematically, the dermal layer of the tissue-engineered skin was composed of three sheets of fibroblasts. The two inferior sheets were plated with or without HUVECs, whereas a superior third sheet was seeded with keratinocytes to provide the epidermal layer. Fibroblasts were seeded at a concentration of 15,000 cells/cm2 in the presence of a paper anchor and grown for 3 weeks in Dulbecco-Vogt modification of Eagle's medium (DMEM; Invitrogen) supplemented with 10% fetal calf serum (HyClone), 100 U/mL penicillin (Sigma-Aldrich), 25 μg/mL gentamicin (Schering), and 50 μg/mL of ascorbic acid (Sigma) in 8% CO2 and at 37°C. After 21 days, HUVECs or HMVECs were plated on two sheets of the ERS at a concentration of 12,000 cells/cm2. Both were cultured for 7 days in a medium of 1:1 ratio of endothelial growth medium-2 (EGM-2) medium (Cambrex Bio Science Baltimore, Inc.) and DMEM supplemented with 10% fetal calf serum and 50 μg/mL of ascorbic acid. Concomitantly, on day 21, keratinocytes were plated on the last sheet at a concentration of 50,000 cells/cm2 and grown in a 3:1 DMEM-Ham's F-12 medium (Invitrogen) supplemented with 5% newborn calf serum (FetalCLone II; HyClone), 0.4 μg/mL hydrocortisone (Calbiochem), 5 μg/mL bovine insulin (Sigma), 10 ng/mL human epidermal growth factor (Austral), 10−10 M cholera toxin (ICN), and 50 μg/mL ascorbic acid and antibiotics. Then, on day 28, cell sheets were stacked, attached with ligating clips (Ethicon Endo-Surgery), and tissues were elevated to the air-liquid interface for 2 weeks in media described above, without epidermal growth factor. Media were changed thrice a week.
Animal and surgical manipulations
All animal procedures were performed using protocols approved by the Canadian Council on Animal Care. To prevent infections, adult male athymic nu/nu mice (42-day old) (Charles River Laboratories) were injected with ceftazidime (3 mg/mouse, Glaxo, Toronto, Canada) 24 h before surgery, during the surgery, and 24 h after surgery. Animals were anesthetized by inhalation of 3% Isoflurane United States Pharmacopeia (USP) (Schein Pharmaceutical). Graft sites on the backs of adult male athymic nu/nu mice were prepared by first removing a 2 cm2 piece of mouse skin and underlying panniculus carnosus. A silicone Fusenig's chamber was then sutured into the defect. 26 Tissue-engineered skins were directly deposited on the mouse dorsal muscle. A cap was used to close the chamber for 2 weeks after grafting. Three animals were used for each group (RS or ERS) and each timepoint. Mice were euthanized and grafts were harvested for analysis at 2, 4, 7, 14, and 30 days posttransplantation. At the time of implant retrieval, no signs of infection were detected and inflammation was minimal.
Histological analysis
To conserve GFP inside human endothelial cells, sections of each graft were fixed in 3.7% formol at room temperature for 2 h, then placed in phosphate-buffered saline (PBS) 10% sucrose at 4°C, and finally overnight in PBS 30% sucrose at 4°C, as previously described. 27 Biopsies were then paraffin embedded for staining with Masson's trichrome.
Immunohistochemical analysis
A section of each biopsy, fixed as previously described, was embedded in optimal cutting temperature (OCT) compound (Somengen) and stored at −80°C. Immunohistochemical analysis of harvested tissue was realized on frozen 5 or 25 μm sections permeabilized in 100% acetone at −20°C. Primary antibodies reactive with mouse CD31 (1/800; BD Pharmingen), human CD31 (1/800; Chemicon), mouse red blood cells (1/800; Cedarlane), laminin (1/100; Abcam), or collagen VII (1/200; Chemicon) were used for characterization of vascular and basal membranes profiles. An Alexa-594 or -488 secondary antibody (1/800; Molecular Probes), mixed with Hoechst 33258 (1/100) (Sigma) to stain the cell nuclei, was used to detect the primary antibody. Control incubations (replacement of primary antibody with PBS bovine serum albumin 1%) were performed. All controls were negative. Sections were examined using a Nikon Eclipse E600 fluorescence microscope (Nikon) or a Nikon C1 laser scanning confocal microscope (Nikon).
Murine endothelial cell neovascularization evaluation
Murine vascular profiles in the dermal compartment of the skin substitutes were characterized by positive staining with mouse CD31. A total of three biopsies per condition were taken on days 2, 4, and 7. Two samples, with the mean of two slides per sample, were analyzed for each triplicate of each group. The grafted dermis' height colonized by murine endothelial cell was measured using Adobe Photoshop CS3 software (Adobe Systems) on digital microphotographs taken in three random high-power fields.
Human endothelial cell density quantification
RS and ERS samples were weighed, snap frozen, and stored at −80°C until use. A 20% homogenate (weight/volume) was prepared using a polytron probe (Qiagen, Mississauga, ON, Canada) in 4°C cell lysis buffer containing 250 mM Tris (BioRad) with 0.5% triton X-100 (BioRad) and protease inhibitors (Roche). After three snap freeze thaw cycles, samples were centrifuged at 13,000 g, and 20 μL of cleared cell lysate was assayed in triplicate along with a standard curve of firefly luciferase enzyme (Sigma). An Orion II microplate luminometer (Berthold Detection Systems) injected 100 μL of D-luciferin substrate (Promega) with each sample, and luminescence was captured over 10 s. Data are expressed as relative light units and show quantitative levels of luciferase activity, which correlate to the human endothelial cell density in each skin equivalent.
Statistical analysis
Differences between values were assessed by bilateral Student's t-test. All data were expressed as mean ± standard deviation, and overall statistical significance was set at p < 0.05. Statistics and graphics were performed using Microsoft Office Excel 2007 software (Microsoft Corporation).
Results
ERS characterization
Transplanted RS (without anchorage) had a surface of 2.68 cm2 (Fig. 1A) and a thickness of approximately 300 μm, with an avascular epidermis of 100 μm (Fig. 1B). After 4 weeks of culture in vitro, the RS exhibited a homogeneous, well-developed, stratified, and cornified human epidermis (Fig. 1B). The basement membrane components (collagen VII and laminin) were detected at the dermal-epidermal junction, showing a continuous line after maturation in vitro (Fig. 1C, D). In our model, human endothelial cells spontaneously formed CLS, as previously described.17,28 These can be observed in transverse sections of ERS stained with Masson's trichrome (Fig. 1B) and are associated with the expression of basement membrane components such as laminin (Fig. 1D) and collagen IV (data not shown), visualized by immunofluorescence analysis. Lumens are well defined in transverse sections of the ERS (Fig. 1D). Reconstructed skin endothelialized with either HUVEC-GFP+ or HMVEC-GFP+ both showed the organization of CLS into a complex microvascular network with a branching morphology that seems to be more ramified with microvascular endothelial cells (Fig. 1E, F).
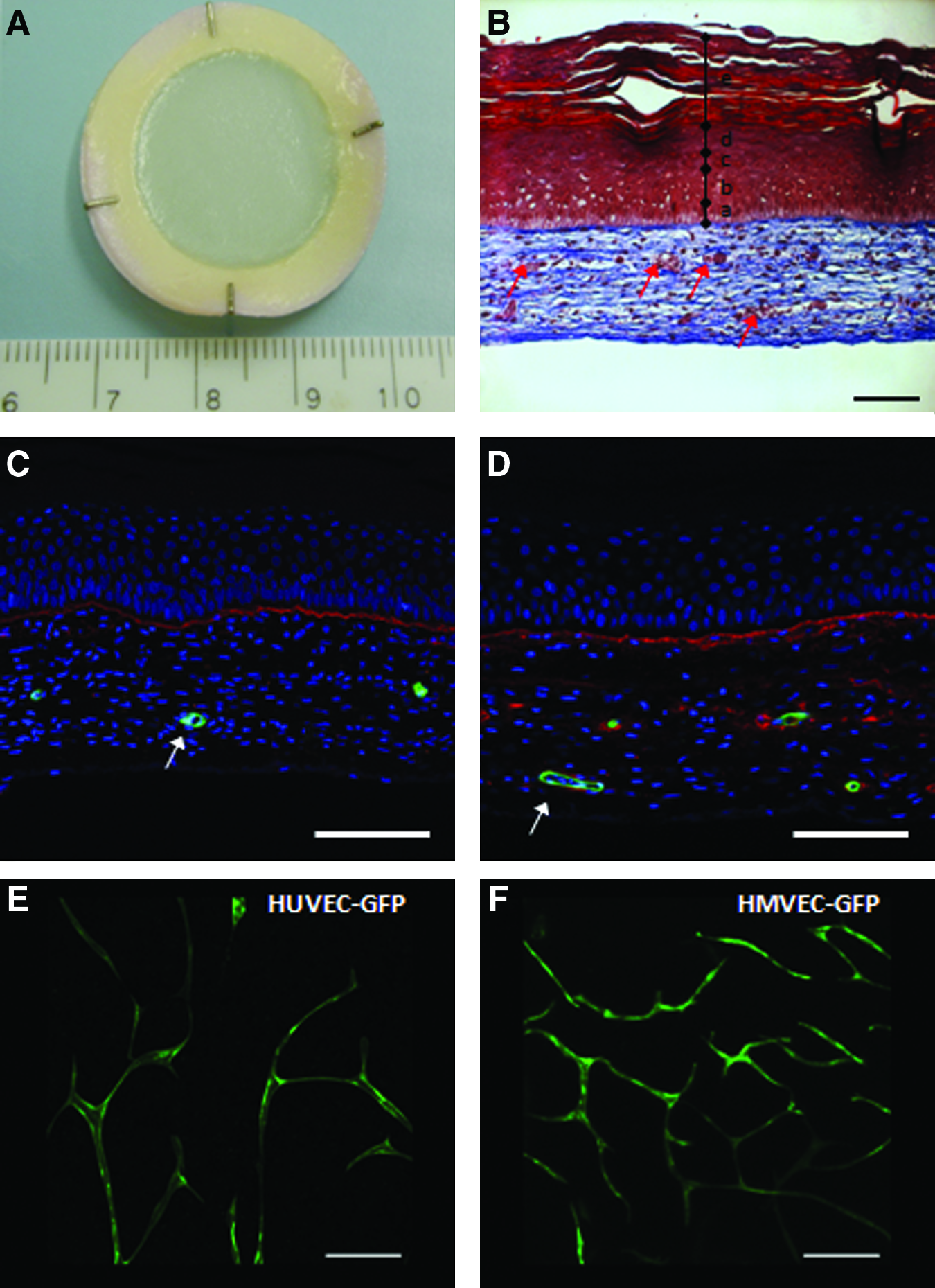
Human endothelialized reconstructed skin (ERS) characterization before transplantation. (
Remodeling of human microvascular network within 4 days after transplantation and development of functional anastomoses between the two microvascular networks
The ERS included its own intrinsic microvascular system before implantation, whereas the RS is considered the negative control, because it did not contain any human endothelial cell. A complete take of all grafts was observed only 2 days after transplantation. Macroscopically, both RS and ERS appeared to have adhered into underlying murine tissues 4 days after transplantation, but the bottom side is much more vascularized in the ERS than in the RS (Fig. 2A). Within the graft, human capillaries had a physiological diameter varying between 15 and 20 μm (Fig. 2B–D), forming a horizontal vascular plexus on the dermis. We showed that on day 4, microvessels lined with GFP+ human endothelial cells transported murine red blood cells (Fig. 2B). The presence of these cells in human capillaries is a clear demonstration of their functional anastomoses with the host's blood vessels (inosculation) between 3 and 4 days posttransplantation. This observation was done in all grafted ERS. These human blood-containing vessels were homogeneously distributed in the graft both in the superficial zone of the dermis and in its deeper zone, ensuring an adequate perfusion of the whole graft. The inosculation phenomenon is a physical connection between two functional microvascular networks. Thus, we observed a well-defined colocalization between human and mouse endothelial cells inside the same capillary, often named a chimeric microvessel 29 (Fig. 2C). At the same time, we observed a regression of nonperfused human blood capillaries, apparently due to apoptosis, as indicated by fragmented nuclei detected with Hoechst 33258 staining.30–32 Human endothelial cell nuclei, in nonperfused capillaries, demonstrated a chromatin distribution characteristic of apoptosis (Fig. 2D).
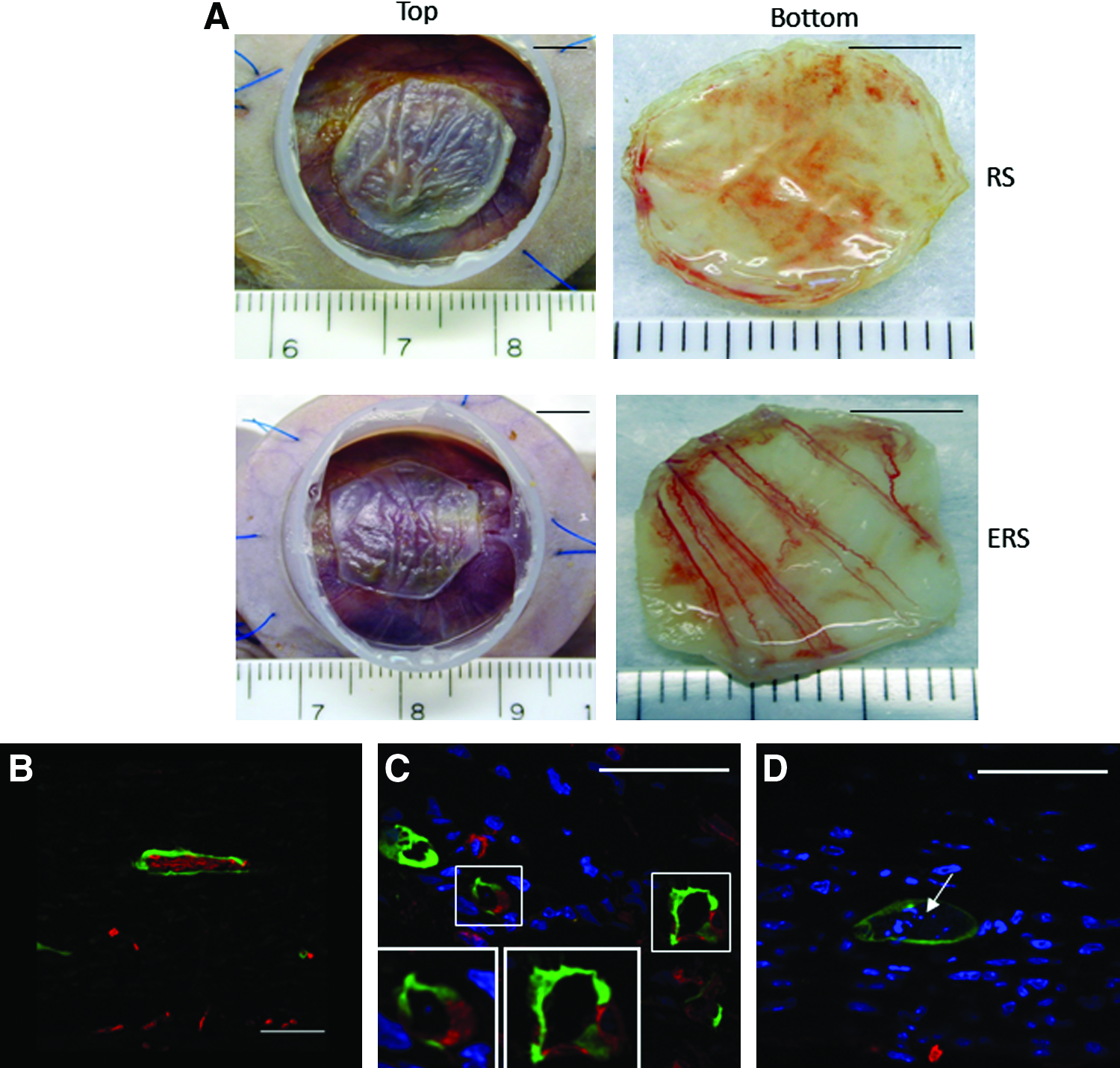
Vascular remodeling characterization of ERS on day 4. (
Medium-term regression of human endothelial cells
Human endothelial cells stably expressing luciferase allowed for quantitative analysis of endothelial cell density in biopsies harvested over time. Remodeling of the human microvascular network was analyzed over a 1-month period. Luciferase assay values from RS samples yielded background levels throughout this whole period. A significant decrease of the ERS luciferase values was observed between samples taken at the time of transplantation and those taken 2 days later, indicating a sevenfold reduction in the total number of living human endothelial cells present in the graft between these two time-points (Fig. 3; p = 0.0006). Total endothelial cell number, as evaluated by luciferase assay values, stayed stable for the first week and began to decrease with a complete loss of detection 1-month postsurgery. These results were supported by in situ fluorescence, as human endothelial cells also stably expressed GFP and by immunostaining using a specific antibody against human CD31.
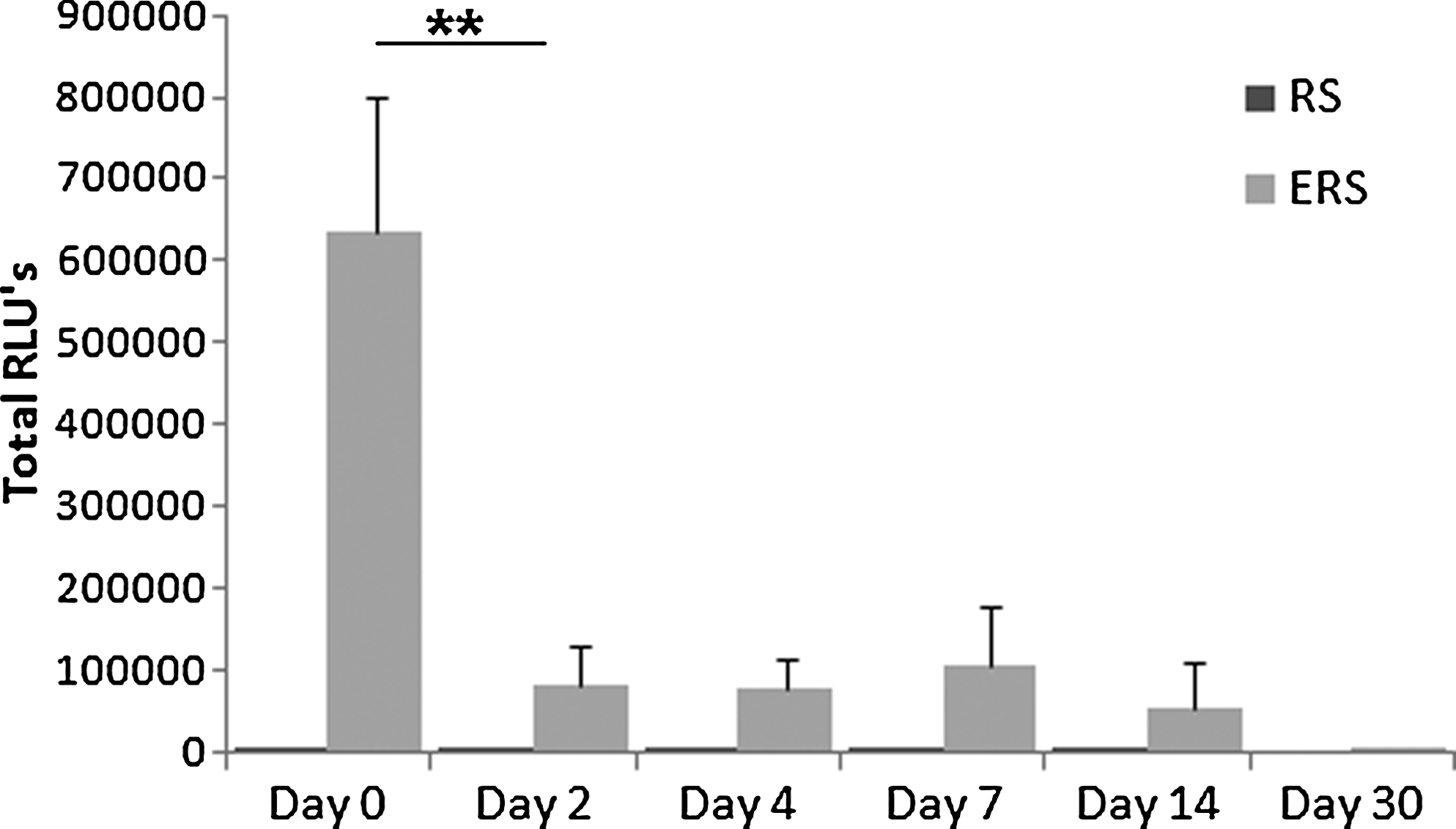
Quantification of human endothelial cell density in skin substitutes over time. HUVEC stably expressed luciferase. Luciferase activity of biopsies (n = 3) from each group (RS and ERS) were quantified using a luminometer. Luciferase activity was reported as total relative light units (RLUs). Values are given as means ± standard deviation. **p < 0.001.
Neovascularization of the human skin substitute by host endothelial cells
Neovascularization was quantified by image analysis of biopsy sections, by measuring the dermal thickness colonized by murine endothelial cells visualized with an antibody specific to murine CD31. Epidermal thickness was not taken into account in data collection, because it is an avascular compartment. We found that 2 days after transplantation, no murine endothelial cells could be detected in the implants, for both RS and ERS (Fig. 4A). The process of neovascularization took more than 2 days to occur in the skin substitute (Fig. 4B). However, after day 4, approximately 80% of ERS dermis thickness was colonized by murine microvessels, whereas this proportion was reduced to approximately 50% in RS, p < 0.001. Neovascularization started with the process of capillary growth in the lowermost portion of the dermis from the vascular bed of the wound. Indeed, murine endothelial cells mostly invaded the wound site from its bed but not at the margin, ensuring an adequate perfusion of the entire surface of the graft. These newly developed vessels were oriented toward the graft's epidermal layer and ascended linearly with almost no mutual intersections for ERS, covering the area up to the superficial zone of the dermis, whereas they partly formed serpentine vascular networks in RS and covered only up to the intermediate zone. One week after transplantation, the entire thickness of the dermal layer exhibited a dense and complex network of newly formed microvessels for both RS and ERS and in the case of ERS grafts integrated human endothelial capillaries. Quantitative analysis of immunohistochemical data demonstrated that our model of ERS increased the neovascularization speed of murine CD31-positive vessels in the dermal layer of the grafts compared with control RS, although after 1 week both RS and ERS were similarly colonized.
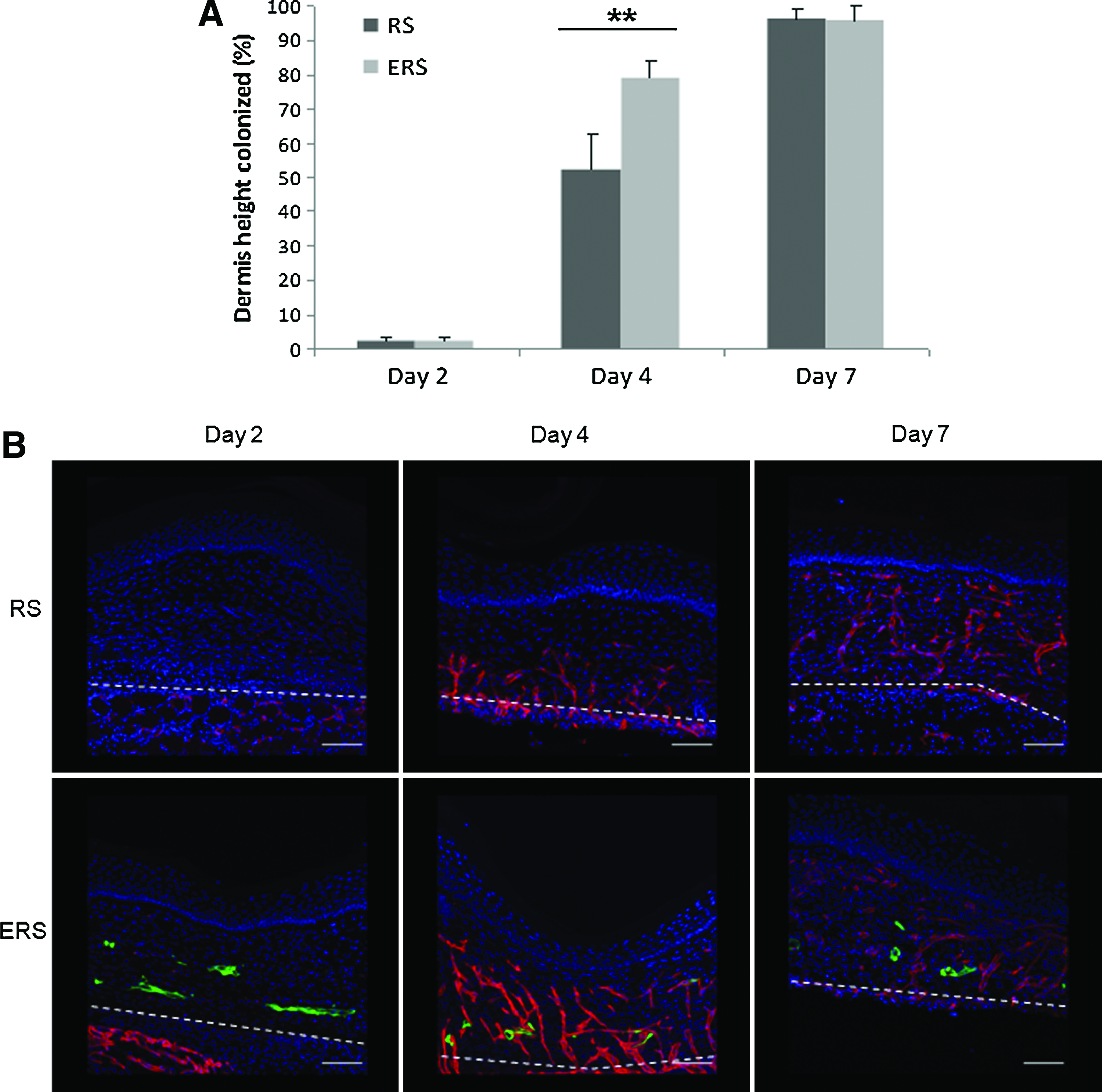
ERS promotes neovascularization of the human skin substitute by murine endothelial cells compared with control RS. (
Discussion
Most of the time, transplantations fail due to the lack of microvascularization. Vascularized grafts would contribute to a better engraftment, long-term survival, and functionality of tissue substitutes.
Previous work conducted in our laboratory led to the development of the first endothelialized human tissue-engineered skin onto a collagen biopolymer in which a network of capillary-like tubes was formed. 17 In this present study, our aim was to develop an easy to handle model of ERS that promotes the spontaneous in vitro formation of a capillary-like network exclusively by coculture of human dermal fibroblasts, endothelial cells (HUVECs or HMVECs), and keratinocytes without any extrinsic scaffold or biomaterial, different from our previous model. Besides, our substitutes could be totally autologous for clinical application. In our model, cells secrete their own extracellular matrix, creating a physiological microenvironment in which 3D cell–cell and cell–extracellular matrix interactions led to a homogenous distribution of endothelial cells that organized into a microvascular network throughout a large 350–400 μm thick substitute. As it is, this substitute's thickness can be compared with native human skin split-thickness grafts used in the clinical arena, which can be categorized as thin (130–300 μm), intermediate (300–460 μm), or thick (460–760 μm).
We assumed that creating a tissue-engineered skin substitute comprising its own intrinsic blood supply would improve graft vascularization after transplantation. Thus, our study presents its in vivo evaluation after grafting them on athymic mice. Foremost, the rapid and high quality take for all transplants, endothelialized or not, is to be noted. Then, the human microvascular network generated in vitro, formed with GFP-positive endothelial cells, rapidly became functionally continuous with the host's vasculature in less than 96 h postsurgery. Red blood cells were found in the lumen of capillaries lined by human cells and indicate the beginning of efficacious blood circulation. The establishment of a blood supply in the graft appears to depend on the growth of host vessels into the graft's dermis, thus establishing observable chimeric endothelial channels as early as day 4, as has been established by other studies with human skin when grafted on athymic mice.33,34 It can be assumed that a delay is needed for the murine vessels to cross through the human dermis and develop functional links with its microvascular network. Complete neovascularization of our RS is similar with previous results from our laboratory with another endothelialized skin, 18 but much faster than observed in other models. Until now, numerous studies have demonstrated that over a period of several weeks host blood vessels invaded engineered tissues composed of synthetic biodegradable polymers.35–39
The persistence of human endothelial cells was studied via the stable expression of luciferase and, thus, we obtained a quantitative evaluation of the vascular remodeling of our capillary-like network after transplantation visualized with GFP expression in human endothelial cells. The density of human endothelial cells in ERS drastically decreased between 0 and 2 days, which may be due to a degeneration of supernumerary vessels to reach a physiological density. A clear decrease in human endothelial cell density was displayed during the first week postsurgery, but a statistically significant difference was not observed. Observations suggested that numerous capillary sprouts from the wound bed formed functional anastomoses with most of human capillaries. However, we had noted a regression by apoptosis of rare nonperfused capillaries. Actually, although initially independent of the circulation, our microvascular system is later shaped by forces, such as shear stress, generated by circulation. 40 Our observations are consistent with other data, indicating that reduction or absence of shear stress is associated with endothelial cell apoptosis leading to vessel regression.41–44 Finally, 1-month postsurgery, human endothelial cells had totally disappeared.
Complete replacement of donor graft vasculature by endothelial cells from the recipient along preexisting channels is a key mechanism for skin graft revascularization. Our skin substitute was neovascularized and remodeled with the host's own endothelial cells. Murine angiogenic blood vessels originated in the wound bed and were directed linearly toward the epidermal layer of the graft. The period required for the ingrowth of new host blood vessels into the ERS was dramatically shortened compared with RS. Although no murine endothelial cells were found in the transplanted human dermis, neither in RS nor in ERS at day 2 postsurgery, 50% of the RS human dermis was neovascularized by murine endothelial cells versus almost 80% in the ERS at day 4. One-week posttransplantation, 100% of the dermis was colonized by host endothelial cells, in both RS and ERS. Thus, the adequate perfusion of the graft was faster in the ERS due to the prefabricated microvascular network. A number of studies have shown that cultured endothelial cells exerted an angiogenic effect in vivo at the graft site and promoted wound healing.45,46 Thus, we may assume that human endothelial cells contained in our substitute secreted cytokines and growth factors that had paracrine functions, leading to murine endothelial cell proliferation, elongation, and orientation.
In summary, we have demonstrated that graft revascularization was achieved by a dual process of direct connection between the graft or host vasculatures and ingrowth of host vessels into the graft. The angiogenic effect induced by an intrinsic microvascular network constructed in vitro in the skin substitute promoted faster vascularization of the graft. In our case, our dermis thickness was only 200 μm, so the beneficial angiogenic effect was limited. However, in the case of thicker skin substitutes, the advantage will be considerable and will result in a more rapid and reliable engraftment.
Clinical application perspectives are very exciting for our ERS, because our model also paves the way to engineer larger and thicker tissues, thanks to their prevascularization. Our endothelialized reconstructed tissues, with more physiologically relevant complexity, will enhance the success of transplantations used to treat deep burns, ulcers, and other tissue loss due to disease or trauma.
Finally, the possibility to build in vitro relevant models of vascularized tissues closer to physiological reality provides an interesting and effective tool for preclinical assays of pharmaceutical agents and for fundamental research studies on physiologic and physiopathologic vasculatures. The investigation of angiogenesis induced by skin cancer during its progression is another avenue where our ERS could be a powerful tool.
Footnotes
Acknowledgments
We wish to thank Mrs. Anne-Marie Moisan and Nathalie Tremblay for their excellent technical assistance, and Dr. Dan Lacroix for his careful reading of this manuscript. This work was supported by the Canadian Institutes of Health Research (MOP-14364).
Disclosure Statement
No competing financial interests exist.