
Abstract
Grafting of elastomeric biomaterial scaffolds may offer a radical strategy for the prevention of heart failure after myocardial infarction by increasing efficacy of stem cell delivery as well as acting as mechanical restraint devices to constrain scar expansion. Biomaterials can be partially optimized in vitro, but their in vivo performance is most critical and should ideally be monitored serially and noninvasively. We used magnetic resonance imaging (MRI) to assess three scaffold materials with a range of structural moduli equal to or greater than myocardial tissue: poly(glycerol sebacate) (PGS), poly(ethyleneterephathalate)/dimer fatty acid (PED), and TiO2-reinforced PED (PED-TiO2). Patches, 1 cm in diameter, were grafted onto the hearts of infarcted rats, with biomaterial-free infarcted rat hearts used as controls. MRI was able to determine scaffold size and location on the heart and identified unexpectedly rapid in vivo degradation of the PGS compared with previous in vitro testing. PED patches did not withstand in vivo attachment, but the more rigid PED-TiO2 material was detrimental to heart function, increasing chamber and scar sizes and reducing ejection fractions compared with controls. In contrast, the mechanically compatible PGS scaffold successfully reduced hypertrophy, giving it potential for limiting excessive postinfarct remodeling. PGS was unable to support systolic function, but it would be suitable for strategies to deliver cardiac stem/progenitor cells, to limit remodeling during the period of functional cellular integration, and to degrade after cell assimilation by the heart. This work has also shown for the first time the value of using MRI as a noninvasive tool for evaluating and optimizing therapeutic biomaterials in vivo.
Introduction
In vitro tissue engineering of a scaffold material seeded with cells before grafting into the infarcted heart may offer a method for improving the efficacy of cell delivery7–10 as well as incorporating the added benefit of direct mechanical support offered by the scaffold material. This support could slow or prevent the development of heart failure by reducing postinfarction wall stress and preventing excessive remodeling or aneurism, while the new cardiomyocytes will augment systolic contraction.11,12 Many different cell encapsulating biomaterials have been suggested for engineering of cardiac tissue constructs, 11 including naturally occurring gels (Matrigel, 13 fibrin glue, 14 alginate,7,15 and collagen 16 ) and synthetic thermoplastic polyester, for example, poly(lactic acid). These materials support cell growth and retention, but they are either mechanically weak or nonelastic. 17
To quantitatively design the heart patch, it is necessary to introduce a concept, structural modulus Ω, which describes the capability of a sheet material to resist expansion under pressure. Structural modulus not only reflects the material's property (i.e., Young's modulus) but also the construct's geometry (i.e., thickness).
17
In the application of a heart patch, the structural modulus Ω is
where E is the Young's modulus of the material and t is the thickness of the sheet. Therefore, mechanocompatibility requires
that is,
There is a hypothesis embedded in equations (2) and (3), that is, the mechanotherapeutic effect is optimal when the injured area is free of stress and its contractile function is temporarily replaced by the elastic patch. The Young's modulus Eheart of heart muscle is 0.05 MPa and rat heart wall thickness at end diastole, theart, is 2 mm, 18 giving a structural modulus of 0.1 N/mm. The heart patch thickness tpatch should be 0.2–0.5 mm to prevent tearing during attachment, and adhesion to or pressure on the chest wall. 19 Using equation (3), a 0.33-mm-thick patch should have a Young's modulus of 0.3 MPa to match the structural modulus of the myocardium. However, the mechanical function of a heart patch is complicated by material degradation and the healing profile of the diseased heart muscle. Further, true restraint of expansion may require a modulus significantly greater than one just matching the properties of the myocardium. This suggests that an initial structural modulus of >0.1 N/mm may be required. Hence, we tested three elastomeric biomaterials, poly(glycerol sebacate) (PGS), poly(ethyleneterephathalate)/dimer fatty acid (PED), and TiO2-reinforced PED (PED-TiO2), with a range of structural moduli, 0.117, 0.924, and 8.811 N/mm, respectively.
To test the theory that an elastically compatible scaffold will reduce postinfarct remodeling and hypertrophy, we used magnetic resonance imaging (MRI) to evaluate in vivo the mechanically related therapeutic effect (mechanotherapeutics) of these three patch materials grafted onto the hearts of infarcted rats. We would anticipate that the benefit of inhibition of scar expansion would be greatest during the first weeks after infarction, which is why we chose to apply the patch at the time of infarct. The results will form the basis for a decision on which material might be taken forward to a combined stem cell/material patch therapy. A further goal was to develop MRI methods that gain information about the interaction between patch materials and the beating heart in vivo. MRI sets the gold standard for measuring in vivo cardiac function in both small animals and humans.20,21 The use of MRI contrast agents gives information on myocardial viability 21 and has been used to track stem cell location in live animals, 3 but its potential for studying material/cardiac interactions has not been fully realized.
Methods
Experimental design
Ex vivo study
A pilot study was performed using the two stiffest materials to ensure that no immediate morbidity or mortality would be seen in the animals and to determine whether they could be detected by MRI under ideal conditions. PED (n = 6) and PED-TiO2 (n = 6) scaffolds were grafted onto control rat hearts, which were excised after 1 week and imaged using three-dimensional (3D) MR microscopy.
In vivo study
PED-TiO2 (n = 6) and PGS (n = 6) scaffolds were grafted onto infarcted hearts. Infarcted hearts without scaffolds were used as controls (MI group, n = 6). In vivo MRI was performed at 1 and 6 weeks after infarction, and then hearts were fixed for histology.
Scaffold material synthesis
PGS was synthesized through polycondensation. Briefly, an equimolar mixture of glycerol (Sigma) and sebacate (Aldrich) was melted at 120°C under argon for 24 h. The prepolymer was dissolved into tetrahydrofuran, cast on glass slides to produce sheets, and incubated for 48 h at 120°C under a vacuum. After cooling at room temperature under vacuum, sheets were autoclaved for sterilization. PGS sheets had Young's modulus of 0.3 MPa and thickness of 0.39 mm.
PED and PED-TiO2 scaffolds were synthesized as described elsewhere. 22 Briefly, transesterification of dimethyl terephthalate (Aldrich) and ethylene glycol (Aldrich) was performed at elevated temperature in the presence of Zn(Ac)2 (Aldrich) and Sb2O3 (Aldrich). A dimer fatty acid (Uniqema; acid value 196 mg KOH/g) and TiO2 nanoparticles of mean particle size 23 nm (Aeroxide® P25; Degussa) were added to the PED-TiO2 scaffolds and polycondensation was carried out at 285°C–290°C and 0.5–0.6 mmHg of vacuum. The Young's moduli of PED and PED–0.2 wt% TiO2 used in this work were 2.8 and 26.7 MPa, respectively. The thickness of sheets was 0.33 mm.
MI and scaffold grafting
All procedures were conducted in accordance with the University of Oxford and Imperial College, London, Animal Ethics Review Committees and the Home Office, London. MI or sham surgery was performed in 30 male Wistar rats by ligation of the left anterior descending coronary artery as described. 23 Scaffolds were attached to the epicardial surface shortly after the induction of infarction using 12–16 continuous stitches.
3D MR microscopy
Hearts were excised, fixed in paraformaldehyde, and embedded in 1% agarose doped with gadolinium diethylenetriaminepentaacetic acid. MRI was performed at 11.7 T using a 40 mm quadrature-driven birdcage coil (Rapid Biomedical) and a 3D fast-gradient echo sequence (TE/TR 1.8/15 ms; 15° pulse; field of view 32 × 32 × 64 mm; matrix size 512 × 512 × 512; voxel size 32 × 32 × 64 μm; six averages). 23
In vivo MRI
Cardiac cine-MRI was performed as described. 24 Briefly, using an 11.7 T MR system with a Bruker console running Paravision 2.1.1 and a 52 mm birdcage coil, a stack of contiguous 1.5-mm-thick true short-axis electrocardiogram and respiration-gated cine images (TE/TR 1.43/4.6 ms; 17.5° pulse; field of view 51.2 × 51.2 mm; matrix size 256 × 256; voxel size 200 × 200 × 1500 μm; 25–35 frames per cardiac cycle) were acquired to cover the entire left ventricle (seven to nine slices). Long-axis two-chamber and four-chamber images were also acquired. Delayed enhancement MRI (DE-MRI) was performed on slices containing scaffold material at 10–25 min after gadolinium diethylenetriaminepentaacetic acid infusion using the same cine-MRI sequence, but with flip angle increased to 60° to induce saturation of signal in normal myocardium. The entire imaging protocol was performed in ∼60 min.
MRI data analysis
Image analysis was performed using Image J (NIH Image). Left ventricular volumes, ejection fractions, and scar sizes (defined as akinetic myocardium) were calculated as described. 23 DE-MR images were thresholded to two standard deviations above the mean signal intensity from normal tissue and qualitatively assessed for regions of tissue necrosis. To measure scaffold volumes, images were thresholded to enhance contrast between the myocardium and the scaffold, and semiautomated analysis of the scaffold area was performed in each MRI slice.
Histology
Hearts were excised, washed, and frozen. Serial 10 μm cryosections were cut in the short axis-orientation and stained with hematoxylin and eosin.
Results and Discussion
Ex vivo detection of grafted patches
Ex vivo experiments aimed to test the mechanical integrity of the patch materials and the feasibility of visualizing the patch using MRI. As the physical integrity of grafted PGS has been demonstrated,25,26 only PED or PED-TiO2 scaffolds were grafted onto normal rat hearts. At 1 week, hearts were excised and MR microscopy was performed. Scaffolds were clearly identifiable as signal voids on the epicardial surface of the myocardium (Fig. 1), indicating that MRI can be used to evaluate scaffold materials. The solid nature and very limited water permeability of the scaffold materials meant that they produced no MRI signal, which allowed their identification as signal voids in a proton-rich, aqueous environment.
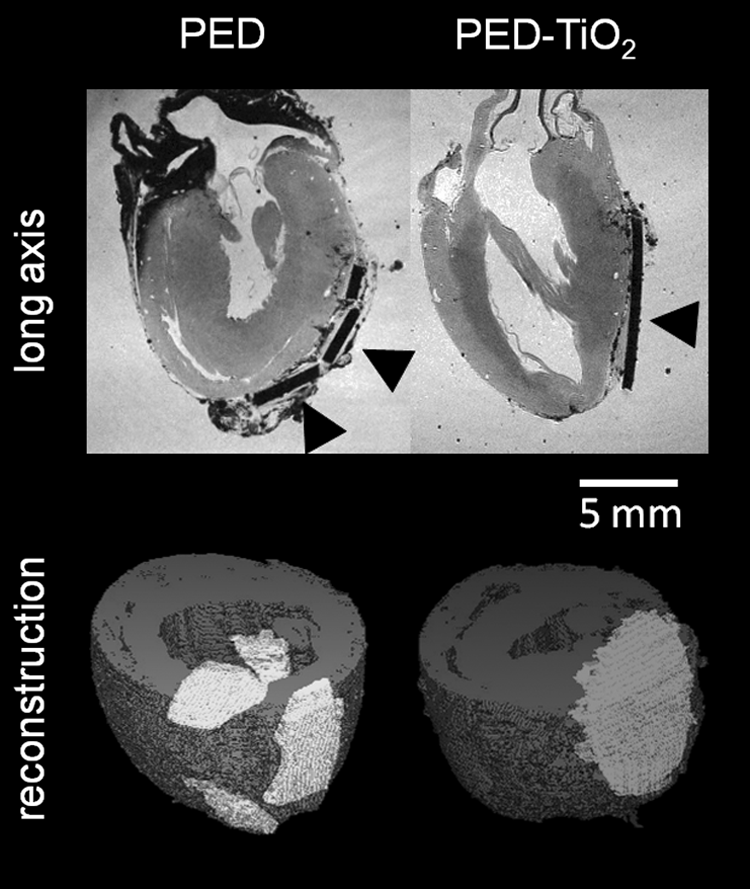
Ex vivo scaffold detection: Upper panel shows MR microscopy images of PED and PED-TiO2 scaffolds attached to the epicardium of control rat hearts. Arrowheads indicate scaffold location. Lower panel shows 3D reconstruction of the hearts with scaffold attached. MR, magnetic resonance; PED, poly(ethyleneterephathalate)/dimer fatty acid; PED-TiO2, TiO2-reinforced PED.
MR microscopy revealed that PED scaffolds had become fractured into two to four pieces by the stresses exerted during repeated cardiac contraction, whereas the PED-TiO2 and PGS remained intact. There was no difference in patch volume between the PED and PED-TiO2 scaffolds (46 ± 6 vs. 42 ± 4 mm3). The fracture of PED was likely caused by hydrolysis of ester links in the soft dimer fatty acid segments, leaving nondegradable polyethyleneterephthalate behind. This may occur faster in vivo owing to the catalytic function of enzymes, including esterase and oxidoreductase. 27 Hence, PED was excluded from further in vivo studies.
In vivo detection of grafted patches
PED-TiO2 and PGS scaffolds were grafted onto infarcted rat hearts shortly after coronary occlusion. Implantation of the patch did not lead to excess mortality or obvious morbidity. In vivo MRI was performed at 1 and 6 weeks after implantation. The grafted scaffolds were identifiable as signal voids on the epicardial surface of the myocardium and were visible throughout the cardiac cycle (Figs. 2 and 3). The PED-TiO2 scaffolds remained in a rigid flat sheet during systole, whereas PGS scaffolds were more compliant, bowing during cardiac contraction and matching the curvature of the heart.
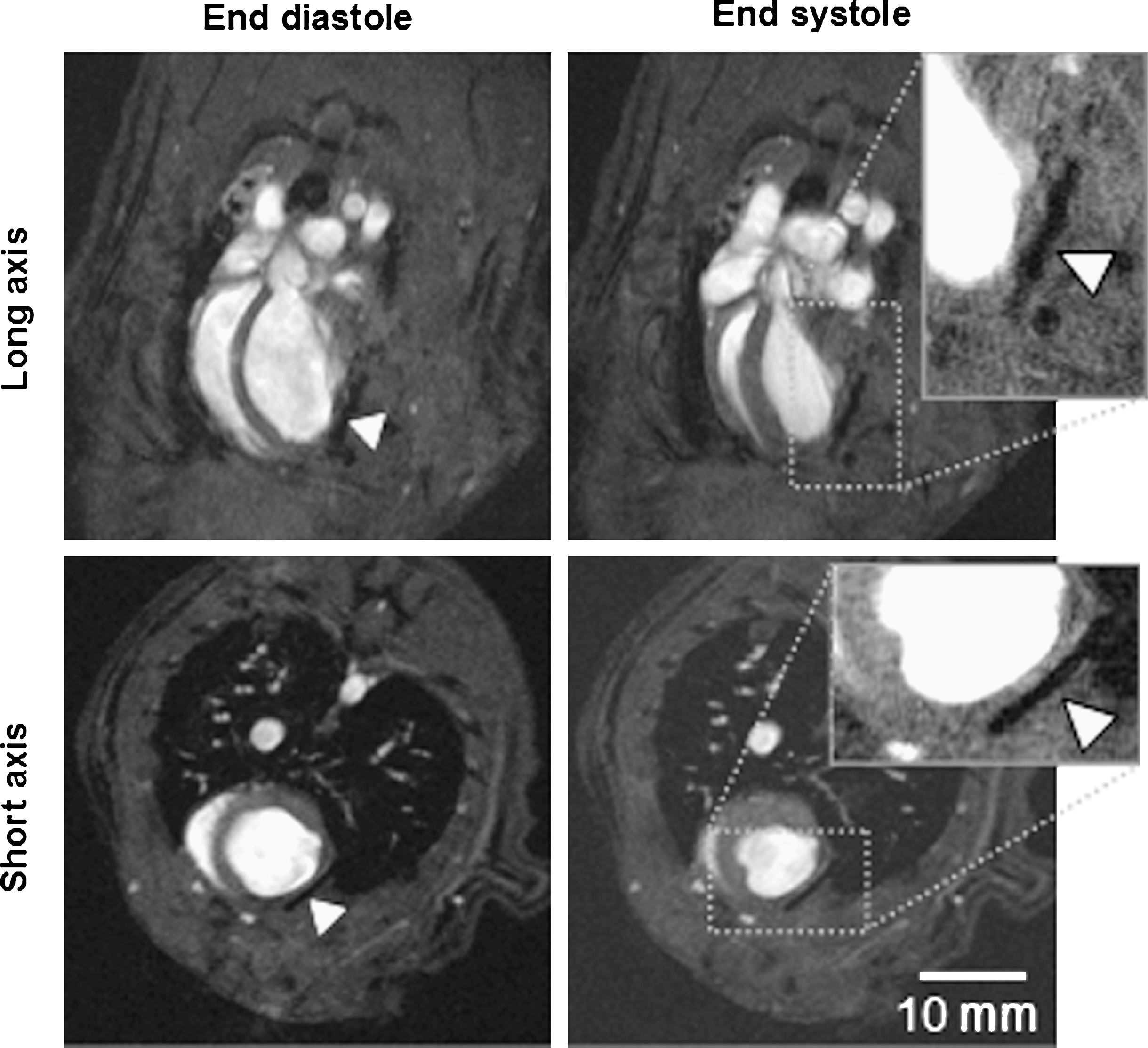
In vivo scaffold detection: Long and short axis cine-MRI acquired at end diastole and end systole. Arrowheads show the location of the PED-TiO2 scaffold. MRI, magnetic resonance imaging.

Serial cine-MRI: Representative end systolic frames of cine images acquired at 1 and 6 weeks after infarction. Arrowheads show the location of the scaffolds. Note the larger end systolic volume of the PED-TiO2 image at 6 weeks; the PGS scaffold has bowed with the curvature of the heart (white arrows); by 6 weeks, little PGS scaffold material is detectable. PGS, poly(glycerol sebacate).
In vivo measurement of heart patch degradation
The high contrast between scaffold and surrounding tissue permitted accurate measurement of scaffold volume and quantification of degradation. The size of the scaffold-induced signal void within each MRI was measured at 1 and 6 weeks after implantation. At 1 week, the volumes of PED-TiO2 and PGS scaffolds were similar (32 ± 7 vs. 36 ± 8 mm3). At 6 weeks, the volumes of the PED-TiO2 scaffolds had not changed, whereas PGS scaffolds had almost completely degraded (32 ± 7 vs. 3 ± 2 mm3), with only small fragments remaining attached to the epicardium. These observations were confirmed by histology (see Histology section). This result was unexpected, as incubation of PGS material for 60 days in cell culture media at 37°C resulted in <4% reduction in weight. 17 The rapid in vivo degradation of PGS can be attributable to esterase- and oxidoreductase-mediated hydrolysis of the ester links.
In vivo measurement of cardiac morphology and function
MI rapidly leads to tissue necrosis and reduced contractility within the territory of the occluded artery. 28 By 1 week after infarction, a collagenous scar begins to form, ejection fraction, normally 72% in similar sized control rats, 24 has decreased, and end systolic volume, normally 115 μL, 24 has increased, as demonstrated by the control MI group of this study (Fig. 3 and Table 1). From 1 to 6 weeks the surviving myocardium undergoes hypertrophy and dilation to maintain cardiac output, even with lower ejection fraction, as is evident from the increased left ventricle (LV) mass and end diastolic volumes of the control MI group (Table 1). Although hypertrophy can initially compensate for the infarcted akinetic myocardium, the increased wall stress associated with chamber enlargement can lead to excessive dilation and eventually heart failure, where cardiac output is reduced to a level insufficient to perfuse the body.
p < 0.05 compared with MI group.
MI, myocardial infarction; PED-TiO2, TiO2-reinforced PED; PGS, poly(glycerol sebacate); LV, left ventricle.
At 1 week there were no significant differences in any of the measured parameters of cardiac morphology and function between the MI, PED-TiO2, and PGS groups (Table 1). However, DE-MRI performed at 1 week identified extensive tissue necrosis adjacent to the sites of attachment of the PED-TiO2 but not PGS scaffolds (Fig. 4). This tissue damage probably resulted from the much higher Young's modulus of the PED-TiO2 patch, which made it insufficiently compliant, leading to different extension profiles during contraction and thus sliding of the heart wall against the attached patch. Consequently, the heart, which is the softer of the two, was damaged. In a separate study, we have confirmed that the TiO2 nanoparticle component of PED-TiO2 has little effect on adult cardiac myocytes, eliminating this as a possible source of the damage observed (Nanotoxicology, in press). Opportunities to improve the PED-TiO2 composite patch are also being explored by reducing TiO2 nanoparticle content and by optimizing the patch design by adding porosity to reduce stiffness.

DE-MRI: Images acquired at 1 week after scaffold attachment. The inset of the upper panel shows extensive hyperenhancement in the vicinity of the PED-TiO2 scaffold attachment sites (white and black arrowheads), whereas in the lower panel enhancement is localized to the site of infarction and not adjacent to the PGS scaffold attachment sites. DE, delayed enhancement.
After 6 weeks, severe remodeling occurred in the PED-TiO2 group, with 33% higher end systolic volumes, 14% lower ejection fractions, and 68% higher scar sizes compared with the MI group (p < 0.05; Table 1). Hence, the rigid PED-TiO2 patch impeded contraction, induced necrosis, and exacerbated postinfarct remodeling and hypotrophy, resulting in increased end systolic volumes and scar sizes and reduced stroke volumes and ejection fractions.
Hearts treated with the PGS scaffold showed similar ejection fractions and end diastolic and systolic volumes to the control MI group at 6 weeks. The increase in myocardial mass was 57% lower (p < 0.0005; Table 1) and LV-to-body mass ratio was also significantly lower compared with control infarcts. This indicates that hypertrophy in the PGS group was reduced. However, this potential benefit was outweighed by a negative effect on stroke volumes and cardiac outputs, which increased from 1 to 6 weeks in the MI group, but remained unchanged in the PGS group (Table 1), suggesting that the scaffold-mediated reduction in hypertrophy had compromised systolic function.
The grafted scaffold materials were designed to perform two functions: (1) limit excessive chamber dilation and (2) aid systolic contraction. Our MRI results indicate that the PED-TiO2 patch was too rigid to perform these functions and that it damaged the myocardium. The PSG scaffold successfully reduced hypertrophy, giving it potential as a biomaterial for limiting excessive remodeling. PGS was unable to assist systolic contraction: cardiac remodeling is a strategy that initially allows cardiac output to be maintained and its prevention may have been counterproductive. Modification of the biodegradation properties to prevent the rapid breakdown in vivo could possibly enhance the support by PGS. We have shown that altering the curing temperature is able to reduce degradation rates. 17 However, if the goal is to use the patch to deliver cardiac stem/progenitor cells, then these will provide the contractile component required for the heart patch to assist systolic function. Embryonic stem cells can be cultured on the surface of elastomeric scaffold materials,17,25 whereas neonatal cardiac fibroblasts and myocytes can be seeded within porous PGS constructs. 29 The properties of PGS in terms of temporary support to reduce remodeling during the period of functional cellular integration, followed by rapid degradation to remove the material, may be advantageous.
Histology
No evidence of infarction was found after patch grafting onto control hearts. When hearts were removed from infarcted rats, PGS scaffolds were found to have few adhesions to the chest wall, whereas PED-TiO2 scaffolds exhibited strong adhesions. Examination of histological sections stained with hematoxylin and eosin indicated that PED-TiO2 scaffolds had remained intact and unchanged in shape. Moreover, fibrous tissue was found on the surface of PED-TiO2 scaffolds, as well as some thinning of myocardium at the adjoining points (Fig. 5), which forms further evidence that there was severe wearing or friction on the surface myocardium caused by PED-TiO2. The majority of PGS scaffolds had degraded with only small strings remaining on the LV. Similarly, a previous study in which porous PGS scaffolds were attached to infarcted hearts found that at 2 weeks after grafting, scaffolds had partially degraded and incorporated into the myocardium, with invasion of host cells and vessels. 29

Histology: Hematoxylin and eosin-stained sections from (
Significance of using MRI in tissue engineering
Tissue engineering has become a reality for bone regeneration, 30 treatment of burns, 31 cartilage replacement, 32 and airway reconstruction. 33 Engineered heart tissue is also under development and has great potential for the treatment of MI and prevention of heart failure. Development of engineered heart tissue requires the application of noninvasive and nondestructive in vivo imaging that can measure scaffold location and degradation and can assess the effect on cardiac function. Here we report the first noninvasive method for measurement of cardiac scaffold location and degradation in vivo.
The properties of scaffold materials implanted into animals have previously been studied by histology of material recovered after sacrifice, precluding serial measurements of the same sample and making temporal changes impossible to record. 6 Noninvasive techniques, including single-photon computed tomography, 34 bioluminescence imaging, 35 and ultrasound 36 have been used to monitor drug- 34 and cell-seeded 35 materials implanted subcutaneously35,36 or into bone 34 of mice and rats. Although these methods give valuable information, the ionizing radiation, poor spatial resolution, and/or requirement for genetic modification of donor cells make the techniques suboptimal. MRI overcomes these limitations and produces high-resolution 3D images from naturally abundant protons within the sample. MRI has been used to characterize cell-seeded bioscaffolds in vitro37,38 and in vivo,39,40 with bone formation serially monitored after subcutaneous implantation of demineralized bone matrix 39 and iron oxide-labeled bone marrow cell-seeded scaffolds located 40 in live rats. The present work showed for the first time that MRI can be used to locate cardiac scaffolds in vivo, characterize the integrity of scaffold materials grafted onto rat hearts, and make serial measurements of biomaterial degradation, in addition to accurate assessment of cardiac function.
Summary
The present work explored the mechanotherapeutic effects of biomaterial heart patches using in vivo MRI. We show that a rigid PED-TiO2 scaffold damaged heart muscle via surface friction, which increased tissue necrosis, scar size, adhesions to the chest, and fibrosis and reduced cardiac function compared with control infarcted rats. It may be possible to improve the PED-TiO2 scaffolds by reducing TiO2 nanoparticle content and by adding porosity—this being investigated separately.
The present results showed that mechanically compatible PGS patch effectively prevented postinfarction hypertrophy but did not assist contractile function, resulting in lower stroke volumes and cardiac outputs. The properties of in vivo biocompatibility and limitation of remodeling, as well as the previously demonstrated tuning of biodegradation rates and support of human embryonic stem cell-derived cardiomyocytes, makes PGS a promising candidate for further development as a heart patch. 25 In addition, this work has shown for the first time that MRI can be used as a noninvasive method for the evaluation of tissue-engineered scaffolds in vivo.
Footnotes
Acknowledgments
The authors thank the staff at CBS, RBH Campus, Imperial College, for their support. This study was funded by the Biotechnology and Biological Sciences Research Council (BB/D011027/1), British Heart Foundation (PG/07/021/22511). The authors also acknowledge Prof. M. El Fray, Polymer Institute, West Pomeranian University of Technology, Poland, for developing the PED and PED-TiO2 materials used in this study.
Disclosure Statement
No competing financial interests exist.