
Abstract
Engineered cartilage composed of a patient's own cells can become a feasible option for auricular reconstruction. However, distortion and shrinkage of ear-shaped constructs during scaffold degradation and neocartilage maturation in vivo have hindered the field. Scaffolds made of synthetic polymers often generate degradation products that cause an inflammatory reaction and negatively affect neocartilage formation in vivo. Porous collagen, a natural material, is a promising candidate; however, it cannot withstand the contractile forces exerted by skin and surrounding tissue during normal wound healing. We hypothesised that a permanent support in the form of a coiled wire embedded into a porous collagen scaffold will maintain the construct's size and ear-specific shape. Half-sized human adult ear-shaped fibrous collagen scaffolds with and without embedded coiled titanium wire were seeded with sheep auricular chondrocytes, cultured in vitro for up to 2 weeks, and implanted subcutaneously on the backs of nude mice. After 6 weeks, the dimensional changes in all implants with wire support were minimal (2.0% in length and 4.1% in width), whereas significant reduction in size occurred in the constructs without embedded wire (14.4% in length and 16.5% in width). No gross distortion occurred over the in vivo study period. There were no adverse effects on neocartilage formation from the embedded wire. Histologically, mature neocartilage extracellular matrix was observed throughout all implants. The amount of DNA, glycosaminoglycan, and hydroxyproline in the engineered cartilage were similar to that of native sheep ear cartilage. The embedded wire support was essential for avoiding shrinkage of the ear-shaped porous collagen constructs.
Introduction
During the past two decades, attempts have been reported by our research groups4–7 and others8–13 that have uncovered difficulties related to engineering three-dimensional human ear-shaped cartilage with its complex architecture and largely unsupported, protruding, three-dimensional structure. The biggest challenge, however, remains to demonstrate specific shape retention of the auricle in longer term in vivo studies. Shape changes inevitably occurred upon degradation of the internal supporting polymer scaffold,6,11 or removal of external stents, which were preserving auricle shape.5,7,9
The success of engineering auricular cartilage largely depends on the ability of the scaffold to support cartilage formation, withstand contractile healing forces, and degrade without inducing a deleterious effect on the newly formed tissue. To maintain implant structural integrity in the presence of immature developing tissue, the supporting scaffold must withstand the aggressive healing forces encountered upon subcutaneous implantation, especially in an immunocompetent animal. The degradation rate of the scaffold material must match the rate of the new tissue formation; premature degradation leads to scaffold collapse and loss of implant shape.
For human ear-shaped constructs, scaffolds have been often manufactured from a combination of polyglycolic acid, poly-L-lactic acid, and polycaprolactone.2,4–6,8,10,11,13,14 Mechanical properties and degradation rates of synthetic materials can be modified, and polymers can be combined in various ratios to meet the mechanical and degradation requirements discussed above. Indeed, the ear-shaped constructs containing polymers with slower degradation rates, such as polycaprolactone, were better preserved at the end of the studies because the shape of the auricle was maintained mostly by the still present scaffold material.6,8,10,11 However, the degradation products of the synthetic materials often cause chronic inflammation that can negatively affect neocartilage formation.15–18
Natural materials, such as collagen, are promising candidates for cartilage engineering; being part of extracellular matrix (ECM), natural materials are abundant and biocompatible and their use eliminates the negative impact of the degrading synthetic polymers on neocartilage.19,20 Although significant immune response can be mounted to collagen-based products, advances in collagen purification and processing have rendered them biocompatible. 21 Scaffolds made of collagen originating from diverse animal tissues are commercially available and have been actively used in research and clinical applications. Employing collagen scaffolds, several types of tissues, including meniscal cartilage, have been successfully regenerated 22 and osteochondral defects have been repaired in patients.23,24
Cartilage formation from sheep auricular chondrocytes cultured in vitro on fibrous collagen (type I collagen originating from bovine dermis; Kensey Nash Corporation, Exton, PA) scaffolds using various methods and for varying times before implantation has been evaluated in the concurrent studies by our laboratories in nude mice and in sheep. Robust neocartilage formation was demonstrated in all study groups after 6 weeks in vivo. However, fibrous collagen is soft and lacks the strength to withstand contraction forces exerted by skin and surrounding tissue during healing. Therefore, a permanent coiled titanium wire framework was embedded within the collagen scaffold to maintain the size and ear-like shape of the construct during neocartilage formation, scaffold remodelling, and exposure to wound healing forces. The results of this proof-of-concept study in immunocompromised mice are presented in this article.
Materials and Methods
Ear-shaped scaffold design and manufacture
Human ear-shaped scaffolds were fabricated for implantation on the back of a mouse. A single half size human adult ear master (28.2 mm×18.4 mm) was carved by hand in clay and used to create polydimethylsiloxane molds. Metal frameworks bent to mimic the shape of the human ear were made of 0.25–mm-diameter coiled titanium wire (Small Parts, Inc., Logansport, IN). Composite metal and collagen (fibrous bovine dermis-derived type I collagen) ear-shaped scaffolds were manufactured by Kensey Nash Corporation (Fig. 1). Metal frameworks were embedded in half of the collagen scaffolds; the remaining collagen scaffolds were manufactured without internal wire support. Scaffolds were sterilized with cold ethylene oxide gas before seeding with chondrocytes.
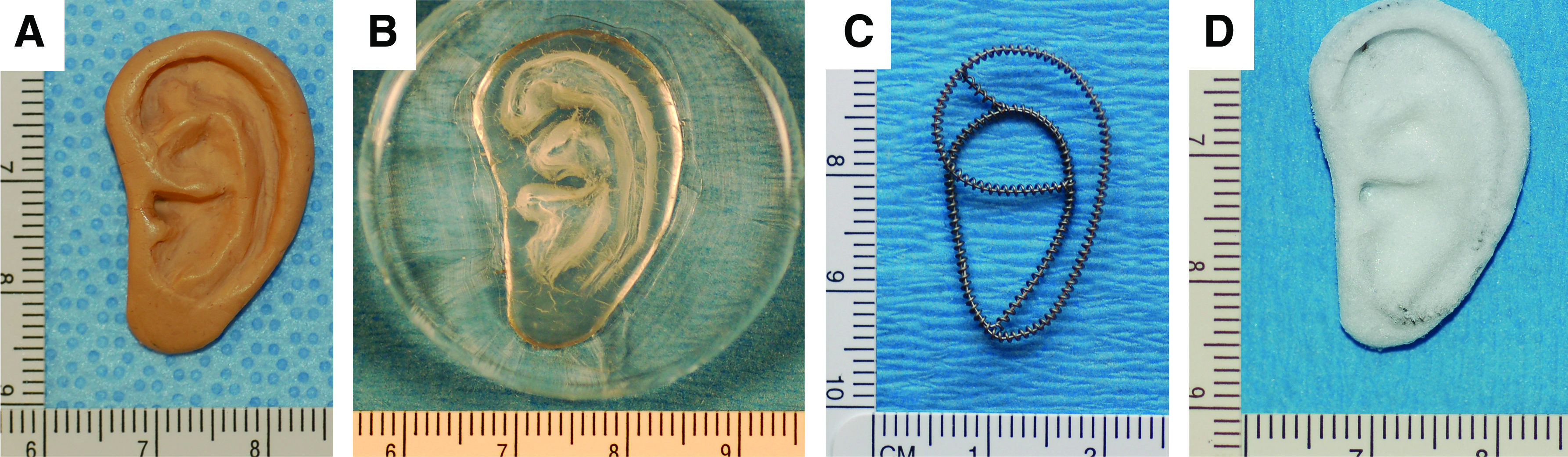
A half size human adult ear master was carved by hand in clay
Chondrocyte isolation and culture
Chondrocytes were isolated from auricular cartilage of 11-month-old Polypay sheep. Ear skin, subcutaneous tissues, and perichondrium were removed and discarded. Cartilage was minced into 1 mm3 fragments and digested with 0.1% collagenase type II (Worthington Biochemical Corporation, Lakewood, NJ) at 37°C for 16 h. Isolated chondrocytes were washed twice with phosphate-buffered saline; cells were counted using trypan blue and a hemacytometer and plated into roller bottles (Corning, Inc., Acton, MA) at 3×103 cells/cm2. Chondrocytes were cultured for ∼10 days in the culture medium, which consisted of Ham's F12 medium (Invitrogen, Grand Island, NY) supplemented with 10% FBS (Sigma-Aldrich, St. Louis, MO), 100 U/mL penicillin, 100 μg/mL streptomycin, 292 μg/mL L-glutamine (Sigma-Aldrich), 0.1 mM nonessential amino acids (Invitrogen), and 50 μg/mL ascorbic acid (Sigma-Aldrich). Upon reaching confluency, the chondrocytes were trypsinized with 0.05% trypsin–ethylenediaminetetraacetic acid and used for this study.
Cell seeding and construct culture
Chondrocytes were suspended in the culture medium at a concentration of 50×106 cells/mL. One milliliter of cell suspension was pipetted onto each scaffold and the cells were allowed to adhere for 3 h with the scaffolds flipped upside down every 20 min to facilitate more uniform distribution of cells. Constructs were cultured in six-well plates in 4 mL of the culture medium on the platform of an orbital RotoMix mixer (Krackeler Scientific, Inc., Albany, NY), which was rotating at 55 rpm 25 in standard incubator conditions (37°C and 5% CO2) for 2 or 14 days. The culture medium was changed twice a week.
Construct implantation
All procedures were approved by the Institutional Animal Care and Use Committee of the Massachusetts General Hospital and performed according to the National Institutes of Health Guidelines for the Care and Use of Laboratory Animals. Sixteen ear-shaped constructs, eight with wire support and eight without, were implanted subcutaneously on the backs of 6–8-week-old female athymic nude mice (Cox-7 Laboratories, Massachusetts General Hospital, Boston, MA), one construct per mouse. General anesthesia was achieved with intraperitoneal injection of 300–500 mg/kg tribromoethanol. Under aseptic conditions, a horizontal incision was performed 1.5 cm proximally from the base of the tail, and a subcutaneous pocket was created through blunt dissection. After insertion of the ear-shaped construct, the skin was closed with nonresorbable monofilament suture that was removed after 7 days. Additionally, in separate mice, four 5–mm-diameter discs were implanted to serve as acellular controls; these discs were punched out of a 2-mm-thick sheet of fibrous collagen identical to the ear-shaped scaffold material (Kensey Nash Corporation).
Gross evaluation and histology
The length and width of all constructs were measured with a sterilized digital calliper by three blinded observers at four time points: before seeding, after in vitro culture on days 2 or 14, and after 6 weeks in vivo.
The implants were harvested at 6 weeks and carefully dissected from the surrounding mouse tissue. For histological evaluation, full-thickness 5-mm-diameter biopsies were punched at three areas of constructs with wire; complete cross sections were obtained at the similar levels from the constructs without wire. Three full-thickness, 5-mm-diameter biopsies for biochemical testing were obtained from similar locations in both types of constructs. Samples for histology were fixed in 10% buffered formalin. Specimens for biochemical testing were snap-frozen and stored at −80°C until analyzed. To assess cartilage formation within wire coils, wires were carefully removed from the fixed tissue before paraffin embedding.
Paraffin-embedded specimens were sectioned at 8 μm. Sections were stained with hematoxylin and eosin; cartilage ECM formation was evaluated with safranin O, toluidine blue, and Verhoeff's elastic stains.
Immunohistochemistry
Tissue sections were pretreated with 1 mg/mL pepsin in Tris HCl (pH 2.0) for 15 min at room temperature, followed by peroxidase block and serum block from M.O.M. kit (Vector Laboratories, Inc., Burlingame, CA). Sections were incubated with mouse anti-human collagen type I antibody (Accurate Chemical & Scientific Corporation, Westbury, NY) or mouse anti-human collagen type II antibody (Developmental Studies Hybridoma Bank, Iowa City, IA) for 30 min. EnVision+ System Peroxidase kit (Dako, Carpinteria, CA) was used to identify the antigens; sections were counterstained with hematoxylin.
Quantitative DNA and ECM analyses
Frozen samples were weighed, minced, and digested with 10% proteinase K from tritirachium album (Sigma-Aldrich) at 56°C overnight; the DNA was extracted and purified with a Qiagen DNeasy kit (Qiagen, Inc., Valencia, CA) according to the manufacturer's instructions. Total DNA content was determined using a PicoGreen dsDNA assay. 26
For biochemical analysis, engineered constructs and native sheep ear cartilage specimens were minced and lyophilized for 24 h. The dehydrated specimens were weighed and digested with papain solution (125 μg/mL papain type III, 100 mM phosphate, 10 mM l-cysteine, and 10 mM ethylenediaminetetraacetic acid, pH 6.3) at 60°C for 16 h. Aliquots of these digests were assayed for glycosaminoglycan (GAG) and hydroxyproline (OH-proline) content. GAG content was measured spectrophotometrically using dimethylmethylene blue dye from the Blyscan Glycosaminoglycan Assay kit (Biocolor Ltd., Carrickfergus, United Kingdom) with chondroitin sulfate as a standard. 27 OH-proline content was measured in the aliquots of the same papain digests using Stegemann's hydroxyproline assay. 28 All samples and standards were analyzed in duplicate.
Statistical analysis
Construct size and biochemical analyses values are expressed as mean±standard deviation. Statistical analyses were performed using SPSS 11.0 (SPSS, Chicago, IL). Comparison of means was assessed by a one-way analysis of variance and the Tukey multiple comparison test (p<0.05 was considered significant).
Results
Gross evaluation and histological analyses
All animals survived until the predetermined endpoints; no extrusion of constructs or wire supports was observed during the study period. All implants maintained their original shape and resembled a human ear (Fig. 2).
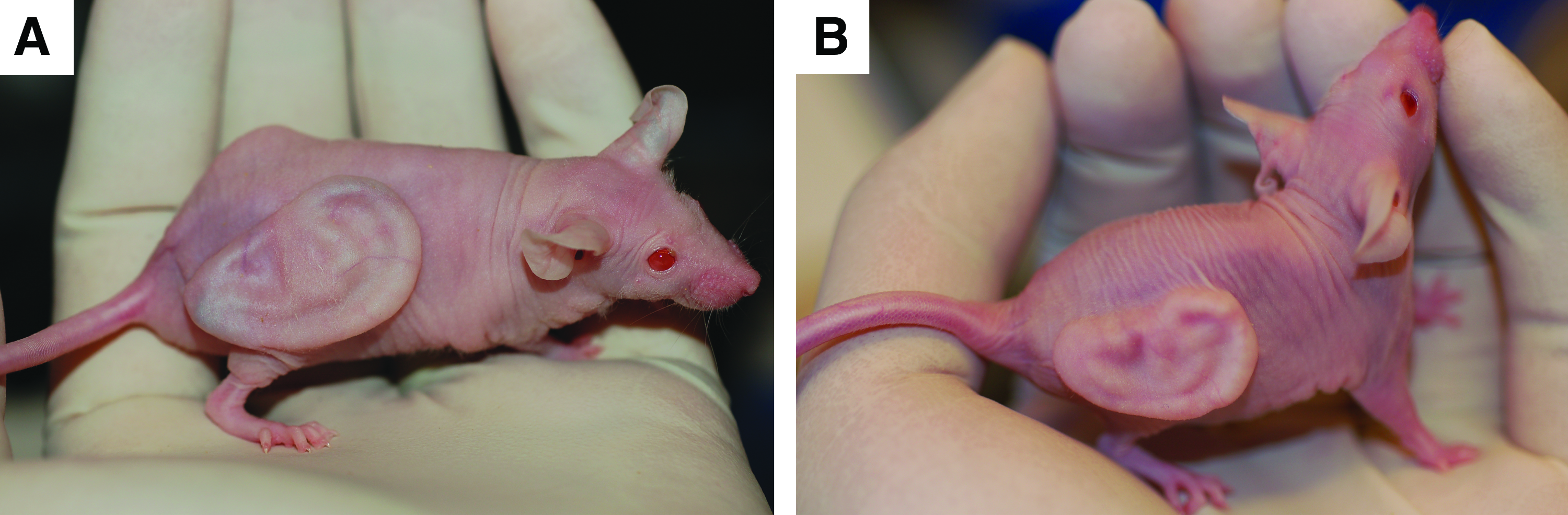
Human ear-shaped constructs with
During the 2-week in vitro culture, the constructs with wire support maintained their size while the constructs without wire support decreased in both length and width (Fig. 3). There was no considerable change in dimensions of either construct type during the 6 weeks in vivo. Construct size changes during the experiment are presented in Figure 4. Significantly less dimensional changes were observed in ear-shaped constructs with wire support than in constructs without wire support (p<0.05). Little changes in length and width were found in constructs with internal wire support (2.0% length and 4.1% width). Constructs without wire support initially swelled at 2 days in vitro but both dimensions decreased and remained smaller at the 6-week in vivo time point (14.4% length and 16.5% width).
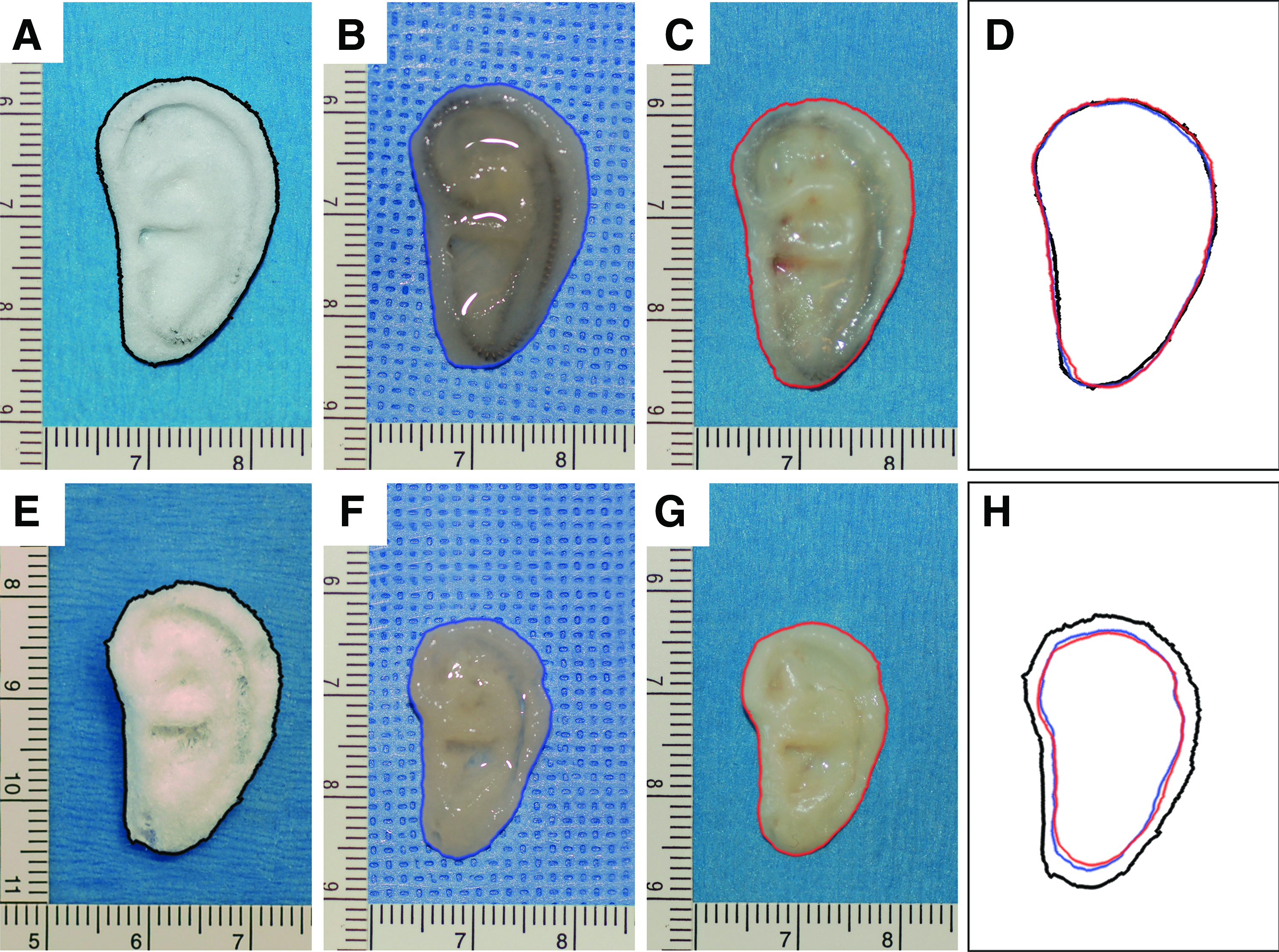
Gross images of ear-shaped constructs.

Construct size changes during the experiment. The length and width of the scaffolds containing wire supports
At 6 weeks postimplantation, all constructs were surrounded by a thin, fibrous capsule that could be easily removed. Grossly, the tissue resembled cartilage, and all ear-shaped constructs, both with and without internal wire support, were flexible (Fig. 5).

Demonstration of flexibility of ear-shaped constructs with internal wire support
The morphology of neocartilage was similar in ear-shaped constructs with and without internal wire support (Fig. 6). The chondrocytes in the newly formed tissue demonstrated similar morphologic characteristics to those seen in native sheep auricular cartilage and were located within evenly distributed ovoid lacunae. Collagen fibers of the scaffold were seen throughout the neocartilage ECM (Fig. 6A, E, I). Similarly, the neocartilage ECM, like native cartilage ECM, stained intensely with safranin O and toluidine blue, indicating the presence of abundant sulfated GAG (Fig. 6B, C, F, G, J, K). Weak positive staining for elastin was detected in the engineered cartilage in both types of constructs at the 6-week time point (Fig. 6D, H).
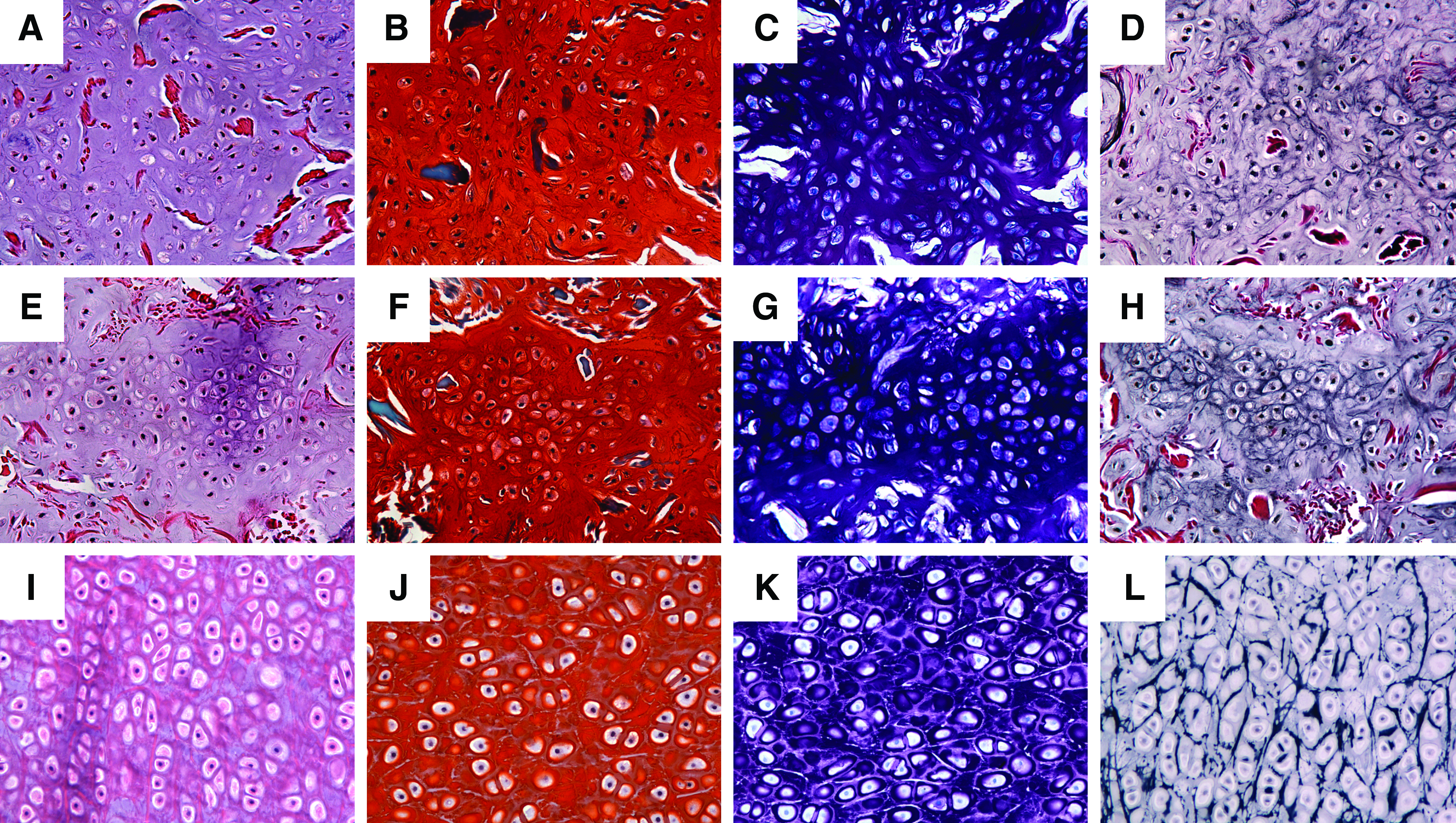
Histological appearance of engineered cartilage after 6 weeks in vivo was similar to that of native sheep ear cartilage.
A composite image of the cross section of the ear-shaped construct without wire (Fig. 7A) demonstrates cartilage ECM formation throughout the construct, as evidenced by safranin O staining. Small areas in the middle of the construct did not stain positively for cartilage ECM; some of those areas appeared to have densely packed scaffold fibers and low cellularity, some areas contained no scaffold fibers and were filled with loose connective tissue. In the cross section of the ear-shaped construct with wire, neocartilage formation was observed within the rings of the titanium coil of the internal wire support (Fig. 7B).

Composite image of the cross section of the ear-shaped construct without wire demonstrates neocartilage formation throughout the construct after 6 weeks in vivo
Immunohistochemistry
Cartilage-specific ECM was demonstrated in constructs, with and without wire support, as collagen type II was expressed in the ECM surrounding the chondrocyte ovoid lacunae (Fig. 8A, B). Collagen type II staining was more intense at the periphery and was less intense near the center of the constructs. Collagen type I was expressed at the surface of the both construct types (Fig. 8D, E). These collagen staining patterns are similar to that observed in native sheep ear cartilage (Fig. 8C, F). Collagen fibers of the scaffold (bovine collagen type I) did not stain for collagen type I, indicating the lack of species cross reactivity for this antibody.
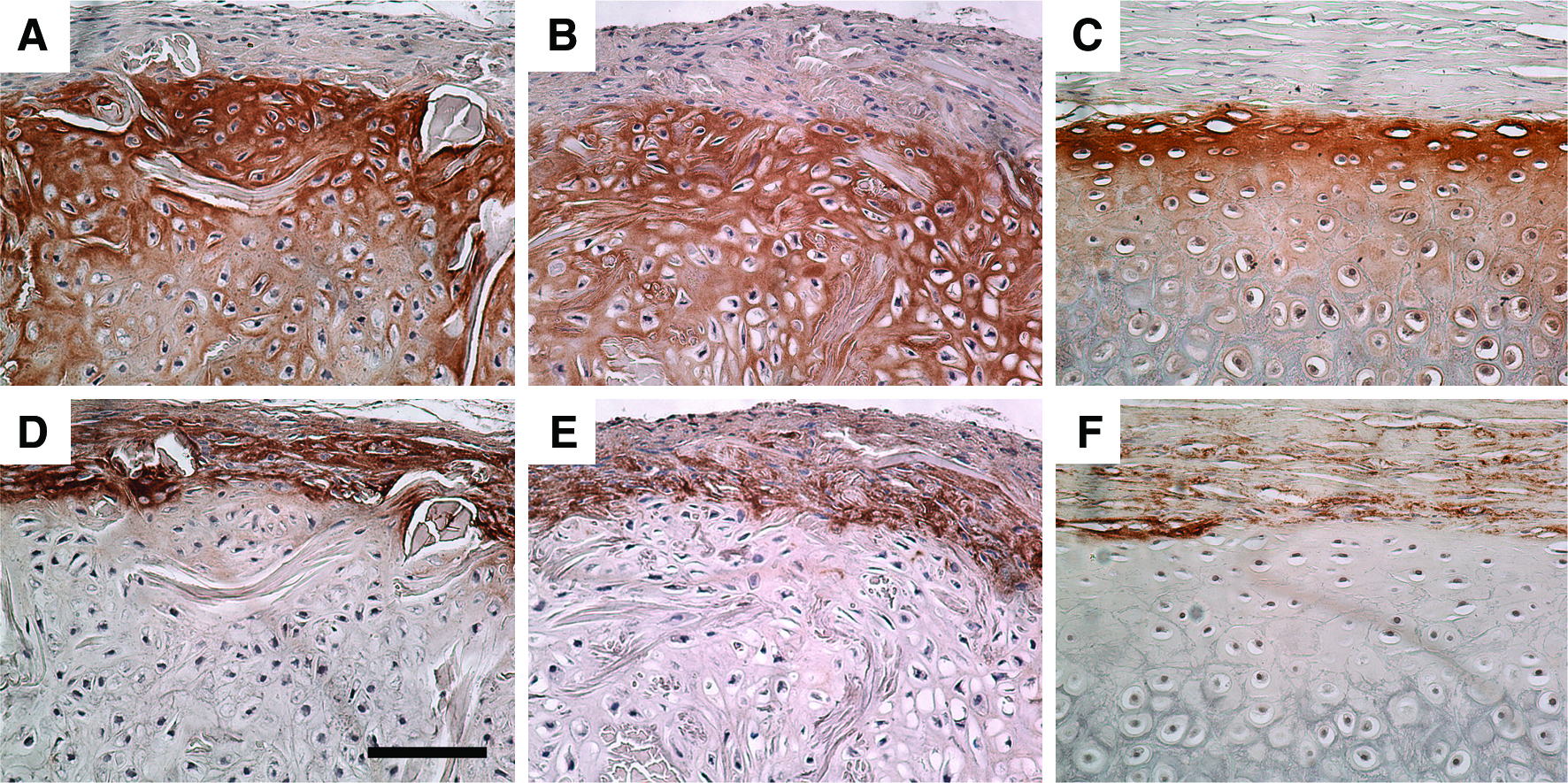
Immunohistochemical staining for collagen type II
Quantitative DNA and ECM analyses
The DNA content (Fig. 9) of engineered, ear-shaped constructs was similar in constructs with and without wire support (245.4±95.7 and 226.1±67.4 ηg/mg wet weight respectively) and similar to that of native sheep ear cartilage (147.2±18.6 ηg/mg, p>0.1). The DNA content of the control acellular scaffolds was low (79.1±9.2 ηg/mg, p<0.05) and could be attributed to the migration of mouse cells into the scaffold upon implantation. The amount of GAG in the constructs was similar: 127.4±61.5 and 122.1±43.6 μg of GAG/mg dry weight in constructs with and without wire support, respectively (p>0.1). The GAG content of engineered cartilage was similar to that of native sheep ear cartilage (133.4±18.1 μg/mg, p>0.1) and no GAG could be detected in the control acellular scaffolds. The amount of OH-proline was 89.5±12.7 and 93.3±19.8 μg/mg dry weight in the constructs with and without wire support, respectively (p>0.1). OH-proline content of ear-shaped engineered cartilage, both with and without wire support, was higher than that of the native sheep ear cartilage (50.2±3.4 μg/mg, p<0.05) and the acellular scaffold control (60.7±3.7 μg/mg, p<0.05). The higher amount of OH-proline in the engineered cartilage, as compared to native sheep auricular cartilage, can be attributed in part to the collagen material of scaffold, which has been digested along with the collagen of engineered cartilage ECM and possibly contributed to the overall OH-proline content. In the acellular scaffold control, OH-proline content is attributed mostly to the collagen of the scaffold material. After 6 weeks in vivo, however, no difference was detected between DNA, GAG, and OH-proline content of the constructs cultured in vitro for 2 days versus those cultured for 2 weeks before implantation (results not shown).

DNA, glycosaminoglycan (GAG), and hydroxyproline (OH-proline) content. Data are presented as mean±standard deviation. DNA is presented as ηg/mg construct wet weight, and GAG and OH-proline as μg/mg construct dry weight.
Discussion
Multiple efforts to engineer human ear-shaped cartilage have been hindered by the inability to retain the size and shape of the construct for the duration of in vivo studies.6,8,9,11,29–31 To preserve the specific shape of a human auricle, many approaches have been investigated including reinforcement of a scaffold with an additional synthetic polymer poly-L-lactic acid,4–6,8,10,12,13,32 use of temporary external stents,5,7,9 acrylic sheet, 12 and implantable external perforated mold. 30 In this study, we proposed a new strategy: reinforce the ear-shaped porous collagen scaffold with an internal titanium wire skeleton. A coiled titanium wire, bent to simulate the ridges of a human auricle, was embedded into porous collagen, thereby combining the advantages of the biological nature of collagen material and the mechanical properties of the titanium wire. Titanium has been demonstrated to be a biocompatible material and is used routinely in medical implants for numerous applications, including auricular replacement. 33
Our results demonstrate that the size and ear-like shape were preserved throughout the experiment in all implants with internal wire support. After the initial swelling, significant reduction in size occurred in constructs made of porous collagen alone; however, the human ear-like shape of the constructs was grossly preserved. The reduction in size occurred after 2 weeks of in vitro culture without any further reduction during subsequent 6 weeks in vivo. The shrinkage is possibly caused by the beginning of ECM formation. This finding corroborates the assessment of the Kensey Nash multiphasic composite scaffold for osteochondral defect repair; the authors observed slight contraction of the cell-seeded collagen layer after 3 weeks of in vitro culture. 34 The lack of further reduction in size during the in vivo period may be attributed to rather loose subcutaneous connective tissue in rodents and the reduced inflammatory response in immunocompromised nude mice as evidenced by the formation of a thin fibrous capsule. In a large animal model, stronger contraction forces are expected to be exerted by skin and surrounding tissue during healing, approximating conditions in humans.
Our results suggest that the internal wire framework was essential for the preservation of the dimensions of the engineered ear during in vitro culture and after implantation into the animal model. Titanium wire was well incorporated into the neocartilage, without any adverse effects on chondrocyte viability, adhesion to scaffold material, and cartilage ECM formation, suggesting low possibility of extrusion in the future. Histologically, we found no difference between neocartilage that formed in the constructs with and with out internal wire support. Weak elastin expression was observed in both types of constructs after 6 weeks in vivo, suggesting that elastic cartilage started to form at this early time point.
We were unable to identify any differences between the cartilage that formed in nude mice after 2 days and 2 weeks of in vitro culture before implantation. However, in a large animal model, in vitro preculture is important to achieve autologous cartilage formation before implantation. Such an approach may help reduce the inflammatory and foreign body response that can be induced by a scaffold made from collagen originating from a different species and by antigen-presenting chondrocyte surface in an immunologically active subcutaneous environment. 35
Staining of the cross sections obtained from the ear-shaped implants without wires with safranin O demonstrated a few areas in the center of the constructs that did not show the presence of cartilage-specific GAG (Fig. 7A). Some of these staining defects appeared to have lower cellularity and may be due to scaffold production artifacts such as uneven distribution of collagen fibers within the scaffold or air bubbles. On the other hand, the thickness of the constructs often exceeded 3 mm, which might have negatively affected chondrocyte survival in the central part of the constructs due to limited nutrient and gas diffusion. We are currently modifying the design of the ear-shaped scaffold to reduce the thickness of engineered cartilage so that it more closely resembles human auricular cartilage; this thickness reduction should eliminate this central defect if it is related to construct thickness.
In this study, auricular cartilage was engineered and the size of the human ear-like construct was retained with the help of the internal titanium wire framework. The embedded wire support was essential for avoiding shrinkage of the ear-shaped porous collagen constructs. Engineering human ear-shaped cartilage with preserved dimensions represents an important milestone in our translational program to develop a replacement living auricle for patients with congenital and acquired external ear defects. The improved composite scaffold will become a viable asset for future clinical applications and serve as an initial step in the development of a fully resorbable ear-shaped scaffold.
Footnotes
Acknowledgments
This research was sponsored by the Armed Forces Institute of Regenerative Medicine award number W81XWH-08-2-0034. The U.S. Army Medical Research Acquisition Activity, 820 Chandler Street, Fort Detrick MD 21702-5014, is the awarding and administering acquisition office. The content of the article does not necessarily reflect the position or the policy of the Government, and no official endorsement should be inferred. Dr. Libin Zhou was sponsored by China Scholarship Council for his study in Massachusetts General Hospital.
Disclosure Statement
No competing financial interests exist.