
Abstract
The current study's purpose was to evaluate the safety and biological effect of a scaffold-based three-dimensional human dermal fibroblast culture (3DFC, also known as Anginera™) to treat chronically ischemic canine hearts. It was hypothesized that treatment with 3DFC would be safe and significantly improve ventricular performance and wall motion. In this study, chronic myocardial ischemia was induced in 40 animals through the surgical placement of an ameroid constrictor. Approximately 30 days after ameroid placement, animals were randomized into four test groups: (1) sham treatment, (2) one unit of acellular 3DFC, (3) one unit of viable 3DFC, and (4) three units of viable 3DFC. Animals were necropsied 30 or 90 days after treatment. Evaluation of the safety endpoint demonstrated the safety of 3DFC at all dosing levels and at both time points. Additionally, parameters of cardiac output, left ventricular ejection fraction, left ventricular end systolic volume index, and systolic wall thickening support the conclusions that 3DFC stimulates a positive biologic effect on ischemic canine hearts. Further, these data support the conclusion that treatment with viable 3DFC improves ventricular performance and ventricular wall motion in chronically ischemic canine hearts 30 days after treatment.
Introduction
The three-dimensional human dermal fibroblast culture (3DFC) cardiac patch is a tissue-engineered human dermal fibroblast-derived therapeutic that has been used for the repair of chronic foot ulcers. 12 It contains structural extracellular matrix proteins and viable cells that synthesize a number of angiogenic growth factors (including VEGF, bFGF, and hepatocyte growth factor) and has been shown to stimulate angiogenic activity. 13 The safety and efficacy of the 3DFC cardiac patch has been extensively evaluated in a variety of preclinical animal models in various laboratories. A summary of current findings is summarized in Table 1. Early investigation on the effects of 3DFC treatment was first explored in the severe combined immunodeficient (SCID) mouse model. Statistically significant increases in microvessel density were reported in these studies along with findings that indicate the development of new arterioles (via arteriogenesis) within the infarcted myocardium. 14 Within the SCID mouse model, 3DFC was shown to provide functional benefits to the hearts with significantly higher ejection fraction and preload recruitable stroke work values in mice treated with 3DFC versus infarct-only controls. 15 Additionally, in these studies normal SCID mice (noninfarcted controls) were treated with 3DFC to evaluate if any safety issues were detectable when evaluating cardiac function or histopathology results. No safety issues were discovered. Next, the normal Sprague-Dawley rat model was used to evaluate the biological benefits and efficacy of 3DFC. First, an acute model in the rat was used, followed by a rat model of chronic heart failure. These studies were conducted in a collaborative laboratory under the guidance of a new investigator. The findings in the SCID mouse studies were confirmed in the rat model, with a fully functioning immune system. These studies reported 3DFC to stimulate angiogenesis, improved cardiac function, and improved cardiac remodeling. Additionally, increases in myocardial blood flow were seen as a result of 3DFC treatment. 16 The second rat study used a well-established model of chronic heart failure where a coronary ligation was first performed, the animal recovered, and incubated for 3 weeks. During this time, cardiac function of the hearts diminished. At the 3-week time point, the chest was re-entered and 3DFC applied in the treated group. In these studies, 3DFC also increased angiogenesis, increased myocardial blood flow, and increased ventricular wall thickness. 17 In other studies using the Lewis rat model of acute infarction, 3DFC treatment was reported to improve microvascular perfusion, increase wall thickness, lead to smaller infarct areas, and preserve overall cardiac function. 18
3DFC, three-dimensional human dermal fibroblast culture.
Finally, a Good Laboratory Practice (GLP) preclinical canine study was completed to primarily evaluate the safety of using 3DFC to treat chronic ischemic hearts. Parameters of efficacy were also evaluated in this study to demonstrate evidence of the biologic effect that has been seen in the numerous small animal studies. It was hypothesized that treatment with 3DFC would significantly improve ventricular performance and wall motion in these hearts after treatment. Finally, as part of this GLP study, echocardiography data were collected and analyzed to evaluate the effect of 3DFC on regional and global left ventricular function.
In the current study, evaluation of the primary safety endpoints (including hemodynamic, electrocardiographic, echocardiographic, and clinical and gross pathology observations) demonstrated the safety of 3DFC at all dosing levels and at both time points. Echocardiography data were collected, and general findings were reported, which suggest an improvement in ventricular function of ischemic hearts treated with 3DFC. Additionally, a separate analysis of heart histology was conducted to confirm evidence of new microvessel formation. Finally, a separate blinded echocardiography analysis, performed on the original echocardiography data, focused on statistical comparisons of key outcome measures that were identified to be most clinically relevant. This analysis indicated statistically significant improvements in ventricular performance and ventricular wall motion in chronically ischemic canine hearts 30 days after treatment.
Materials and Methods
This study was conducted in compliance with the Food and Drug Administration GLP regulations. After completion of the GLP study, additional histologic and echocardiographic studies were performed.
Chronic myocardial ischemia was induced in 40 animals (four groups of five male and five female mongrel dogs) through the surgical placement of an ameroid constrictor on the ventral interventricular branch of the left anterior descending coronary artery. Approximately 30 days (±2 days) after the surgical placement of an ameroid constrictor, the animals received one of four treatments (Group 1: sham surgical treatment; Group 2: surgical application of one unit of acellular 3DFC; Group 3: surgical application of one unit of viable 3DFC; Group 4: surgical application of three units of viable 3DFC). These treatment groups were selected based on previous published work14–17 and direct FDA input. Acellular 3DFC patches are nonviable patches, where patches were subjected to a standardized freeze–thaw cycle to lyse cells. This renders the patch acellular and nonviable to serve as a control for any contribution by the patch alone. All investigators performing tests or analyzing data were blinded as to the identity of an animal's treatment. Two animals per sex were necropsied on day 30 (±1 day), and three animals per sex from each treatment group were necropsied on day 90 (±1 day) (Table 2).
On day −30 (±2 days), all animals had placement of an ameroid constrictor on the left anterior descending coronary artery. The actual treatment group identity of each individual animal was coded.
Group 1=ischemia only, Group 2=acellular 3DFC, Group 3=single 3DFC treatment, Group 4=three-piece 3DFC treatment.
Safety evaluations
Safety was assessed by evaluating clinical observations, physical and ophthalmic examinations, body weights, body temperatures, cardiac monitoring (including electrocardiography [ECG], arterial blood pressure, heart rate, and echocardiographic determination of left ventricular function), clinical pathology (including hematology, coagulation, serum chemistry, Troponin T, and urinalysis), anatomic pathology, and histopathology of selected organs and tissues (including adrenal glands, aorta, bone marrow, brain, esophagus, eyes, reproductive tissues, femur, gallbladder, heart, intestine, kidneys, liver, lungs, lymph nodes, pancreas, para thyroid glands, pituitary glands, salivary glands, sciatic nerve, skeletal muscle, skin, spinal cord, spleen, stomach, thymus, thyroid glands, tongue, trachea, and urinary bladder). Additional evaluation of the echocardiography data from all treatment groups at both the day 30 and 90 time points was performed. Finally, a separate analysis of heart histology was performed.
Echocardiography evaluations
Echocardiograms were collected within 4 weeks before day −30, approximately 8 days before day 1, and approximately 8 days before sacrifice/necropsy (day 30 or 90). Trans-thoracic resting and stress echocardiography were performed using methods to standardize echocardiographic windows and views. Echocardiographic evaluation was performed after the animals had achieved a stable heart rate followed by a second echocardiographic examination under dobutamine-induced increased heart rate. Dobutamine was administered intravenously starting at 5 μg/kg/min and titrated to a maximum infusion rate of 50 μg/kg/min to achieve 50% increase in heart rate (±10%). Animal ID numbers (blinding animal treatment group), study dates, and views were annotated on the video recording of each study. Segmental contractility, measured as wall thickening (in cm), was quantified in the ischemic region and the control region of the left ventricle. These measurements were performed in three cross-sectional planes to include basal plane, mid papillary plane, and a low-papillary plane. Left ventricular dimensional measurements were taken from 2D images. Two-chambered and four-chambered long axis images were recorded for the determination of left ventricular volumes, ejection fraction, and cardiac output (CO). The mathematical model for this determination was the biplane, modified Simpsons approximation. Electrocardiograms were recorded coordinate with the echocardiography. Images saved to optical disc were stored in a DICOM image format for review in chronological order of the study by at least one Board-certified veterinarian cardiologist, blinded as to the identity of the samples. Three measurements were performed on all echocardiographic data and reported as a mean of the three measurements. Statistical significance was determined using analysis of variance and t-tests where appropriate (p<0.05).
A separate echocardiography analysis performed on the original echocardiography data focused on statistical comparisons of key outcome measures that were identified to be most clinically relevant. One-way analysis of variance was used to determine a significant difference (p<0.05) between treatment groups. Comparisons were made between and within groups with specific focus on parameter changes under resting conditions versus dobutamine-stress conditions at both the 30 and 90 day time points.
Results
Canine model evaluation
No animals were observed during the baseline preameroid echo evaluation with significant left ventricular dysfunction or congenital heart disease. At baseline resting conditions all animals were within normal species ranges for hemodynamic values and wall dimensions. These data demonstrate that animals from all groups began the study with normal range values of left ventricular function. Further, pretreatment, postameroid left ventricular wall dimensions demonstrated a blunted response to dobutamine stress at the basilar (mitral valvular), high papillary, and low papillary levels in comparison to the preameroid baseline assessment, demonstrating diminished wall function in the anterior and lateral wall of the left ventricle. These pretreatment, postameroid echo observations are consistent with the ameroid experimental model that resulted in mild left ventricular dilation secondary to ventricular ischemia, and demonstrate that the ameroid canine model used in this study was successful at creating ventricular ischemia measurable by echocardiography.
Results of safety evaluations
After the day 1 surgical application of treatment, no animal deaths were observed during the in-life phase of the study.
Clinical observations common to the surgical procedures associated with the exposure of the heart via thoracotomy (ameroid placement) or sternotomy (3DFC placement) were observed (e.g., swelling, erythema, open incisions, and abrasions). The distribution and frequency of these clinical observations before day 1 was similar between the final treatment groupings. After the day 1 surgical administration of treatment, clinical observations were similar between the four treatment groups. Ophthalmologic examinations, physical examinations, body weights, body temperatures, hematology, coagulation, serum chemistry, Troponin T, urinalysis, surgical hemodynamic/cardiovascular monitoring, and weekly cardiovascular monitoring were all evaluated to be within normal species ranges and were not different between the four groups of animals. Collectively, these data demonstrate the safety of 3DFC at all dosing levels within the parameters evaluated. Qualitative evaluation of the ECGs demonstrated normal cardiac rhythms for all but three animals (two Group 2 animals and one Group 3 animal). The arrhythmias or conduction disturbances observed in these three animals were evaluated to be either normal variants in dogs or a temporary residual effect associated with surgery and manipulation of the heart during surgical placement of the 3DFC onto the myocardial surface.
Gross macroscopic pathology observations were limited to numerous myocardial adhesions (between the heart and the pericardium and the pericardium and the lungs or chest wall) and nodular lesions or discolorations in the myocardial tissue surrounding the ameroids. No differences were detected in the frequency or intensity of these observations among the four treatment groups of animals. These types of gross observations are consistent with the surgical procedures utilized in this experimental protocol (i.e., thoracotomy and sternotomy).
Transmural infarction was not observed in any of the tissue samples examined. Overall, no trends in the incidence or severity of infarction could be associated with specific treatment at the day 30 or 90 evaluation time points.
In summary, evaluation of the primary safety endpoints demonstrated the safety of 3DFC at all dosing levels and at both time points.
Results of histology evaluation
Evaluation of heart histology was performed to identify evidence of new microvessel formation. These findings confirm previously reported and published findings of new microvessel formation with the presence of a mature microvasculature (arterioles, venules, and capillaries) after treatment with 3DFC (Fig. 1).
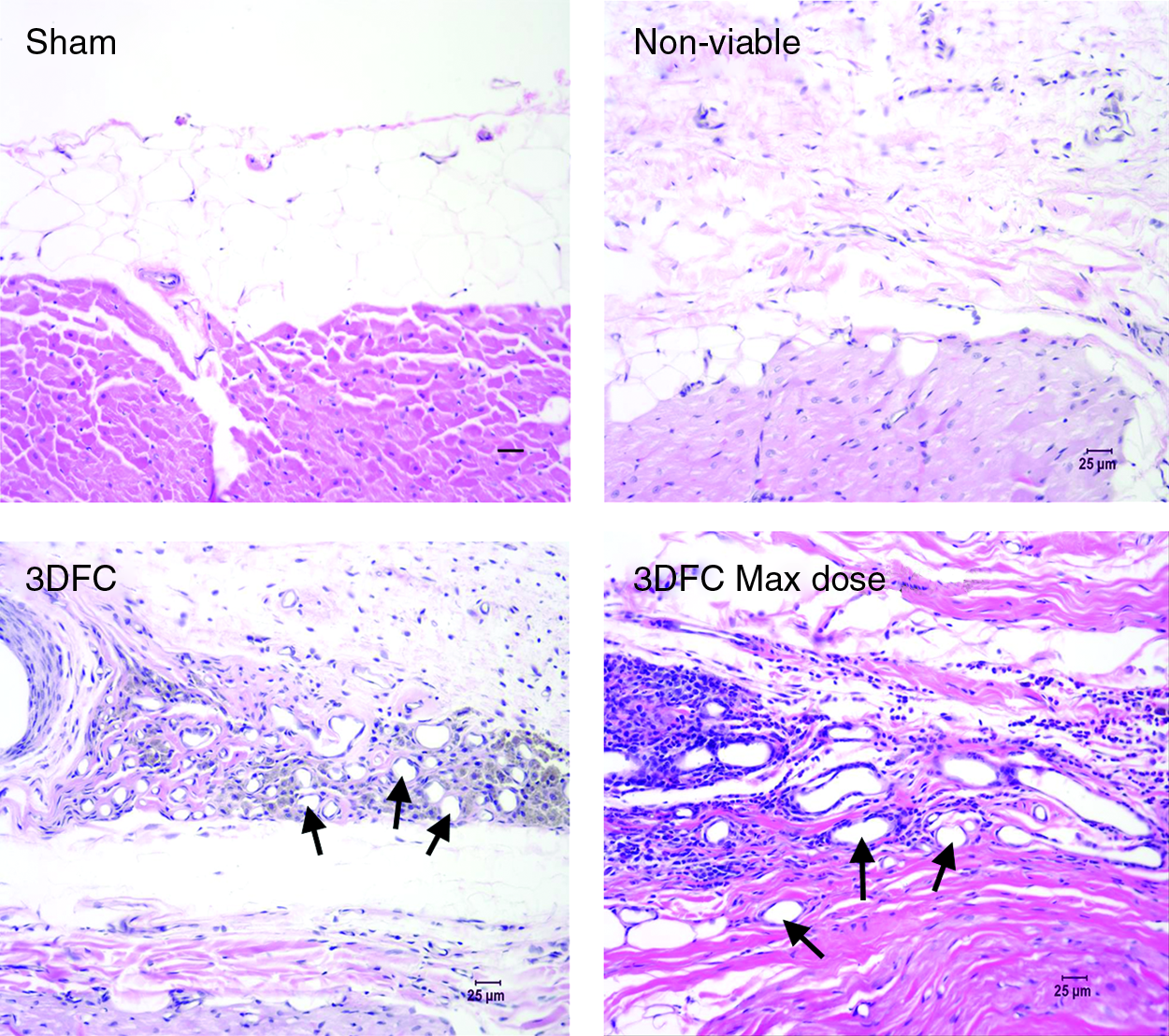
Representative heart histology from canine study. Hematoxylin and eosin-stained sections reveal evidence of new microvessel formation in the tissue surrounding Anginera (3DFC). Scale bars=25 μm. Arrows indicate new microvasculature. 3DFC, three-dimensional human dermal fibroblast culture.
Hematoxylin and eosin-stained sections from the canine GLP study were further analyzed. This evaluation was performed to specifically evaluate the cellular infiltrate in association with 3DFC and the epicardial tissue. Therefore, this analysis was performed on tissues that were in direct contact with the 3DFC material.
Conclusions from this histology analysis include the following observations:
1. Scarring indicative of subendocardial ischemic damage was seen in all groups. 2. Group 1 (ischemia only) specimens showed minimal focal pericardial thickening without inflammation. 3. Group 2 (acellular 3DFC) implants had diffused, mild, and focally increased pericardial thickening with minimal inflammation and focal mesothelial proliferation. 4. Groups 3 (single dose 3DFC) and Group 4 (three pieces of 3DFC) had fibrous pericardial thickening with varying amounts of moderate, focal, multifocal, or band-like inflammation between the patch and the epicardium, and focal foreign body reaction (most associated with sutures). 5. Less inflammation was seen at 90 than at 30 days. 6. No definitive evidence of immunological reaction was seen. 7. In no case was there inflammation involving the myocardium. 8. Increased vasculature was seen focally in areas of pericardial inflammation.
These histopathologic evaluations demonstrated no definitive evidence of an immunologic reaction to 3DFC. There was a transient inflammatory response observed in all four treatment groups associated with the experimental conditions. In the viable 3DFC groups there was evidence of a cellular response, which included an increase in microvasculature specific to the epicardium and pericardium. There was no evidence of a localized fibrosis, associated with the treatment, in the epicardium or myocardium that might lead to arrhythmias. The infiltrates had the morphologic appearance of macrophagic rather than lymphocytic cell types.
Results from echocardiography evaluations
Global functional assessment
Prenecropsy echocardiographic assessment demonstrated dose-dependant decreases in left ventricular chamber volumes. Resting stroke volume and CO indices were decreased in Group 3 (one unit dose 3DFC), but these mild decreases normalized in response to dobutamine infusion. Resting stroke volume and CO indices decreased in Group 4 (three unit dose 3DFC), whereas decreases in left ventricular chamber volumes were marked compared with pretreatment values and were diminished over baseline values. These changes were more dramatic in Group 4 than in Group 3. The response to dobutamine infusion in terms of percent difference in Group 4 was better than that seen in baseline values. Stroke volume and CO indices did not return to normal baseline values, but trended to near-normal baseline values.
Specifically, Group 3 animals (one unit dose 3DFC) at the 30-day prenecropsy time point had larger left ventricles than Group 3 animals at the 90-day prenecropsy time point or Group 4 animals (three units dose 3DFC) at either the 30- or 90-day prenecropsy time point. Group 4 animals had smaller left ventricles than Group 1, 2, or 3 animals. Compensatory mechanisms in and of themselves cause a decrease in left ventricular size (volume) as was seen in Group 1 (untreated animals) and Group 2 (acellular 3DFC treated) animals. However, the fact that the left ventricular volumes were actually smaller in Group 4 animals than in Group 1, 2, or 3 animals suggests a positive treatment effect. Decreases in left ventricular sizes/volumes are at least in part responsible for the decreases in stroke volume index and CO index. These decreases returned both cardiac output index and stroke volume index to values similar to or better than normal baseline values that were also improved compared to the pretreatment values. The most improved function compared with pretreatment values was in Group 4 animals at the 90-day prenecropsy time point.
Echocardiography evaluations
A comprehensive secondary evaluation, performed on the original raw data, focused on specific statistical comparisons of clinically relevant echocardiographic parameters. The general findings of the primary echo evaluation and the specific findings of the secondary echocardiography evaluation support each other. In addition, CO, left ventricular ejection fraction (LVEF), left ventricular end systolic volume index (LVESVI), and systolic wall thickening (SWT) support the conclusions that 3DFC stimulates a positive biologic effect on ischemic hearts of this canine model.
Cardiac output: After 30 days of treatment, dogs in the acellular, single, and multiple 3DFC patch groups showed a significant (p<0.05) improvement in CO with dobutamine (4273±450, 4238±268, and 4144±236 mL/min, respectively) compared to their baseline, resting CO. The sham surgical group did not significantly improve its CO with dobutamine infusion. Further, the animals with multiple patch treatment (Group 4) demonstrated the greatest improvement in CO with dobutamine infusion (Fig. 2). However, at 90 days all dogs improved their CO with dobutamine, including the sham operated animals (Fig. 3). CO was expected to increase from resting to stress conditions. It is expected that diseased hearts would demonstrate a compromised ability to increase CO under dobutamine-stress conditions. These data suggest that dogs treated with acellular, single, and multiple pieces of 3DFC had a better CO response to dobutamine than the control sham group at 30 days. By 90 days, all groups performed statistically equivalent to each other.
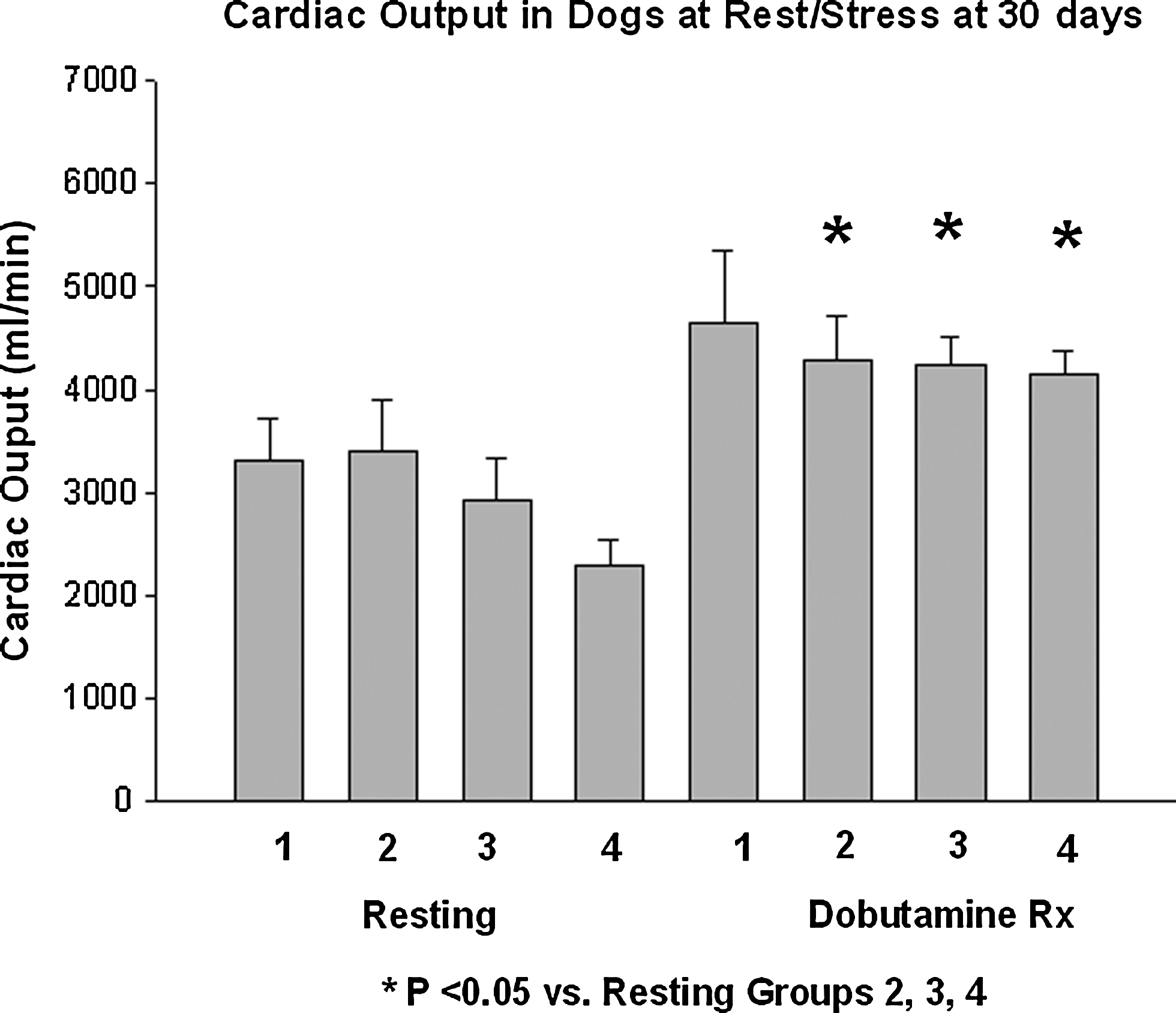
Cardiac output values under resting and stressed conditions (dobutamine treated) in all treatment groups at the 30 day. Group 1=ischemia only; Group 2=acellular 3DFC; Group 3=single 3DFC treatment; Group 4=three-piece 3DFC treatment.
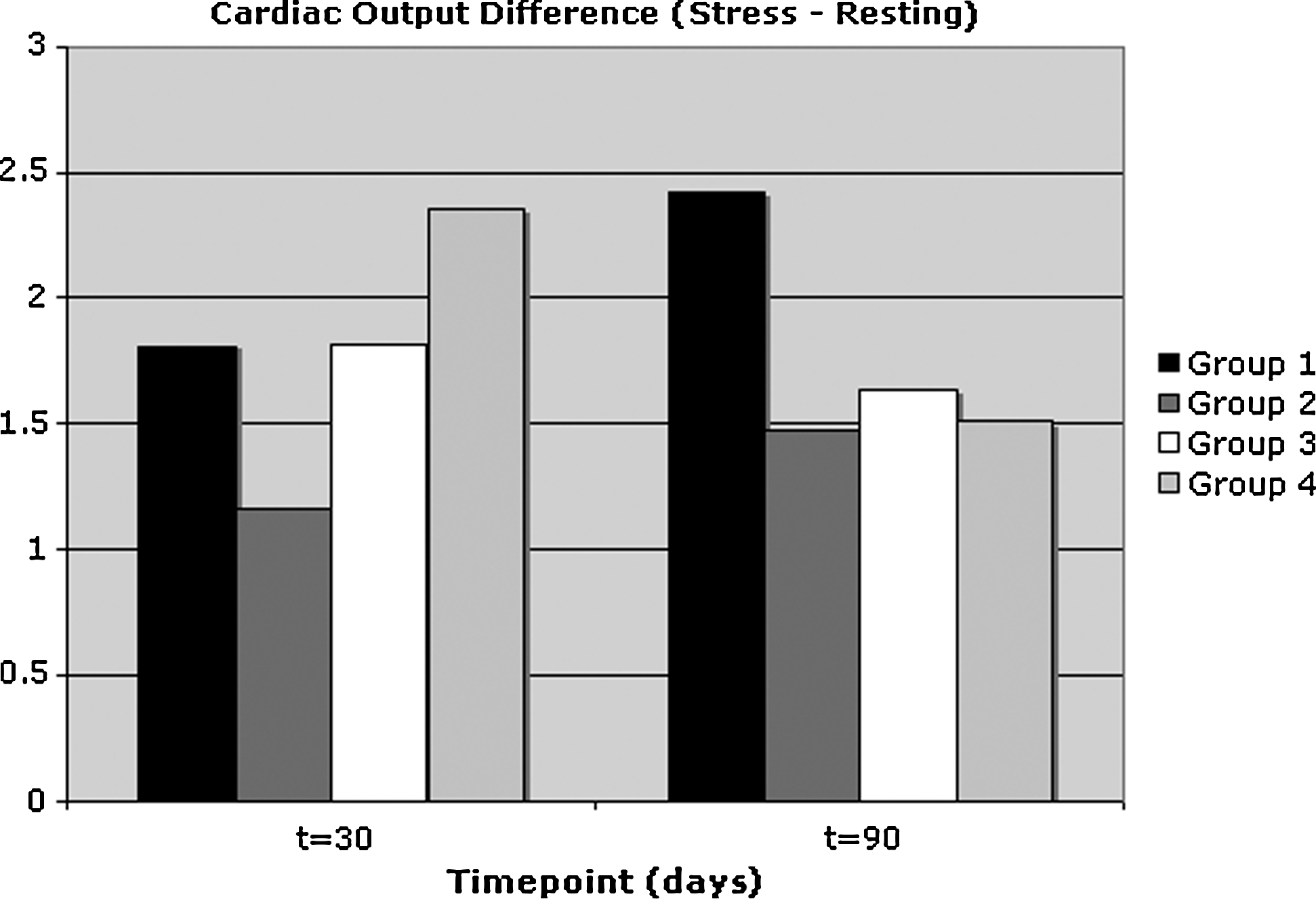
Cardiac output difference between resting and stressed conditions (dobutamine treated) in all treatment groups at the 30 day 90 day time points. Group 1=ischemia only; Group 2=acellular 3DFC; Group 3=single 3DFC treatment; Group 4=three-piece 3DFC treatment.
Left ventricular ejection fraction: LVEF demonstrated a similar stress response to dobutamine as CO at 30 and 90 days (Figs. 4 and 5). Specifically after 30 days of treatment, dogs in the acellular (Group 2), single, and multiple 3DFC patch groups (Groups 3 and 4) showed a significant (p<0.05) improvement in LVEF with dobutamine compared to their baseline, resting LVEF. The sham surgical group (Group 1) did not significantly improve its LVEF with dobutamine infusion. However, at 90 days all dogs improved their LVEF with dobutamine, including the sham operated animals. These data suggest that dogs treated with acellular, single, and multiple pieces of 3DFC had a better LVEF response to dobutamine than the control sham group at 30 days. Further, at 30 days the percent increase of EF values from baseline to dobutamine-stress conditions was most notable in the acellular, single, and multiple pieces of 3DFC: 17%, 23%, and 42%, respectively (Fig. 6).
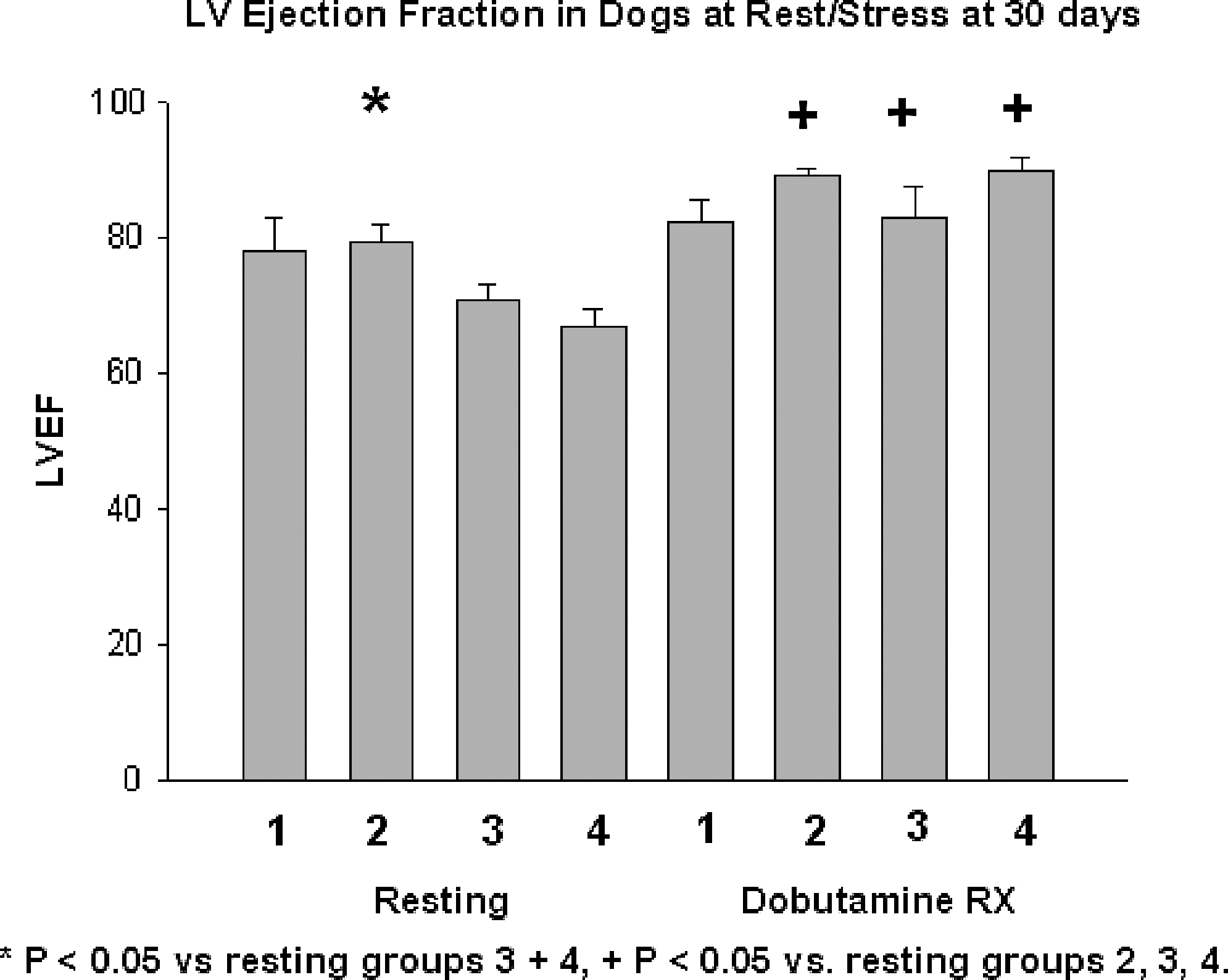
Ejection fraction values under resting and stressed conditions (dobutamine treated) in all treatment groups at the 30 day. Group 1=ischemia only; Group 2=acellular 3DFC; Group 3=single 3DFC treatment; Group 4=three-piece 3DFC treatment.

Ejection fraction difference between resting and stressed conditions (dobutamine treated) in all treatment groups at the 30 and 90 day time points. Group 1=ischemia only; Group 2=acellular 3DFC; Group 3=single 3DFC treatment; Group 4=three-piece 3DFC treatment.

Percent ejection fraction value increase from baseline (stress vs. dobutamine) at 30 days. Group 1=ischemia only (sham); Group 2=acellular 3DFC; Group 3=single 3DFC treatment; Group 4=three-piece 3DFC treatment.
Left ventricular end diastolic volume: The left ventricular end diastolic volume (LVEDV) index was measured at rest and during stress in all groups at 30 and 90 days. At rest the LVEDV index was similar in all groups at 30 and 90 days. However, during stress at 90 days there is a significant (p<0.05) decrease in LVEDV index at the highest 3DFC dose (Group 4). Therefore, the result of Group 4 animals at 90 days under dobutamine stress having significantly lower LVEDV index values suggests that the maximum treatment group (three pieces of 3DFC) provides additional benefit to the ischemic heart. With progression of heart failure, one would expect increased LVEDV. As shown in Figure 7, the LVEDV difference between resting and stress decreases in Groups 2, 3, and 4, while increasing in the untreated Group 1.
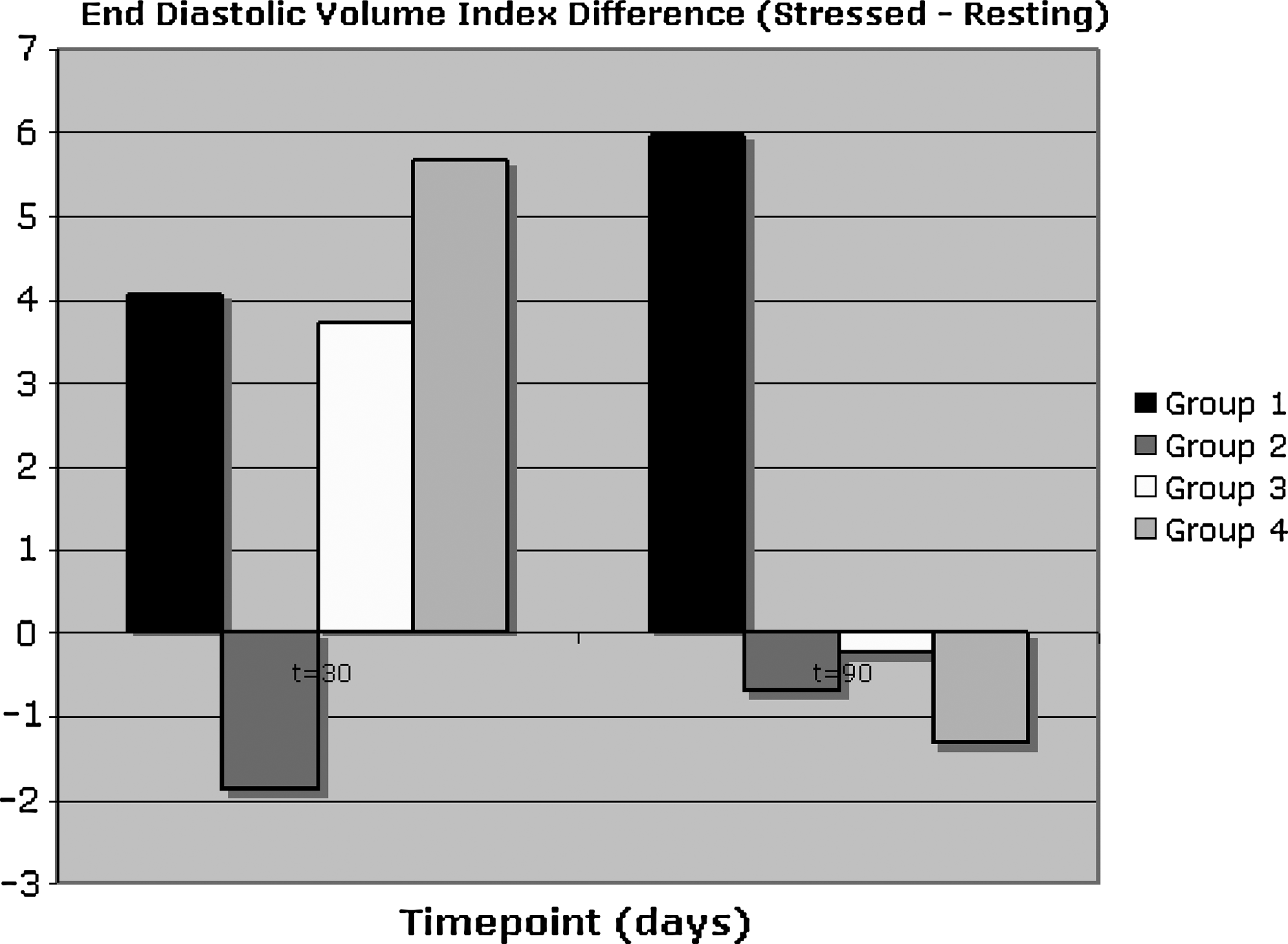
Difference left ventricular end diastolic volume index (stressed – resting) at the 30 and 90 day time points. Group 1=ischemia only; Group 2=acellular 3DFC; Group 3=single 3DFC treatment; Group 4=three-piece 3DFC treatment.
Left ventricular end systolic volume index: Consistent with the data from LVEF and CO, LVESVI values also significantly decreased with either viable or acellular 3DFC at stress compared to baseline at 30 days. At 90 days, there was also an improvement in the LVESVI with the sham surgery animals. These data suggest that dogs treated with acellular, single, and multiple pieces of 3DFC had a better LVESVI response to dobutamine than the control sham group at 30 days (Fig. 8).

Left ventricular end systolic volume index difference (stressed – resting) in all treatment groups at 30 and 90 day time points. Group 1=ischemia only; Group 2=acellular 3DFC; Group 3=single 3DFC treatment; Group 4=three-piece 3DFC treatment.
Systolic wall thickening
During the early ischemia period (30 days), dobutamine increased (p<0.05) SWT in all four groups; however, there appears to be a dose-dependent relationship since the most significant increase in SWT occurred in dogs that had the three patches of 3DFC (Group 4) implanted (Fig. 9). Furthermore, at 30 days the percent increase of SWT values from baseline to dobutamine-stress conditions was most notable in the single and multiple pieces of 3DFC: 55% and 144%, respectively (Fig. 10).
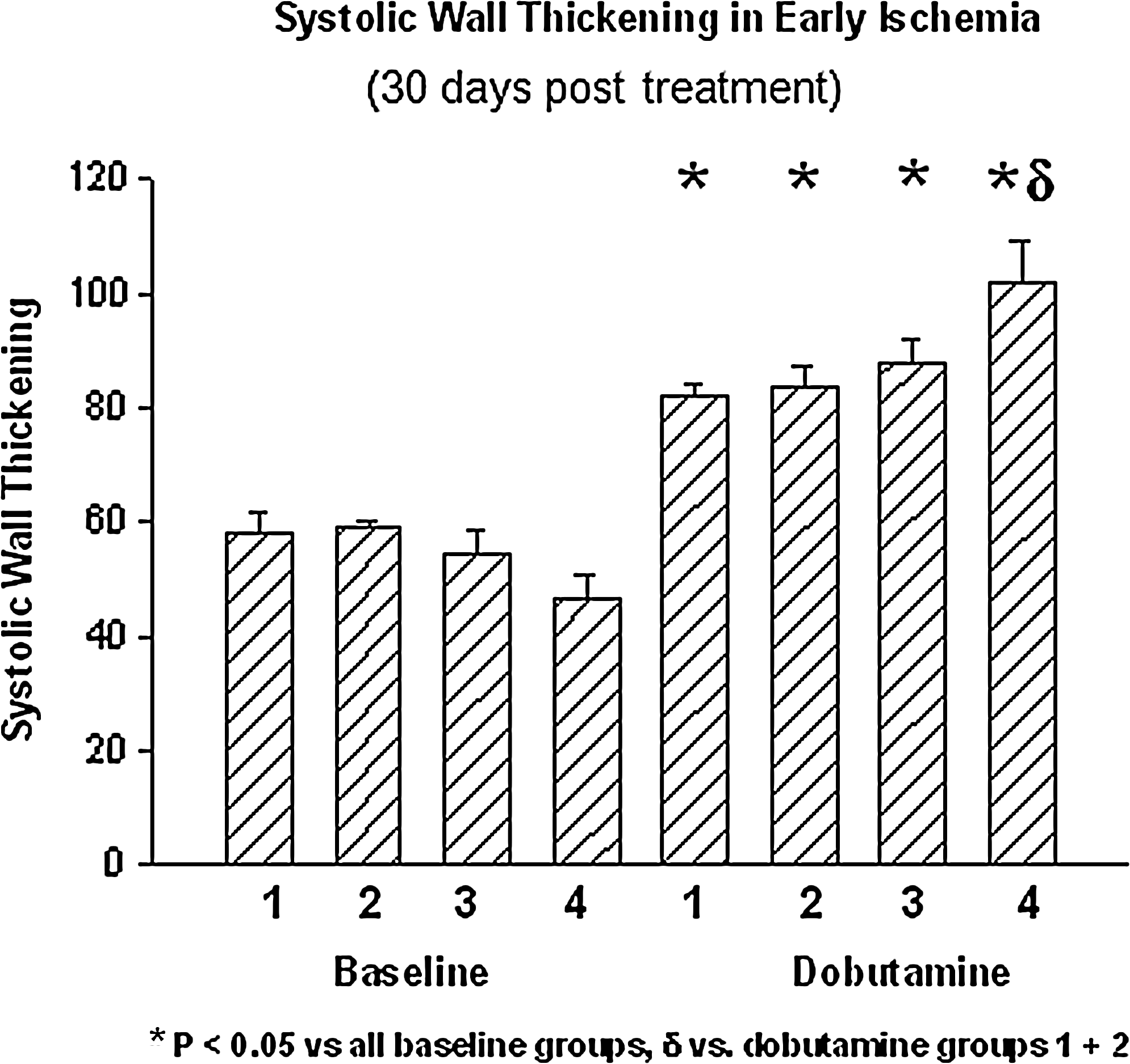
Systolic wall thickening values under resting and stressed conditions (dobutamine treated) in all treatment groups at the 30 day time point. Group 1=ischemia only; Group 2=acellular 3DFC; Group 3=single 3DFC treatment; Group 4=three-piece 3DFC treatment.

Percent systolic wall thickening increase from baseline (stress vs. dobutamine) at 30 days. Group 1=ischemia only (sham); Group 2=acellular 3DFC; Group 3=single 3DFC treatment; Group 4=three-piece 3DFC treatment.
Discussion
The objective of this study was to evaluate the safety of 3DFC (Anginera™) after application to the epicardial surface of the heart in a canine model of chronic ischemia. Evaluation of the primary safety endpoints (including hemodynamic, electrocardiographic, echocardiographic, and clinical and gross pathology observations) demonstrated the safety of 3DFC at all dosing levels and at both time points. Additionally, from the separate histopathologic evaluation, no evidence of an immunologic reaction to 3DFC was noted and an increase in microvasculature specific to the epicardium and pericardium was found (Fig. 1).
Regarding effects on ventricular performance, the primary echocardiographic assessment strongly suggests a dose-dependent improvement in left ventricular global function resulting from the epicardial application of 3DFC to chronically ischemic hearts. In addition, from the separate echocardiography analyses, changes in CO, LVEF, LVESVI, and SWT (Figs. 2–6 and 8–10) support the conclusions that treatment with 3DFC improves ventricular performance and ventricular wall motion in chronically ischemic canine hearts 30 days after treatment. Additionally, dose-dependent improvements are seen in the current study where greatest increases in EF values are seen with the highest dose of 3DFC treatment (Fig. 6). This dose-dependent improvement is also characterized by SWT values where the highest dose of 3DFC treatment caused a 144% increase in wall thickening values compared to 55% in the single dose arm (Fig. 10). Collectively, the histologic findings and the evidence of improvements in LV function in the current chronic ischemia study support previous findings where the 3DFC technology has been used to treat acute infarction or chronic heart failure (Table 1).
The placement of either acellular or viable 3DFC patches, irrespective of the number of patches implanted, resulted in an improved LVEF and increased CO during stress with dobutamine at 30 days after induction of ischemia. In the chronic ischemia animals (Group 1), this response was only seen at 90 days; at this time point the chronic ischemia animals were able to mount a response to dobutamine even though they had not received the 3DFC treatment. This finding is congruent to the published literature where the canine model is described as a model that has an intrinsic ability for coronary collateralization.19–21
While other investigators have evaluated a variety of growth factors and cytokines as angiogenic therapies, the 3DFC technology provides a unique strategy. The 3DFC technology is a cell-based therapy where living human fibroblasts, their extracellular matrix, and a variety of growth factors and cytokines that these fibroblasts produce are implanted as a therapeutic solution. Fibroblasts in this 3D matrix have been described in the literature to be immunoprotected, 22 and the histopathology results from the current study support this same finding where no evidence of an immunologic reaction could be found (Fig. 1). Furthermore, the angiogenic potential of these fibroblasts that compose the 3DFC technology has been well described in in vitro work 12 and in various in vivo experiments in multiple animal models (Table 1).
The angiogenic potential of the 3DFC technology may be primarily responsible for the favorable wound healing response demonstrated clinically in patients with diabetic foot ulcers12,13 and also in animal models of heart disease where improvements in cardiac function have been shown after treatment to infarcted cardiac tissue in mouse and rat models.14–18 However, there may also be paracrine influences that the 3DFC technology is modulating. This activity of the 3DFC technology may afford the opportunity for improvements to be made with future cell replacement therapies. For example, less than optimal outcomes have resulted from a variety of clinical trials using different replacement cells for patients with myocardial infarctions or left ventricular dysfunction. 23 Specifically, published results for the beneficial effects of bone marrow cell transplantation after acute myocardial infarction come from the Bone Marrow Transfer to Enhance ST-Elevation Infarct Regeneration (BOOST) trial. 24 In this study the relative improvement in LVEF improvement after treatment with bone marrow cells at 6 months, compared to no infusion, was no longer significant at 18 months. 24 Furthermore, 5-year follow-up data from the BOOST trial demonstrate that a single intracoronary application of autologous bone marrow cells does not promote a sustained level of left ventricular systolic improvement. 25 Authors of the BOOST trial raise a concern around the therapy being that of cell retention. Additionally, other investigators have reported cell retention as a major obstacle for these type of cell replacement therapies, indicating that only 1.3% to 2.6% of infused bone marrow cells are retained in the heart. 26 Therefore, using a delivery vehicle that creates a hospitable environment for the fibroblasts in the 3DFC technology could also be used to house and deliver replacement cells with functional capacity such as a myoblast, cardiac progenitor cell, or a stem cell population.
Results from the current study support the continued development of the 3DFC technology as a therapy for cardiac patients. Evaluation of the primary safety endpoints (including hemodynamic, electrocardiographic, echocardiographic, and clinical and gross pathology observations) demonstrated the safety of 3DFC at all dosing levels and at both time points. Furthermore, changes in CO, LVEF, LVESVI, and SWT support the conclusion that 3DFC stimulates a positive biologic effect on ischemic hearts in this canine model. These data support the conclusion that treatment with viable 3DFC improves ventricular performance and ventricular wall motion in chronically ischemic canine hearts 30 days after treatment.
The investigation and evaluation of the 3DFC technology for cardiac applications has occurred over the better part of a decade. Previous to this application, the 3DFC technology was extensively evaluated for dermatology applications12,13 where it continues to be used clinically to treat a variety of conditions. In this application, the 3DFC technology has provided a valuable tissue-engineered product that has benefited tens of thousands of patients to date in the United States alone. Research and development activities for cardiac applications of 3DFC continue. The history of 3DFC for cardiac therapy is promising, and early clinical data continue to support the many published preclinical findings of this tissue-engineered product.
Footnotes
Acknowledgments
The authors would like to acknowledge the contributions of Dr. Mark Cunningham (Charles River Laboratories) for his management of the GLP study, Drs. Steven Goldman and Hoang Thai (University of Arizona and Tucson VAMC, Cardiology) for analysis of echocardiography data from the canine study, and Dr. Frederick Schoen (Harvard Medical School, Pathology) for his histological analysis of canine study heart tissue samples. The work described in this article was funded by the former Advanced Tissue Sciences, Inc., and subsequently Theregen, Inc.
Disclosure Statement
Robert S. Kellar, Ph.D., Member of Scientific Advisory Board and shareholder, Theregen, Inc.
Stuart K. Williams, Ph.D, Member of Scientific Advisory Board and shareholder, Theregen, Inc.
Gail K. Naughton, Ph.D, Head of Scientific Advisory Board and shareholder, Theregen, Inc.
Michael Siani-Rose, President, shareholder, and founder of Theregen, Inc.
Gianine M. Figliozzi, Director of Operations, Theregen, Inc.