
Abstract
Conventional biological heart valves treated with glutaraldehyde (GA) reveal a limited lifespan due to calcification. This is assumed to be an immune response initiated process, which is not seen with decellularized valves. However, their immunological potential is still a matter of debate. Therefore, serum samples from patients undergoing heart valve surgery were obtained before (Pre), after (Post), and 9–12 months after operation (Follow Up). Immunoglobulin G (IgG) and M (IgM) antibodies against porcine collagen I and α-Gal (Gal-alpha1,3-Gal-beta1,4-GlcNac-R) were determined for decellularized and GA treated valves. Antibody titers for collagen type I revealed no significant alteration for both types of valves. However, a considerable anti-α-Gal antibody response was observed in patients with GA-treated porcine valves. In detail, IgM antibodies were increased during follow up (p<0.05), whereas decellularized valves revealed a minor decrease in the IgM response (p<0.001). IgG antibodies were considerably increased with GA-treated porcine (p<0.05) and bovine (p<0.01) xenografts, whereas there was lack of response with decellularized valves. This indicates that GA treatment is not sufficient to eliminate immune response to the α-Gal epitope completely. Future investigations will have to verify whether immune response to α-Gal can be linked to the limited durability of conventional valves.
Introduction
Another alternative are allografts, 8 which are valves of deceased humans. However, adverse immunologic reactions 9 and their limited availability are severe disadvantages. During the last few years, tissue engineering (TE) of heart valves became a promising alternative to the conventional implants. With TE-techniques it is possible to create functional tissues with specific characteristics. Recent investigations have focused on achieving valves free of cells.10–13 The decellularization protocols are complex, and only a few approaches were able to show removal of cells and cellular compounds completely without affecting the extracellular matrix (ECM). 14 Most of the suitable decellularization techniques, however, are still in a laboratory stage, and so far only two methods have gained clinical approval.15,16 One of theses methods is the Synergraft protocol, and the other technique led to the development of cellfree porcine pulmonary valves Matrix P® and Matrix P plus® by using deoxycholic acid (DOA) for decellularization.16,17 Other protocols also employ DOA but use it in combination with other detergents 14 , which affect their clinical suitability. A major advantage of the Matrix P plus valves is that they do not calcify in vivo18,19 and possess remodeling and growth potential 16 that all other presently available implants lack. Since they consist solely of the ECM, they might, therefore, have a lower immunologic potential.20,21 However, this is still a matter of debate. 22
The aim of the present study was, therefore, to compare the immunologic potential of conventional and TE heart valves in patients with regard to the immune response they elicit.
Therefore, patients who received a conventional heart valve were compared with patients receiving a decellularized valve (Matrix P plus®) with regard to their antibody titers for an ECM protein (collagen I) and for the xenoantigen α-Gal (Gal-alpha1,3-Gal-beta1-4GlcNac-R). The titers were estimated pre-, post-, and late postoperatively (Follow Up). To differentiate between early and late immune response immunoglobulin, class M (IgM) and immunoglobulin class G (IgG) antibodies were investigated.
Material and Methods
Patients
Serum samples of 159 patients who underwent heart valve surgery and received a xenograft, either GA treated or decellularized, were collected. Additionally, 24 sets of samples from patients with mechanical heart valves or with a coronary artery bypass graft were investigated as controls. The samples were obtained earlier (Pre), up to one week after (Post), and 9–12 month after surgery (Follow Up). For anti-porcine collagen I antibodies, 44 recipients with porcine GA-treated xenografts were compared with 106 patients receiving porcine decellularized heart valves (Matrix P plus, AutoTissue GmbH, Berlin Germany). The Matrix P plus valves were decellularized with DOA, according to a patented protocol of AutoTissue GmbH. Hereby all cells are removed from the tissue, and the valves were sterilized as described thereafter. 16 The valves were not treated with GA or similar substances.
To estimate the anti α-Gal response in patients, GA-treated porcine valves (n=33), GA-treated bovine valves (n=9), and decellularized valves (n=70, Matrix P plus) were compared. All patients gave written consent for blood sampling and participation in the study.
Table 1 summarizes the patients' characteristics and their age. Serum was obtained from patients' coagulated blood by centrifugation at 2000g for 10 min. The supernatant was collected and stored frozen at −80°C until further use.
yrs, years; SD, standard deviation; n, number of patients investigated.
Collagen assay
Antigens
Human collagen type I was purchased from Sigma-Aldrich (Deisenhofen, Germany). Porcine collagen I was isolated from porcine skin according to a protocol of Enriquez-Verdugo et al. 23 Briefly, porcine skin (400 mg) was homogenized using an Ultra Turrax T8 (IKA Labortechnik, Staufen, Germany) in 12 mL 0.5M acetic acid solution containing 333 mg/L Pepsin A (Worthington Biochemical Corp., Lakewood, NJ) The homogenate was incubated for 76 h at 4°C on a shaker. Thereafter, collagen type I was received in the pellet after precipitation and centrifugation for 1 h at 10,000g after successive stirring overnight with 0.7M NaCL, 1.7M NaCl, and 2.5M NaCl, respectively. Protein concentrations were determined according to Bradford et al. 24 using the BioRad assay (BioRad, Hercules, CA).
Collagen I antibody assay
The enzyme-linked immunosorbent assay (ELISA) technique was used to measure the specific antibody concentration (IgM & IgG) in serum of patients against porcine and human collagen type I. Collagen type I from the different species was coated onto high-bind micro-titer plates (Corning, NY) at 4°C over night. Thereafter, unspecific binding sites were blocked with block buffer (Starting block, Pierce, Rockford, IL). Blocked plates were used either directly or stored at 4°C until use.
Plates were incubated with diluted serum for 75 min, washed, and treated with a secondary antibody for another 75 min (either anti-human IgG or anti-human IgM, Rockland, Gilbertsville, PA). Both antibodies were conjugated with biotin, to bind the streptavidin-conjugated horseradish-peroxidase (HRP, Rockland). Finally, a colour reaction was obtained with peroxidase reagent 3.5′,5.5′-tetramethylbenzidine (TMB, Pierce, Rockford, IL). Absorbance was determined at 450 nm with 620 nm as reference wavelength after terminating the reaction with TMB stop-reagent (Sigma-Aldrich) using an Anthos Labtec HTII plate reader. All samples were measured in triplicate. Pre, post, and follow-up samples of each patient were estimated on the same plate to eliminate differences due to plate variances.
α-Gal antibody assay
Gal-alpha1,3-Gal-beta1-4GlcNAc-BSA (α-Gal) was obtained from MoBiTec (Göttingen, Germany). α-Gal was immobilized on micro-titer plates at a concentration of 500 ng/well over night. All other processing was done according to the anti collagen assay just described.
Statistical analysis
Statistical analysis was performed using Instat (GraphPad Inc, CA). Since assay data failed to be normally distributed (tested by the Kolmogorow-Smirnow-test), the nonparametric paired Wilcoxon test was used to calculate significance. A p-value <0.05 was considered statistically significant, p<0.01 to be very significant, and p<0.001 as highly significant.
Inter- and intra-assay-variance
To estimate the reproducibility of the ELISA assay, the inter-assay- and intra-assay-variances were determined. The inter-assay-variance describes the variance of the assay at different days, and the intra-assay-variance shows the variance of the replicates.
For these assays, human collagen I as immobilized surface antigen and a human serum pool (AutoTissue GmbH, Berlin, Germany) containing primary antibodies were used. The conditions of the inter- and intra-assay-variance determinations were essentially the same as just described for the ELISA assay. To estimate the intra-assay-variance for IgG and IgM antibodies, ten independent measurements were performed for each of the antibodies on the same micro-titer plate under equal conditions. The inter-assay-variance was determined by measuring ten samples at seven different days on different micro-titer plates. From the results of both assays, the coefficients of variation were calculated.
Results
Collagen assay
In the first experiments, the linear range of the ELISA was determined for IgG and IgM specific anti collagen I antibodies with different dilutions of human serum. A linear range from∼0.5 to 2.5 arbitrary units (AU) for the IgG specific anti-collagen I antibodies and from ∼0.25 to 1.2 AU for the IgM specific antibodies was achieved (data not shown).
To verify the designed ELISA for collagen type I, intra- and inter-assay-variance (Table 2) and the resulting variation coefficients were additionally determined. The coefficients achieved were either below 10% or slightly more, which is considered satisfactory. 25
SD, standard deviation; IgG, immunoglobulin G; IgM, Immunoglobulin M.
In this study, two groups of patients were investigated with regard to their anti-porcine collagen I titers. The first group were patients who had received a GA-treated valve of porcine origin, and the second were patients receiving a decellularized porcine valve (Matrix P plus). The results of the statistical evaluation are presented as box plots showing the mean (+), the median (-), and the inter-quartile range (25th–75th percentile). The whiskers represent the 10th and 90th percentile, respectively. Figure 1 represents the results for the Matrix P plus valves and Figure 2 those for the GA-treated porcine heart valves.

Statistical evaluation of anti-porcine collagen type I in patients with a decellularized porcine xenograft. Immunoglobulin G: IgG, Immunoglobulin M: IgM Pre: preoperatively, Post: postoperatively, Follow Up: 9–12 months postoperatively, AU: arbitrary units, n: number of patients investigated.
Statistical evaluation of anti-porcine collagen type I in patients with a glutaraldehyde (GA) treated porcine xenograft. Immunoglobulin G: IgG, Immunoglobulin M: IgM Pre: preoperatively, Post: postoperatively, Follow Up: 9–12 months postoperatively, AU: arbitrary units, n: number of patients investigated.
The decellularized valves revealed minor but significant changes in the measured anti-porcine collagen type I antibody titers from Post to Follow Up for the IgG (p=0,0363) and from pre- to postoperative (p=0,0099) and to follow up (p=0,0028) for the IgM antibodies. However, the changes of the mean values (IgG=−0.004; [0.6%]; IgM=−0.029, [4.0%] and 0.024, [3.3%]) are negligible, as they are considerably smaller than the estimated inter-assay variance for the assay.
To verify this assumption, anti-human collagen type I titers of the serum samples were determined additionally to estimate the variation among the serum samples itself. Changes in the anti-human collagen I level may only be due to the sample variance and, therefore, are suitable to normalize the anti-porcine collagen I levels. For the anti-human collagen titers, a similar range of variation was found as for the anti-porcine antibodies. After normalization of anti-porcine collagen titers to the anti-human collagen titers, the normalized values were analyzed again. They proved that there is no significant change in anti-porcine collagen titers in serum samples of patients who received a decellularized porcine valve.
The same set of analysis was done for the group with GA-treated valves. Here, no significant changes in the anti-porcine antibody titers (see Fig. 2) were observed, neither measured directly nor after normalization. Although the median and mean values of the follow-up samples for the porcine collagen I titers were increased compared with Pre and Post samples, they revealed no significant changes because of the lower sample numbers. An increase in follow-up values were also observed with human collagen I titers of this group.
α-Gal assay
Three groups of patients receiving different types of heart valves were investigated for their anti α-Gal antibody titers. The first two groups consist of patients who received a GA-treated heart valve of porcine or bovine origin. The third group were patients receiving a Matrix P plus decellularized porcine heart valve. In addition to these groups, a control group was investigated, too, consisting of patients who had undergone bypass surgery or received a mechanical valve. In Controls, no significant alterations in IgG or IgM titers were observed (see Fig. 3). However, for this group, only the pre- and postoperative samples were investigated, because too few follow-up samples were available.
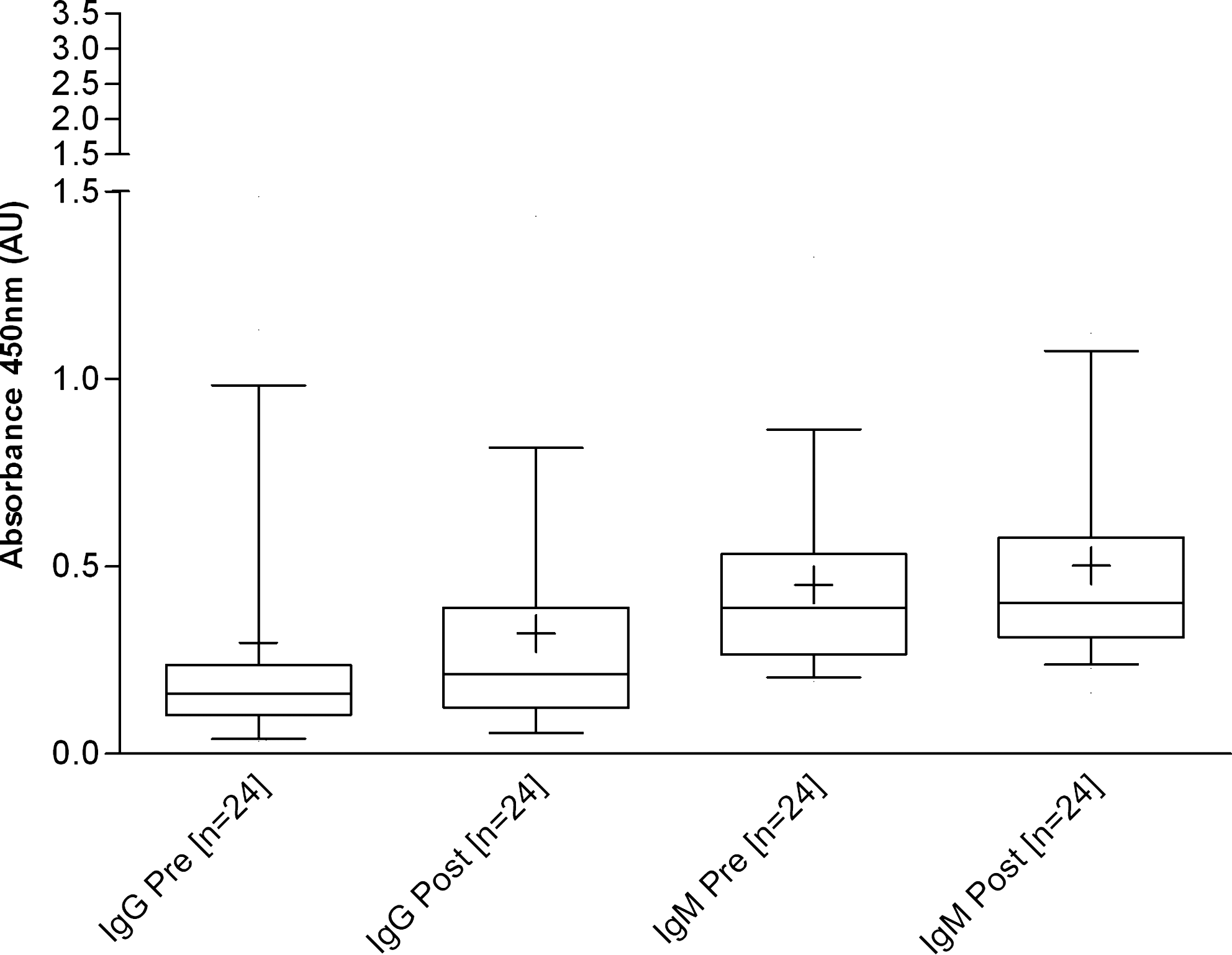
Statistical evaluation of anti- α-Gal in patients with a mechanical heart valve or with bypass surgery. Immunoglobulin G: IgG, Immunoglobulin M: IgM Pre: preoperatively, Post: postoperatively, Follow Up: 9–12 months postoperatively, AU: arbitrary units, n: number of patients investigated.
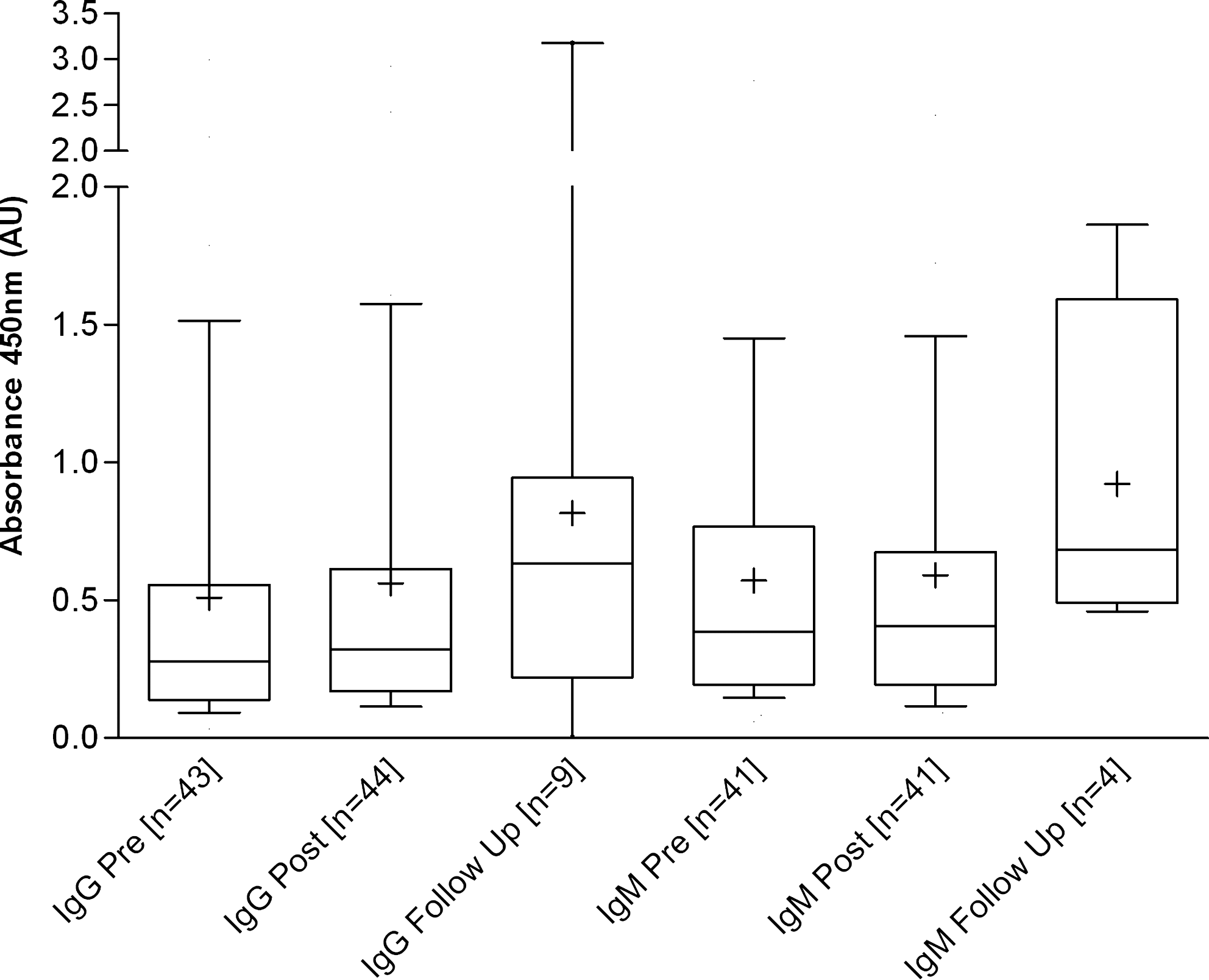
In all three groups, a decrease of α-Gal specific IgG antibodies was observed directly postoperatively. These levels stayed unaltered for the Matrix P plus group up to 12 month after implantation (see Fig. 4), whereas for the GA treated bio-prostheses, the α-Gal specific IgG levels increased significantly during follow up. For the porcine GA-treated group, a p-value of 0.0391 (see Fig. 5) and for the bovine GA treated group, a p-value of 0.0078 (see Fig. 6) with regard to the postoperative value was achieved. Additionally, for the bovine valves, a significant increase of preoperative versus follow-up values (p=0,0117, see Fig. 6) was observed.
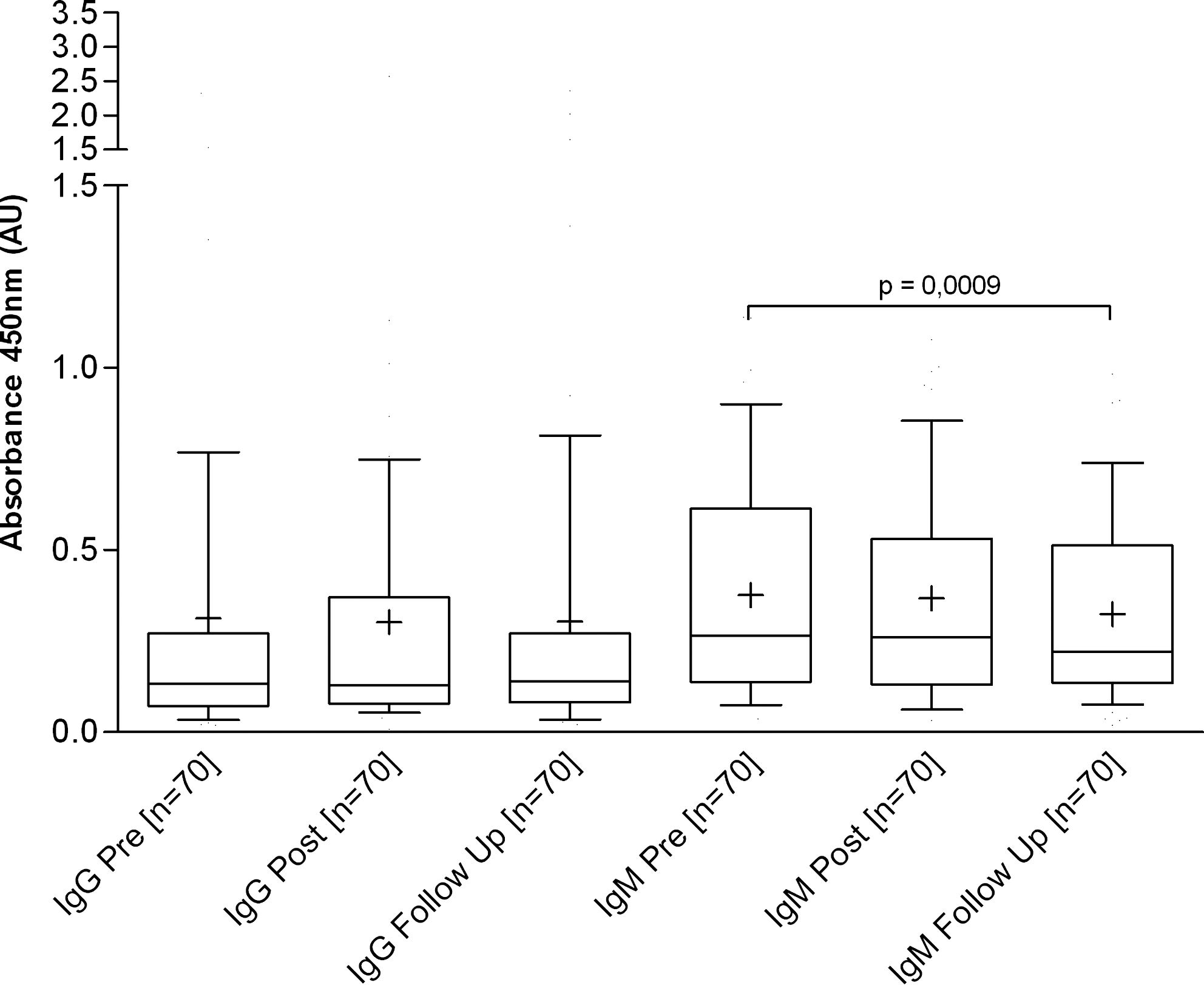
Statistical evaluation of anti- α-Gal in patients with a decellularized heart valve. Immunoglobulin G: IgG, Immunoglobulin M: IgM Pre: preoperatively, Post: postoperatively, Follow Up: 9–12 months postoperatively, AU: arbitrary units, n: number of patients investigated.
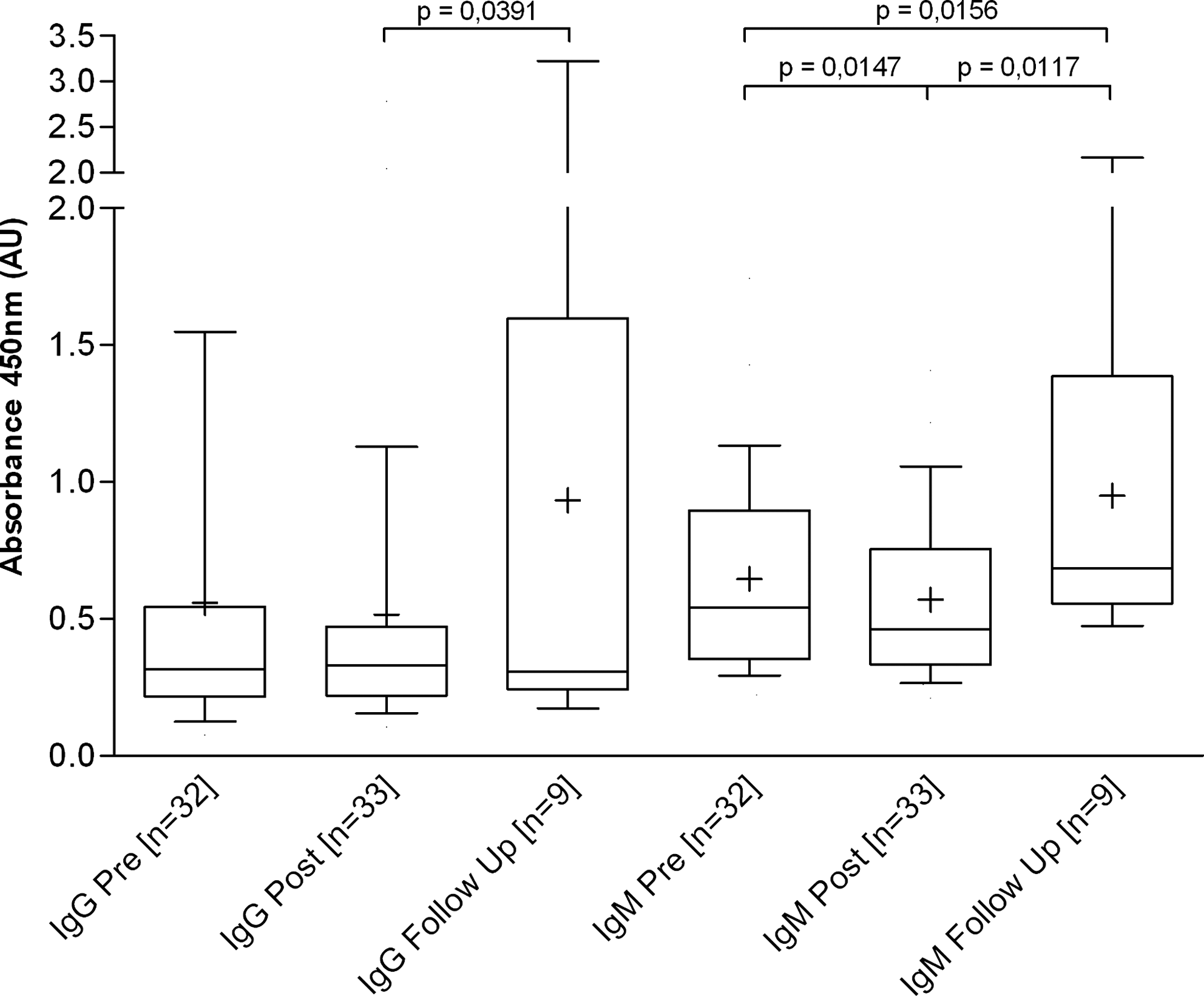
Statistical evaluation of anti- α-Gal in patients with a GA-treated porcine heart valve. Immunoglobulin G: IgG, Immunoglobulin M: IgM Pre: preoperatively, Post: postoperatively, Follow Up: 9–12 months postoperatively, AU: arbitrary units, n: number of patients investigated.
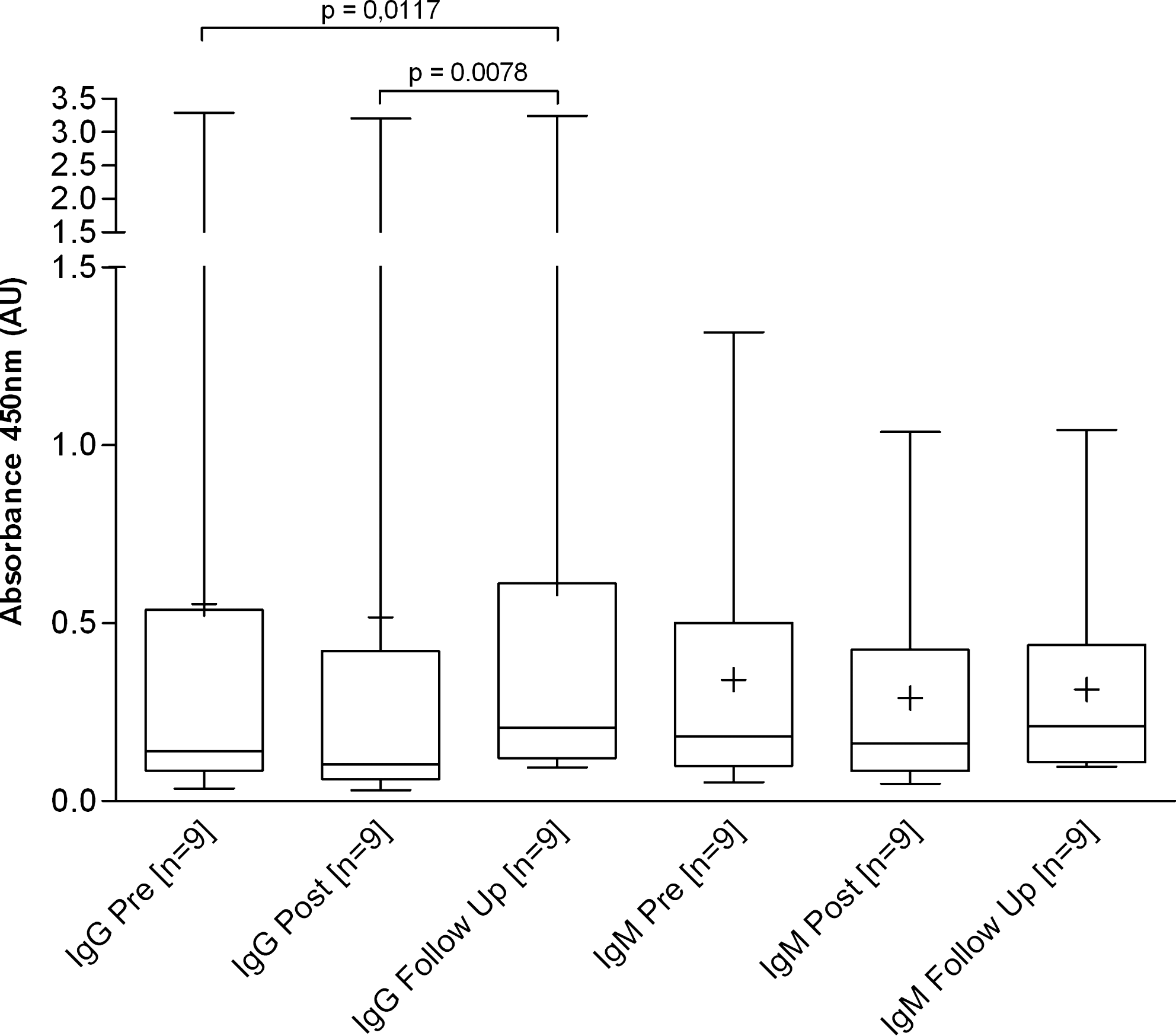
Statistical evaluation of anti- α-Gal in patients with a GA-treated bovine heart valve. Immunoglobulin G: IgG, Immunoglobulin M: IgM Pre: preoperatively, Post: postoperatively, Follow Up: 9–12 months postoperatively, AU: arbitrary units, n: number of patients investigated.
For α-Gal specific IgM, a similar decrease from pre- to postoperative samples was detected as for the IgG specific antibodies in both GA-treated groups. This effect again was not observed with samples from patients receiving a decellularized heart valve. Here, we found a highly significant decrease pre versus follow up (p=0.0009, see Fig. 4) of the α-Gal specific IgM titers.
Discussion
In recent years, tissue-engineered heart valves, which are completely free of all viable cells, became clinically available. However, the immunologic potential of decellularized tissues is still a matter of debate.22,26 Almost every other commercially available heart valve prostheses is being treated with GA. This treatment is necessary to reduce the immunological potential of the native tissue and to avoid degeneration. 4 However, this cannot prevent the main disadvantage of the conventional biological heart valves, which is their limited lifespan. The main cause for this is calcification, which is presumably an immune response initiated process. 7 This led to the assumption that the GA treatment is not sufficient to entirely eliminate the immunologic potential of the valves. Some immunogenicity seems to persist after the GA treatment and might be able to trigger calcification.27–29
The present study, therefore, wanted to find proof whether the ECM, and/or the xenoantigen α-Gal of heart valves, might contribute to an immune response in patients and might thereby help understand the initial process of calcification. Therefore, GA-treated heart valves of biological origin, which are known to calcify lately, were compared with decellularized heart valves which lack calcification.18,19 In earlier performed investigations, it has been histologically shown that α-Gal epitopes are still present in GA treated valves and in the vessel wall of Synergraft valves but not in completely decellularized valves. 14
To address this question, a species specific ELISA against collagen I, the most common protein of the ECM, was developed. In conjunction with the collagen assay, the response to α-Gal, a major xenoantigen present on the valves, was investigated. α-Gal titers in blood samples from patients who had received GA-treated heart valves of bovine or porcine origin were determined and compared with samples from patients who had received a decellularized heart valve.
This investigation revealed that with regard to collagen I there was no significant alteration in the porcine or human antibody titers in samples of GA-treated or decellularized valves of porcine origin. This leads to the conclusion that there is no immune response toward porcine collagen I in patients receiving a heart valve prosthesis of porcine origin, regardless of whether they are treated with GA or decellularized.
On the other hand, an immune response against α-Gal in patients receiving a GA-treated porcine heart valve could be observed. IgM antibodies were considerably increased during follow up in patients receiving these valves, whereas with decellularized valves there was even a decrease in the IgM response. The subsequent immune response of the specific IgG antibodies showed a considerable increase in porcine GA-treated valves and bovine GA-treated xenografts as well, whereas there was no response in decellularized valves. The data on conventional GA-treated xenografts confirm previous results achieved in similar designed studies such as those of Park et al. and Mangold et al.30,31 Park et al. reported a significant decrease of the IgG and IgM titers on the first postoperative day, which corresponds well with our findings. They further observed an increase of titers for both isotypes during the first week after implantation. After one week, the IgM titers decreased, whereas the IgG remained increased after two months. Mangold et al. showed similar results in their study, where they investigated 19 patients who had received a GA-treated bioprosthesis. They also described a significant increase in IgG antibody titers 3 months post operation. This corresponds with our data, as we observed an equal decrease in antibody titers directly postoperatively for all groups followed by an increase during follow up for the GA-treated valves up to 12 months. Opposite to this, we were able to show that there is no immune response in patients who received a decellularized porcine heart valve up to 12 months after surgery.
It is known from previous investigations that valves free of cells such as the Matrix P plus in contrast to conventional valves do not calcify at all, as shown in the juvenile sheep model18,19 and in midterm results with patients. 32 Further they demonstrated that seeding of the valves is not necessary for repopulation, which confirms the assumption that the decellularized tissue is not cytotoxic.
From the present results, it can be ruled out that the process of calcification is being triggered by an immune response initiated by collagen I, because there is no detectable immune response toward collagen I. This is regardless of whether the collagen I is crosslinked with GA or in its native form present in decellularized valves. This, however, is not self-evident. Although there is a considerable homology between human and porcine collagen, a former study revealed that human and porcine collagen I both elicit proliferation in co-stimulated immune cell sub-populations associated with a strong release of Th1 cytokines. 33
Previously, it has been discussed that phospholipids might induce calcification, observed in conventional biological heart valves. 34 However, several investigators now believe that the α-Gal epitope plays a major role in calcification. 7 Moreover, α-Gal is the major xenoantigen, and it has been assumed to be responsible for hyper-acute rejection of xenogenic tissues.35,36 The α-Gal epitope is conserved in most mammalian species except human, apes, and old-world monkeys 37 and it has been shown that approximately 1% of all circulating B cells are able to produce antibodies against α-Gal. 38
Previously conducted investigations by Kasimir et al. 14 detected α-Gal in GA-treated heart valves and in the vessel wall of Synergraft valves, the first clinically used decellularized heart valve. In the same study, a complete lack of α-Gal could solely be achieved by an extensive decellularization protocol, which combines three different substances with one of them being DOA. The absence of anti-α-Gal antibodies in the serum of patients receiving Matrix P plus valves leads to the conclusion that the α-Gal epitopes must have been entirely removed or masked by the employed decellularization protocol for these valves using DOA alone. 16
The results achieved in the present study indicate that α-Gal present in xenogenic tissues might elicit an immune response in GA-treated or incomplete decellularized implants,21,22 which is lacking in complete decellularized tissues. Future investigations on the role of the α-Gal epitope will have to find proof whether this observed response is the reason for inducing calcification in conventional valves or whether there are additional factors responsible for the limited durability by calcification of these valves in patients. 39
Footnotes
Acknowledgments
The excellent technical assistance of Mrs. Soren Lück and Mrs. Elke Wachsmuth is gratefully acknowledged.
Disclosure Statement
The authors want to disclose the following relations to AutoTissue GmbH, the manufacturer of the Matrix P plus valves Prof. Dohmen and Prof. Konertz are shareholders, Dr. Erdbrügger and Dr. Posner are employees, and Mr. Bloch and Mrs. Golde have done some work presented here in their Ph.D. and diploma thesis at AutoTissue, respectively.