
Abstract
The use of mesenchymal stem cells (MSCs) for tissue regeneration is often hampered by modest engraftment in host tissue. This study was designed to quantitatively compare MSCs engraftment rates after delivery using a polysaccharide-based porous scaffold or endocardial (EC) injection in a rat myocardial infarction model. Cellular engraftment was measured by quantitative reverse transcription–polymerase chain reaction using MSCs previously transduced with a lentiviral vector that expresses green fluorescent protein (GFP). The use of a scaffold promoted local cellular engraftment and survival. The number of residual GFP+ cells was greater with the scaffold than after EC injection (9.7% vs. 5.1% at 1 month and 16.3% vs. 6.1% at 2 months, respectively [n=5]). This concurred with a significant increase in mRNA vascular endothelial growth factor level in the scaffold group (p<0.05). Clusters of GFP+ cells were detected in the peri-infarct area, mainly phenotypically consistent with immature MSCs. Functional assessment by echocardiography at 2 months postinfarct also showed a trend toward a lower left ventricular dilatation and a reduced fibrosis in the scaffold group in comparison to direct injection group (n=10). These findings demonstrate that using a porous biodegradable scaffold is a promising method to improve cell delivery and engraftment into damaged myocardium.
Introduction
The approach to improve exogenous cell delivery to tissue, whatever the cell source, is of major clinical importance and has stimulated further investigation on the use of bioengineered scaffolds as cell delivery vehicles. 6 One of the challenges involves the development of optimized biocompatible materials functioning as synthetic analogs of the extracellular matrix, that would both provide a substrate for transplanted cells and promote cell engraftment. 7 Many materials have been used including polyglycolic acid, collagen gel, alginate, and gelatin mesh. In this context, we previously described the preparation of a polysaccharide-based scaffold as a novel biomaterial for cardiovascular engineering. 8 Naturally derived polysaccharides are hydrophilic, biodegradable, and biocompatible and can form highly hydrated gels that could mimic the extracellular matrix. 9
In the present study, we used a rat model of acute myocardial infarct to examine MSCs engraftment in infarcted tissue using this polysaccharide-based porous scaffold in comparison with EC injection. Syngeneic MSCs stably transduced with a lentiviral vector allowed accurate in vivo assessment of cell retention after cardiac delivery. The effects on cardiac remodeling and function were then evaluated.
Materials and Methods
Culture, characterization, and preparation of MSCs
MSCs were obtained from the bone marrow of syngeneic adult Lewis rats (Janvier). Briefly, cells were collected by flushing femurs and expanded in Dulbecco's modified Eagle's medium (Gibco) supplemented with 1% penicillin/streptomycin and 10% fetal bovine serum at 37°C in a 5% CO2 atmosphere. Cells were subcultured every 4–7 days.
Characterization of rat MSCs was performed by flow cytometry analysis with a phycoerythrin-conjugated anti-human CD45 (Immunotech) antibody (MoAb) (BioLegend) and with fluorescein isothiocyanate (FITC)-conjugated anti-CD90 (Becton Dickinson), anti-CD106 monoclonal, and anti-CD29 MoAbs (BioLegend). MSCs were also characterized by their capacity to differentiate along adipogenic, chondrogenic, and osteogenic lineages. 10 The ability of MSCS to differentiate toward cardiac lineage is controversial. We did not obtain any cardiac differentiation from rat MSCs during our in vitro culture.
Scaffold preparation
Polysaccharide-based scaffolds were prepared using a mixture of pullulan (Hayashibara) and dextran (Pharmacia), and sodium carbonate was added as a porogen agent. 11 Chemical cross-linking was carried out using trisodium trimetaphosphate STMP (Sigma) under alkaline conditions as described. 12 After a freeze-drying step, a circular punch was used to cut 6 mm diameter and 1 mm thickness round-shaped porous scaffolds. Scaffolds were observed with environmental scanning electron microscopy (ESEM) using an ESEM-FEG (Philips XL 30) with an accelerating voltage of 15 kV at a pressure of 4 torrs. Fluorescent scaffolds were prepared by adding 1% of Fluorescein-IsoThioCyanate-dextran (Sigma) before cross-linking for confocal miscroscopy observation. Optical sections were acquired using a Zeiss LSM 510 confocal microscope (Carl Zeiss), equipped with a 10×Plan-NeoFluar objective lens (numerical aperture of 0.3) (Carl Zeiss). FITC-dextran was excited at 488 nm with an argon laser and its fluorescent emission was selected by a 505–530 nm bandpass filter. Scaffolds were submitted to UV before cell seeding. Cell loading was performed after cell trypsinization by rehydration of a dried scaffold with 20 μL of cell suspension. In a first set of in vitro experiments, optimal cell density was determined using from 2×104 to 106 cells/scaffold, with scaffold size ranging from 2 to 10 mm in diameter. A metabolic MTT assay was performed 1 day later, by incubating seeded scaffolds with 0.5 mg/mL of MTT (3-(4,5-dimethyldiazol-2-yl)-2,5 diphenyl tetrazolium bromide, Sigma) for 3 h at 37°C. Resulting formazan crystals were solubilized in 0.5 mL of dimethyl sulfoxide and absorbance was recorded at 570 nm with a microplate reader. Noncellularized porous scaffolds were used as controls. Cell viability was assessed with a Live/dead kit (Invitrogen). Briefly, cellularized scaffolds were incubated with 4 μM calcein AM and 2 μM ethidium homodimer-1 solution (Invitrogen) for 1 h at 37°C. Cellularized scaffolds were then observed with a Zeiss LSM 510 confocal microscope using a standard fluorescein bandpass filter for calcein and a propidium iodide filter for EthD-1.
Before in vivo administration, 106 cells were seeded on a 6 mm porous scaffold with 20 μL of cell suspension; 30 min after, once cells attached, scaffolds were placed in 1 mL culture medium for complete rehydratation.
Animal study
Both the procedure and the animal treatment complied with the Principles of Laboratory Animal Care formulated by the National Society for Medical Research. The studies were carried out under authorization 006235 of the Ministere de l'Agriculture, France.
In a first set of three experiments, migration from scaffold to cardiac tissue was evaluated in healthy myocardium. Afterward, male syngenic Lewis rats were submitted to the ligation of the descending anterior left coronary artery. Fifteen minutes after infarct, rats received 1×106 MSCs according to the following procedures: the EC group received 5 myocardial injections of MSCs suspended in 20 μL of culture medium in the peri-infarct and infarct zones. In the patch group, the cellularized scaffold was covered by a clinical polytetrafluoroethylene (PTFE) membrane (Pericardial) that was glued onto the infarcted area. For the control scaffold group, noncellularized scaffolds were implanted in the same conditions.
Determination of cellular engraftment
For assessment of cell retention, Lewis rat MSCs were transduced using a lentiviral vectors construct consisting in a dual-promoter that included green fluorescent protein (GFP) under the regulation of the human EF1α promoter (EF1αGFP) and PAC under the human puromycin resistance gene (puromycin-N-acetyltransferase; PAC) promoter. Evaluation of the transduction efficiency was based on the percentage of GFP+ cells. Three syngeneic lines of transfected MSC were thus obtained and mixed for in vivo administration (passages 4 to 9). Animals were randomly assigned to the delivery method, scaffold or EC group. Engraftment was evaluated 1 and 2 months after GFP+ MSC delivery in the two groups (n=5 per group for each time point).
GFP+ cell quantification in cardiac tissue was performed using molecular analysis of gene expression by quantitative polymerase chain reaction (PCR). The heart was removed and infarct region, border zone and large area of peri-infarct healthy myocardium were cut into slices <0.5 mm thick and immediately submerged in RNA later stabilization reagent (Sigma). A reference curve was established on the basis of the GFP expression level from defined numbers of GFP+ cells (triplicate samples from 10×103 to 1×106 GFP+ cells per sample) used as calibrator. Quantitative PCR was performed on a 7500 Real Time PCR System (Applied Biosystems) with standard cycling conditions. GFP expression levels were normalized relative to the expression of rat HPRT, UBC, and Ywhaz. The number of residual GFP+ cells after EC injection or scaffold administration was estimated by report to the reference curve.
Histology, immunofluorescence, and immunohistochemistry analysis
Analysis were performed after administration of GFP+ MSCs or MSCs double labeled with thymidine analog 5-bromo-2′-deoxyuridine BrdU (10 μM for 24 h) and with a fluorescent dye (PKH26; Sigma) (n=3, each condition).
Left ventricles were harvested, fixed in buffered formalin, and embedded in paraffin for histological stains or in OCT for cryosections and immunohistochemical study. Histological sections were stained with hematoxylin and eosin (H&E) and with Sirius red stain (0.1% in saturated picric acid solution). Fibrosis area and total ventricular area (LV) were quantified by histomorphometric measurement on Sirius red stained sections with Histolab software (Microvision). Fibrosis percentage was calculated as follows: (fibrosis area/total LV area)×100.
Direct observation of PKH-labeled cells in myocardial tissue was performed on cryosections. Immunostaining of myocardial sections was performed using the primary antibodies, anti cardiac sarcomeric α-actinin (Sigma), anti-connexin-43 (Dako), anti-smooth muscle actin (Dako), anti-CD31 (Dako) and anti-GFP (Torrey Pines), secondary Alexa fluor goat anti-mouse 488, and 532 antibodies, all from Molecular Probes (Invitrogen), using a double-labeling technique. Immunostaining of BrdU-positive cells was performed by indirect immunohistochemistry with anti-BrdU mouse antibody (Calbiochem) and DAB staining. Sections were counterstained with hematoxylin before mounting.
Molecular analysis of gene expression by quantitative reverse transcription-PCR
Matrix metalloproteinase (MMP)-2, MMP-9 and vascular endothelial growth factor (VEGF) expression were measured on infarcted heart administered with MSCs using scaffold or EC injection, 1 and 2 months after infarct, in comparison with control animals submitted to infarct without cell administration. Immediately after sacrifice, samples were fixed in RNA stabilization reagent (RNA Later; Sigma). All primers were designed using intron-flanking method. Quantitative PCR was performed on a 7500 Real- Time PCR System (Applied Biosystems) with standard cycling conditions. For housekeeping gene selection, the stability of various reference genes was investigated from different samples of rat infarcted hearts. The expression stability of 7 commonly used reference housekeeping genes (GAPDH, 18S, ActB, CycA HPRT, UBC, and YWHAZ) was analyzed using geNorm and expression stability was determined by the Genorm program. HPRT, UBC, and YWHAZ were identified as most stable genes. Then, gene expression levels were normalized relatively to the expression of rat HPRT, UBC and Ywhaz. Quantification was done with the Pfaffl's method. 13 Relative expression ratios were calculated by reporting values to those of the control animals.
Echocardiographic and catheterization protocols
For determination of cardiac function related to MSC delivery, nontransduced MSCs were used. Animals were randomly assigned to the delivery method, either control, scaffold or EC group. All cardiac echocardiograms were recorded using an Acuson 128XP (Acuson corporation) utilizing a 7–10 Mhz transducer. The heart was first imaged in two-dimensional (2D) mode in the parasternal long axis and short axis views, to position the M mode cursor perpendicular to the interventricular septum and left ventricular posterior wall. Then, M mode images were obtained at a 100 mm/s speed. At least three measurements of LV end-diastolic (LVEDD) and end-systolic diameters (LVESD) were selected and averaged from each animal and the analysis of contractile function was derived from the LV fractional shortening fraction (LVFS): (LVEDD-LVESD/LVEDD×100). The echocardiographic examination was performed 7 days and 2 months after myocardial infarction by a blinded observer.
Statistics
All parameters were expressed as mean values±standard deviation, except for engraftment results expressed as median values. A t-test was performed on fibrosis and mRNA data, a one-way analysis of variance (ANOVA) test was performed on echocardiographic data and a two-way ANOVA was performed on engraftment data. Statistical significance level was set at 0.05.
Results
Cellularized scaffold for implantation
We first examined the optimal conditions of MSCs seeding on the scaffold. Scaffolds from 2 to 50 mm in diameter could easily be obtained and a 6 mm diameter porous scaffold, suitable for the size of rat hearts, was chosen (Fig. 1A). Porosity of scaffolds was observed with ESEM (Fig. 1B). The use of FITC-labeled dextran into polysaccharide scaffolds allowed confocal laser scanning microscopy observation of the inner structure of hydrated scaffolds. A typical single optical slice of a porous scaffold is shown on Figure 1C. A mean pore size of 195 μm and a porosity of 41% were calculated. Cells infiltrated very quickly (<1 min) within the scaffold porous structure like in a sponge, and the maximum volume contained was 15 μL. Using a metabolic MTT assay at day 1, we confirmed that 2×104 to 106 cells/scaffold could be seeded into 6 mm porous scaffold. Absorbance data as a function of the initial cell number is shown on Figure 1D. Cells within the transparent scaffold could be observed with light microscopy as cell clusters (Fig. 1E). Cell viability at day 1 was demonstrated with a live & dead assay (Fig. 1F).
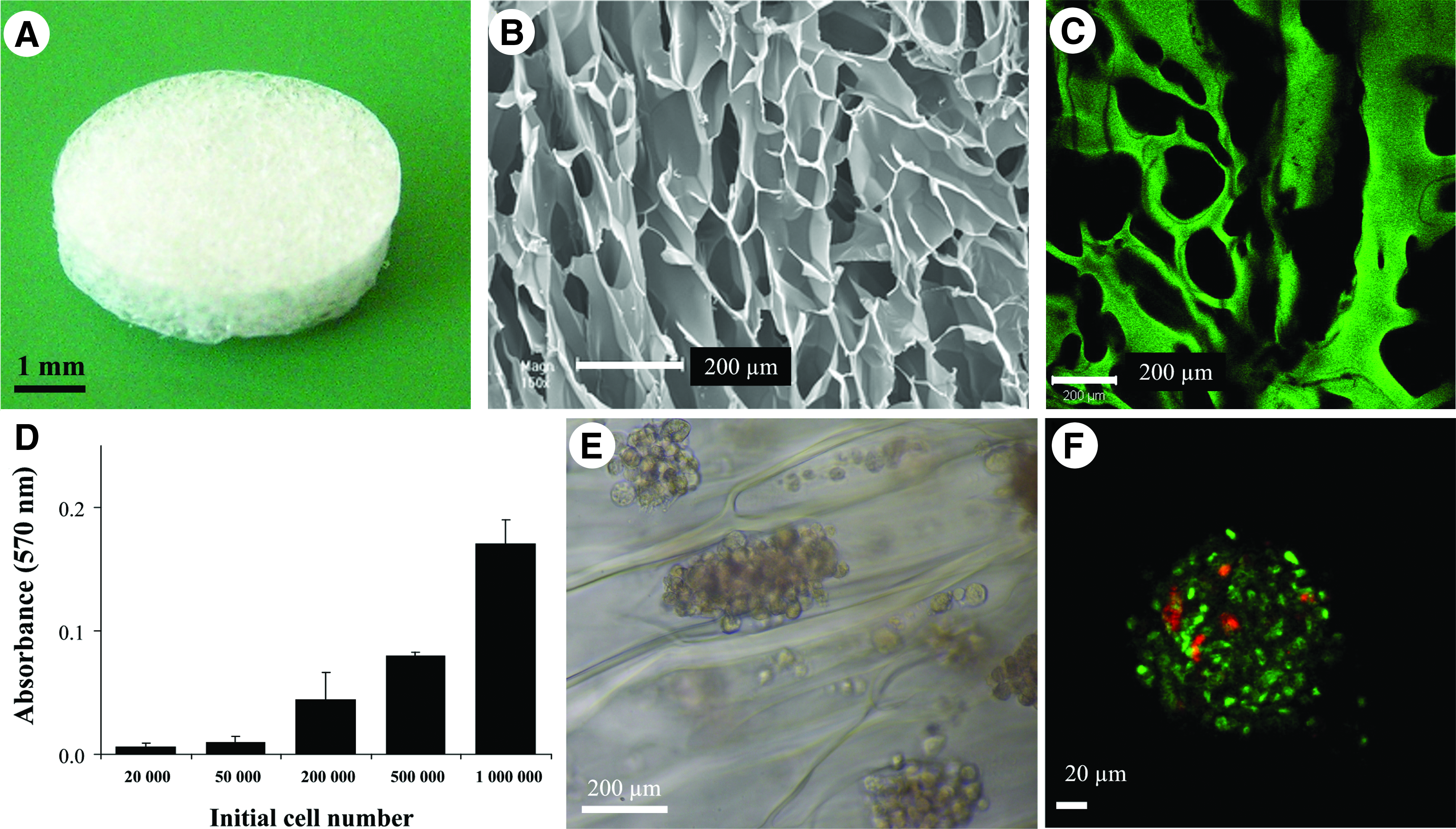
Polysaccharide-based scaffold. Macroscopic view of a dried porous scaffold
A first series of experiments was conducted with FITC-labeled noncellularized scaffolds to determine the in vivo fate of porous scaffold in rat cardiac tissue (n=2). One month after implantation, scaffold was found intact on normal cardiac tissue (Fig. 2A, scaffold stained with alcian blue dye for imaging purposes), as confirmed by fluorescent microscopic observation of heart sections showing cardiac tissue green autofluorescence and FITC-labeled scaffold (Fig. 2B). In contrast, the scaffold on infarcted cardiac tissue was progressively degraded after implantation and only some remnants of the FITC-scaffold were seen embedded or integrated into the adjacent tissue on infarcted heart sections at 1 month (Fig. 2C, D).
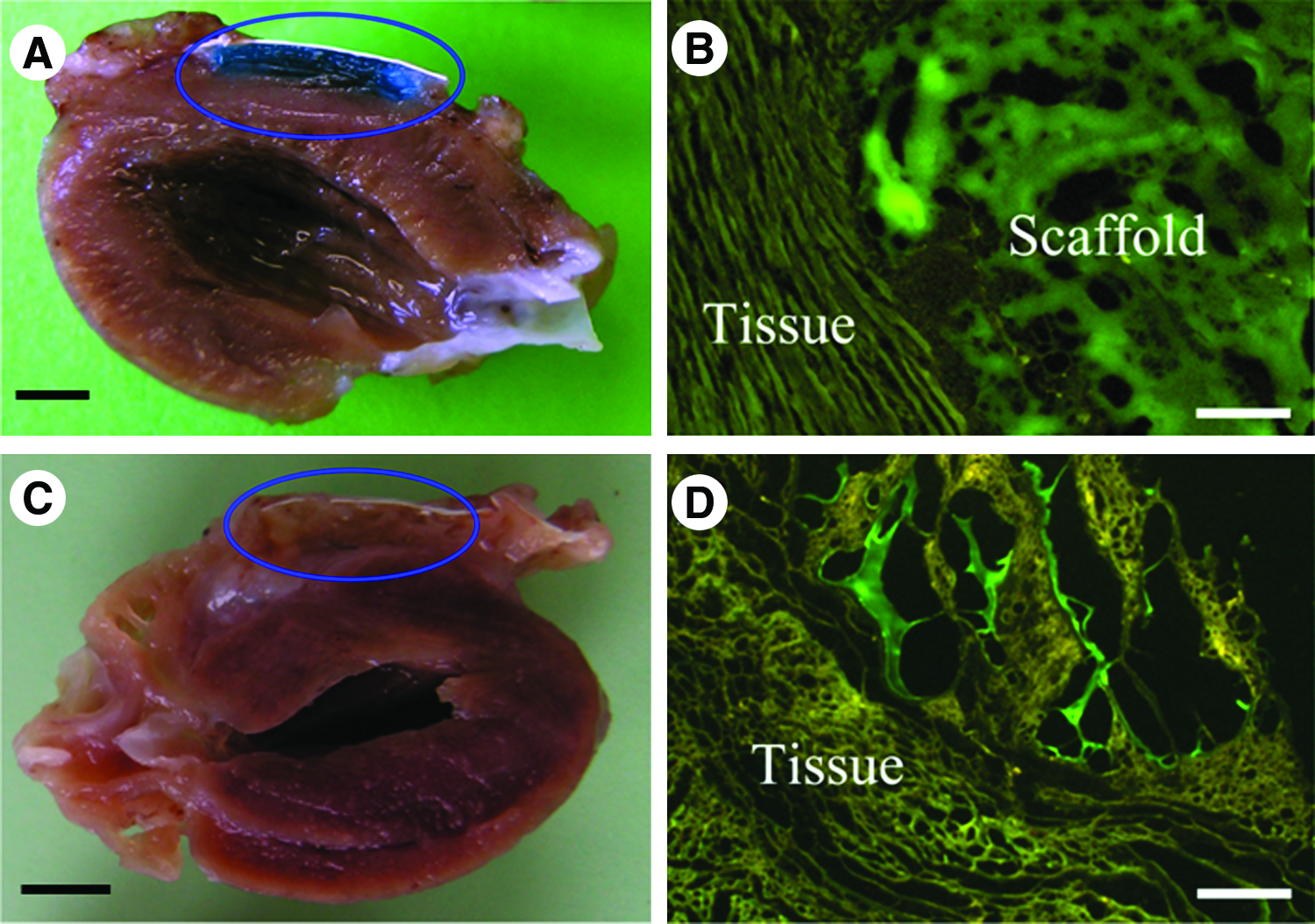
Implantation of scaffolds on rat heart. One month after implantation, scaffold on normal cardiac tissue was found intact
Engraftment of MSC
Typical MSCs were obtained and characterized by their spindle shaped morphology (Fig. 3A) and a CD45-CD90+, CD45-CD29+ and CD45-CD106+ phenotypic profile. From the third passage, CD45-CD90+ cells represented 93%±3% of the cultured cells (Fig. 3B). Additionally, under appropriate inducing in vitro conditions, rat MSCs could display osteogenic, chondrogenic, and adipogenic differentiation (Fig. 3C).
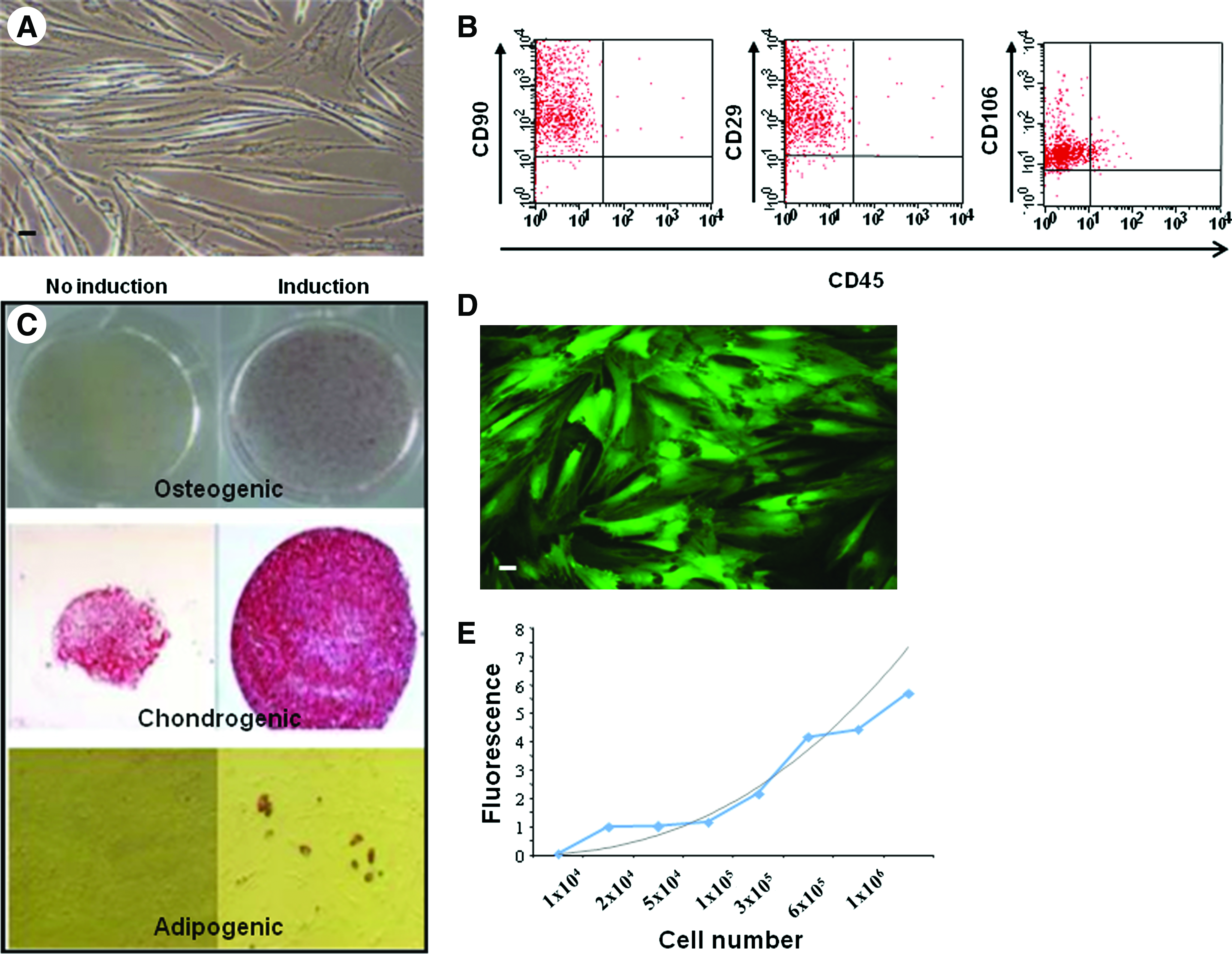
Cell transfer into myocardium. MSCs were characterized by their spindle shaped morphology, scale bar: 20 μm
Quantification of cell engraftment into the infarcted heart was performed using MSCs transduced with a lentiviral vector that expresses eGFP (Fig. 3D). The transduction efficiency of MSCs assessed by FACS as a percentage of GFP+ cells reached 98.8%±2.5% (n=3). The number of residual eGFP+ cells was estimated by quantitative reverse transcription (RT)-PCR, after calibration with defined numbers of sorted eGFP+ MSCs (Fig. 3E). One month after administration of 1×106 eGFP+ MSCs, the median number of eGFP+ cells in the myocardium was greater after administration using scaffold than after EC injection with, respectively, 9.7% and 5.1% of the administered cells in the myocardium (Table 1). Engraftment was confirmed at 2 months. The median number of eGFP+ cells in the scaffold group and EC group represented 16% and 6.1% of the initial administered cells, respectively (n=5).
Results were expressed as a median value of GFP+ cells (with range) and as a percentage of engraftment (n=5 per condition). No significant difference was observed between groups.
EC, endocardial.
MSC localization
We then examined the ability of MSCs to migrate from the scaffold to the targeted tissue. MSCs localization was examined using eGFP+ cells or cells double-labeled with a fluorescent dye PKH26 and BrdU (n=3). When cellularized scaffolds were implemented on healthy myocardium, no labeled cells were detected in cardiac tissue. On the contrary, 1 month after implantation of cellularized scaffold on injured myocardium (Fig. 4A), immunofluorescence staining detected numerous PKH-labeled cells in the thin peri-infarcted cardiac tissue (Fig. 4B); some BrdU-positive MSCs were also observed in the same border area (Fig. 4C). This suggested the influence of attractive signals from infarcted area to induce cells moving from the implanted scaffold toward the targeted area (Fig. 4D). These data were confirmed using eGFP+ cells. In animals having MSCs implemented on scaffold, clusters of GFP+ cells were clearly detected in the peri-infarct area and in bordering healthy myocardium, 1 month (n=3) and 2 months (n=3) postinfarct (Fig. 4E) but no GFP+ cells were detected within the infarct area. Most of the cells weakly co-expressed the CD106 marker indicating that the infused cells remained mainly phenotypically consistent with immature MSC cells (data not shown). Nevertheless, few cells expressed the cardiac tissue-specific marker, α-actinin (Fig. 4E) and connexin 43 (data not shown).
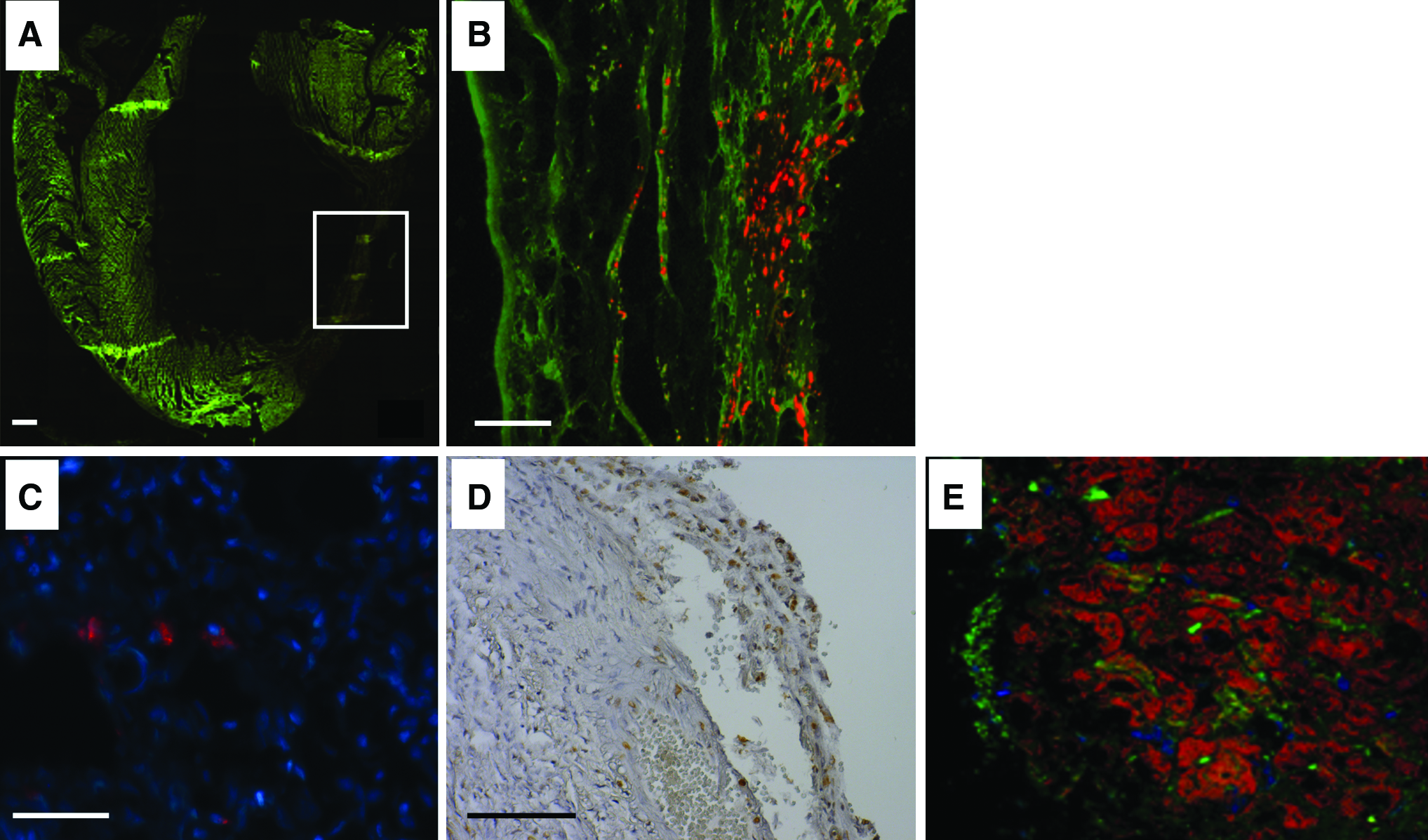
Cell localization in infarcted area. Microscopic observation of green autofluorescent cardiac tissue
Ventricular remodeling and biochemical modifications after MSC delivery using scaffold or EC injection
It is believed that MSCs sustain the heart repair predominantly by facilitating endogenous processes, through paracrine effect particularly on scar formation and neovascularization. H&E (Fig. 5A, top row) and sirius red (Fig. 5A, bottom row) staining in histological heart sections were examined in animals having received cellularized scaffold or EC injection. Sirius red staining indicated collagen production into the infarcted area related to fibrosis. Quantitative measurement of fibrosis area on cardiac sections showed a trend, but not reaching significance, toward the reduction of fibrosis in the scaffold group compared to EC group (12%±1% vs. 16%±3%, respectively) (Fig. 5B).

Histology and RT-PCR analysis.
We also measured the local production of MMP-2 and MMP-9 using qRT-PCR. MMP-2 and MMP-9 mRNA per milligram of infarcted hearts were similar 1 and 2 months after MSC administration, whatever the delivery condition (not shown). In contrast, VEGF mRNA level was significantly higher 2 months after administration in the scaffold group (Fig. 5C, bottom row; p<0.05).
Echocardiographic and catheterism studies
Functional assessment by echocardiography was performed 7 days and 2 months after myocardial infarction and cardiac graft implantation. At the baseline (7th postoperative day) LVEDD, LVESD, and LVFS were similar in both EC (respectively, 7.0±1; 5.5±1; 21.8±6.7; n=9) and scaffold groups (respectively, 7.4±1.8; 5.4±1.8; 27±9.2; n=9) as in the control group having received noncellularized scaffolds (respectively, 7.3±1.2; 5.2±1.4; 30.5±9.9; n=9). Progressive left ventricular dilatation and deterioration of LVFS were observed in the control group at 2 months. On the contrary, there was a trend toward a higher LVFS and a lower LVESD in the cellularized scaffold group at 2 months (Fig. 6).
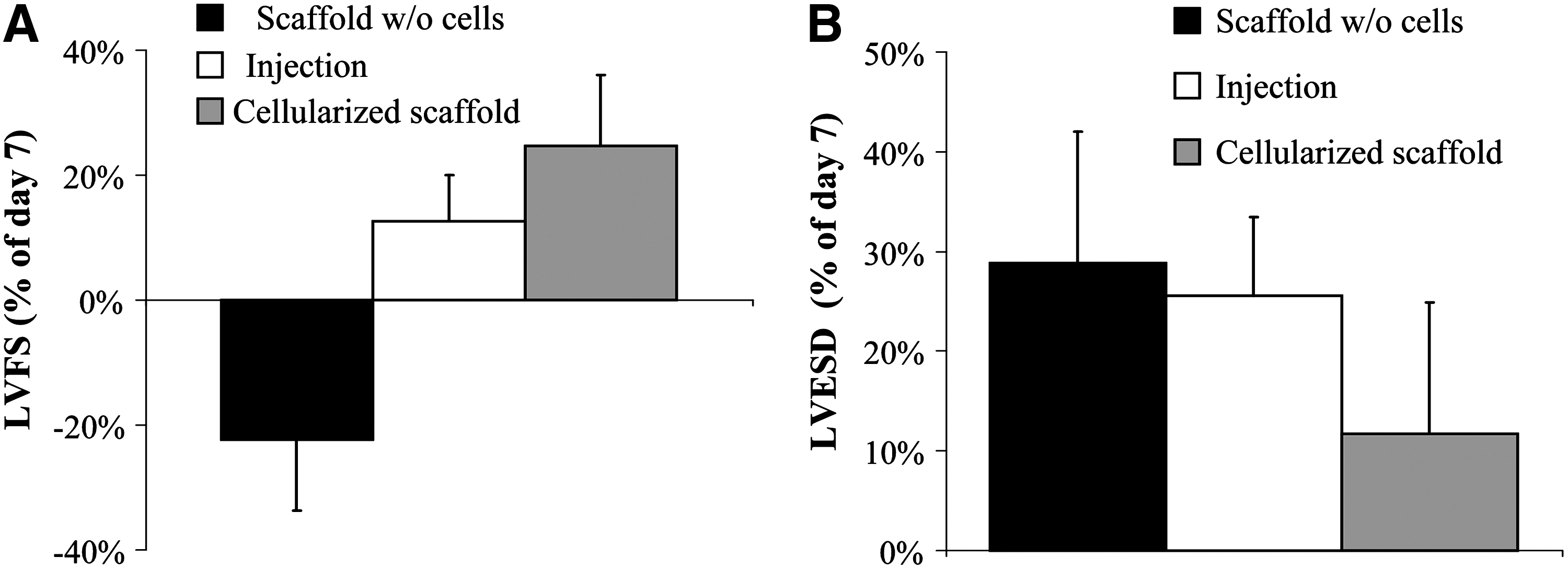
Functional assessment by echocardiography. Echocardiography was performed at 7 days and 2 months after myocardial infarction and results are presented as a percentage of day 7 value for animals having received either a control scaffold without cells, endocardial injection or a cellularized scaffold (n=9). LVFS: left ventricular fractional shortening
Discussion
The approach to administer stem cells for cell therapy is mainly dependent of our ability to safely ensure sufficient delivery of cells within the target tissue and adequate local engraftment and function at this site. Different delivery strategies are required with regard to delivered cell types. For cardiac tissue, the intramyocardial route is suited to large, adherent cells and has been safely used for MSC infusion but suffers of a low engraftment rate. The potential interest of scaffolds in cardiac cell therapy is increasingly investigated to repair damaged tissue.14,15 The use of cells in combination with appropriate scaffold should provide not only a physical support for cell orientation and proliferation but also molecular cues to direct cell survival, cell cycle progression, and the expression of different phenotypes. 16 In this context, cell-seeded biocompatible cardiac patches could be considered as a promising approach. This study was designed to evaluate quantitatively MSC delivery in ischemic myocardium using a three-dimensional (3D) scaffold in comparison with EC injection. Using a novel chemical cross-linking process combined with a porogen agent, polysaccharide-based porous scaffolds were prepared. MSCs were seeded into this porous scaffold that supports rapid integration of seeded cells. The hydrogel structure would allow exchange of oxygen, nutrients, and metabolites inside the porous scaffold, as well as the diffusion of cells. We found that homing of MSCs from the scaffold to myocardium required a signal such as infarct remodeling. After 30 days, cell delivery was associated with a greater number of engrafted cells when compared to EC delivery, with about 10% of the initial seeded cells present in the scaffold group, in comparison with 5% after EC administration. This concurred with the MSC engraftment rate previously reported by Freyman et al. after EC delivery in a porcine myocardial infarction model. 4 Differents factors could contribute to the improvement of cell delivery after implantation using a porous scaffold. A scaffold would provide a cell-friendly micro-environment as well as a substrate for the transplanted cells that would prevent cell loss. 17 It could also act as a mechanical support to enhance cell survival and cell proliferation. Indeed we observed an increase in GFP+ cell number from 1 to 2 months after implantation, although this increase was not statistically significant. This suggests that a slight proliferation of implanted MSCs occurred.
Even if the mechanism of cardiovascular repair from adult stem cells remains highly unknown, it is believed that MSCs act through paracrine actions. In agreement, a significant, despite modest, difference in the mRNA level of VEGF between scaffold and EC group was achieved here at 2 months, although no improved vascularization was evidenced (data not shown).
Quantitative analysis of engrafted cells was performed using GFP+ transgenic cells. In comparison with engraftment assessment using immunohistochemical analysis that samples only a small fraction of the myocardium, this method enables the quantification of a low number of residual cells and their accurate detection through the entire myocardium. To our knowledge, this is the first time that cellular engraftment and survival in injured myocardium were measured by quantitative RT-PCR. Internalized iridium technique, as performed by Freyman et al., offers quite similar interest. 4 Overestimation linked to nonspecific labeling of macrophages after phagocytosis of dead cells can be excluded with this method. In contrast, underestimation could be related to a potential immune reaction to GFP+ cells or to silencing of the GFP reporter gene during the process of differentiation, although these risks are not usually expected.18,19 The relationship between GFP quantification by RT-PCR and cell number was thus determined by analyzing heart samples with known number of cells.
Some experimental studies in large animal models and early clinical trial support the concept that MSCs improve heart function after myocardial infarction. Our seeded scaffold group demonstrated a trend toward an improvement of ventricular functions and fibrosis size. To expect better clinical effects, the number of seeded cells should be considered. Pouzet et al. have shown that there was a linear relationship between efficacy of functional improvement and the number of injected cells. 20 A recent study in a large animal model revealed evidence of a dose-response effect to the MSC therapy after surgical injection and only a high dose of 200×106 MSCs reduced infarct size. 21 MSC delivery using the EC method is limited by the adverse events reported with high cell concentration and injection volume of 0.3 mL. In contrast, the initial number of cells can be easily increased using larger scaffolds; large porous scaffolds (2 cm in diameter) containing 200×106 autologous bone marrow-derived MSCs are currently implanted in a pig model of myocardial infarct. We are also conducting a dose-effect study with GFP+ cells to evaluate the relative contribution of cell engraftment to functional recovery. At the moment, limited functional data with GFP labeled cells suggested that a residual number of 3×105 MSC could sustained a regenerative effect.
PTFE membrane could be also involved in the lack of significant benefit in terms of functional improvement in animal receiving cellularized scaffold maintained using this membrane. Significant foreign body reaction and undesirable fibrous membrane with fibroblast proliferation has been reported using PTFE membrane22,23; we observed by ourselves that membrane alone altered the epicardial anatomy. Control groups did not include the use of the PTFE membrane. At the time of the study, the membrane was the more convenient system to maintain our scaffold on the myocardial injury but we are now considering others devices.
Another approach is to construct 3D functional tissues by layering 2D cell sheets.24,25 This system allows for cell interconnection with gap junctions, resulting in electrically synchronous beating. Hamdi et al. recently compared such a bilayer myoblast cell sheet and a myoblast seeded collagen sponge. 26 In both cases, significant improvements in left ventricular ejection fraction compared with the controls were reported but could not be related to the detectable persistence of the myoblasts at the studied time point neither to an increased cytokine production. Residual cells were more abundant in the patch-treated hearts than in those covered with the myoblast sheets and the authors suggested that the benefits of cell transplantation could be potentiated by an epicardial deposition of a preshaped cellularized patch. In their study, the number of MSC at the time of delivery was not assessed since myoblast sheets production required 7 days of culture. 26 In another study, cells were embedded into a type I collagen matrix secured to heart with a fibrin sealant then cultured for 7 days. Despite high initial engraftment rates at 1 week, no human MSCs or residual patches were detectable at 4 weeks. 27 Addition of bioactive factors could modify the scaffold to specifically recruit stem cells in the cardiac injury site. 28 An injectable MMP-responsive, bioactive hydrogel was recently described as an in situ forming scaffold to deliver vascular cells derived from human embryonic stem cells. 29 Tissue-engineered cardiac grafts were also prepared by using various biomaterials such as small intestine submucosa 30 and biodegradable porous alginate scaffolds, cultured for 4 to 7 days before implantation. 31 However, insufficient cell migration into scaffolds and inflammatory reaction due to scaffold biodegradation were reported. In comparison, our approach did not require any delay between seeding and implantation. Indeed, a fast infiltration of cells within the porous scaffold led to a cellularized patch that could be implanted rapidly and seeded cells were thus evidenced here 1 and 2 months after scaffold implantation. A complete degradation of the scaffold was observed after implantation on infarcted tissue, but not on normal cardiac tissue. We have preliminary evidence of scaffolds degraded in vitro by leukocyte hydrolytic enzymes such as acid and alkaline phosphatase, as well as lysozyme, activities (unpublished results). Acid phosphatase and lysozyme have been shown to be more active in patients with acute myocardial infarction and might contribute to the in vivo degradation of scaffolds. 32 This complete degradation of the scaffold that was observed within a month might have promoted the local engraftment and survival of the cells.
In conclusion, we showed the feasibility to deliver MSCs to injured rat myocardium using a polysaccharide porous scaffold that improved engraftment in comparison with the most currently used approach of EC injection. Refinements of this approach, such as using injectable porous scaffolds containing appropriate molecules for cell differentiation or maintenance and sustained degradation profile may serve to enhance any benefits gained by cellular cardiomyoplasty.
Footnotes
Acknowledgments
This work was supported by Inserm, Universities Paris 7 and Paris 13 and in part by Fondation de France, Fondation de l'Avenir (IM7-475) and grants from Agence Nationale de la Recherche (ANR-09-EBIO-001 3D and ANR-08-BIOT-012). Olivier Gournay was a recipient of “Société Française de Cardiologie”. Sofiane Hamidi is a recipient of a DIM STEM-Pole Ph.D. fellowship. We are grateful for the assistance of E. Balse (Inserm UMRS 956, Paris) for immunofluorescence staining, L. Louedec for animal care (Inserm U698, Paris) and F. Nadaud (UTC Compiègne, France) for ESEM images.
Disclosure Statement
No competing financial interests exist.