
Abstract
Tissue engineering technique seems to be the best strategy for treating the urethra disease in the near future. In present study, porcine acellular corpus spongiosum matrices (ACSMs) were combined with autologus corporal smooth muscle cells (CSMCs) and lingual keratinocytes by static-dynamic seeding method to form three-dimensional (3D) “neourethra” tissue for repairing the urethral defection. Six scaffolds with two kinds of cells (Group C), six scaffolds with only lingual keratinocytes (Group B), and six matrices alone (Group A) were used to repair the rabbit urethral defection. Retrograde urethrography and histological analyses were performed to evaluate the results of urethroplasty. In vitro, hematoxylin and eosin staining of seeded ACSM showed multiple epithelial layers and well-distributed CSMCs into the matrix. In vivo, the urethra kept a wide caliber in Group C. Strictures were observed in groups A and B. Histologically, the retrieved urethra in group A showed fibrosis and inflammation during 6 months. Simple epithelial layer regenerated in group B while there was no evidence of CSMCs growing into grafts during study period. Stratified epithelial layer and organized muscle fiber bundles were evident after 6 months in group C. Our study suggested that lingual keratinocytes and CSMCs could be used as a source of seed cells for urethral tissue engineering. Using the dynamic-static seeding method, 3D urethra could be constructed in vivo.
Introduction
Acellular matrices and cell-seeded constructs have been used in patients with urethral strictures.7,8 It was hypothesized that building a three-dimensional (3D) urethra structure will minimize the inflammatory response toward the matrix, thus avoiding graft contraction and shrinkage. 9 Therefore, we cultured autologus lingual keratinocytes and corporal smooth muscle cells (CSMCs) and then seeded them onto the acellular corpus spongiosum matrix (ACSM) to obtain a new kind of 3D urethral tissue.
Materials and Methods
Scaffold preparation
Porcine penile tissues were harvested from anesthetized male white pigs weighing 20–25 kg. For the ACSM, corpus spongiosum matrix was separated from the corpus cavernosum. Isolated matrices were stirred for 14 days at 37°C to induce cell lysis using 1% Triton X-100 (Sigma) and 0.1% (v/v) ammonium hydroxide. Hematoxylin and eosin (H&E) staining was used to identify whether all cells were removed from scaffolds. Then they were stored in 0.25% chloramphenicol solution before use.
Scaffold evaluation
Uniaxial tensile mechanical testing was conducted under normal room temperature. Normal rabbit urethra was chosen as the control tissue. Before testing, all tissues were rehydrated in the phosphate-buffered saline (PBS) solution for 30 min. The Young's modulus, stress at break, and strain at break were determined using the manufacturers' software.
Scanning electron microscopy (SEM) was performed to investigate the pore size of each surface. First, all samples were dehydrated in graded ethanol (50%–100%). They were dried using supercritical carbon dioxide extraction, coated with gold, and then examined with SEM (Jeol 6300-F). The pore sizes of the scaffold of each sample were measured at five different areas using a computerized system.
Cells isolation and characterization
Eighteen 10-week-old male rabbits were used in this study, and a 1.0×0.5 cm piece of lingual mucosa was taken from 12 rabbits. Lingual keratinocytes were dissociated form the specimens using Dispase II (Roche) and isolated in keratinocyte serum-free medium (KSFM; Gibco). The cells were expanded to a density of 1.1–2×106 cells/cm2 for seeding. 10
From these 12 rabbits, we obtained autologous cavernosal tissues from 6 and digested those tissues in 0.5% collagenase I (Worthington). Enzymatic digestion was terminated by adding 10 mL Dulbecco's modified Eagle's medium (DMEM) supplemented with 10% fetal bovine serum. A differential velocity adherent technique was used to purify the CSMCs. The isolated CSMCs were expanded to a density of 2×108 cells/cm2 for seeding. 11
The cultured cells were identified using an immunofluorescent staining method. To determine the lingual keratinocytes, the mouse monoclonal antibody AE1/AE3 (Abcam) was used; the CSMCs were identified by alpha smooth muscle actin (α-SMA) and myosin (Sigma Chemical Co.). In addition, the purity of cultured cells was analyzed by flow cytometry using α-SMA and AE1/AE3 (FACS Calibur; Becton Dickinson).
Cell seeding
To seed the ACSM, CSMCs and the lingual keratinocytes were gathered at the fifth and third cellular passages, respectively. Then, seven scaffolds (1×2 cm each) were seeded with those cells using a dynamic-static seeding method. 12 Briefly, all scaffolds were first sterilized using compound iodine solution for 1 h. After being carefully washed by PBS, they were blotted using sterilized papers. Then, 500 μL of a CSMC suspension (2×108 cells/mL) and ACSMs were placed in 50 mL tubes on an orbital shaker and agitated at 250 rpm for 6 h. All compound scaffolds were cultured in DMEM for 1 week, refreshing the culture fluid every 3 days. Subsequently, lingual keratinocytes were gathered and poured onto the urethral surface of the ACSM. The cells were allowed to settle and aggregate in the incubator for 3–4 h, followed by addition of enough medium (DMEM:KSFM, 1:1) to culture the compound at an air–fluid level. Seven additional days of incubation was needed for cell expansion; the medium was changed daily. Another seven scaffolds were seeded only with lingual keratinocytes by using the aforementioned static method. All compound grafts were assessed using H&E staining and immunohistological analysis.
Rabbit urethroplasty
For the animal experiment, 18 New Zealand white rabbits were classified into three groups of 6 rabbits each. Group A was given unseeded grafts, group B was given autologous lingual keratinocyte-seeded grafts, and group C was given grafts seeded with autologous lingual keratinocytes and CSMCs. All rabbits were anesthetized with pentobarbital and an 8F transurethral catheter was placed in situ. The urethra was mobilized from the corpora through a ventral midline penile skin incision. A ventral urethral defect with a mean length of 1.5 cm and width of 0.8 cm was created in those rabbits' anterior urethra, about 2.0 cm from the external urethral orifice. The compound grafts were placed over the defect as an onlay. The urethral repair was performed with 6-0 vicryl sutures applied in a continuous fashion. Multiple nonabsorbable marking sutures were placed at the anastomatic margins. The catheter remained for 14 days after operation.
Two animals in each group were euthanized at 1, 2, and 6 months postimplantation after the urethral caliber was assessed with retrograde urethrograms. The entire urethra was then removed and assessed by viewing the mucosal membrane with sections of tissue subsequently stained with H&E staining. The epidermal cell layers were identified by immunohistochemistry for the AE1/AE3. To verify the smooth muscle cells in the repaired urethra, immunohistochemical staining with α-SMA and myosin was used. Immunohistochemical staining with T-cell–specific antibody (UCHL-1), B-cell–specific antibody (CD20), and macrophage-specific antibody (CD68) were also used to identify the inflammatory cells in wax sections.
Results
Scaffold evaluation
After decellularization, histological results showed that ACSMs were completely acellular (Fig. 1a, b). This kind of scaffold demonstrated a good response to Young's modulus and stress at break, which was better than normal rabbit urethra (Table 1). In additional, the pore diameters of the urethral surface were significantly different from the cavernosal surface in the ACSM (2.04±0.32 μm vs. 11.12±1.43 μm; p<0.05; Fig. 1c, d).
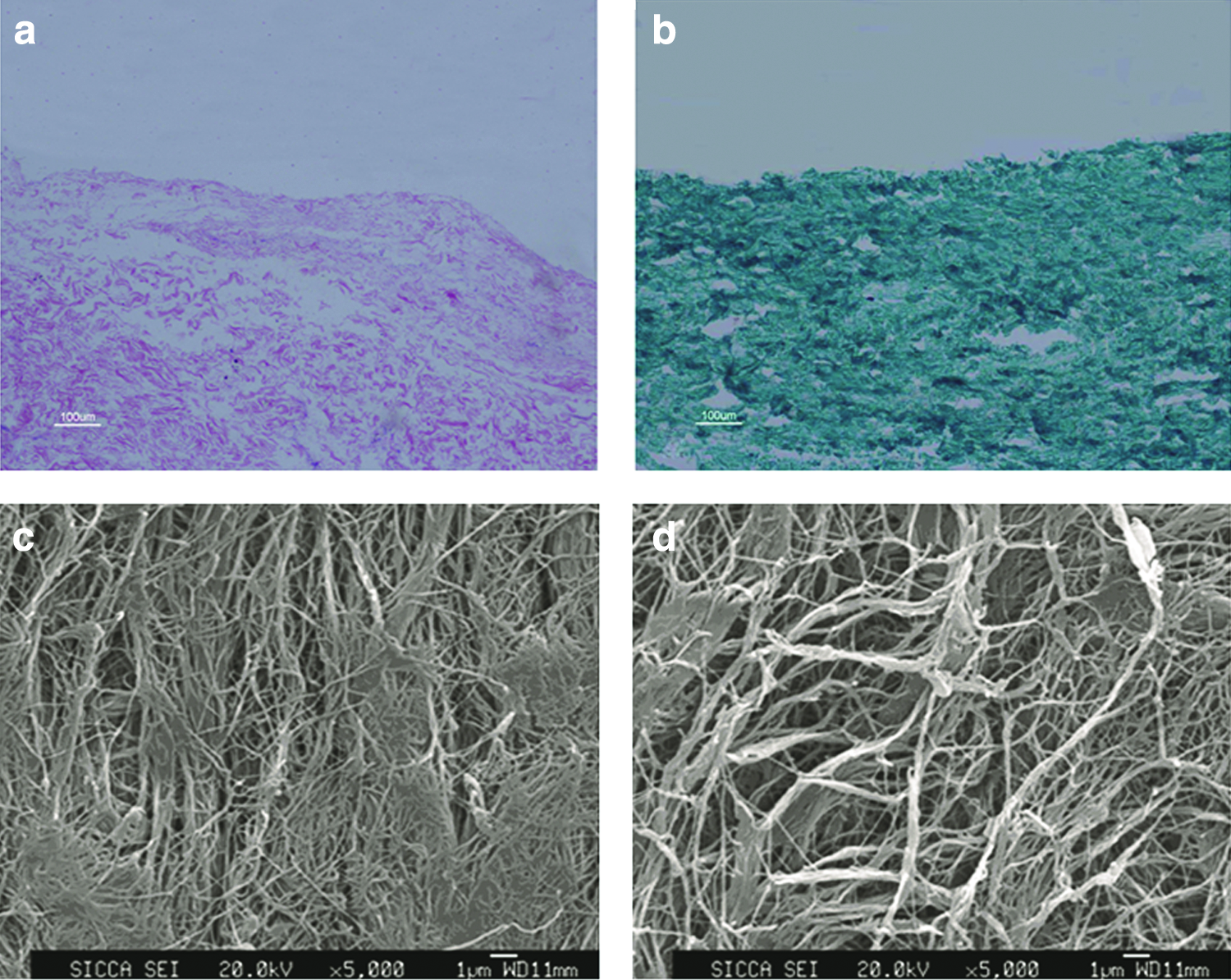
Histological and EMS examination of ACSM.
p<0.05.
ACSM, acellular corpus spongiosum matrices.
Cell culturing and identification
After incubation for 2–3 weeks, the CSMC population covered 90% of the culture plate, with the cells showing a “hills and valleys” phenotype. Immunofluorescent staining demonstrated that these cells expressed α-SMA and myosin. The lingual keratinocytes showed a typical cobblestone shape. Immunofluorescent staining also showed the cellular response to AE1/AE3 markers (Fig. 2). In flow cytometry analysis, the purity of the fifth-passage CSMCs was 91.2% as analyzed using α-SMA. The purity of third-passage lingual keratinocytes was 90.3%, as analyzed by flow cytometry using AE1/AE3. As the other cells were of spindle shape and grew fast, we believed that they were all fibroblast cells.
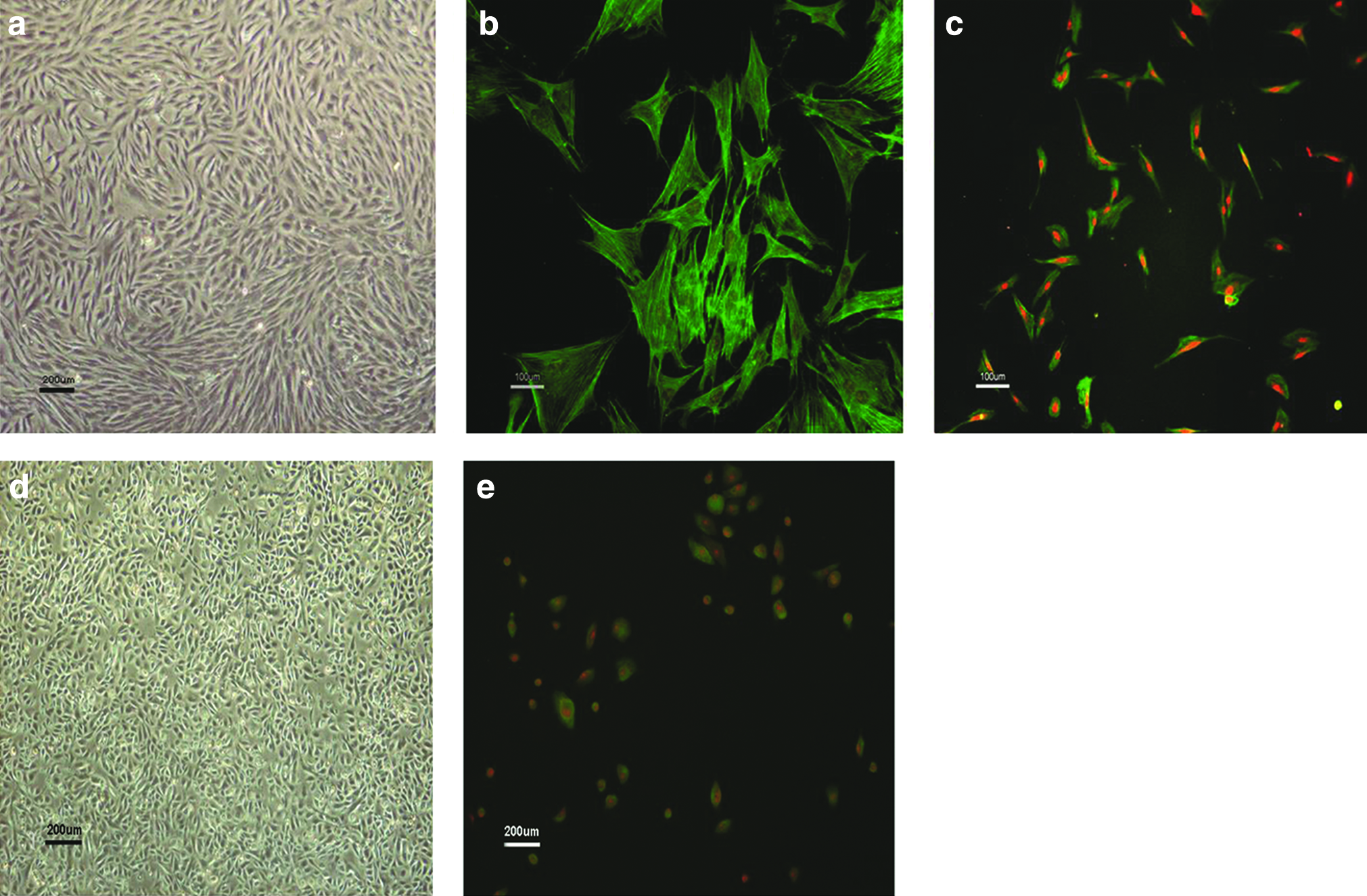
Morphology and identification of CSMCs and lingual keratinocyte.
Cell seeding in vitro
H&E staining showed that the compound matrices had one to two epidermal layers confirmed with AE1/AE3 at 7–14 days after the dynamic-static seeding. Further, we were surprised to see that CSMCs, identified by α-SMA and myosin, were distributed into the scaffolds. Most importantly, the epidermal cellular layers and smooth muscle cells were easily distinguished in the sections.
Compound matrix for urethroplasty in vivo
All rabbits in each group survived until sacrifice. There were no oral or penile complications, such as difficulty in eating, bleeding, and hematoma during the 6-month postoperation period. No animal had noticeable voiding dysfunction during the study period.
No animal showed evidence of a fistula or diverticulum in the urethrogram. However, group A revealed strictures at 1 and 2 months after surgery. In group B, a slight narrowing of the urethra near the operation site was found at 1 month postoperatively, which ameliorated after several months. The animals in group C maintained a wide urethral caliber without any sign of strictures (Fig. 3).

Comparison of urethrography image in each group at 1, 2, and 6 months after operation. Arrow indicates the stricture site of urethra.
Under macroscopy, severe fibrosis and shrinkage were observed in group A at each time point. Progressive narrowing and marked shrinkage of implanted matrices were also found in group B. In contrast, gross examination at retrieval in group C demonstrated normal-appearing tissue without any evidence of fibrosis or scarring at the end of 6 months (Fig. 4).
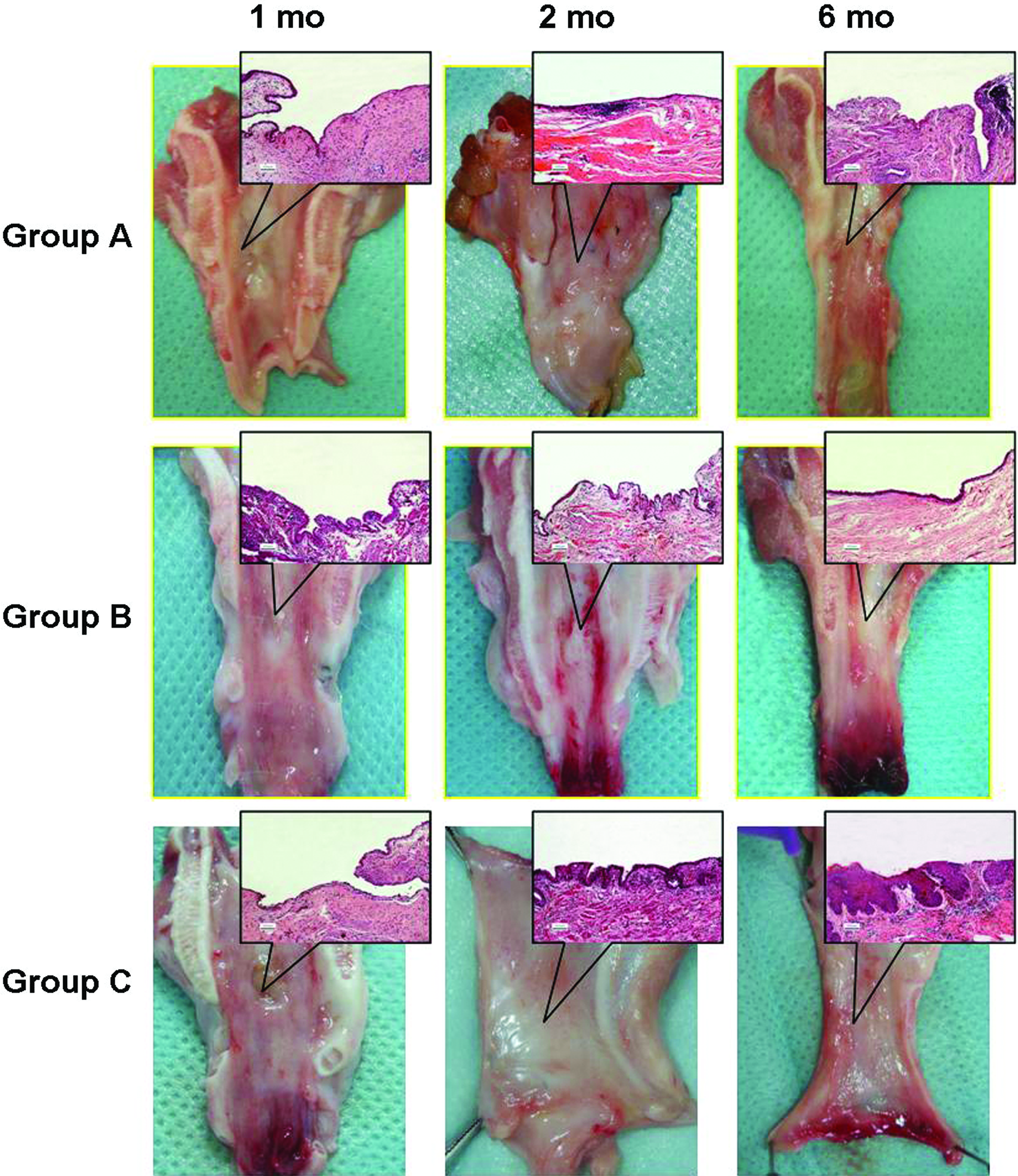
Macroscopic inspection and H&E staining (inset) of retrieved urethra in each group at 1, 2, and 6 months after operation. In group A, urethral stricture existed at each study time point. H&E staining did not show the continuous epithelial layers, but severe inflammatory reaction could be found in H&E sections. In group B, strictures were still noticed in gross inspection. Only one to two epithelial layers were formed at 6 months after implantation. In group C, patent lumen without stricture sign could be observed by the end of 6 months. Also, multilayer squamous epithelial layers covered the surface of urethra. H&E, hematoxylin and eosin. Color images available online at www.liebertonline.com/tea
Histologically, the discontinued epidermal layer developed on the lumen surface of retrieval urethra in group A at 1 and 2 months after surgery. However, the cellular layer did not completely regenerate at the end of 6 months. Also, there was no evidence of smooth muscle cells growing into the compound graft during the study period. Further, progressive infiltration of inflammation cells was observed, representing a chronic inflammatory reaction (Fig. 5). Some giant cells could be seen in those sections. Further immunohistochemical results demonstrated that 10%–20% of the cells responded to the UCHL-1 or CD20 marker. Another 10% of cells were positive for the CD68 marker (Fig. 6).

Immunohistochemical analysis of retrieved urethra in group A at 1, 2, and 6 months after operation.
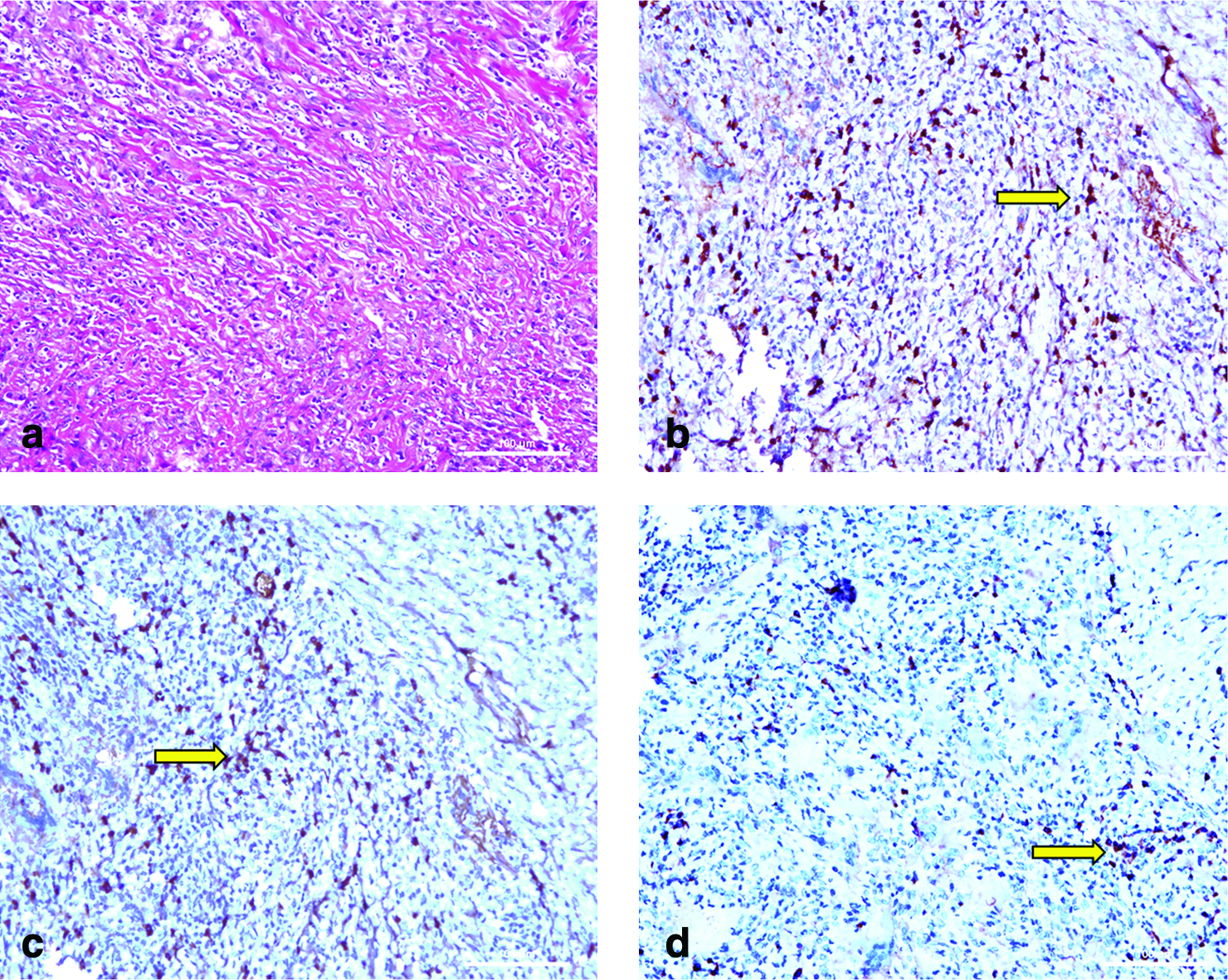
H&E staining and immunohistochemical analysis of retrieved urethra in inflammatory site.
In group B, an intact epidermal cellular layer formed at 1 month. The cellular layer continued to increase to two to three layers for another month but then did not change at the end of 6 months. Unorganized muscle fiber bundles were evident with histological analysis at 1 month after implantation. Nevertheless, no evidence of increasing muscle bundles could be identified at 6 months after surgery. A minimal number of inflammatory cells were present after surgery (Fig. 7).
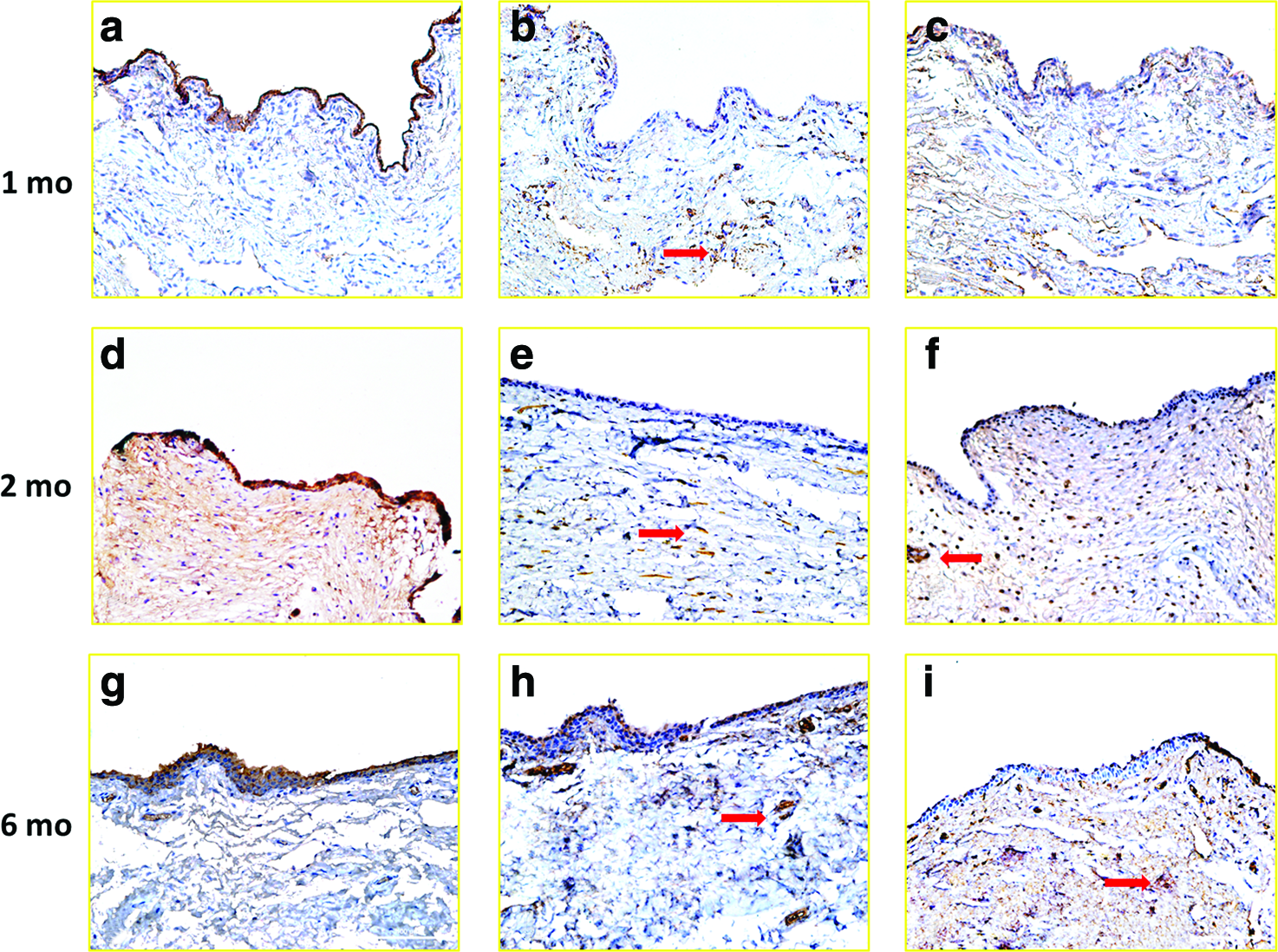
Immunohistochemical analysis of retrieved urethra in group B at 1, 2, and 6 months after operation.
In group C, the epidermal cellular coverage was regenerated in the one layer with minimal inflammatory cells at 1 month after surgery. A well-developed five to seven layers of stratified keratinocytes was present. Increased numbers of organized muscle bundles were observed at 2 months. Normal-appearing organized muscle fiber bundles were evident at 6 months after implantation (Fig. 8).
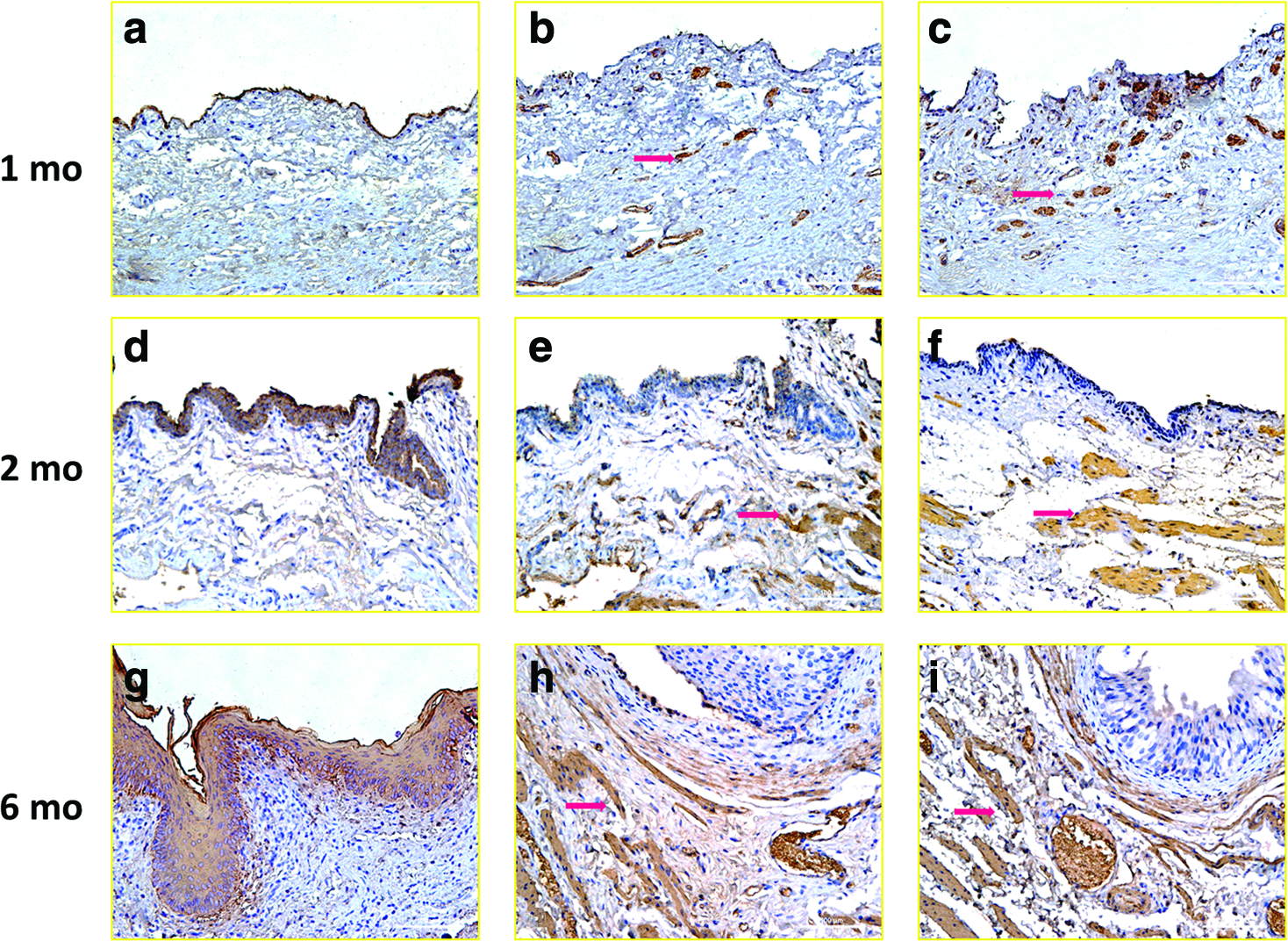
Immunohistochemical analysis of retrieved urethra in group C at 1, 2, and 6 months after operation.
Discussion
Many tissues have been used for urethral reconstruction, including vascularized or free grafts of skin, buccal, lingual, or colonic mucosa.2–4 The limited amount of autologus donor tissue confines the urethral reconstruction, especially for those patients with long segment of strictures. Clinically, cellular matrix patches, especially porcine small intestinal submucosa, have been proven to be feasible in patients for urethroplasties with short length of urethral strictures. 13 In animal experiments, cell-seeded scaffolds have been successfully used to repair longer urethral defections in rabbit model.5,8 However, few investigations have tried to construct artificial urethra, including urethral mucosal and cavernosal muscle layers, beyond simple tissue-engineered urethral mucosa. It has also been hypothesized that building 3D structure constructs in vitro prior to implantation would facilitate matrix vascularization in vivo and minimize the inflammatory response toward the matrix. 14 Therefore, the advent of urethral tissue-engineering technology requires reconstructing the 3D “neourethra.”
Because acellular collagen scaffolds can be loaded with bioactive signals that can regulate cellular function, we chose ACSM, a type of acellular collagen matrix, as the biomaterial in our study. There were several reasons to use ACSM as a new type of biomaterial in this study. First, the length of the porcine penis is enough to generate large scale matrixes for this experiment. Second, the excellent mechanical properties in ACSM suggested that this matrix may prevent the occurrence of fistula or diverticula, the most common complications after urethroplasty. 15 Moreover, different pore sizes in each surface of ACSM may be suitable for seeding different kinds of cells. According to Bernhard's theory, 16 the small pore sizes on the urethral surface make it suitable for forming multilayer epithelial coverage. Using compound iodine solution instead of ethanol to sterilize the scaffold before seeding, we could preserve intact 3D structures, avoiding scaffold contraction. Therefore, the pore diameters on the cavernosal surface were large enough for smooth muscle cells to infiltrate and grow. However, we must mention that we mainly reported a new type of biomaterial in our study. The source of ACSM should be further investigated.
In this experiment, we chose the onlay type of ACSM to repair the urethral defection (1.5 cm) as the control group because of some considerations. Although some studies have shown that an acellular scaffold could be used to repair the urethral distraction within 1 cm, 17 other reports have demonstrated that an acellular matrix was often insufficient for long defects (>1 cm) due to graft shrinkage or restriction, chronic immune reactions, fibrosis formation, and calcification.18,19 We thus created long urethral defect (1.5 cm) in our rabbit models. Moreover, Atala has admitted that limitations of nutrient and gas exchange currently restrict tissue-engineered implants to a volume of approximately 3 mm. 20 Hereby, onlay techniques could be used instead of tabularized techniques when creating the control group because of the ACSM thickness. In group A, the strictures and shrinkage were present in the study. The normal transitional layer of epithelium and muscle layer did not entirely regenerate as well, confirming that native cells could not regenerate over the defect before fibrosis took place. Interestingly, severe infiltration of inflammatory cells and fibroblasts could always be seen in group A. The immunohistochemical assay in the inflammatory site demonstrated that UCHL-1 or CD20- and CD68-positive cells were present. Also, giant cells could also be noticed in those sections, indicating that the inflammatory site consisted of giant cells, T cells, B cells, and macrophages. This phenomenon can be explained by several reasons: (1) transplant immunity still existed after the urethral reconstruction using ACSM alone, wherein a slight retention of cellular compounds within the ACSM might cause chronic immunoreactions and fibrosis; (2) the long urethral defect length limited the regeneration of native urothelium; and (3) the thickness of the scaffold hindered the penetration of vascular into the matrix.
To solve this problem, various seed cells played an important role in repairing long tissue defects. In our experiment, we harvested lingual keratinocytes as seeding cells. In clinic, the epithelial cells from a lingual site can be obtained more easily than from a buccal site or genitourinary tract. No specific instrument was necessary for cellular isolation and culturing during the lingual tissue harvest. Only minor operative wounds resulted after the procedure. Also, the cells expressed β-defensin and interleukin-8, inducing an innate immune response against microbes. 21 Therefore, the compound grafts easily resisted the infection in vitro and in vivo. In addition, the lingual keratinocytes in our study expressed AE1/AE3, which is similar to epidermal cells or buccal mucosa cells. 8 Therefore, we believed that lingual keratinocytes could be an alternation for epithelial seeding cells. Striated cellular coverage formed on the lumen of retrieved compound graft instead of the urothelian layer in the group C rabbits; invasion could also be found in the basal lamina. These results are similar to our previous study that reported seeding buccal keratinocytes onto the bladder acellular matrix. It can be believed that epithelial cellular layer developed from seeded lingual keratinocytes instead of native urothelial cells. Nevertheless, urethral stricture, which ameliorated slowly, still existed in group B. Although the patent urethral caliber could be found at 2 months after implantation, shrinkage of grafts was easily noticeable, indicating the tendency for recurrent strictures. In addition, there were fewer epithelial layers in group B than in group C, suggesting that lingual keratinocytes were insufficient for urethral reconstruction alone. Other types of seeding cells are necessary to accelerate the regenerative progression and avoid the recurrence of strictures. We then focused on CSMCs as second seeding cells in this study, which are one of the major components of the phallus.9,22,23 Clinically, CSMCs are easy to harvest through biopsy. By differential velocity adherent technique, the purification of CSMCs is enough for tissue engineering reconstruction. Recent reports also indicate that angiogenic growth factor (vascular endothelial growth factor) and its tyrosine kinase receptor (Flt-1) play an important role in penile angiogenesis and are present in CSMCs.24,25 After seeding CSMCs, we believed that the vascularity in compound grafts could be enhanced. In our study, well-developed striated cellular coverage could be observed in group C; however, this coverage was not found in group B, which only seeded lingual keratinocytes on the scaffold surface, suggesting that CSMCs may play an important role in angiogenesis ensuring epidermal cellular layer growth. In our study, organized muscle bundles could only be seen in group C; conversely, unorganized muscle bundles or few smooth muscle cells were observed in group B and group A. According to those results, we believed that the autologous smooth muscle could infiltrate into the compound biomaterial with the effect of growth factors released from preseeded CSMCs. The autologous smooth muscle cells combined with preseeded CSMCs could finally form organized smooth muscle bundles. The poor results in groups A and B also indicate that preseeded CSMCs were one of the keys to regenerate the cavernosal smooth muscle tissue. Of course, the corporal endothelial cells also play an important role in urethral regeneration. 26 Because of the difficulty in seeding three kinds of cells into the same scaffold, endothelial cells will be considered in our later studies.
We also attempted to determine the best method of seeding cells onto the acellular matrix. Growth of seed cells on acellular scaffolds with layered and sandwich coculture technique in vitro has been studied. 27 The limitation of low seeding efficiencies and minimal cell penetration into scaffolds could not be easily resolved. 28 We chose a dynamic-static seeding method to maximize the 3D cell growth into the scaffold. Several advantages are associated with the dynamic seeding method, namely, (1) increased infiltration of cells during agitation and (2) good distribution of nutrition and oxygen leading to uniform growth of cells on the matrix. 18 Further, previous reports have demonstrated that lactate dehydrogenase leakage as an index of cell damage and death was lower with agitation seeding than with static seeding, supporting that the dynamic seeding method did not do more harm to cells than the static seeding method in our study. 10 Admittedly, it is very difficult to control the cell distribution into the scaffold, as the cells gather in some areas and are sparse in other regions. This will be further studied in our later experiments.
Footnotes
Acknowledgments
This study was supported by National Natural Science Foundation of China (30772159), Doctor Research Foundation of Chinese Education Department (20070248072), and Doctor Creative Research of Shanghai Jiaotong University School of Medicine (BXJ0928).
Disclosure Statement
None of the authors has direct or indirect commercial financial incentive associated with publishing this article.