
Abstract
The ability of recombinant human bone morphogenetic protein 2 on absorbable collagen sponge (rhBMP2/ACS) to regenerate bone in segmental defect has been well characterized. However, clinical results of rhBMP2/ACS constructs in secondary reconstruction of large mandibular and craniofacial defects have not been consistent. We hypothesized that rhBMP2 delivery triggers an endogenous response in the soft tissues surrounding the defect, in the form of expression of BMP2 and vascular endothelial growth factor (VEGF). Such osteogenic response will occur only after immediate, as opposed to delayed, rhBMP2 delivery, suggesting a new explanation to the difference in bone regeneration between the two settings. A 35-mm segmental bone and periosteum defect was created on one side of the mandible in 16 dogs divided in three groups. Group 1 (Gp1, n=6) ACS was loaded with 8 mL of rhBMP2 (0.2 mg/mL). In Gp2 (n=5) the same dose of rhBMP2/ACS was delivered into the defect 4 weeks after surgery. In Gp3 (control; n=5) the defect was reconstructed using ACS loaded with 8 mL of buffer only (devoid of rhBMP2). Tissues were collected after 12 weeks of reconstruction in all groups. Direct measurement of physical dimensions of regenerates and bone morphometry was performed to evaluate bone regeneration. The mRNA expression of both BMP2 and VEGF in the soft tissue surrounding the defect was evaluated using real-time quantitative PCR. Both BMP2 and VEGF proteins were quantified in immunostained sections. Immunoflurescence colocalization of BMP2 and acetylated low density lipoprotein (AcLDL) was done to detect the source of BMP2. Immediate delivery yielded better bone regeneration. Both BMP2 and VEGF mRNA expression was upregulated only in Gp1 (+7.3, p=0.001; +1.53, p=0.001, respectively). BMP2 protein was significantly higher in the immediate reconstruction group; however, VEGF protein was undetected in the examined sections. Immediate delivery of rhBMP2 seemed to induce endogenous release of BMP2 from the surrounding soft tissues, an effect that was lacking in delayed delivery and may explain the variability of clinical results associated with BMP2 use. Colocalization of BMP2 and endothelial cells (ECs) suggested that ECs could be the source of endogenous BMP2.
Introduction
One explanation to the discrepancy between experimental and clinical results of rhBMP2 in large segmental defects may be that experimental trials have been testing immediate rhBMP2 delivery, where implantation is done at the same setting when the defect is created. In many clinical instances, on the other hand, the implantation is done at a delayed setting, during secondary reconstruction.5–8
In theory, delayed reconstruction of large segmental defects in the mandible is expected to be more taxing than immediate reconstruction. In immediate reconstruction, the biological process of graft incorporation is comparable to that of fracture repair. 9 The healing cascade starts with the surgical hematoma into which an inflammatory response is triggered. This inflammatory reaction is crucial for the healing process. 10 If the fracture hematoma subsides, the osteogenic stem cell population at the fracture site is diminished, retarding the early healing process of these fractures.9,11 It has been reported that a 4-day-old fracture hematoma has osteoinductive potential while peripheral blood hematoma does not. Thus, absence of acute fracture hematoma can impair callus formation, which may result in delayed union or nonunion. 12 In delayed reconstruction of critical size defects, the facture hematoma is minimal. Therefore, the endogenous microenvironment during delayed reconstruction could be less conductive to rhBMP2-induced bone regeneration than that of the immediate reconstruction.
Another possible explanation to the observed deficiency of rhBMP2 effect in some large segmental bone defects is that rhBMP2 is effective in situ for only up to 2 weeks after delivery (based on the manufacturer's information). About 60% to 75% of the initial dose of rhBMP2 is lost within the first week of its application when using ACS as a carrier. 13 Therefore, the effect of the delivered rhBMP2 needs to be sustained by endogenous mechanisms. During the remodeling phase, bone formation needs to be maintained at a higher rate than bone resorption until the optimal quantity and quality of bone regenerate is achieved. Such endogenous responses within the soft tissue bed of the defect have not yet been investigated.
Our hypothesis is that rhBMP2 delivery would elicit endogenous expression of BMP2 and VEGF in the soft tissue bed of the defect. Such response will be more pronounced in the immediate than delayed reconstruction, which will correlate with the quantity and quality of bone formation in the two settings. We also hypothesize that vascular endothelial cells (ECs) of the surrounding soft tissue contribute to the endogenous production of BMP2. This study suggests a novel mechanism of rhBMP2 action in large segmental mandibular defect that could, at least partially, explain why rhBMP2-induced bone regeneration is deficient in delayed reconstruction of large mandibular segmental defects, compared with immediate reconstruction.
Animals and Methods
This study included 16 skeletally mature (age >2 years) foxhound dogs weighting at least 31.5 kg. In all animals, a unilateral, 35-mm-long, linear segmental (full-thickness) defect was created in the mandible. Animals were divided into three groups: Group 1 (Gp1, immediate reconstruction group; n=6), Gp2 (delayed reconstruction group; n=5), and Gp3 (control group). The study protocol was reviewed and approved by the Institutional Animal Care and Use Committee (IACUC).
Surgical procedure
Anesthesia was performed using endotracheal isoflurane anesthesia after preanesthetic of diazepam 0.5 mg/kg IM to calm the animal and facilitate restraint. The mandibular teeth bordering the osteotomy site (fourth premolar and second molar) as well as the maxillary teeth opposing the potential defect were extracted. Root canal treatment of the left mandibular canine was performed due to the close proximity of its root to the site of drilling to secure the reconstruction plate. The left side of the mandible was accessed through a 20 cm submandibular incision. Supraperiosteal dissection was done in the area overlying the potential defect, so that the bone would be excised with the enveloping periosteum both buccally and lingually (Fig. 1).
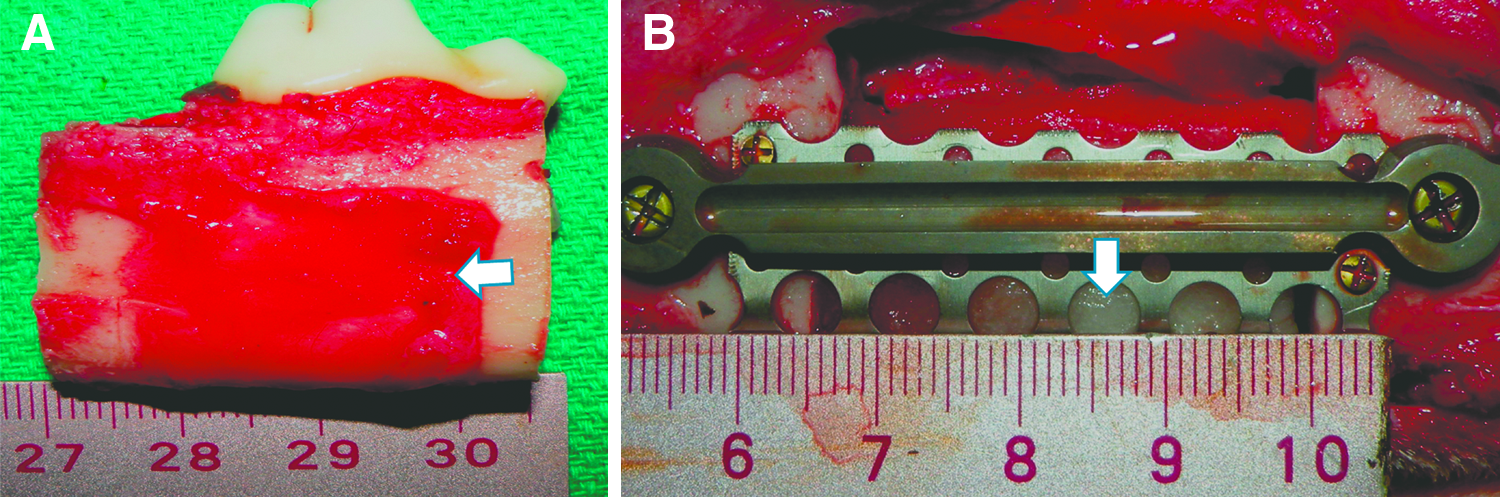
Surgical procedure.
A total of 8 cc of rhBMP2 (Medtronic, Inc.), at a concentration of 0.2 mg/mL, was infused into a 51×76 mm ACS (Medtronic, Inc.) at least 15 min before loading (total delivered dose in each defect was 1.6 mg rhBMP2). Then, the rhBMP2/ACS composite was rolled and loaded into the mesh (Fig. 1) followed by closure of intra- and extraoral wounds. In Gp1 the titanium mesh was packed with rhBMP2/ACS, immediately after defect creation. In Gp2 animals, the defect was created in the same way as in Gp1. Then the defect was bridged with reconstruction plate and titanium mesh without BMP2. Four weeks later, the defect was explored via an intraoral incision. After minor freshening of the bony edges, the rhBMP2/ACS (same dose as in Gp1) was loaded into the titanium mesh. The intraoral wound was reclosed with 3/0 PTFE. In the control group (Gp3) the defect was created in the same way and loaded immediately with ACS soaked with 8 mL of buffer free of rhBMP2.
After 12 weeks of delivering the rhBMP2 in Gp1 and Gp2 and buffer without rhBMP2 in Gp3, animals were sacrificed. Soft tissue samples immediately outside the mesh in the three groups and from the intact periosteum, of the contralateral side, were collected and properly preserved for different procedures. The regenerates with the bordering bone as well as the corresponding segment from contralateral sides were resected before the animal received a lethal dose of Penobarbital (Euthasol).
Physical dimensions of the regenerate
Using a digital caliber (Mitutoyo, Inc.), we measured the thickness and height of both the formed regenerate and the resected (original) bone segment. The anterior, middle, and posterior third heights were recorded. The upper, middle, and lower third thicknesses were measured in the anterior middle and posterior zones (thirds) of regenerates and resected pieces of bone. Percentages of the bony dimensions of each regenerate relative to corresponding dimensions in the resected bone segment were calculated. These percentages were compared between the three groups.
Three-dimensional morphometry with micro-CT
For bone mineral density (BMD) and 3D bone morphometry, samples were scanned by a micro-CT system (Skyscan 1174; Skyscan). An oversize scan was performed at an image pixel size of 66 μm. Reconstruction was done using a Skyscan Nrecon program. Datasets were loaded into Skyscan CT-analyzer software for measurement of 3D bone morphometric parameters and BMD. The 3D bone morphometric parameters measured included bone volume (BV), percent bone volume (BV/TV), trabecular thickness (Tb.Th), trabecular number/mm (Tb.N), trabecular separation (Tb.Sp), and degree of anisotropy (DA). The normal control side was used to adjust the grey scale ranging from 60 to 170. This range allowed viewing of the normal bone architecture seen in the raw images. All reconstructed images were adjusted to this grey scale before running the 3D analysis. A standardized region of interest (ROI) yielding a standardized volume of interest (VOI) (1776 mm3) was used for the 3D morphometric analysis in three different regions within the same regenerate (anterior, middle, and posterior) of each dog.
Each of the mentioned parameters was measured in the anterior, middle, and posterior zones of the regenerates and the mean was plotted as a value of each regenerate. The same VOI was uploaded to the scanned contralateral normal control side. We were cautious to avoid roots of teeth in measurements made in normal bone. Within each group, means of the measured parameters of the regenerates were compared between groups and with the parameters of the contralateral control side. Standardization of all the scanning and reconstruction parameters was done to all the scanned samples. Nomenclatures used were based on standards of the American Society of Bone and Mineral Research (ASBMR) for bone histomorphometric parameters. 14
Concerning the BMD, calibration was done using 0.25 and 0.75 mg/cc hydroxyapatite phantoms (0.8-mm diameter) provided by Skyscan. Another ROI yielding another VOI was used to calculate BMD in the anterior middle and posterior zones of the regenerates. The mean was used as the BMD value of each regenerate to compare it with the BMD of the normal contralateral side.
RNA isolation and purification
RNA isolation was carried out from three soft tissue pieces harvested from the tissues outside the mesh (treated side) and three pieces from the contralateral periosteum side (control side). Each piece was roughly 5×5 mm. Thus in each group, n=number of dogs within group X3, that is, Gp1, n=18; Gp2, n=15; and Gp3, n=15. We combined the TRIzol® reagent (Invitrogen) and RNeasy spin columns (QIAGEN, Inc.) methods for RNA isolation. Each sample was snap freeze with liquid nitrogen then grinded followed by treatment with 600 μL TRIzol® reagent for 10 min then centrifuged at 10,000 rpm for 10 min. The lysate was pipetted and equal volume of ethanol (70%) was added to it then both were gently mixed by pipetting. The procedure was then completed as previously described. 15
mRNA expression using real-time PCR
cDNA synthesis was performed using the 1 μg of the purified RNA and the High-Capacity cDNA Reverse Transcription Kit® (Applied Biosystems) with random primers in 20 μL reaction volume according to the manufacturer's instructions. The preformulated assay primers (20X mix) used in this study were individual TaqMan® Gene Expression Assays (BMP2 Ref. Seq. XM_534351.2; VEGF Ref. Seq. NM_001003175.2; Applied Biosystems), and all PCRs were carried out using the TaqMan® Universal PCR Master Mix (Applied Biosystems) on a 7300 real-time PCR system (Applied Biosystems). For analysis of both BMP2 and VEGF expression by real-time PCR, the times to cycle threshold (Ct) responses were normalized to the gene for 18S as endogenous control (Ref. Seq. ×03205.1; Applied Biosystems). Amplification efficiency for housekeeping primer (18S) was tested using serial dilutions with standard curve analysis (data not shown). Analysis of gene expression in the treated versus the control side using Ct values calculation carried out by ΔCt and ΔΔCt method. 16 After performing PCR, the relative expression was determined using the ΔΔCt method to calculate results, expressed as “fold regulation” of genes. 17
Immunohistochemistry
The soft tissue samples adjacent to the outer surface of the mesh from three dogs in Gp1 were examined for BMP2 and VEGF in paraffin-embedded sections. Sectioning and staining was performed in 4 μm serial sections of fixed tissues. The primary antibodies used were mouse antihuman BMP2 (catalog# sc-57040; Santa Cruz Biotechnology, Inc.) and goat anticanine VEGF (catalog# AF1603; R&D Systems). Random three samples of each group were examined using bright field light microscope. Digital images of one section of each sample were taken at 20× magnification. Quantification of immunostaining was done by a blind operator using the imaging analysis software program Bioquant NOVA PRIME version 6 (R&M Biometrics).
BMP2 and microvascular EC immunoco-localization
Frozen sections (10 μm) from the soft tissue bed surrounding the defect were prepared for immunoco-localization of both anti BMP2 antibody (catalog# sc-57040; Santa Cruz Biotechnology, Inc.) and BODIPY® FL anti acetylated low density lipoprotein (AcLDL) antibody (catalog# L3485; Invitrogen) (microvascular EC marker). Sections were fixed with 5% paraformaldehyde for 5 min, followed by washing with PBS and blocking with 5% normal mouse serum for 30 min. Slides were incubated with BMP2 antibody (catalog# sc-57040; Santa Cruz Biotechnology, Inc.) and the BODIPY FL AcLDL (catalog# L3485; Invitrogen) for 2 h at room temperature followed by Texas Red® goat anti-mouse IgG secondary antibody (catalog# T862; Invitrogen). Immunostained slides were covered and examined by confocal microscopy (LSM 510; Carl Zeiss).
Statistical analysis
Data were expressed as the mean±standard deviation. Significance level was set at p<0.05. Concerning the physical dimensions, the percentiles of bony dimensions within different zones of the regenerates were compared using one-way ANOVA test (Tukey-Kramer multiple-comparison test). The same test was used to assess the immunostaining and the 3D morphometric parameter differences between various zones (anterior, middle, and posterior) within the regenerates of the same group and the mean of these three zones were compared between the three groups. Comparisons between the regenerate and contralateral bone were made using paired Student's t-test. The BMD of Gp1 and Gp2 was compared with each other using a Student's t-test and each of these groups was compared with its normal side using a paired t-test. Concerning the real-time quantitative PCR results, the results expressed as fold regulation for each group were tested using a paired Student's t-test between the ΔCt of the treated side and the control side within each group individually. All statistical analyses were done using NCSS©2007 (NCSS, Inc.).
Results
All animals tolerated the surgery and postoperative period well. In one animal, the defect span was accidentally larger (∼40 mm) and, thus, was excluded from the study.
Gross examination and physical dimensions of regenerate
In Gp1, bone regenerate had an outline comparable to that of the neighboring bone. It was noticeable that bone formation followed the outline of the mesh in Gp1. In Gp2, however, the formed bone tended to taper centrally (hourglass appearance) in four of the five dogs. This was confirmed radiographically (Fig. 2). In Gp3, it was obvious that the gap created healed only by fibrous tissue that also had a tendency to have the least dimensions within the center of the defect (Fig. 2L–P).
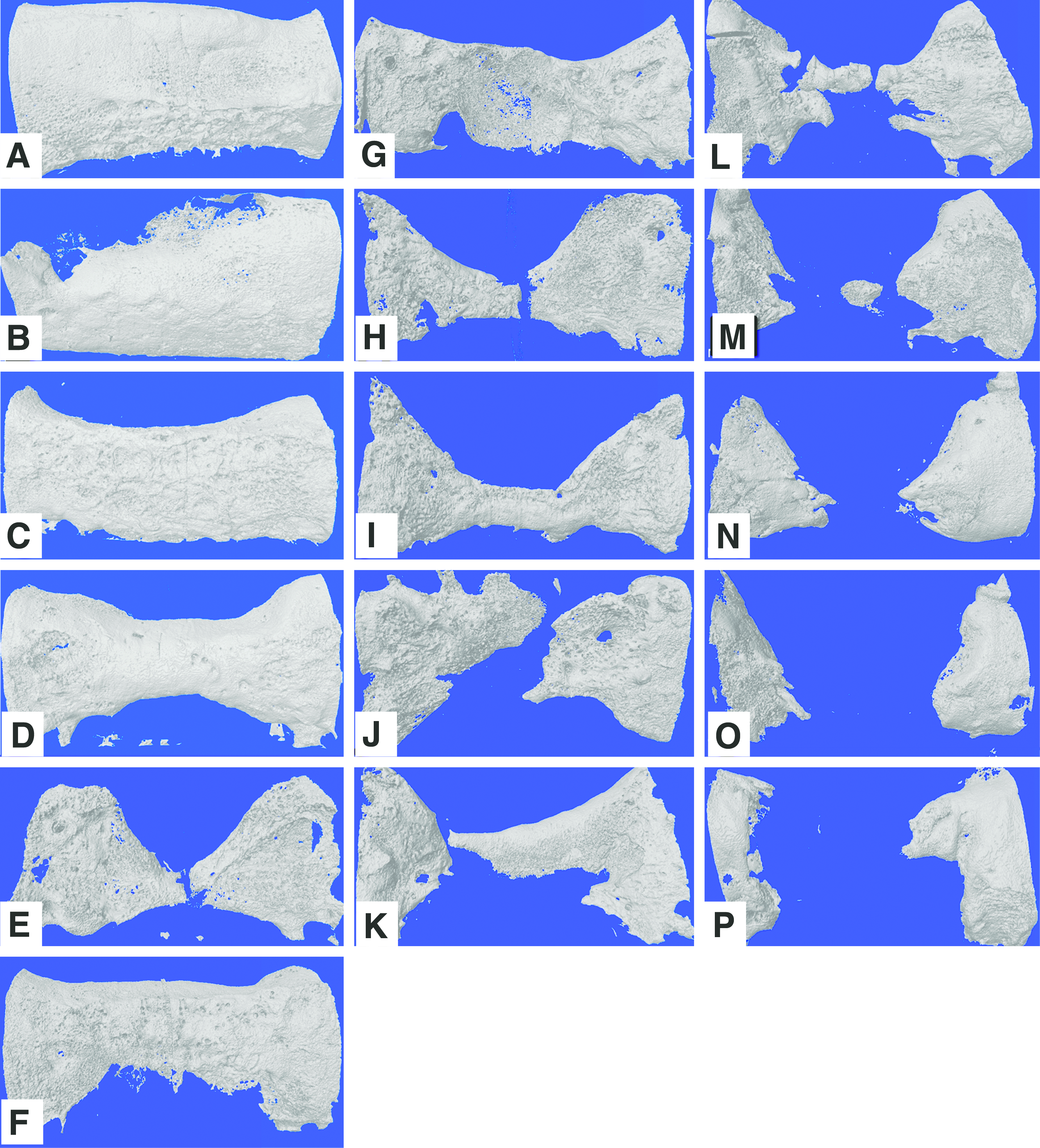
Three-dimensional micro-CT reconstructed images showing the ability of the formed regenerates to bridge the defect gaps. Any bony discontinuity is considered a failure.
Concerning physical dimension, Gp1 showed more superior regenerates in comparison with both groups. It showed significant difference between Gp1 and the other two groups in many of the measured dimensions shown in Figure 3A–L. The means±SD of all % physical dimensions of the three groups are shown in Table 1. Successful bridging of the defect gap was seen in five of the six dogs in Gp1 (Fig. 2A–F), only two of the five dogs of Gp2 (Fig. 2G–K), and none of Gp3 dogs (Fig. 2L–P).
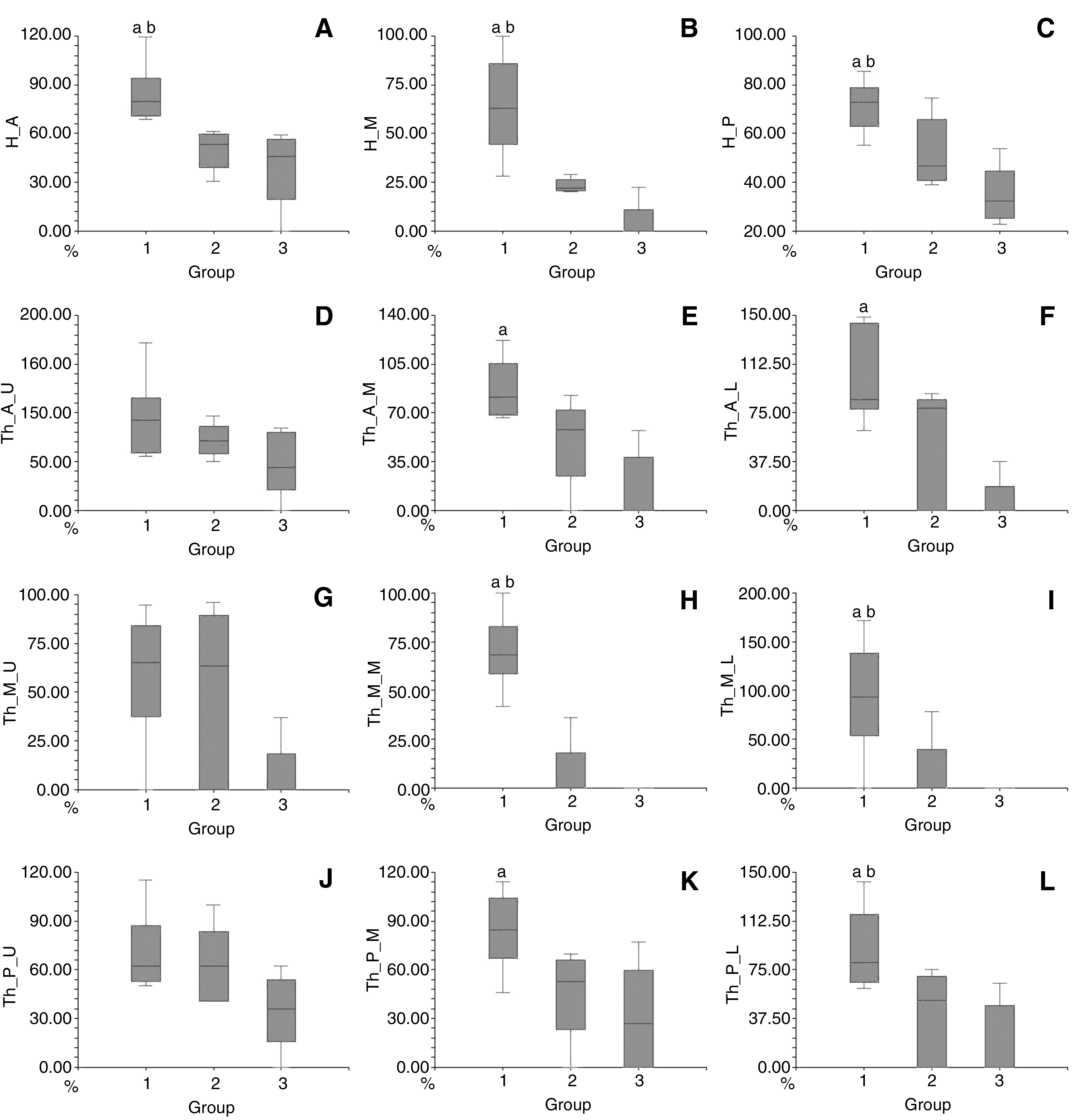
Box plots representing % of physical dimensions of resected bony segments in relation to the control normal bone. Gp1: immediate reconstruction group, Gp2: delayed reconstruction group, and Gp3: control group. H: height, Th: thickness, A: anterior, M: middle, P: posterior, Up: upper, I: inferior. (ap<0.05 between Gp1 and Gp3; bp<0.05 between Gp1 and Gp2). Gp1 showed more superior physical dimensions in comparison with both groups. It showed significant difference between Gp1 and Gp3 in the H_A
In order to evaluate the success of recombinant human bone morphogenetic protein 2 on absorbable collagen sponge treatment in restoring the physical dimensions, we used the percent of the formed bone within the regenerate in relation to the normal resected piece of bone within each dog. The total mean of all measurements made in Gp1 was 80.9%±13%, which is almost the double of that of Gp2 [40.6%±16%] and four times more than Gp3 [20.1±17].
Gp, group; H, high; Th, thickness; A, anterior; M, middle; P, posterior; U, upper; L, lower.
Micro-CT analysis
Micro-CT analysis of 3D bone morphometric analysis showed no significant difference between Gp1 regenerate and contralateral control bone in quantitative and qualitative parameters except for BMD (p=0.02) (Table 2). Meanwhile, all morphometric parameters of Gp2 lagged behind normal bone (Tb.Th, p=0.03; TV/BV, Tb.N, and Tb.Sp, p<0.01; BMD, p<0.001) except for DA (Table 2). When the regenerates of the three groups were compared, Gp1 regenerates parameters surpassed Gp2 and Gp3 in BV/TV, Tb.N, and Tb.Sp (Fig. 4). To validate the intergroup differences, we also compared the normal contralateral bone of the three groups (data not shown) and they showed no statistical significant differences concerning all 3D morphometric parameters and BMD.
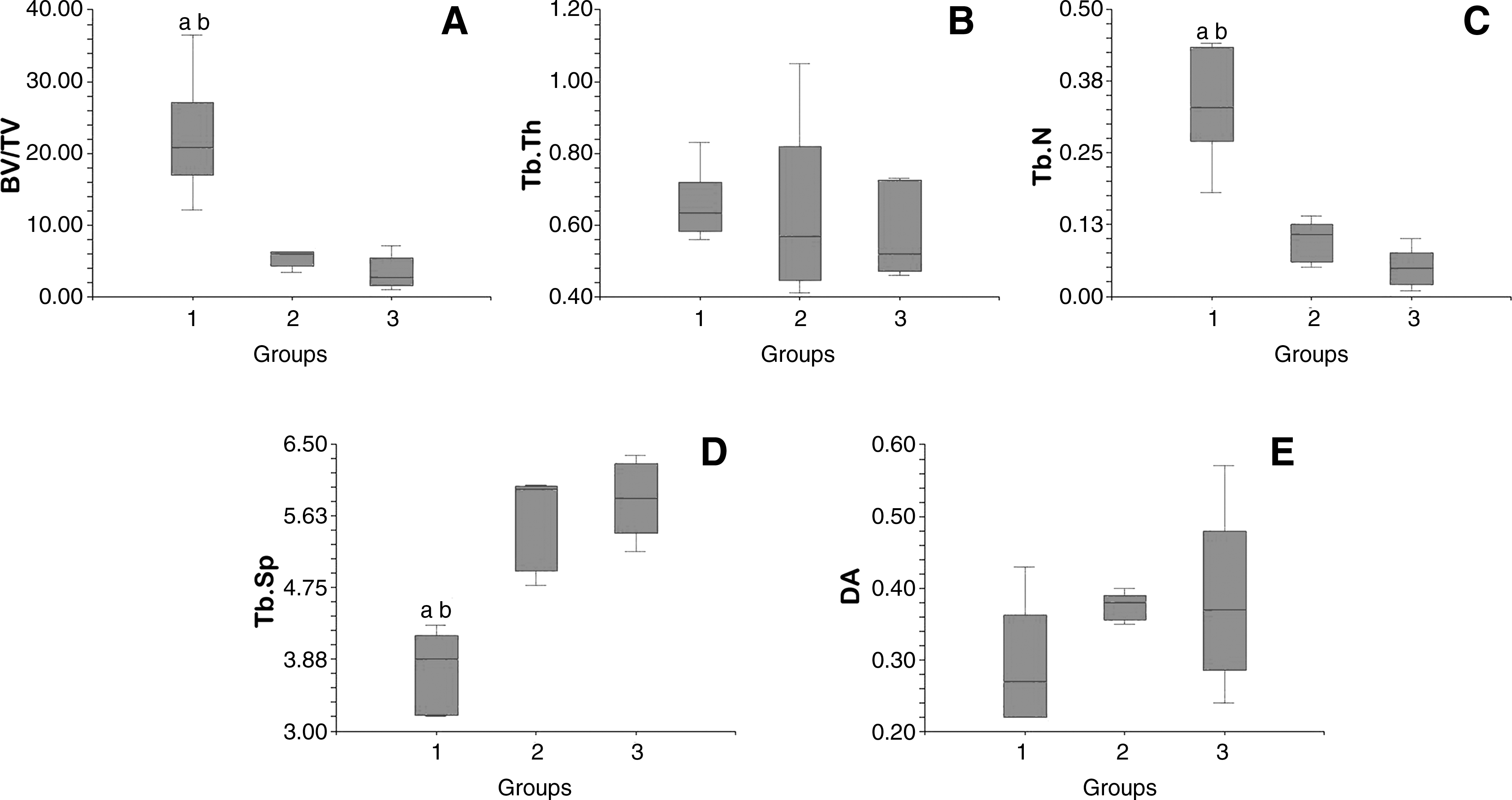
Box plots representing 3D bone morphometric analysis using micro-CT. Gp1: immediate reconstruction group, Gp2: delayed reconstruction group, and Gp3: control group.
No significant difference between Gp1 regenerate and contralateral control normal bone in quantitative and qualitative parameters except for BMD. All morphometric parameters of Gp2 and Gp3 lagged behind normal bone.
BV/TV, percent bone volume; Tb.Th, trabecular thickness; Tb.N, trabecular number/mm; Tb.Sp, trabecular separation; DA, degree of anisotropy; BMD, bone mineral density; Cnt, control.
mRNA expression using real-time quantitative PCR of BMP2 and VEGF
In the soft tissue bed of the defect, the mRNA expression of BMP2 was upregulated in Gp1 (mean=+7.3-fold change, p value=0.001), nonsignificantly downregulated in Gp2 (mean fold difference=−1.2, p value=0.91), and not changed in Gp3 (mean fold difference=−0.27, p value=0.74). Concerning the VEGF it was significantly upregulated in Gp1 (mean fold change=+1.53, p value=0.001), nonsignificantly downregulated in Gp2, and no fold change in Gp3 (mean fold change=−1.3, p value=0.6; mean fold change=−0.96, p value=0.09, respectively) (Fig. 5).
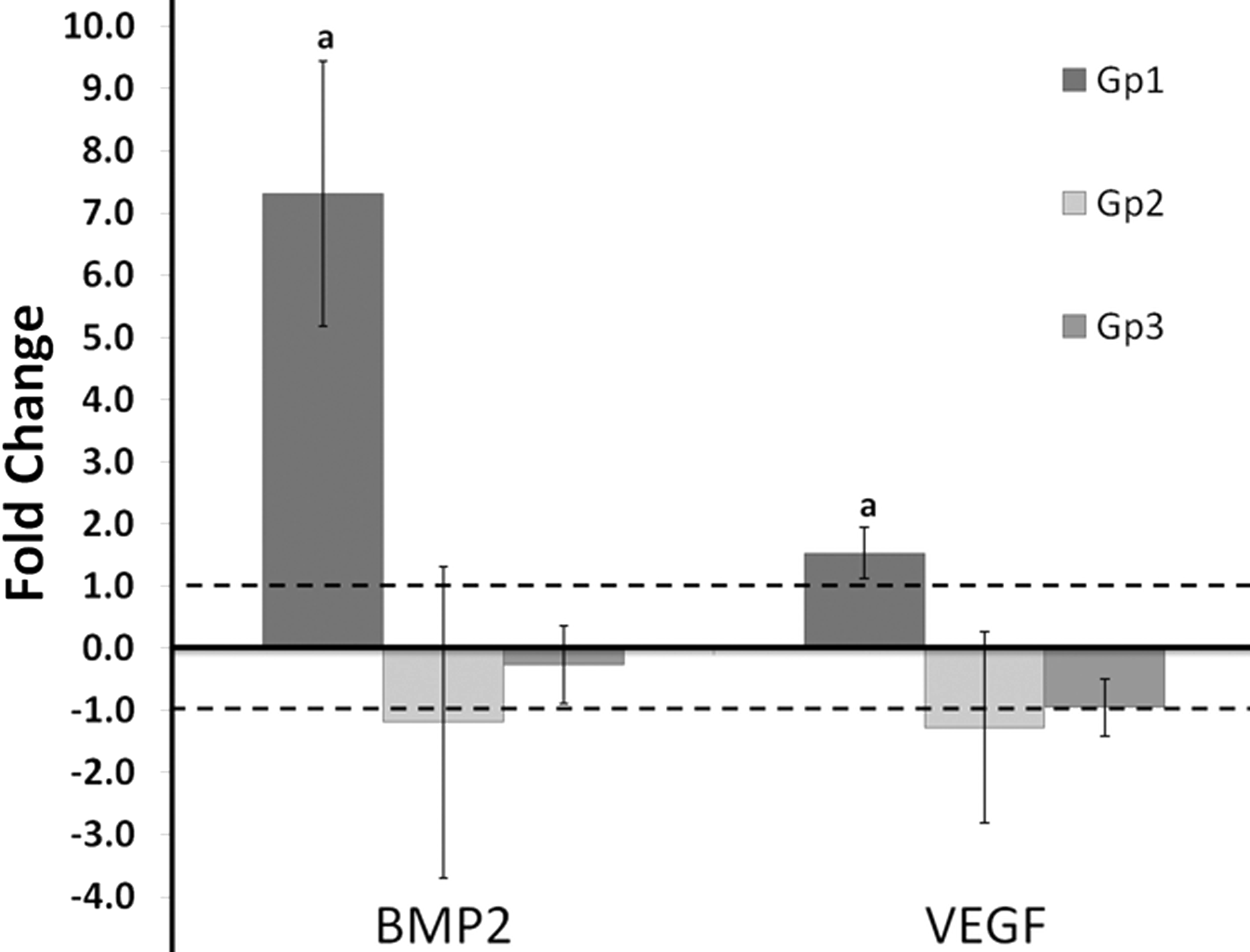
Bar graph showing mRNA expression of BMP2 and VEGF in all groups. The area between the dotted lines represents no fold change (−1 to +1). The “a” indicates significant difference between Gp1 and both other groups. Gp1: BMP2 mean=+7.3-fold change and p value=0.001; VEGF mean fold change=+1.53 and p value=0.001. Gp2: BMP2 mean fold difference=−1.2 and p value=0.91; VEGF mean fold change=−1.3 and p value=0.6. Gp3: BMP2 mean fold difference=−0.27 and p value=0.74; VEGF mean fold change=−0.96 and p value=0.09. VEGF, vascular endothelial growth factor.
Immunohistochemistry of BMP2 and VEGF
The BMP2 staining was detected in higher concentrations in Gp1 (mean=423, p value<0.0001) than in Gp2 and Gp3 (mean=112 and 61, respectively) (Fig. 6). Quantification of BMP2 immunostaining signal is shown in Figure 6F. A consistent colocalization of BMP2 and ECs of blood vessels within Gp1 was also observed (Fig. 6B, C) throughout the sections examined. VEGF was undetected in all samples of all groups.

Immunohistochemistry against BMP2 in soft tissue samples enveloping the regenerates of all groups.
BMP2 and microvascular EC immunoco-localization
BMP2 was detected in higher concentrations related to blood vessels, with obvious colocalization of both BMP2 and AcLDL throughout the sections examined (Fig. 7).
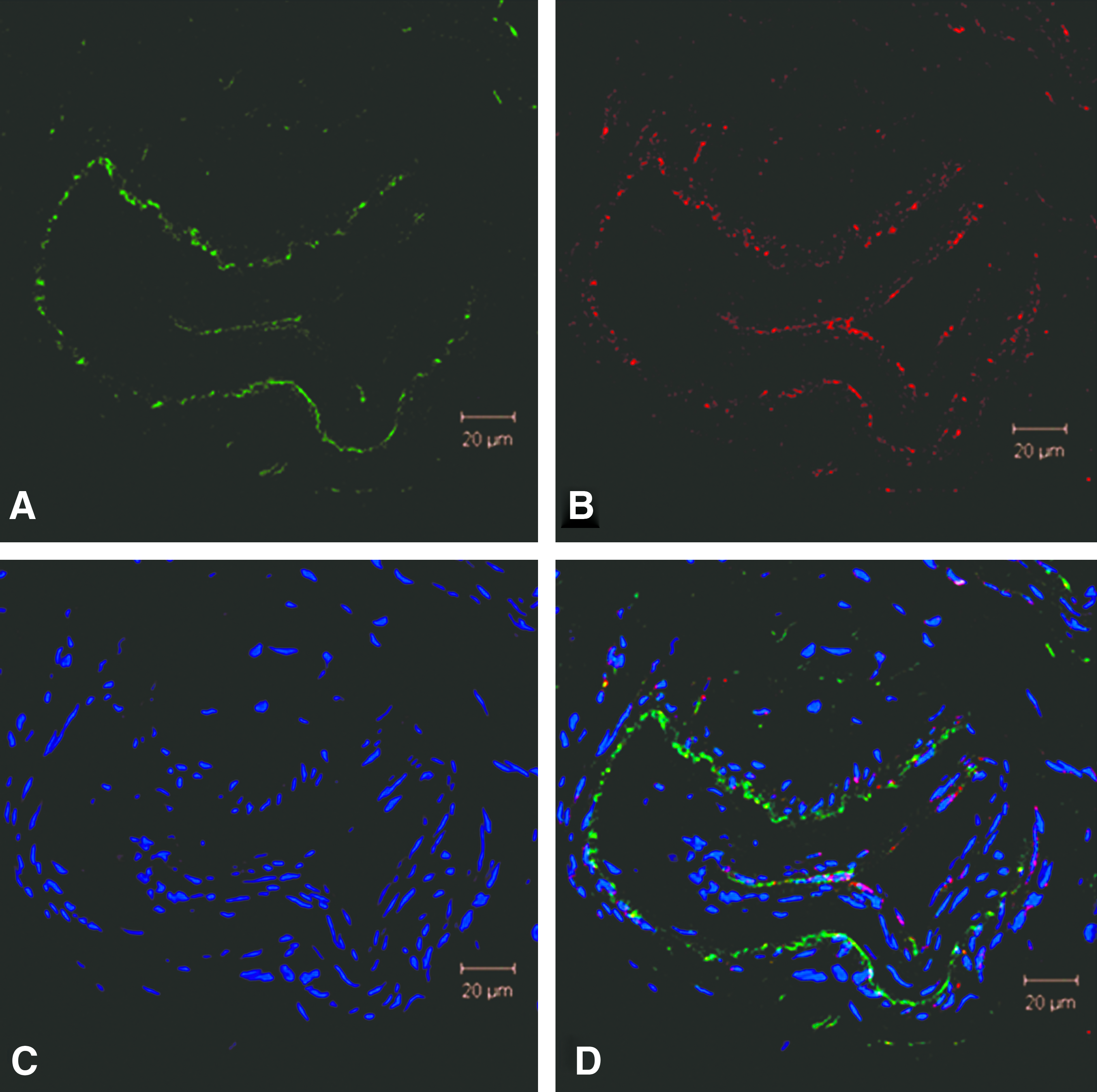
Immunofluorescence showing colocalization of AcLDL (endothelial cell marker) and BMP2.
Discussion
This study demonstrated that rhBMP2 delivery is more effective in immediate than delayed reconstruction of large mandibular segmental defects. Although new bone formation was evident in both the immediate and delayed delivery groups, immediate delivery of rhBMP2 yielded more complete reconstruction of the defect after 12 weeks, evident by the quantity and quality of the bone regenerate. The advantageous parameters recorded in Gp1 were associated with significant upregulation of BMP2 and VEGF mRNA expression that was not detected in the other two groups. However, on the protein level, BMP2 was higher in Gp1 while VEGF was undetected in all groups. This suggests that endogenous, soft tissue–based, osteoinductive mechanisms may be important in maintaining the short-acting effect of the delivered rhBMP2. This novel mechanism is therefore expected to play critical role in determining the outcome of the reconstruction of large segmental defect, in which active bone regeneration needs to be sustained for several months. In this study, endogenous soft tissue osteoinductive mechanism was triggered only when rhBMP2 was delivered immediately after defect creation. In contrast, delayed rhBMP2 delivery did not produce similar soft tissue response and was also associated with less robust bone regeneration within the defect. Protein colocalization suggested that ECs could be the source for this endogenous BMP2 secretion in response to rhBMP2 treatment.
Very often, delayed reconstruction becomes the setting of choice in the reconstruction of large segmental defects in the mandible in human patients. During the primary surgery, when the defect is surgically created, intraoperative communication between the oral cavity and the skin is often present, raising the incidence of failure and complications if a nonvascularized construct is used for immediate bone reconstruction.5,6 According to van Gemret and colleagues, 5 immediate use of nonvascularized bone grafting should be limited to cases where only an extraoral approach is used to avoid intraoral wound contamination with oral microorganisms. Other factors may necessitate the delay of definitive bone reconstruction, including planned radiotherapy and soft tissue restrictions.6,7 Delayed mandibular reconstruction is also recommended in management of bisphosphonate-induced osteonecrosis of the jaws. 8 For many of the same reasons, delaying the reconstruction may provide more appropriate conditions for the use of rhBMP2/ACS constructs in the human mandible. However, efficacy of rhBMP2 in delayed reconstruction of mandibular segmental defects has not been experimentally tested before.
The canine model is ideal for studying regeneration of mandibular segmental defects. Based on our own experience with this model and supported by previous studies, a 35-mm segmental mandibular defect with excision of overlying periosteum will not heal spontaneously in dogs.18–20 The untreated control group in this study was necessary to confirm that under the same conditions and fixation methods of the experimental animals, the unloaded ACS would not cause significant regeneration within the defect. The control animals were also necessary to verify control gene expression around the defect.
Many investigators used rhBMP2 in canine models since interspecies homology is almost 100% in mammalian species sequenced so far.21–23 In 1991, Toriumi and coworkers 24 performed immediate reconstruction of 30-mm canine mandibular defect using 0.25 mg rhBMP2 added to 500 mg inactive dog bone matrix and 5 mM/L aminocaproic acid. The study reported very promising results and was followed by a series of studies testing different concentrations of rhBMP2 in canine and nonhuman primate models.20,25–27
In contrast to the very promising experimental results, clinical results of rhBMP2/ACS have been variable. 28 Inability of rhBMP2 to regenerate bone in mandibular defects has been reported by Carter and coworkers. 3 Five cases treated with rhBMP2 were presented in their study where two patients required secondary bone graft procedures. Both cases were nonunion cases; thus, could be considered delayed reconstruction situations. In other studies, BMP2 did not improve bone healing in treatment of nonunion fractures.29,30 One possible reason for the impaired effect in delayed reconstruction is the diminished responding cell population at the nonunion sites compared with acute fractures. 11
Periosteum plays a key role in bone growth and repair as a reservoir of mesenchymal and osteogenic progenitor cells. In addition, the alkaline phosphatase activity in periosteum precedes that in fracture site. In absence of periosteum, the adjacent soft tissues including muscles, fascia, and blood vessels are expected to be the major osteogenic cell sources in case of bone repair.31,32 In our study we analyzed mRNA expression of both BMP2 and VEGF within the soft tissue bed of the defect compared with the normal periosteum of the contralateral side within the same animal. The delivered rhBMP2 has a much shorter effective time, at the site of delivery, than the time needed to regenerate a large defect. 1 Endogenous release of BMP2 detected 12 weeks after delivery of rhBMP2 suggests that endogenous BMP2 may play a role in sustaining the effect of the delivered rhBMP2. However, the upregulation of BMP2 mRNA was only seen in the immediate reconstruction group (Fig. 5). This was confirmed on the protein level where Gp1 immunostaining of BMP2 was significantly higher than Gp2 (Fig. 6E). This may be due absence of the responsive cell population due to subsidence of the bony surgical hematoma.
ECs are a known source of BMP2 in response to hypoxia and VEGF. 33 The in vitro coculture of ECs and osteoprogenitor cells increases the differentiation and bone matrix formation by osteoblasts. 34 Our results show consistent colocalization of BMP2 and ECs in blood vessels within the soft tissue bed of the defect as seen in the Gp1 (Fig. 6B, C). This was further confirmed using immunofluorescent colocalization of BMP2 and AcLDL (Fig. 7). These results are in concordance with the findings of Colnot et al., 35 which confirmed that vascular invasion and ossification are linked in both time and space. The study also suggested that a direct cell-to-cell contact between EC and osteoblast precursors could be essential for osteoblast differentiation. Our results show that ECs could be one of the main responders to rhBMP2 treatment by secreting endogenous BMP2 (positive feedback loop), inducing the differentiation of osteoblasts. Meanwhile, rhBMP2 application in a delayed setting (Gp2) was insufficient to induce this positive feedback loop, possibly due to the absence of the angiogenic effect of the fracture hematoma, which may explain the impaired bone regeneration in this group. The positive feedback in response to BMP2 treatment has been also proven in adipose-derived stromal cells. 36
The fracture hematoma is known to have a potent angiogenic activity, mainly due to VEGF, and removal of this hematoma significantly compromises bone repair.37,38 BMP2 is known for its potent angiogenic effect mediated via VEGF-A. 39 Although VEGF is one of the main mediators of angiogenesis during BMP2-induced bone formation in addition to its synergistic interaction with BMP2 enhancing mineralized bone formation, 38 only Gp1 VEGF mRNA was upregulated in the 12th postoperative week after rhBMP2 delivery. However, the VEGF protein was undetected in all groups. We expect that the BMP2/VEGF relation could have been detected at an earlier time point as VEGF is normally upregulated in early stages of bone repair. 10
The height and thickness of regenerated bone are of immediate relevance to functional rehabilitation of the mandible using osseointegrated dental implants. The average dimensions were around 81%, 41%, and 20% of the excised normal bone segment in Gp1, Gp2, and Gp3, respectively. In Gp1, thickness exceeded 90% of the normal in several zones. Therefore, ridge dimensions in Gp1 animals were optimal for dental implant placement. On the other hand, none of Gp2 regenerates could allow restoration of function using dental implants at the examined time point, mainly due to insufficient bone dimensions in different zones of the formed regenerates. The untreated control defects showed either deficient or absent bone regeneration, especially within the center of the defect.
The micro-CT results show that bone quality and quantity were very similar to the control bone in Gp1, with the exception of BMD. We can expect that as bone remodeling continues, BMD would continue to increase as well, given an optimal loading environment.40,41 On the other hand, delaying the rhBMP2 delivery seemed to negatively affect all qualitative and quantitative parameters of the regenerate.
More experimental studies are underway to explore the cellular and molecular mechanisms that regulate endogenous BMP2 release and function in acute versus delayed defect reconstruction and to determine ways to optimize its osteoinductive effect of rhBMP2 during delayed delivery.
Conclusion
In large segmental bone and periosteum defect in the mandible, delaying the rhBMP2 delivery for 1 month after the creation of the defect negatively affects its efficacy. While immediate delivery of rhBMP2 stimulated endogenous BMP2 expression, delayed delivery failed to elicit such response, a difference that may explain the relative deficiency of bone regeneration in the delayed setting. Finally, ECs are potential source of this BMP2 release mechanism in addition to their earlier role in angiogenesis. More studies are underway to examine the mechanism of endogenous rhBMP2-induced BMP2 and VEGF expression and how to optimize the soft tissue response to rhBMP2 delivery.
Footnotes
Acknowledgments
This study was supported by Medtronic, Inc., the Egyptian Ministry of Higher Education, and a faculty start-up fund from the Georgia Health Science University. The authors affirm that the sponsor did not take part in the execution of the outlined experiments, collection or analysis of the data, making the decision to publish, or editing the published data in anyway.
Disclosure Statement
No competing financial interests exist.