
Abstract
Objectives:
We investigated the potential of different scaffolds for in vivo construction of bladder muscular and urothelial wall. Bladder wall was used as a bioreactor to create a model of the natural environment for cellular interactions, growth, and differentiation.
Methods:
Forty rabbits were divided into 10 groups. Different scaffolds were implanted between bladder mucosa and seromuscular layer. Scaffolds used in each group were one layer or a three-layered combination of tissue-engineered pericardium (TEP), biofilm, and polyglycolic acid (PGA). In all groups, a biopsy of full thickness of bladder was dissected. Muscular and urothelial layers were separated and minced into small fragments. Fragments were seeded above the urothelial layer and urothelial fragments were placed on the scaffold under the seromuscular layer. One group served as control and no scaffold was inserted between the separated bladder layers. After 2 and 6 weeks, biopsies were performed for histologic examinations (trichrome, smooth muscle α-actin, and pancytokeratin AE1/AE3, CD34, CD31).
Results:
Histopathological examinations showed granulomatous reaction and severe inflammation in biofilm-containing groups. Samples with TEP alone and with PGA-coated TEP as scaffolds revealed more organized bladder wall in two different layers with mature urothelial and smooth muscle cells. The number of CD34+ cells and CD31+ microvessels increased continuously during 6 weeks.
Conclusions:
Our results demonstrated the effective role of PGA-coated TEP as a potential scaffold for muscular and urothelial fragment seeding in bladder wall acting as a natural bioreactor. Biodegradable scaffolds could be helpful in association with acellular matrices to optimize the cell attachment and in vivo bladder wall construction.
Introduction
An appropriate biocompatibility and mechanical strength—the potential to induce cell attachment and proliferation and to provide designable three-dimensional structures—are the principals of an ideal scaffold. 3 Previous studies demonstrated that synthetic, naturally derived, and biodegradable scaffolds might induce regeneration of native bladder components into a functional urinary reservoir.4–6 Regarding these results, we decided to choose one scaffold from each type. The cell-seeded polyglycolic acid (PGA) polymer was chosen as a biodegradable scaffold because it has been shown to facilitate smooth muscle cell regeneration. 3 Among different types of naturally derived collagen matrices, tissue-engineered pericardium (TEP) was used as an appropriate natural scaffold approved in our previously reported results. 2 Biofilm derived from parafilm was selected as the synthetic scaffold because of its optimal flexibility, mechanical strength, good biocompatibility, and low density.
Since the ex vivo construction of urinary bladder wall using hybrid scaffolds from combined PLGA and collagen sponge or gel was successful in previous studies, 7 we designed our study based on the application of hybrid scaffolds and different possible combinations of PGA, biofilm, and TEP. The aim of this study was to establish a new method in preparing graftable bladder layers using a suitable temporary scaffold. We compared various arrangements of TEP, biofilm, and PGA combinations as hybrid scaffolds seeded by urothelial and muscular fragments. The bladder wall was used as a natural bioreactor, preserving the host bladder urothelium and muscular layers around the scaffold as feeder, preservative, and complementary layer and to obtain the two in vivo constructed layers of bladder wall.
Materials and Methods
Animals
The animal research committee of our university approved this project. Forty male New Zealand white rabbits with body weight of about 3 kg were divided into 10 groups. In the control group (G0), muscle and urothelial fragments were seeded on the separated urothelial layers and muscular layers of the bladder, respectively, without insertion of scaffold. Other groups (G1–G9) underwent bladder augmentation and insertion of different fragment-seeded scaffolds between bladder mucosa and seromuscular layers.
Scaffolds used in each group were as follows: G1, TEP; G2, biofilm; G3, PGA; G4, biofilm-coated TEP; G5, PGA-coated TEP; G6, TEP-coated biofilm; G7, PGA-coated biofilm; G8, TEP-coated PGA; and G9, Biofilm-coated PGA.
Scaffolds
Preparation of tissue-engineered pericardium (TEP)
Fresh rabbit pericardium was flushed by normal saline and was then cut longitudinally into 2 cm×2 cm pieces. Preparation of acellular pericardial matrix was done according to the method of Courtman et al., with slight modifications. 8 Briefly, pericardium pieces were washed with 2% sodium dodecyl sulfate (SDS) for 24 h at 4°C and Ethylenediaminetetraacetic acid (EDTA) (0.01 %) was added for 4 h at 4°C. The tissue was rinsed for 48 h with Hank's balanced salt solution (HBSS). Acellular tissues were reserved in phosphate buffered saline (PBS) containing a cocktail of antibiotics (penicillin and streptomycin) and amphotericin at 4°C. The acellular pericardial matrix was preserved no longer than 1 week. It was washed with distilled water and PBS before any case of use to remove any anti-fungal or anti-bacterial components.
The tissue-engineered pieces were prepared for histopathological staining including hematoxylin and eosin (H&E), masson's trichrome, to evaluate the extracellular matrix and orientation of fibers. Staining with 2,4-diamidino-2-phenylindole dihydrochloride n-hydrate (DAPI) (0.5 μg/mL; Sigma, St Louis, MO) was performed to confirm the removal of any nuclide components from TEP.
Biofilm scaffolds
The petrolatum sheets made of hydrocarbon wax were trimmed to 2×2 cm patches. This material is not cytotoxic to our knowledge and does not react to air, water, or other common materials. It only has incompatibility with chlorine, fuming nitric acid, and strong oxidizing agents. It is impermeable to water but permeable to oxygen and carbon dioxide. 9
PGA scaffolds
The PGA scaffolds were formed from unwoven sheets of PGA polymers (Smith and Nephew, Heslington, York, United Kingdom), and trimmed to 2×2 cm patches. Scaffolds were designed to degrade via hydrolysis during a 4-week period. They were coated with a liquefied copolymer poly-lactic-glycolic acid (PLGA) (Sigma Chemical Co, St Louis, Mo). The patches were packed and sterilized with ethylene oxide and stored in a desiccator until application.
Surgical technique
All rabbits received preoperative cefazolin (25 mg/kg intravenous) and were sedated with an intramuscular injection of 30 mg/kg ketamine and 6 mg/kg xylazine. The bladder was catheterized with a 6-Fr Foley catheter. Then it was exposed through a lower midline laparotomy incision and was washed and filled with normal saline followed by measurement of bladder volume.
A 1×0.5 cm biopsy of full bladder thickness was dissected at an appropriate site of the bladder where no major visible vessels were seen. The muscular and urothelial layers of the biopsy were separated under a dissecting microscope in Dulbeccos Modified Eagle Medium (Sigma, MO) supplemented with 10% fetal bovine serum (Gibco, NY). The two separated layers were minced into 20 fragments to be seeded on the scaffolds.
In the opposite side of the bladder at an appropriate site of the bladder with no major superficial vessels, the muscular layer was dissected from the urothelial layer. The prepared muscle fragments were seeded on the mucosal layer. Then the 2×2 cm scaffold or the three-layered scaffold covered the fragments. The urothelial fragments were placed on the surface of the scaffold afterward, and the seromuscular layer covered the surface of minced urothelial tissues. Fragments were seeded at a concentration of 10 tissue fragments per cm2 on each side. The inserted tissue-coated scaffold was fixed over the bladder and the edges were marked with 6/0 non-absorbable monofilament sutures (Figs. 1 and 2). The perivesical fat layer was fixed over the bladder graft to make the potential vascularization support. 2 Rabbits were treated with a combination of analgesic agents and antibiotics (ceftriaxone, 30 mg) for 5 days postoperatively. They were being monitored for any signs or symptoms every day, until resuming a normal diet.

Schematic model of scaffold-implanted bladder wall between urothelial cell (UC) and smooth muscle cell (SMC) host bladder layers. The scaffolds are seeded interiorly by SMC and exteriorly by UC tissue fragments.
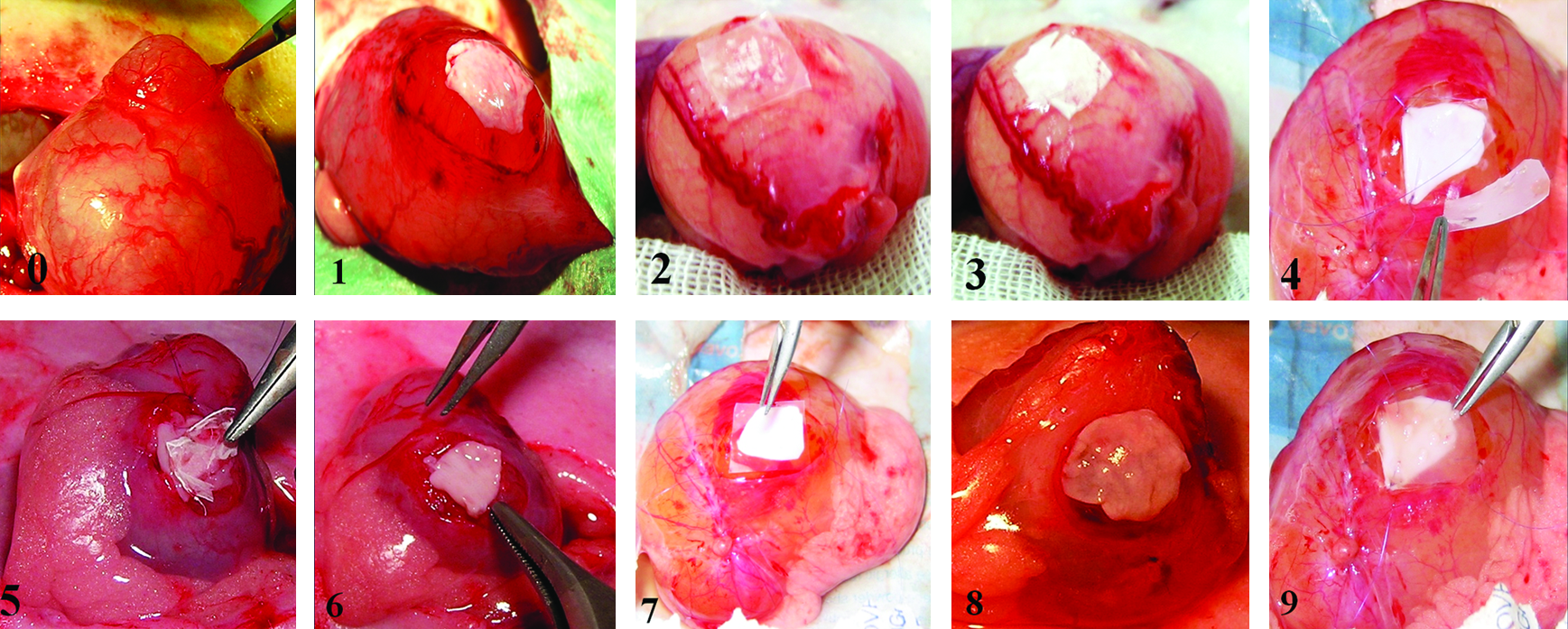
Scaffold preparation, surgical, and bioengineering methods in different groups.
Histology and Immunohistochemistry
Two and six weeks after surgery, all animals were sedated and a 1×1 cm, full thickness biopsy was dissected from a corner of implanted scaffold after obtaining bladder volume. The biopsy included a 0.5×0.5 cm full thickness sample of host bladder, to be used as the standard tissue. Samples were divided into two pieces; one piece was fixed in formalin, embedded in paraffin. Sections of 5 μm were cut and stained with hematoxylin and eosin and masson's trichrome in order to evaluate the formed tissue, amount of inflammatory cells, and fibrosis in grafts. The other piece of each sample was prepared for immunohistochemistry (IHC). They were immediately fixed in ice-cold 0.1 M PBS, ph 7.4, containing 4% paraformaldehyde for 24h, followed for cryoprotection in 15% sucrose for 4h and 30% sucrose overnight at 4°C. The IHC staining methods were employed with several specific primary antibodies in order to characterize urothelial cell (UC) and smooth muscle cell (SMC) differentiation in the retrieved bladder. Mouse-derived monoclonal antibodies to smooth muscle α-actin and pancytokeratin AE1/AE3 were studied. Anti CD31 was used for staining of microvessels and anti CD34 was applied for identification of angioblasts and progenitor hematopoietic stem cells. All antibodies were purchased from Dako (Trappes, France). Image analysis was performed using Photoshop 10.0 software. For cytokeratin AE1/AE3 and expression of α-actin, the ratio of positively stained areas to the full thickness of host bladder areas was calculated by computerized image analysis. For CD31+ and CD34+ staining, numbers of positively stained elements were used for quantization. In each sample, four to five photomicrographs (100×original magnification) were used for scoring, and the mean of score was assigned as the final value for data analysis.
Statistical analysis
Results were expressed as the mean±SEM. The statistical evaluation of data was performed using analysis of variances (ANOVA), followed by Tukey post hoc test; p values <0.05 were considered statistically significant.
Results
None of the rabbits died during the first 48 h after grafting. One rabbit of G2 died after the first biopsy, possibly due to prolonged duration of surgery and effects of anesthesia. Another one from G6 died 3 weeks after surgery because of urine leakage into the peritoneal cavity. The remaining 34 rabbits were included in our evaluation. Intraoperative bladder volume measurement in G1, G3, G5, and G8 revealed no significant changes during follow up in comparison with the initial volume. Bladder ultrasonography was performed on all rabbits before biopsy during week 6. Bladder stones were found in each of two animals of group G2, two animals of G4, and one animal of G7, and G9 represented the incidence of lithogenesis in biofilm-containing groups.
Gross appearance
All groups except the biofilm-containing groups retained a grossly normal bladder appearance on augmentation site and remained stable with no obvious expansion over the original size of the implant. The Biofilm-containing groups had a gross shrinkage of approximately 50% of grafts. However, the sizes of the TEP-containing grafts (G1, G5, and G8) were larger as compared with the PGA-containing ones (G3) (mean 2.46 cm2 vs. 2.05 cm2). All adhesions due to surgical manipulations were easy to detach.
Inflammation
No obvious evidence of inflammation or infection was detected in macroscopic evaluation of the site of operation. Through the microscopic evaluations, biofilm-containing groups (G2, G4, G6, G7, and G9) demonstrated foreign body granulomatous reaction following different grades of acute inflammation. The most severe inflammation was seen in Biofilm-coated scaffolds (G2, G4, and G9) after the second week, and a moderate inflammation was still detectable 6 weeks after surgery. Mild inflammation in other groups was determined by the degree of leukocyte infiltration without congestion and edema after 2 weeks and there was a relatively resolved inflammation after 6 weeks. Figure 3 shows H&E results of different groups.
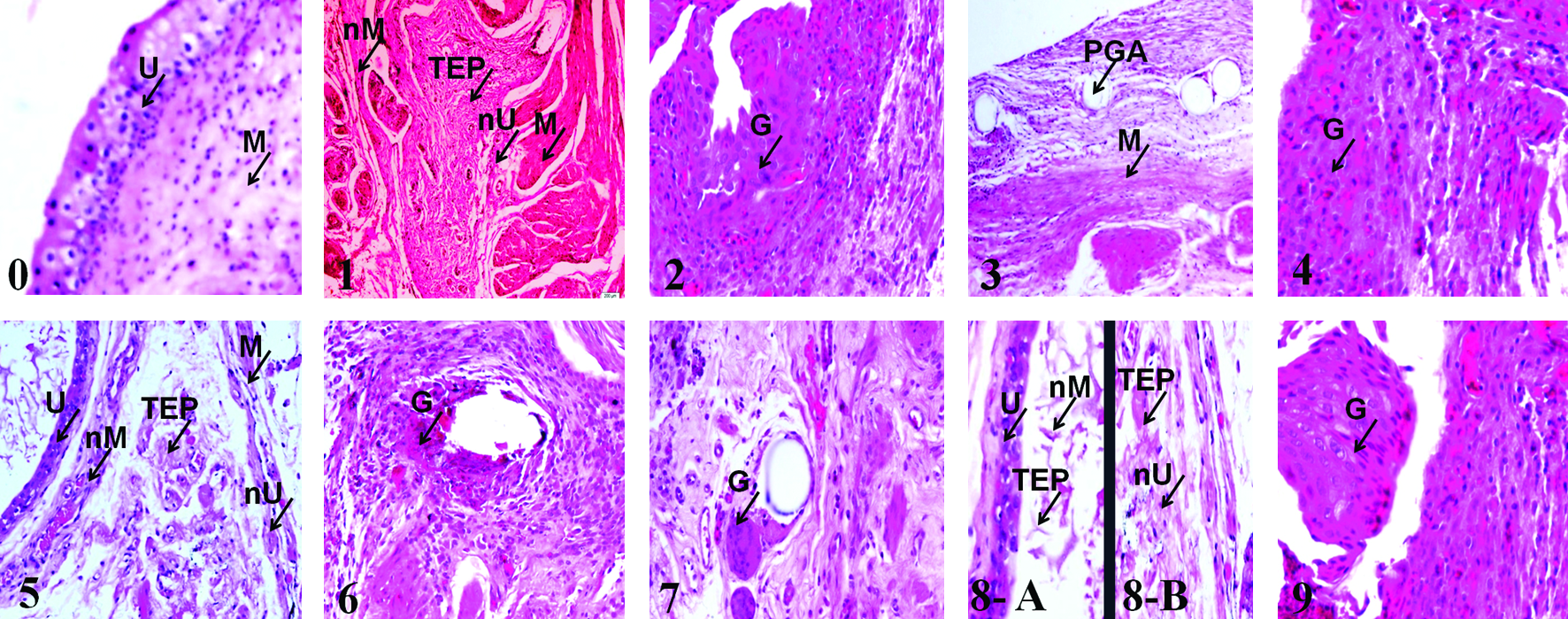
H&E results of different grafts 6 weeks post-implantation (40×).
Smooth muscle and urothelial layer regeneration
Two weeks after the surgery, sections obtained from G1, G3, G5, and G8 resembled fibroblasts, and a small number of spindle-shaped cells were positively stained for α-actin on the interior surface of the scaffold, above the host urothelial layer. However, very few cells were stained for α-actin in G6 and G7 and there were no α-actin stained cells in the biofilm-coated scaffolds (G2, G4, and G9).
The scaffold layer was present in all groups. The exterior surface of scaffolds, under the host bladder muscular layer, in G1, G3, G5, G6, and G8 was 1% to 78% positively stained for urothelial cells. While there were few stained cells as urothelium in biofilm-coated scaffolds (G2, G4, and G9), inside there was severe inflammation and fibrosis reaction in these groups.
Six weeks after implantation, bladder wall grafts in G1 and G5 demonstrated organized bladder wall generation in two different expanded layers with the significantly most mature UCs and SMCs on both surfaces of the scaffold, alongside the host bladder layers in comparison with other groups (p<0.05 in G5). G5 (PGA-coated TEP) contained the most organized layers. (Fig. 4A, B). The expanded layers in G3 were not well organized, especially on the interior surface; regenerated tissue layers demonstrated disoriented muscle fibers. G8 resulted in two separated scaffolds seeded by urothelial and muscular fragments. G2, G4, G6, G7, and G9 did not develop a significant new UC or SMC layer on any surface of the scaffolds, while they showed granulomatous reaction and severe inflammation. The PGA layer was partially degraded in PGA-containing groups after 2 weeks and it was relatively resolved after 6 weeks. However, the degraded particles were still detected in some samples (Fig. 3).
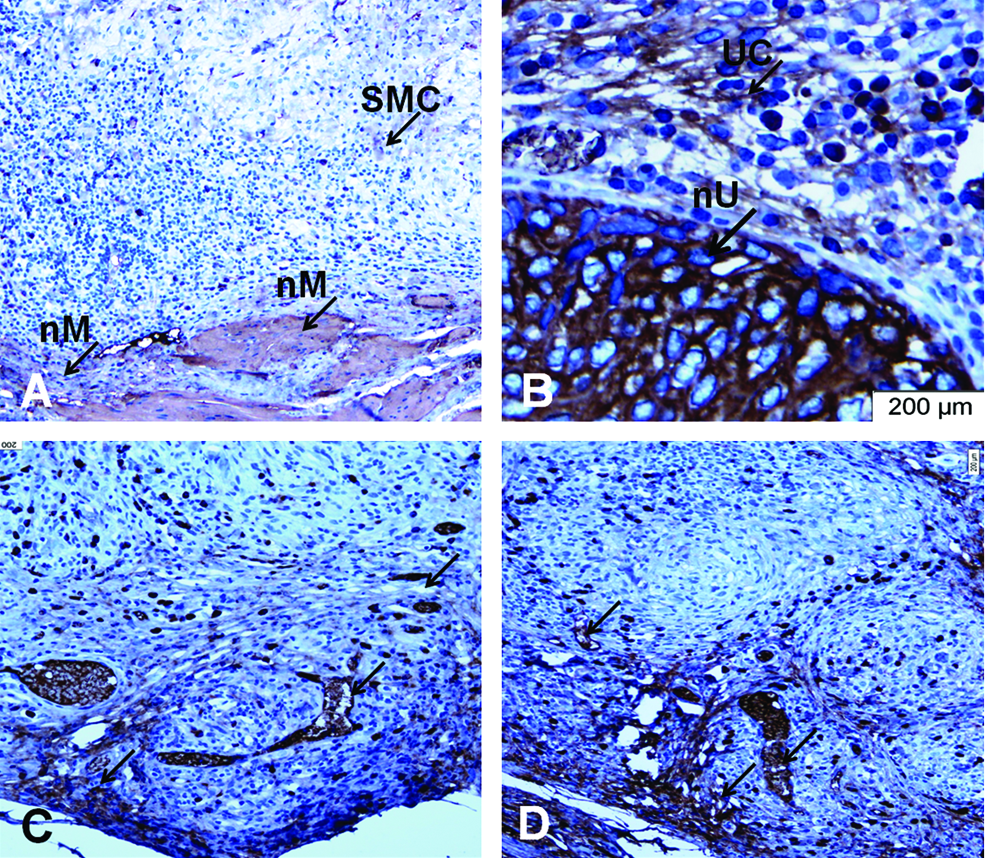
Immunohistochemical results of G5 (PGA-coated TEP) 6 weeks post-implantation.
Computerized analysis of SMC specific α-actin and urothelial cell density was expressed as a percentage of normal host bladder tissue 6 weeks after operation (Table 1).
SMC, smooth muscle cell; UC, urothelial cells.
CD34+ progenitor cells
Numerous CD34+ progenitor cells were found near scaffold borders under host bladder layers after 2 weeks in G1, G5, G6, and G8, most prominently in G5. The number of CD34+ cells on scaffold surfaces increased by about two to three times 6 weeks after implantation compared with results of 2 post-surgical weeks. However, since most of the groups were still devoid of new UC and SMC layers, the average number of CD34+ cells was significantly lower than control values except in G1 and G5 (mean number, 103% of control values 6 weeks after implantation) (p<0.01) (Table 1, Fig. 4C).
Formation of new vessels
CD31+ microvessels were found during the second post-surgical week in almost all grafted matrices, especially in G1, G3, G5, G6, and G8. The number of vascular elements increased continuously until it reached control values in regenerated layers 6 weeks after surgery. At that time, there was pronounced capillary infiltration in the full thickness matrix, which was prominent near the inner surface. However, the mean number of CD31+ cells in G1 and G5 reached 120% of control values 6 weeks after grafting (p<0.01) (Table 1, Fig. 4D).
Discussion
This preliminary study showed the potential of fragment-seeded scaffolds in construction of bladder muscular and urothelial layers. Implementation of autologous tissue fragments serves as one of the main advantages of this method, resulting in diminished inflammatory response and pathologic reactions.
Multiple investigations have reported successful in vitro growth of bladder urothelial cells.10–12 Furthermore, it has been shown that the cell–cell and cell–matrix signaling are integral for appropriate bladder wall development. 13 To achieve these essential interactions, multiple investigations have been performed in developing recombinant models of in vitro bladder construction. Following our previously reported study, using bladder wall as bioreactor for bladder muscular wall regeneration, 2 this study is the one in which the bladder wall is used as an environment for recreation of both autologous muscular and urothelial layers. Using bladder wall as a natural bioreactor provides an appropriate setting for autocrine, paracrine, and endocrine interactions in favor of tissue growth and differentiation, which is unachievable in ex vivo models of tissue culture. Being implanted between the two host layers, the recombinant graft with isolated SMCs and UCs would be protected against the adverse effect of urine exposure. Covering host layers around the scaffold diminishes the risk of urine leakage and provides an appropriate feeding layer for tissue fragments on both sides of scaffolds.
Bladder augmentation, with preserved native urothelium, is currently being used to avoid probable complications of traditional enterocystoplasty. However, no significant increase in bladder capacity and compliance has been shown in many of these methods.12,14,15 Native urothelium has a low turnover rate. However, mucosal defects or denudation rapidly activates the adjacent UCs to migrate, replicate, and re-epithelialize the defects.16,17 Using a small biopsy from the host urothelium for urothelial wall recreation is a new method, suggesting a potential technique for bladder augmentation and the increase of bladder compliance while the native urothelium is being saved concurrently.
This study showed that the recruitment and differentiation of seeded fragments into complete layers with appropriate vascularization was optimal in grafts using hybrid scaffolds of PGA and TEP. Different naturally derived and biodegradable scaffolds have been used in bladder augmentation cystoplasty. 18 However, problems such as lack of efficient epithelialization, inflammation, and thrombogenicity of newly implanted grafts have remained a consideration. 19 Tissue-engineered pericardium is a natural collagen-based scaffold promoting various in vivo regenerating processes. It has been reported to provide a structural support, stability, and biochemical signals for rapid regeneration of bladder muscular layer. 2 Results from pathologic evaluations of TEP-containing groups in this study could prove our previously reported results and would suggest a supportive effect of this natural scaffold.
Grafts containing PGA-coated TEP (biodegradable-coated acellular matrix) demonstrated the best pathologic results with the most organized architecture and restored cellular components 6 weeks after implantation. The PGA itself had been degraded relatively after 6 weeks and the layers were laid and integrated into pericardial matrix. Polymers of PGA have an inherited strength before the degradation of polymer fibers. They offer a reliable mechanical support for organized regeneration of seeded cells.8,19 While observing promising results from groups with PGA-coated TEP, the PGA-coated biofilm groups did not show good pathologic results because of severe inflammatory reactions. These finding revealed that besides PGA support for structural integrity, the inner layer of biofilm does not provide a suitable matrix for cellular growth and tissue regeneration and the role of TEP would be more enhanced. Moreover, microscopic evaluations showed no viable developed SMC or UC layers in most of the biofilm-containing groups. They showed severe inflammation, and fibrosis 2 and 6 weeks post-implantation. Bladder stone formation, scaffold shrinkage, and the only animal death because of urine leakage occurred in these groups. Although this study cannot disqualify the use of synthetic scaffolds, it can provide evidence to show that biofilm (the synthetic scaffold used in this study) has a weak biocompatibility and strength in favor of bladder wall regeneration.
It should be noted that the current study was a preliminary report focusing on histological responses; thus, functional evaluation of the bladder was not evaluated. We used a small graft (2×2 cm) which was not reimplanted into the host bladder, and intraoperative bladder volume measurements confirmed that the grafts did not influence the volumes proposing limited changes in bladder volumes, which seem non-significant using conventional cystometric study systems. According to our promising results in reconstructing a full thickness bladder tissue using TEP and PGA-coated TEP as scaffolds, further investigations with application of large graft size in a partial cystectomy model is required to enable assessing the impact of the grafts on bladder capacity and volume. In this case it is possible to remove the scaffolds and dissect the two newly constructed bladder bi-layers, which can be grafted to the host bladder as autoaugmentation cystoplasty.
Conclusion
This study demonstrates promising results in development of urothelial and muscular layers by implantation of PGA-coated TEP seeded with the autologous UC and SMC fragments between host bladder layers. Host layers provide an appropriate support for tissue fragments to regenerate the layers and to develop the vascularization. The created recombinant layers would be a potential grafts to the host bladder wall through the auto-augmentation cystoplasty.
Footnotes
Disclosure Statement
The authors have no conflicts of interest.