
Abstract
In full-thickness injuries caused by extensive burns or penetrating traumatic injuries, the natural epidermal stem cell niche is destroyed, and wound healing occurs through migration of cells from the wound edges and wound contraction. This can lead to significant contracture formation, especially in large full-thickness injuries, causing lack of mobility and pain. Contraction is reduced when wounds are treated using split-thickness skin grafts (STSG) or dermal substitutes, particularly in combination with cultured autologous keratinocytes, delivered as confluent sheets or sprayed as a single cell suspension (SAK). Here, we show that the application of keratinocytes alone or keratinocytes with fibroblasts, delivered on microcarriers, in combination with STSG or a dermal substitute, significantly reduces contraction of wounds in vivo in a porcine model of wound repair and regeneration. A decrease in alpha-smooth muscle actin–positive myofibroblasts, the cell type responsible for wound contraction, accompanies the reduction in contraction. These findings demonstrate the potential for a significant clinical advantage in the treatment of full-thickness injuries.
Introduction
Skin replacement therapy is used for epithelial closure and reduces contraction during the wound healing process. 13 Split-thickness skin grafts (STSG) are the most appropriate intervention for the closure of large full-thickness wounds. Harvested skin grafts approximately 200 μm thick are passed through a meshing device, which creates perforations and increases the surface area of the skin graft. Epithelial cells from the STSG migrate onto the wound bed, where they facilitate epithelial repair. Because the amount of healthy skin available for grafting in large burns is sometimes a major limitation, alternative therapies have been developed for such cases.
Dermal reconstruction is achieved by the application of dermal templates such as Integra (Integra Bioscience, Hudson, NH). Its collagen matrix becomes vascularized after application to the wound bed, facilitating reconstruction of the dermis. Subsequently an ultra-thin skin graft (150 μm) is applied to the surface of the Integra to reconstruct the epidermis. The quality of epithelial repair achieved using widely meshed STSG may be augmented using cell-based therapies such as cultured autologous keratinocytes (AK) applied in sheet form14,15 or as a sprayed cell suspension,16,17 although each of these treatments presents its own problems. Enzymes used to release the sheet of keratinocytes from tissue culture plastic may damage anchoring proteins and impair dermal–epidermal adhesion, leading to mechanical instability. 18 In vivo observations show that sprayed AK (SAK) fail to adhere to the wound bed, resulting in the loss of considerable numbers of cells during the surgical process. 19 An alternative mode of culture and delivery of keratinocytes is therefore indicated.
Microcarriers (MC) are particles 100 to 400 μm in diameter and composed of a stable matrix that facilitates the attachment and culture of anchorage-dependent cells in suspension culture. First described by van Wezel et al., 20 MC made from a range of materials have been extensively used in tissue engineering research.21,22 Keratinocytes grown on MC have been shown to facilitate re-epithelialization of wounds in vivo in mouse models,23–27 but only one report of the clinical use of keratinocyte–MC culture in wound repair has been published. Liu et al. demonstrated that treating venous leg ulcers using keratinocytes grown and delivered to the wound bed on Cultispher-G gelatin MC (Percell Biolytica, Åstorp, Sweden) resulted in re-epithelialization and reduction in size in a small number of wounds studied. 28
In the present study, we have described the culture of porcine keratinocytes and fibroblasts on microcarriers and used an established porcine model of wound repair to investigate whether keratinocytes alone or keratinocytes with fibroblasts, cultured and delivered to the wound bed on microcarriers, affect wound closure and contraction in vivo when compared with STSG or Integra™ in conjunction with SAK.
Materials and Methods
In vivo experimental procedure
Female large white out-bred pigs (30 - 35 kg) were used under Home Office project licence PPL 80/2215. All procedures were performed under general anaesthesia. Skin grafts (10×10 cm×0.8 mm) were harvested from the back of each animal using an air dermatome (Zimmer, Swindon, UK), and cells were prepared as described below. Photographs were taken at each dressing change for qualitative assessment of wounds. Animals were killed using an injection of a lethal dose of barbiturates. Wounds were excised and divided into four quadrants, along the horizontal and vertical axes, and snap frozen at optimal cutting temperature.
Treatment groups
Experiment 1
The first study investigated whether MC-delivered keratinocytes had a greater rate of survival on the wound bed than sprayed cultured keratinocytes. An early time point of 2 weeks was chosen because green fluorescent protein (GFP) expression in transplanted cells is limited to that duration in vivo. Round full-thickness wounds were created on the flank of each animal (three per side) and 4-cm-diameter polytetrafluoroethylene chambers implanted. The rim of the chambers extended underneath the peripheral wound margins, preventing wound contraction and re-epithelization from the edges.29,30 Wound treatments are shown in Table 1. All wounds were dressed as previously described 19 and the experiment terminated at day 15.
MC, microcarrier; MCAK, MC with autologous keratinocytes; MCK (allo), MC with allogeneic keratinocytes; MCAK/AF, MC with autologous keratinocytes and fibroblasts; SAK, sprayed autologous keratinocytes; SK (allo), sprayed allogeneic keratinocytes; STSG, split-thickness skin graft; uSTSG, ultra-thin STSG.
Experiment 2
The aim of this study was to investigate the effect that MC-delivered keratinocytes had on wound contraction when combined with meshed STSG, as has been undertaken previously in the clinical treatment of full-thickness burns. 17 Square 4-×4-cm full-thickness wounds were created. The average wound size at day 0 was 20 cm2 because of retraction of the skin edges after excision. Wounds were treated using meshed STSG (6:1 ratio) and treatment groups as indicated (Table 1). The experiment was terminated at day 21.
Experiments 3 and 4
The final two studies aimed to evaluate the effect of MC-delivered keratinocytes on wound contraction and epithelialization after dermal reconstruction using the dermal template Integra. Wounds were created as in experiment 2 and treated with Integra. Vascularization of the Integra took 3 weeks in experiment 3 and 2 weeks in experiment 4. Wounds were subsequently treated as indicated (Table 1), and the experiment was terminated 21 days after the application of the treatments to the vascularized Integra.
Porcine cell culture
Porcine keratinocytes were cultured as described by Bevan et al., 31 a modification of the method of Rheinwald and Green 32 that has been described elsewhere. 33 Cells were retrovirally transduced to express GFP as previously described. 31 GFP-positive cells were examined using a Nikon Eclipse TS100 microscope (Nikon) and NIS-Elements software. Porcine fibroblasts were released from the dermis by incubation in 0.5% collagenase I (GIBCO) for 2 hours and cultured in Dulbecco's modified Eagle medium with Gluta-Max (GIBCO) supplemented with 10% FCS (paa, Hampshire, UK).
MC culture
Two g of Cultispher-G were reconstituted in 100 mL phosphate-buffered saline (PBS) for 1 h and sterilized by autoclaving. Before use, MC were washed twice in PBS and medium. Cultured cells at 80% to 90% confluence were released from flasks using 0.05% trypsin–ethylenediaminetetraacetic acid (GIBCO). Cells were transferred to a 100-mL Cellspin magnetic stirrer flask (IBS Integra Biosciences) at a seeding density of 5×106 cells per 5 mL of MC stock solution in a total volume of 40 mL. Cultures were left static for 24 hours, then stirred at 45 rpm for 5 minutes with 40-minute static intervals. At day 7, the total volume was increased to 100 mL and the speed to 50 rpm with continuous stirring. Half of the medium was replaced three times per week. 34
Application of cells
To ensure that an equal number of cells was applied in each treatment group, cells from all groups were counted before application. Aliquots of keratinocytes and fibroblasts were removed from MC using trypsin, and cells were counted in a hemocytometer (Weber); 1×107 keratinocytes (SK (allo), SAK) were applied using a 1-mL syringe fitted with a sterile spray nozzle, as described previously.17,33 MC without cells (MC only), 1×107 keratinocytes (MCK (allo), MCAK) and 1.7×106 fibroblasts (MCAF) on MC were applied to the wound beds using sterile pipettes. Because fibroblasts can outcompete keratinocytes in vitro, the latter were applied in excess. 35
Histology
Twelve- to 15-μm-thick cryostat sections were cut from each quadrant and stained with hematoxylin and eosin (H&E). Immunohistochemistry was used to visualize cytokeratin 14 (CK14), a marker for basal keratinocytes (1:250; Abcam, UK); laminin, an early marker of basement membrane formation (1:250; Abcam); collagen VII, a late marker of the basement membrane (1:200; Abcam); and alpha-smooth muscle actin (α-SMA; 1:200; Sigma), a marker for myofibroblasts. Collagen VII was detected using an ABC staining kit (Vector Laboratories) and slides mounted in DPX (Fisher). K14, laminin, and α-SMA were detected using DyLight secondary antibodies and mounted in Vectamount with 4',6-diamidino-2-phenylindole (Vector Laboratories). Images were acquired and analyzed using a Zeiss Axioscope and Axiovision software (Zeiss).
Image analysis for presence of GFP
Duplicate sections along a horizontal and a vertical line through each wound were photographed (Olympus, BH2), and images were analyzed using ImageJ (National Institutes of Health, Bethesda, MD) to detect the GFP-positive area per total area per section. For statistical analysis, multiple measurements were compared between treatment groups using analysis of variance (ANOVA; all pair-wise comparisons).
Measurement of wound contraction rate
Wound size was plotted using Visitrak (Smith & Nephew, UK), which facilitates accurate measuring of wound size by tracing the wound edges and digitally capturing the measurements. Wound groups were unblinded after animal termination. Measurements from all three animals per experimental group were analyzed using a mixed-model ANOVA.
3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) assay
Reduction of 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) was used to assess cell proliferation; 500-μL samples were removed from MC cultures in duplicate, and medium was replaced with fresh medium containing 10% MTT (Sigma Aldrich, 5 mg/mL stock solution) for 4 hours at 37°C. Samples were washed with PBS to remove unbound MTT, and formazan crystals were dissolved by vortexing in 1 mL of dimethyl sulfoxide (Fisher); 100 μL of each sample was plated in triplicate in 96-well plates and absorbance read at 590 nm (reference filter 620 nm, Sunrise plate reader, Tecan, Switzerland). Absorbance readings were plotted against a standard curve obtained using a serial dilution of porcine keratinocytes or fibroblasts.
Acridine orange
Samples were incubated briefly using acridine orange (BDH Laboratories) at a final concentration of 0.1 mg/mL and then washed with PBS to remove excess stain. Images were acquired using a Nikon Eclipse TS100 microscope and NIS-Elements software.
Results
MC culture
MC were found to support the growth of porcine keratinocytes and fibroblasts in stirred suspension culture after initial expansion of cells on tissue culture plastic. 34 Acridine orange staining showed cells populating the surface of MC (Fig. 1C). Although fibroblasts had populated essentially all MC particles evenly, keratinocytes had attached to only a portion of MC (data not shown). Proliferation on MC was assessed according to the conversion of MTT and showed an increase in the number of keratinocytes and fibroblasts over 13 days in MC culture (Fig. 1A). In the treatment of skin defects, it is beneficial to use highly proliferative cells at low passage numbers in a subconfluent state. 42 Thus, although the rate of cell expansion on MC was significantly lower than on tissue culture plastic (data not shown), our experiment showed that MC culture can support the expansion of porcine keratinocytes and fibroblasts, which can subsequently be used in in vivo experiments.
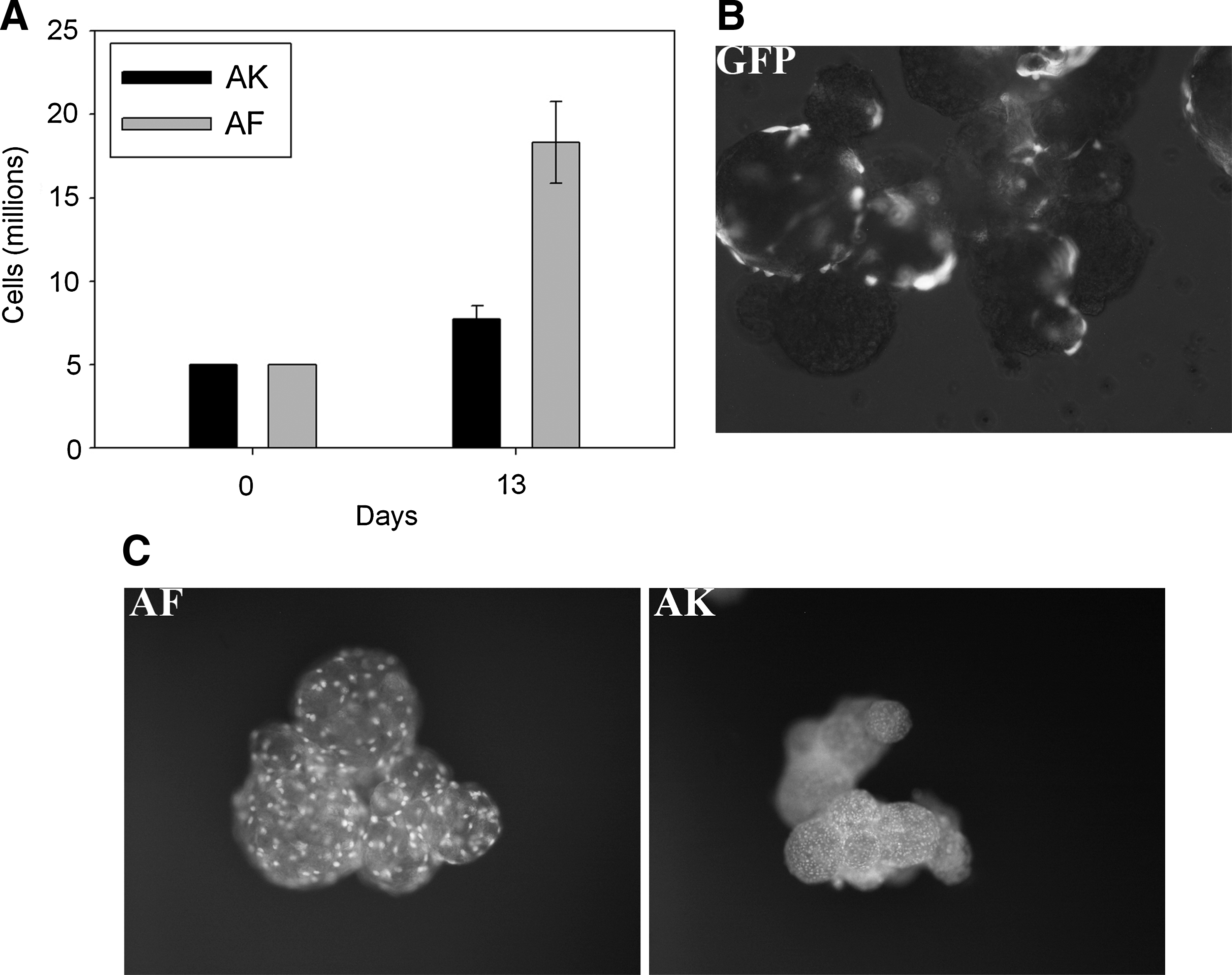
No adverse reaction to any of the treatments and no signs of infection or foreign body–type reaction were observed in any of the animals in any of the four in vivo experiments. To track the fate of keratinocytes when introduced onto the wound bed, cells were transduced with GFP (Fig. 1B).
Experiment 1
Experiment 1 was designed to compare how well keratinocytes on MC (MC with AK (MCAK)) survived when introduced onto the wound bed with how well those applied as a free suspension (SAK) survived. All wounds were isolated in chambers to prevent endogenous re-epithelialization from the wound margins.29,30 This ensured that any repopulation of epidermal elements would occur only as a result of the exogenous keratinocytes applied to the wounds. To assess the biocompatibility of the MC in the wound, MC without cells (MC only) were applied to one group of wounds.
GFP-positive regions, primarily located at the surface of the wounds, were observed in wounds treated with MCAK and SAK (Fig. 2B and C). To remove observational bias, all wounds were assessed for GFP content. MC-only wounds showed low levels of autofluorescence, whereas MCAK and SAK wounds showed significant GFP-positive areas (Fig. 2B and C). There was no statistically significant difference in GFP-positive areas between the MCAK and SAK groups, indicating a comparable level of integration of GFP-positive cells between the two application methods (Fig. 2B). Intact epithelia were not observed in any of the wounds at day 15 (Fig. 2A and B), all wounds at this time being characterized by the presence of granulation tissue (Fig. 2C, panel H+E). Immunolabeling for laminin, a component of the basement membrane normally found at the dermal–epidermal junction, showed a striatal distribution of bundles throughout the wounds, rather than the clearly formed basement membrane characteristic of normal tissue (Fig. 2C). We found no evidence of persistence of MC in the tissue by day 15 after application in the MCAK or MC-only groups, although the cells clearly remained, as evidenced by GFP-positive areas. This would suggest resorption of the gelatin MC. Treatment with MC only did not elicit any adverse reactions, indicating that gelatin MC are biocompatible. These outcomes demonstrated that keratinocytes survive the transport and delivery onto the wounds in suspension and on MC and that gelatin MC become resorbed without any adverse reaction.

Experiment 2
We investigated the ability of MCAK or SAK to re-epithelialize the wound bed in conjunction with widely meshed STSG, a situation closely resembling a relevant clinical treatment regime. In this instance, the meshing procedure increased the surface area of the graft 6 times (6:1). STSG alone served as the control group. The effect of these treatments on wound contraction was also assessed. Wound contraction was measured by tracing the edges of the wounds and digitally capturing the images using Visitrak (Smith & Nephew).
At day 21 after treatment, all wounds displayed an intact epithelial layer (Fig. 3). GFP-positive cells were not detected at this point. This is in agreement with our previous findings after treatment with GFP-SAK 36 and those of others,37–39 where GFP was not detectable in long-term studies despite evidence that transplanted cells survived. 36 All wounds showed similar distributions of K14, a marker of proliferating basal keratinocytes (Fig. 3). Immunolabeling for laminin and collagen VII revealed the presence of an intact basement membrane, indicating that the quality of epithelial repair was comparable in all groups (Fig. 3).

Histology shows epithelial cover in all wounds (H+E staining, ×5), the presence of a basement membrane (collagen (Coll) VII, ×20 and laminin (Lam), ×5) and proliferating basal keratinocytes (K14, ×20).
Significantly less wound contraction was found in wounds treated with MCAK (n=6) than with STSG alone (n=6) or SAK (n=6) (p<0.05; Holm-Sidak post hoc test) (Fig. 4, Fig. 6B). This is beneficial to wound healing because it suggests that there might also be less contraction in a human clinical setting. At day 21, there were significant differences (p<0.05) between all treatment groups. STSG wounds had contracted from 20 cm2 to 6.3±0.37 cm2, indicating that these wounds had contracted to 31.7%±1.9% of their original size. In contrast SAK wounds had contracted to 38.7%±2.7% and MCAK to 42.5%±3.2% of their original size (Fig. 4). SAK-treated wounds contracted 22%±8.6% less and MCAK treated wounds 34%±10.1% less than STSG wounds (Fig. 4). The outcomes of this experiment therefore showed that the quality of epithelial repair was comparable between treatment groups but that treatment with MCAK and STSG resulted in significantly less contraction of wounds than STSG alone (p<0.001) or with SAK and STSG (p=0.007).

Experiments 3 and 4
Experiments 3 and 4 investigated the effects on wound contraction and healing of the dermal substitute Integra, which is known to reduce contraction, 33 in combination with sprayed cells or cells delivered on MC. Integra was applied to the wound bed and allowed to vascularize for approximately 2 to 3 weeks while forming a neodermis. The silicon layer covering the Integra was then removed and the wounds treated as indicated. For both experiments, Integra with an ultra-thin sheet skin graft (uSTSG) served as the control. In experiment 3, allogeneic cells were delivered to the wound bed in suspension (SK allo) or on MC (MCK allo), whereas in experiment 4, autologous cells (SAK or MCAK) were used. Comparison of results from these groups allowed determination of any benefit of the delivery of autologous cells over allogeneic cells. Experiment 4 additionally assessed wound contraction in response to treatment with MCAK with the addition of MC with autologous dermal fibroblasts (MCAK/AF).
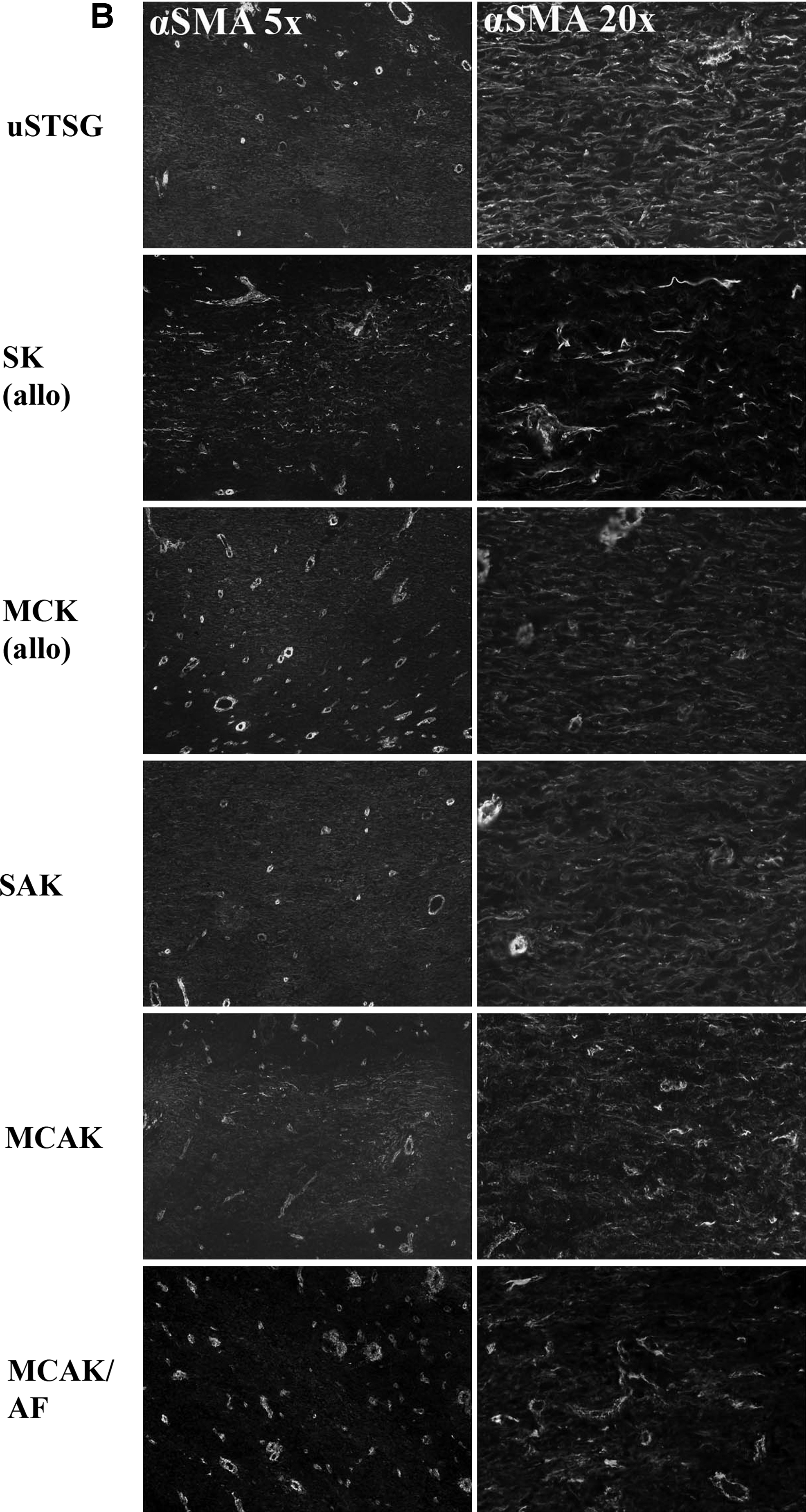
Histological examination showed an intact epithelial layer in all wounds (Fig. 5), which was thought to be derived from the uSTSG in the control wounds and from transplanted keratinocytes in the experimental groups. Immunohistochemistry showed comparable distribution of markers for K14, laminin, and collagen VII (Fig. 5), indicating a comparable quality of epithelial repair in all treatment groups. Staining for αSMA revealed the presence of myofibroblasts, the cell type most closely associated with wound contraction. αSMA in uSTSG wounds was distributed in distinct areas deep within the dermis (Fig. 5), with the myofibroblasts arranged in flat arrays. These were found to be parallel to the dermal–epidermal junction at lower magnification (data not shown). This particular alignment is characteristic of myofibroblasts in a remodelling wound and allows the cells to exert contractile forces on the surrounding tissue.50 There was markedly less αSMA in all other wounds (Fig. 5). Wound contraction was significantly lower in SK (allo) and MCK (allo)–treated wounds than in uSTSG wounds (p<0.001), despite the addition of allogeneic cells (Fig. 6B), with MCK (allo) wounds contracting less than SK (allo) wounds. Contraction of wounds treated with autologous cells (SAK, MCAK, and MCAK/AF) was significantly less (p<0.001) than in uSTSG wounds and (allo) groups. There was no statistically significant difference between the delivery of autologous cells on MC or as a sprayed suspension, although wounds treated with MCAK/AF contracted significantly less (p<0.001) than those treated with AK without fibroblasts (SAK and MCAK) (Fig. 6B). Overall, the uSTSG wounds contracted from 20 cm2 to 3.6±0.24 cm2, which is comparable with the degree of contraction in previous studies 33 and may have been due to poor or slow take of the uSTSG. In comparison, the remaining treatment groups showed less wound contraction by the following percentages: SK (allo) 55%±5.6%, MCK (allo) 79%±7.6%, SAK 152%±11%, MCAK 160%±23.8%, and MCAK/AF 212%±6% (Fig. 6B).


These results show that a significant reduction in wound contraction was achieved by combining Integra with the application of epidermal and dermal cells on MC.
Discussion
The present study describes the culture of porcine keratinocytes and fibroblasts on gelatin MC and presents the results of experiments to test the effects of these constructs on wound healing and contraction in vivo using a porcine model for full-thickness wounds. Previous work has shown good correlation between our porcine model and human wound healing,17,33,40 indicating the suitability of this model in the investigation of treatments for full-thickness wounds in humans.
The relationship between time of healing and contracture formation is well established. There is less scarring and contracture formation in wounds that heal within 3 weeks.41–43 Thus, clinical treatment in the first 3 weeks after injury is critical, and the availability of cells for cell-based therapy is therefore essential. Currently, cells are cultured for clinical use in standard tissue culture flasks and passaged several times to maintain them in a subconfluent state until they are required for surgery. Subconfluent keratinocytes have been shown to facilitate better epithelial repair than cells grown to confluent sheets because these change from a proliferative to a differentiated phenotype. 18 Although the rate of proliferation of keratinocytes and fibroblasts in MC culture was less than with culture in plastic flasks, we were able to obtain sufficient amounts of highly proliferative subconfluent cells at low passage numbers. Thus, the use of MC for the culture of cells for clinical application presents several advantages over established methods.
Our initial in vivo experiment showed that keratinocytes applied as MCAK and SAK survived the transport onto the wound bed. GFP-positive cells were primarily observed in the superficial wound regions, which is consistent with our previous work and that of others.44,45 Despite the application of keratinocytes, intact epithelium was not detected, and wounds consisted primarily of dense granulation tissue. This is consistent with our earlier work, which compared the application of SAK and AK in fibrin glue to full-thickness wounds in a chamber model. In this previous work, 19 only approximately 25% of the wounds displayed epithelial cover after 3 weeks of treatment. In the present study, the wound chambers prevented residual cells from reconstituting dermal and epidermal elements. Therefore we were not surprised to observe that all of the full-thickness wounds were unhealed at 15 days, although because the detection of GFP-positive cells in the wound environment was the primary aim of this experiment, the 15-day time point was chosen. We were also able to confirm the biocompatibility of gelatin Cultispher MC in the porcine model without adverse reaction.
We then assessed whether treatment with MCAK and SAK, in conjunction with widely meshed STSG (6:1), would improve epithelial repair and result in less wound contraction than treatment with STSG alone. Wounds treated with STSG have already been shown to contract less than wounds left to heal by secondary intention. 13 The epidermal and dermal elements in the STSG allow the wound to close by cells migrating from the STSG in addition to migration from the wound margins and contraction.
We found no evidence of GFP at 21 days in wounds treated with GFP-labelled MCAK or SAK. This is consistent with previous studies that have shown that GFP does not persist.36–39 Evidence exists in the porcine in vivo model that expression of transfected marker genes is lost in cells that integrate in the more basal layers of the regenerating epithelium, 45 and our data appear to bear this out.
The quality of epithelial repair was consistent between experimental groups. We did not investigate the contribution of exogenous cells to the mechanism of re-epithelialization due to the loss of GFP, although we observed that the addition of cells, as MCAK or SAK, had a clear effect on wound healing, in relation to wound contraction. Contraction was significantly less after treatment with MCAK or SAK than in wounds treated solely with STSG. This lower contraction could be due to the keratinocytes themselves or their expression of paracrine factors, which may reduce myofibroblast differentiation and subsequent wound contraction. This suggests there may be benefits from combining a cell-based therapy with the application of STSG. Our data are consistent with our previous results comparing STSG and SAK treatments. 33 Furthermore, wounds treated with MCAK contracted significantly less than those treated with SAK, indicating that the delivery of keratinocytes on MC may be beneficial in the treatment of full-thickness wounds.
We also investigated the use of the dermal substitute Integra in combination with allogeneic and autologous cells. The use of allogeneic cells facilitated epithelial closure in a way comparable with that of wounds treated with autologous cells or uSTSG. Allogeneic skin grafts have been shown to be rejected in the porcine model within 12 days of application, 46 but there is evidence that cultured allogeneic sheets grafts survived longer than noncultured allogeneic grafts in a mouse model. This finding was attributed to the loss of Langerhans cells in culture. 47 These highly specialized cells are involved in the graft rejection process through the activation of host T-cells. 46 Allogeneic fibroblasts delivered to partial-thickness porcine wounds on poly (L-lactide) MC were also reported to be well tolerated. 40 Other studies have suggested that allogeneic cells are beneficial in the treatment of skin defects, such as recalcitrant leg ulcers, when combined with the commercial product Apligraf. 48 In our studies, cultured sprayed or MC-associated allogeneic keratinocytes may have contributed to wound re-epithelialization due to the loss of Langerhans cells after cell culture, although oOur data suggest that wound contraction is further reduced when Integra is combined with autologous cells.
Lamme et al. previously reported that the use of autologous fibroblasts in conjunction with acellular dermis reduced contraction in porcine full-thickness wounds. This was accompanied by a reduction in αSMA-positive myofibroblasts. 49 In the present study, we also observed a reduction in αSMA-positive cells in wounds treated with keratinocytes alone or keratinocytes with fibroblasts. Our data suggest that the addition of a cellular component leads to a decrease in contraction of healing wounds. We have yet to test whether the number of cells transplanted to the wound bed has a direct effect on contraction, as Lamme et al. found, 49 although we observed a significantly greater reduction in wound contraction than reported by Lamme et al. 49 by using MC to deliver keratinocytes or keratinocytes with fibroblasts in combination with STSG (6:1) or Integra. Like Lamme et al., 49 we can speculate that the presence of additional cells in the granulation tissue might reduce the need for cells to migrate from the wound margins. This is a process that would normally bring them into contact with the signals necessary for myofibroblast differentiation. We speculate further that keratinocytes or keratinocytes with fibroblasts delivered on MC are more suitable for reducing wound contraction than those delivered in suspension because the latter are damaged by the process of removal from tissue culture plastic. Our data support this idea because wounds treated with cells on MC contracted approximately 10% less than those treated with sprayed cells. This may represent a small but clinically significant change in wound contraction because small reductions in contracture formation can lead to large improvements in function, particularly where the formation of contractures over joints impairs movement. We therefore argue that MC offer a better method of delivery for keratinocytes and fibroblasts and facilitate their efficient integration into the wound, enhancing wound healing.
In conclusion, we have demonstrated that porcine keratinocytes and fibroblasts can be expanded on gelatin MC in suspension culture and applied directly to full-thickness wounds in a porcine in vivo model of wound healing. By using keratinocytes alone and keratinocytes with fibroblasts delivered on MC in combination with STSG or Integra, wound contraction was significantly less than with STSG alone, Integra with uSTSG, or STSG and Integra in combination with cells delivered in suspension. This reduction in contraction represents a highly desirable outcome in the treatment of full-thickness wounds. Our in vivo findings are significant because they show a real potential for clinical benefit to patients being treated for large full-thickness wounds.
Footnotes
Acknowledgments
This work was funded by grants to the Blond McIndoe Research Foundation by SPARKS (The Children's Medical Research Charity) and The Charles Wolfson Trust. The authors are grateful to members of staff at Northwick Park Institute for Medical Research for their help.
Disclosure Statement
No conflicting financial interests exist.