
Abstract
The objective of this study was to assess the effects of maxillary sinus floor elevation with a tissue-engineered bone constructed with bone marrow stromal cells (bMSCs) and calcium-magnesium phosphate cement (CMPC) material. The calcium (Ca), magnesium (Mg), and phosphorus (P) ions released from calcium phosphate cement (CPC), magnesium phosphate cement (MPC), and CMPC were detected by inductively coupled plasma atomic emission spectroscopy (ICP-AES), and the proliferation and osteogenic differentiation of bMSCs seeded on CPC, MPC, and CMPC or cultured in CPC, MPC, and CMPC extracts were measured by MTT analysis, alkaline phosphatase (ALP) activity assay, alizarin red mineralization assay, and real-time PCR analysis of the osteogenic genes ALP and osteocalcin (OCN). Finally, bMSCs were combined with CPC, MPC, and CMPC and used for maxillary sinus floor elevation in rabbits, while CPC, MPC, or CMPC without cells served as control groups. The new bone formation in each group was detected by histological finding and fluorochrome labeling at weeks 2 and 8 after surgical operation. It was observed that the Ca ion concentrations of the CMPC and CPC scaffolds was significantly higher than that of the MPC scaffold, while the Mg ions concentration of CMPC and MPC was significantly higher than that of CPC. The bMSCs seeded on CMPC and MPC or cultured in their extracts proliferated more quickly than the cells seeded on CPC or cultured in its extract, respectively. The osteogenic differentiation of bMSCs seeded on CMPC and CPC or cultured in the corresponding extracts was significantly enhanced compared to that of bMSCs seeded on MPC or cultured in its extract; however, there was no significant difference between CMPC and CPC. As for maxillary sinus floor elevation in vivo, CMPC could promote more new bone formation and mineralization compared to CPC and MPC, while the addition of bMSCs could further enhance its new bone formation ability significantly. Our data suggest that CMPC possesses moderate biodegradability and excellent osteoconductivity, which may be attributed to its Ca and Mg ion composition, and the tissue-engineered bone constructed of CMPC and bMSCs might be a potential alterative graft for maxillofacial bone regeneration.
Introduction
As an important element for bone tissue engineering, a material scaffold could provide mechanical support and act as a suitable substrate for cell proliferation, osteogenic differentiation, and consequent bone ingrowth in vivo.6–7 As a typical representative of cement materials, calcium phosphate cement (CPC) has generated much interest in dental and medical material research since 1986 due to its excellent biocompatibility and bioactivity. 8 It has been investigated as a bone graft and has been used clinically to repair bone defects. 9 CPC, which initially contained an equimolar mixture of tetracalcium phosphate and dicalcium phosphate anhydrous, has been formulated into hydroxylapatite (HA) as a final product. Unfortunately, HA has a slow degradation rate, which may not be sufficient to match the speed of new bone formation and remodeling.10,11 Thus, a new material based on CPC modification, which may possess a more rapid degradation rate to match the rate of new bone formation, is required for bone regeneration in certain clinical situations. 12
Magnesium phosphate cement (MPC), which is composed of magnesium oxide and ammonium phosphate, shares some similar properties with CPC, such as self-hardening performance. Compared to CPC, MPC possesses additional properties, such as rapid setting, high initial strength, and more importantly, fast degradation rate. MPC has been used to fix bone fracture; however, its excessively fast degradation rate and lack of sufficient osteoconductivity compromise its role as an ideal graft for bone regeneration. Based on the above-mentioned properties of CPC and MPC, a novel calcium-magnesium phosphate cement (CMPC) was fabricated by incorporating MPC into CPC to improve the degradation properties of CPC.13,14 Moreover, magnesium (Mg) added to CPC may enhance osteoblast adhesion, thus directly stimulating osteoblast proliferation, and indirectly influencing new bone formation.15,16
For maxillary sinus floor elevation, a large amount of newly formed bone is required to support dental implants, especially for patients with severe atrophic posterior maxillary alveolar bone or who require multiple simultaneous dental implantations. 1 In the present study, we hypothesized that a novel CMPC featuring calcium (Ca) and Mg ions in its chemical composition could enhance the proliferation and osteogenic differentiation of bone marrow stromal cells (bMSCs), while a tissue-engineered bone constructed with CMPC and bMSCs, the most widely used seed cells for bone tissue engineering, may have a better effect on bone regeneration compared with CPC. To verify this hypothesis, the effect of bMSCs for CMPC on proliferation and osteogenic differentiation was assayed by MTT analysis, alkaline phosphatase (ALP) activity assay, alizarin red mineralization assay, and real-time PCR analysis of osteogenic genes in vitro for the first time. A rabbit maxillary sinus floor augmentation model was used to investigate the effect of this novel scaffold for tissue engineering applications in vivo.
Materials and methods
Isolation and culture of primary rabbit bMSCs
Thirty-six male New Zealand white rabbits (body weighing from 2 to 2.5 kg) were used in this experiment. All animal procedures were approved by the Animal Research Committee of the Ninth People's Hospital affiliated to Shanghai Jiao Tong University School of Medicine.
Under general anesthesia with intramuscular ketamine (10 mg/kg) and xylazine (3mg/kg), bone marrow was harvested from the fibula of the rabbits and bMSCs were cultured in Dulbecco's modified Eagle's medium (DMEM, Gibco) with 10% fetal bovine serum (FBS, Gibco) in an incubator, as described previously. 1 The cells were cultured for about 10 days until a confluence of approximately 80% was reached following the first passage; the medium was then replaced with osteogenic medium (DMEM, 10% FBS, 50 μg/mL L-ascorbic acid, 10 mM glycerophosphate, and 100 nM dexamethasone) (Sigma). It usually takes 6∼7 days for an additional passage to occur; bMSCs obtained after the second passage were used for further studies.
Preparation of biomaterial extracts
Three kinds of porous granules (CPC, MPC, and CMPC) were prepared as described previously (Rebone Biomaterial Co. Ltd.) and were sterilized by cobalt 60 (60Co) irradiation.17,18 One gram of CPC, MPC, and CMPC scaffold was soaked in 5 mL osteogenic medium and incubated for 1 day in an incubator. Then, the extracts were centrifuged and the supernatant was sterilized through a 0.22μm filter (Millipore) (ISO10993-1). 19
The ion concentrations of magnesium (Mg), calcium (Ca) and phosphorus (P) in each extract were measured by inductively coupled plasma atomic emission spectroscopy (ICP-AES, IRIS 1000, Thermo Elemental). 17
Cell proliferation assay
To determine the proper working concentrations of the extracts for further studies, a series of dilutions (to 1/2, 1/4, 1/8, 1/16, 1/32, and 1/64) was tested. The cells were seeded in 96-well plates at a density of 5×103 cells/well in triplicate and cultured in the osteogenic medium. After 1 day, the culture medium was replaced with the osteogenic medium supplemented with various concentrations of the extracts, and then cultured for an additional 1 day, 2 days, 3 days, and 4 days. The MTT assay was used to assess the amount of viable cells. In brief, the cells were placed in culture medium containing MTT and incubated for 4 h. DMSO (Sigma) was used to stop the reaction, and the absorbance value was measured at 490 nm with a microplate reader (Bio-tek, Elx800,). The results are expressed as units of optical density (O.D.) absorbance values. In addition, bMSCs were also seeded on scaffolds (CPC, MPC, and CMPC) in 96-well plates at a density of 2×107 cells/mL in triplicate and cultured from 1 day to 8 days in the osteogenic medium for MTT assay. 20
Osteogenic differentiation of bMSCs
Real-time polymerase chain reation (PCR) assay was performed for osteogenic gene expression of bMSCs cultured in osteogenic medium supplemented with the biomaterial extracts described above. bMSCs were seeded in 6-well plates at a density of 8×104 cells/well, and total RNA was harvested using the Trizol reagent (Invitrogen) at days 4 and 7. The RNA was used to synthesize complementary DNA (cDNA) with a PrimeScript 1st Strand cDNA Synthesis kit (TaKaRa, Japan). Real-time PCR analysis was performed with using a Bio-Rad real-time PCR system (Bio-Rad, MyiQ™), on markers of ALP and osteocalcin (OCN); glyceraldehyde-3-phosphate dehydrogenase (GAPDH) was analyzed as the housekeeping gene for normalization. 21 . The primers used in this experiment are shown in Table 1.
PCR, polymerase chain reaction; ALP, alkaline phosphatase; OCN, osteocalcin; GAPDH, glyceraldehyde-3-phosphate dehydrogenase.
At day 3, 6, and 9, the ALP activity of bMSCs seeded on CPC, MPC, and CMPC was measured with the ALP assay in osteogenic medium. 22 Briefly, cells were detached with 0.25% trypsin/ethylenediaminetetraacetic acid and suspended in lysis buffer with 0.1 mL of 0.2% NP-40 in 24-well plates; then, the cells were mixed with 0.1 mL of 1 mg/mL p-nitrophenyl phosphate (Sigma) in 1 M diethanolamine buffer and incubated at 37°C for 15 min in a bench shaker. The reaction was stopped by adding 3 N sodium hydroxide. ALP activity was quantified by absorbance measurements at 405 nm. The total protein content was determined by the Bradford method using the Bio-Rad protein assay kit (Bio-rad) and a series of bovine serum albumin standards. ALP levels were normalized to the total protein content at the end of the experiment.
To detect mineralization, bMSCs cultured on scaffolds for 28 days were washed twice with PBS and fixed in 70% ethanol for 1 h. Then, the cells were stained with 40 mM Alizarin red solution for 20 min at room temperature. After staining, the cells were washed with PBS and then incubated in 10% hexadecylpyridinium chloride (Sigma) for 1 h. Finally, the absorbance of the resulting solutions was measured at 590 nm (Bio-tek, Elx800), as described previously. 22
Preparation of cell material complex used in vitro and in vivo
The bMSCs were detached from culture dishes, resuspended in the culture medium without FBS, and then combined with the scaffolds (CPC, MPC, and CMPC) at a density of 2×107 cells/mL for maxillary sinus elevation in vivo. 23 Meanwhile, the extra cell/scaffold complexes were cultured for 1 day, fixed in 2% glutaraldehyde for 2 h and then observed by scanning electron microscopy (SEM, Philips SEM XL-30), and the compositions of three scaffolds were detected by energy dispersive spectrometry (EDS, JEOL). 24
Maxillary sinus floor augmentation procedure
Thirty-six rabbits were randomly divided into week 2 and week 8 groups. Maxillary sinus floor elevation surgeries were performed bilaterally on all rabbits from both groups, and the cavities randomly filled with the following six groups of grafts: group A, CPC materials alone; group B, MPC materials alone; group C, CMPC materials alone; group D, CPC/bMSCs complex; group E, MPC/bMSCs complex; and group F, CMPC/bMSCs complex. Six cases were analyzed for each group at each time point.
The rabbits were anesthetized with an intramuscular injection, using ketamine (10mg/kg) and xylazine (3 mg/kg). A 3 cm vertical midline incision was made and the skin and periosteum was subsequently raised to expose the nasal bone and nasoincisal suture line. Under continuous sterile saline solution irrigation, two oval nasal bone windows (8×4 mm) were outlined bilaterally on the nasal bone using a round bur. To avoid damage to the antral membrane, a Freer elevator was used to gently push the membrane inward with the respiratory rhythm of the subject. The membrane was then raised from the floor and lateral walls of the antrum to provide a large compartment (13×3×5 mm). Then, the compartment was slightly filled with a graft from each group. Finally, the periosteum and skin were restored and sutured.
Sequential fluorescent labeling
A polychrome sequential labeling method was carried out to label the mineralized tissue and assess the time course of new bone formation and mineralization in the week 8 groups. 25 At 2 and 4 weeks after surgery, the animals were intraperitoneally administered 25 mg/kg of tetracycline (TE, Sigma) and 30 mg/kg of alizarin red (AL, Sigma). Finally, 20 mg/kg of calcein (CA, Sigma) was administered 3 days before the animals were sacrificed at week 8.
General and histological observation
The rabbits were sacrificed at 2 or 8 weeks after operation, exsanguinated, and perfused via the jugular vein with 10% buffered formaldehyde. The augmented maxillary sinus was bisected by the sagittal plane of mesiodistal direction and cut into two blocks along the top of augmented maxillary sinus. One half was further decalcified, embedded in paraffin, sectioned into 4 μm thick sections, and stained with hematoxylin–eosin (HE). The other half was dehydrated in ascending concentrations of ethyl alcohol ranging from 75% to 100% and finally embedded in polymethylmethacrylate. The specimens were cut into 200 μm thick sections using a microtome (Leica) and were subsequently ground and polished to a thickness of 40–50 μm.
Histological and histomorphometric observation
General histological analysis was performed using an automated image analysis system (Image-Pro Plus). Four HE slides randomly selected from serial sections of each sample were used to analyze the newly formed bone area (i.e., the percentage of newly formed bone area in the raised area).
To observe the fluorescent labeling of the undecalcified sections, a confocal laser scanning microscope (Leica TCS Sp2 AOBS) was used. Excitation/emission wavelengths for each of the fluorochromes were as follows: 405/580 nm (TE, yellow), 543/617 nm (AL, red), and 488/517 nm (CA, green).26–28 To quantify the bone formation and mineralization in the raised area, fluorescence microscopy images were taken at the top, mesial, center, distal, and bottom of each section as described in our previous study; 25 this included fluorescence microscopy images of the fluorochromes TE, AL, and CA, one merged image of the three fluorescent labels for evaluating mineralization of elevated sinus floor, and one image using transmission light microscopy without a specific filter combining the former merging image. Then, the percentage of each fluorochrome staining was calculated using the automated image analysis system (Image-Pro Plus) as described previously, which represented the bone formation and mineralization at 2, 4, and 8 weeks after the operation. 1
The undecalcified sections were further stained with Van Gieson's picro fuchsin for histological observation. The percentage of residual material scaffolds for each group in the raised area at week 8 was calculated using an automated image analysis system (Image-Pro Plus).
Statistical analysis
Statistical analysis was performed by ANOVA and SNK post hoc or Kruskal–Wallis nonparametric procedure followed by the Mann–Whitney U test for multiple comparisons based on the normal distribution and equal variance assumption test. All statistical analyses were performed using the SAS 8.2 statistical software package (SAS) and significant differences were indicated by p<0.05.
Results
The Ca, Mg, and P ion concentrations of the biomaterial extracts
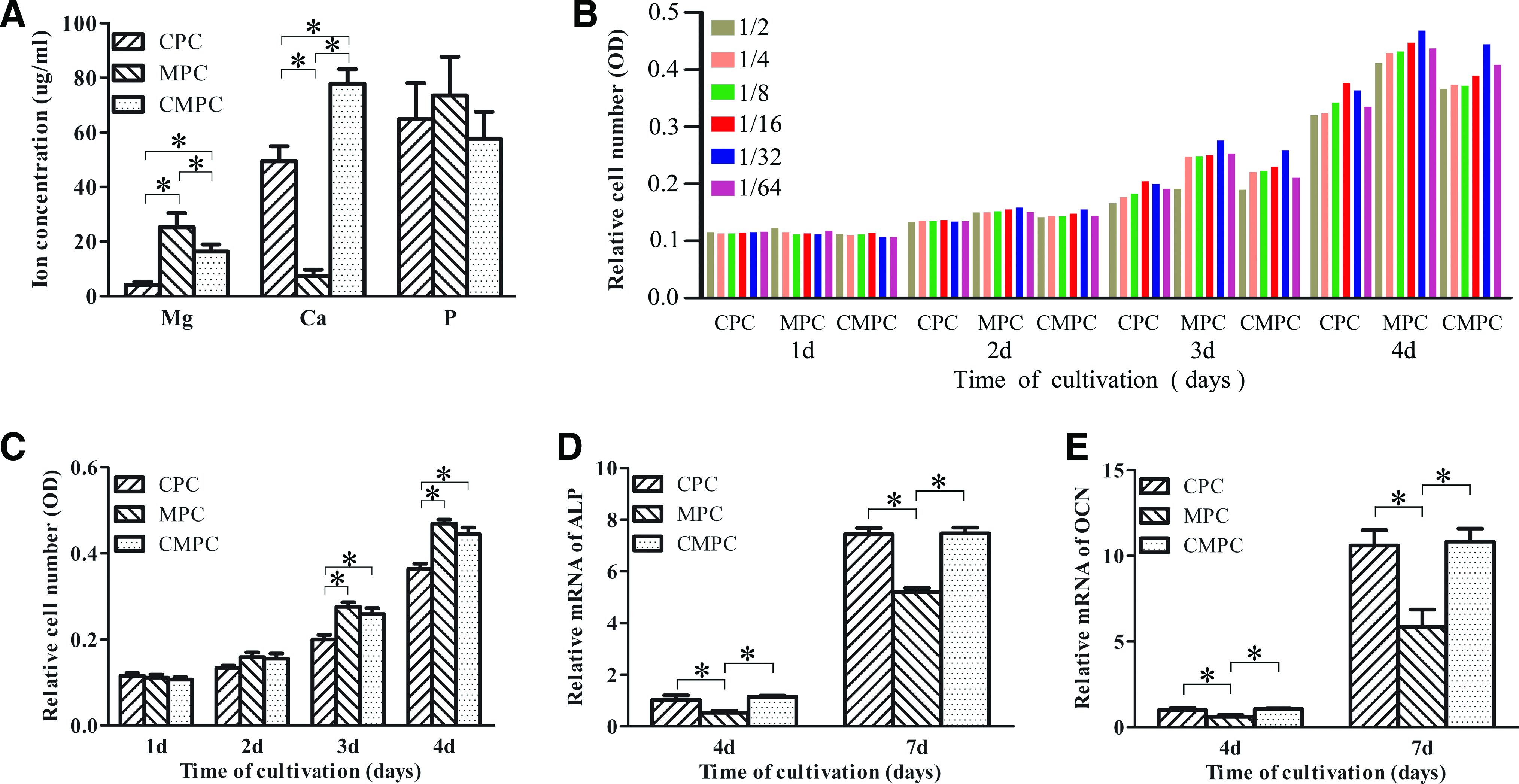
The concentrations of the Mg, Ca, and P ions in osteogenic medium after soaking the CPC, MPC, and CMPC scaffold for 1 day are shown in Fig. 1A. The CMPC and MPC scaffolds showed a more intensive release of Mg compared with the CPC scaffold. In addition, the Ca ion concentrations of the CMPC and CPC scaffolds were significantly higher than that of the MPC scaffold. As for the P ion concentration, no significant difference was detected among the three extracts.
The ion concentrations of magnesium (Mg), calcium (Ca), and phosphorus (P) in osteogenic medium after soaking the calcium phosphate cement (CPC), magnesium phosphate cement (MPC), and calcium-magnesium phosphate cement (CMPC) scaffolds for 1 day
Cell proliferation
The proliferation of bMSCs cultured under different concentrations of the CPC, MPC, and CMPC extracts was detected by MTT assay, which was used to define an optimal concentration of the three extracts for further studies. The MTT assay suggested that proliferation proceeded more significantly when the bMSCs were cultured in a 1/32 dilution of the CPC, MPC, and CMPC extracts (Fig. 1B), and the proliferation of bMSCs cultured in the CMPC or MPC extracts was significantly higher than that of cells cultured in the CPC extract (Fig. 1C). In addition, Fig. 2A shows that bMSCs seeded on CMPC and MPC proliferated faster than the cells seeded on CPC between days 4 and 8 (p<0.05), with no significant differences presented between days 1 and 3. Furthermore, there were no significant differences between CMPC and MPC. These results indicate that CMPC is superior in facilitating cell growth and promoting cell proliferation compared to CPC, which might be related to the ions released from the material. In this study, a 1/32 dilution of the CPC, MPC, and CMPC extracts was chosen as the appropriate concentration for further study.

Cell proliferation time course.
Osteogenic differentiation of bMSCs cultured in biomaterial extracts or on porous scaffolds
The real-time PCR results show an increased expression of osteogenic genes (ALP and OCN) from days 4 to 7 for cells cultured in CPC, MPC, and CMPC extracts (Fig. 1D, E). The expression of ALP and OCN was significantly enhanced for bMSCs cultured in the CMPC or CPC extract compared with the cells cultured in MPC extract (p<0.05). However, there were no significant differences between the cells cultured in CPC and CMPC extracts. Moreover, the results from the ALP activity assay and semiquantitative alizarin red mineralization analysis show that the osteogenic differentiation of bMSCs seeded on CMPC and CPC was significantly higher than that of bMSCs seeded on MPC, while there were no significant differences between the differentiation of bMSCs on CMPC and CPC; this trend is similar to that observed in the real-time PCR results (Fig. 2B, C). In summary, these results suggest that CMPC also possesses favorable properties for the osteogenic differentiation of bMSCs.
Adhesion and spreading of bMSCs on porous scaffolds
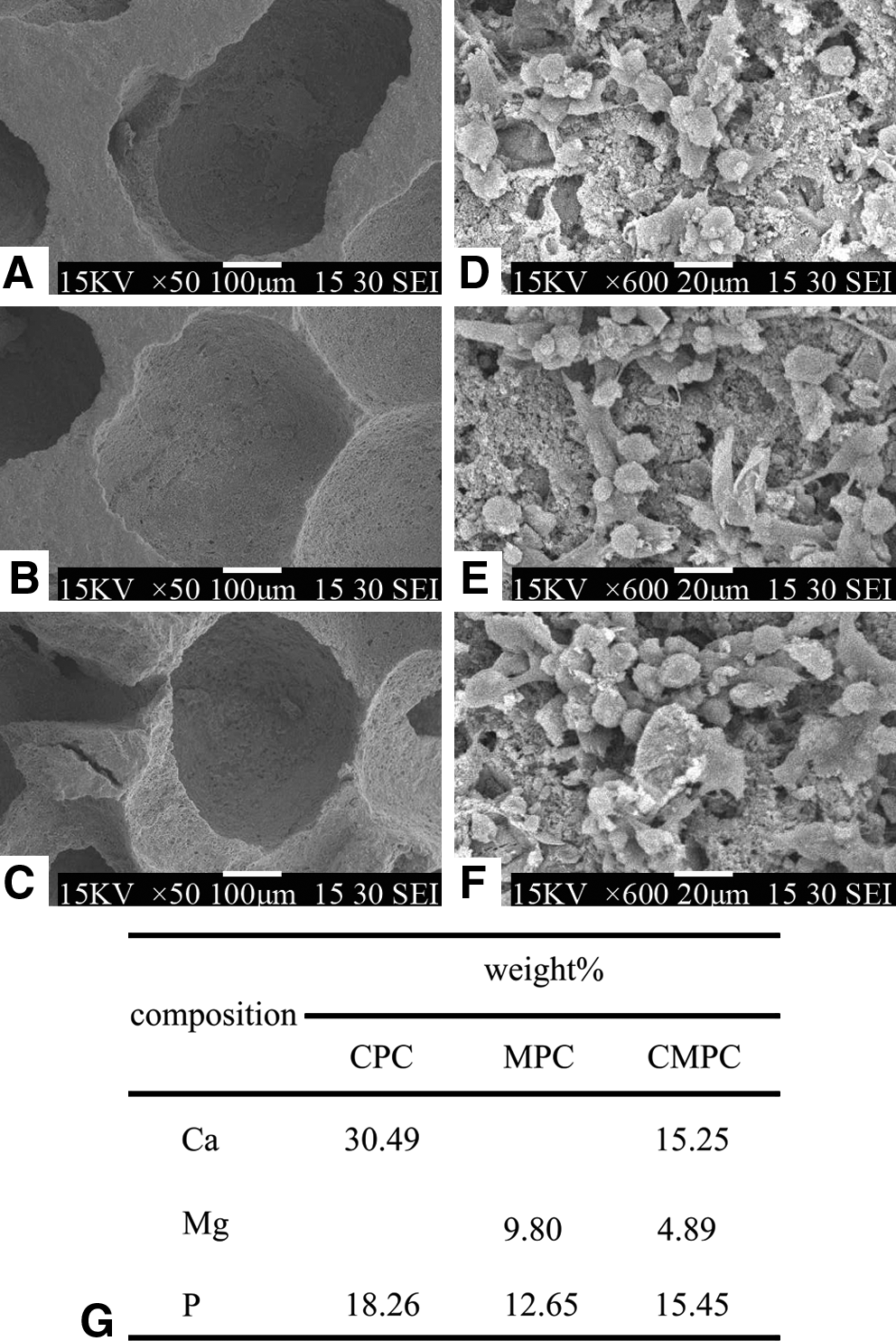
SEM analysis of CPC, MPC, and CMPC indicates that the average pore diameter ranged from 400 to 500 μm (Fig. 3). At 1 day after bMSCs were seeded on the scaffolds, the cells were observed to have adhered well to the scaffold surfaces, which suggested that these porous scaffolds were suitable for the following in vivo study. The corresponding EDS analysis showed that Ca and Mg ions in a ratio of 3.11 were detected on the surface of CMPC, while only Ca ions were present on CPC and only Mg ions on MPC (Fig. 3G).
Scanning electron microscope evaluation of porous CPC (50×)
Histological and histomorphometrical findings
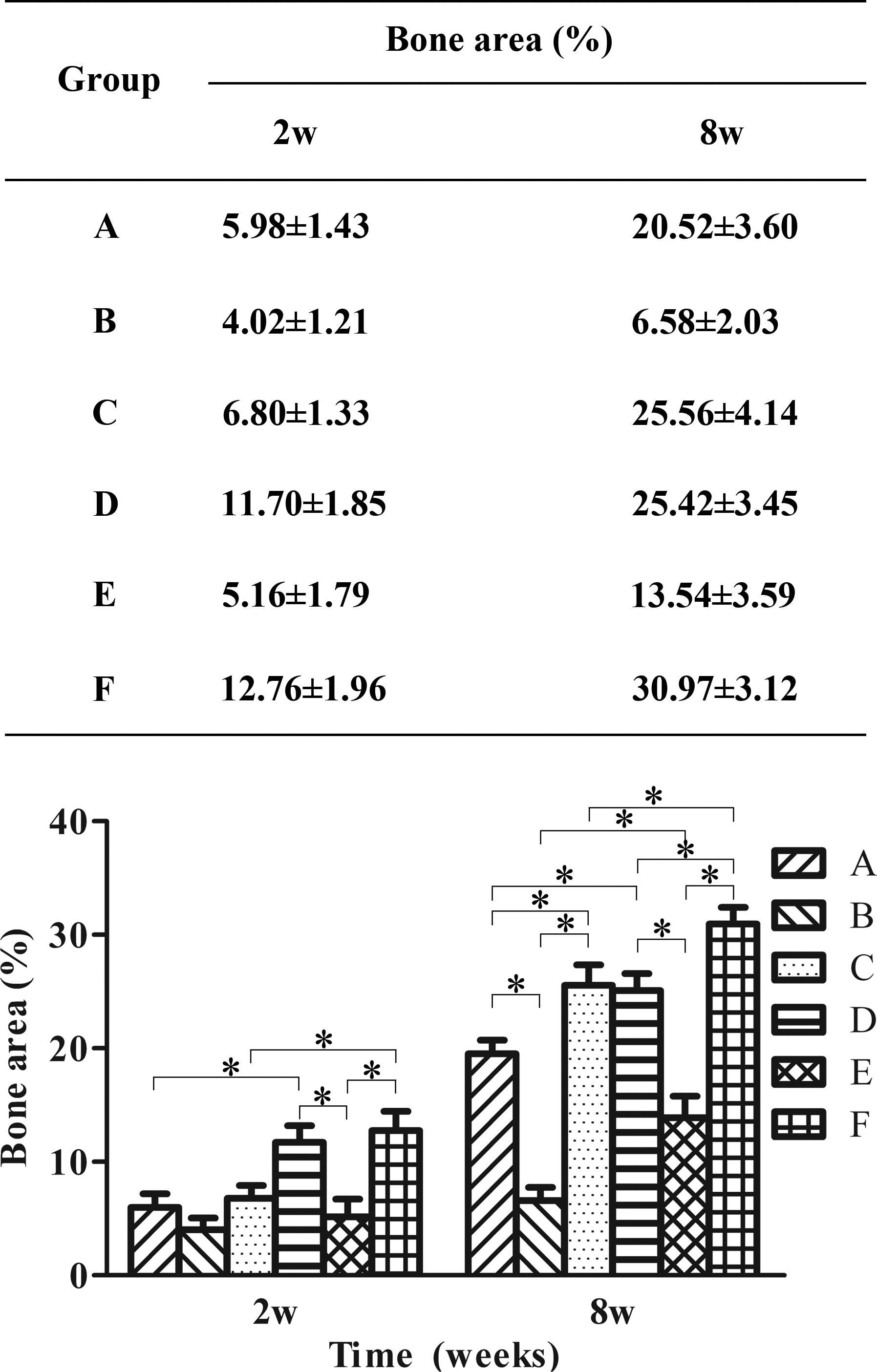
Figure 4 shows that the augmented space was convex and newly formed trabeculae appeared mainly close to the parent bony wall with the raising membrane in all six groups at 2 weeks after operation. The areas of new bone formation were 5.98±1.43%, 4.02±1.21% and 6.80±1.33% for groups A, B, and C, respectively; no significant difference was observed among these groups. The area of new bone formation of group E (5.16±1.79%) was less than the areas of group D (11.70±1.85%) and group F (12.76±1.96%) (p<0.05), and there was a significant difference between group A and group D and between group C and group F (Fig. 6). When the implantation time was extended to 8 weeks (Fig. 5), the extent of new bone formation increased in all six groups. It was also observed that the amount of newly formed bone in the group containing cement material alone was less than that in the cement material/bMSCs complex group. However, there was still less new bone formed in group B (6.58±2.03%) than in group A (20.52±3.60%) and C (25.56±4.14%) throughout the maxillary sinus, and there was a significant difference between group A and group C (p<0.05). The area of new bone formation for group F (30.97±3.12%) was higher compared to those of group D (25.42±3.45%) and group E (13.54±3.59%), and the area of new bone formation for group E was least.

Sequential histological findings of newly formed bone in the maxillary sinus 2 weeks after the operation.
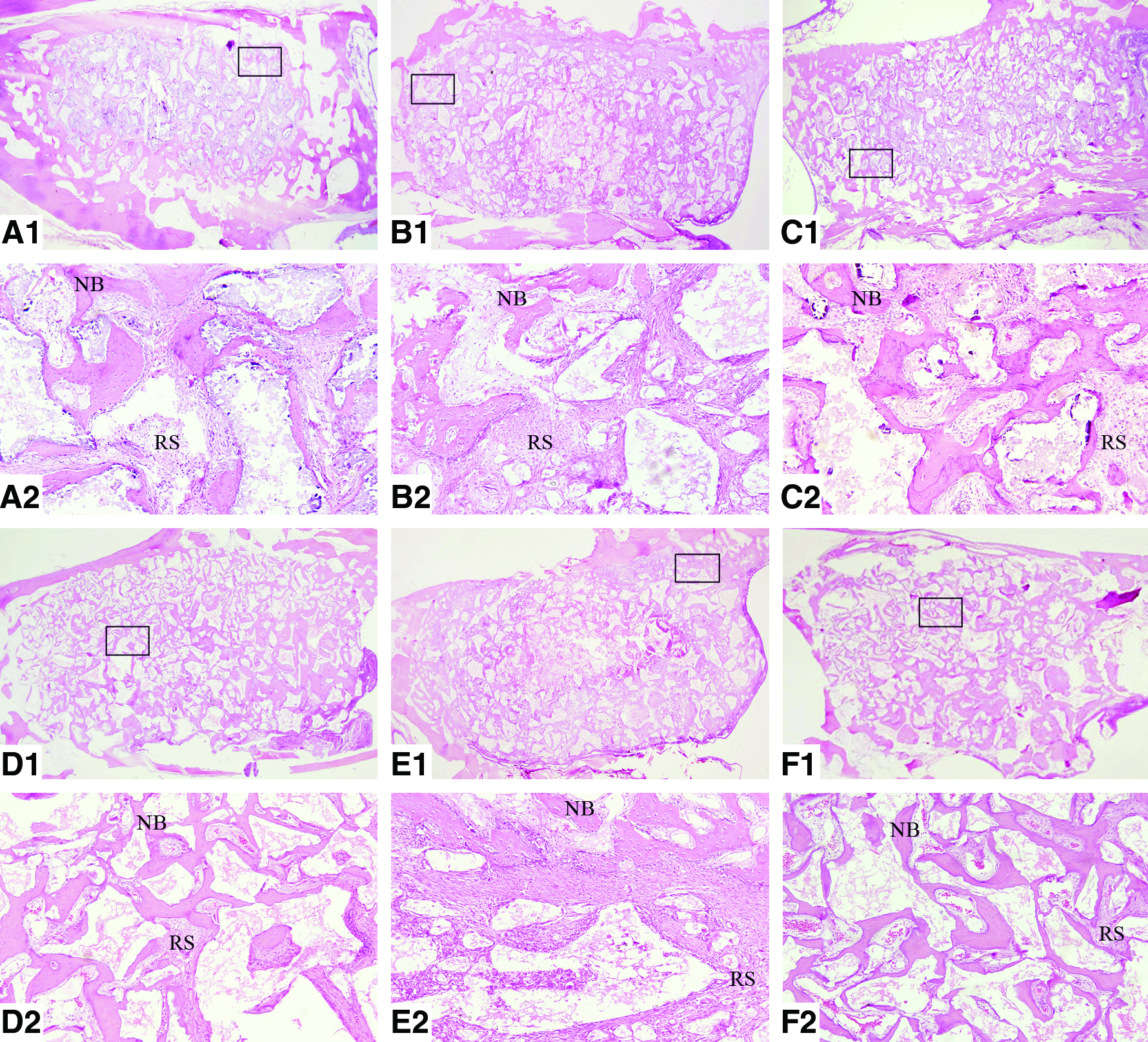
Sequential histological findings of newly formed bone in the maxillary sinus 8 weeks after the operation. A, B, C, D, E, and F represent the CPC, MPC, CMPC, CPC/bMSCs, MPC/bMSCs, and CMPC/bMSCs groups, respectively (NB, new bone; RS, residual scaffold; HE, Hematoxylin-eosin; A1, B1, C1, D1, E1, F1, 12,5×; A2, B2, C2, D2, E2, F2, 100×) (* indicates significant differences, p<0.05). Color images available online at www.liebertonline.com/tea
Sequential histological findings of newly formed bone in maxillary sinus at weeks 8 after operation.
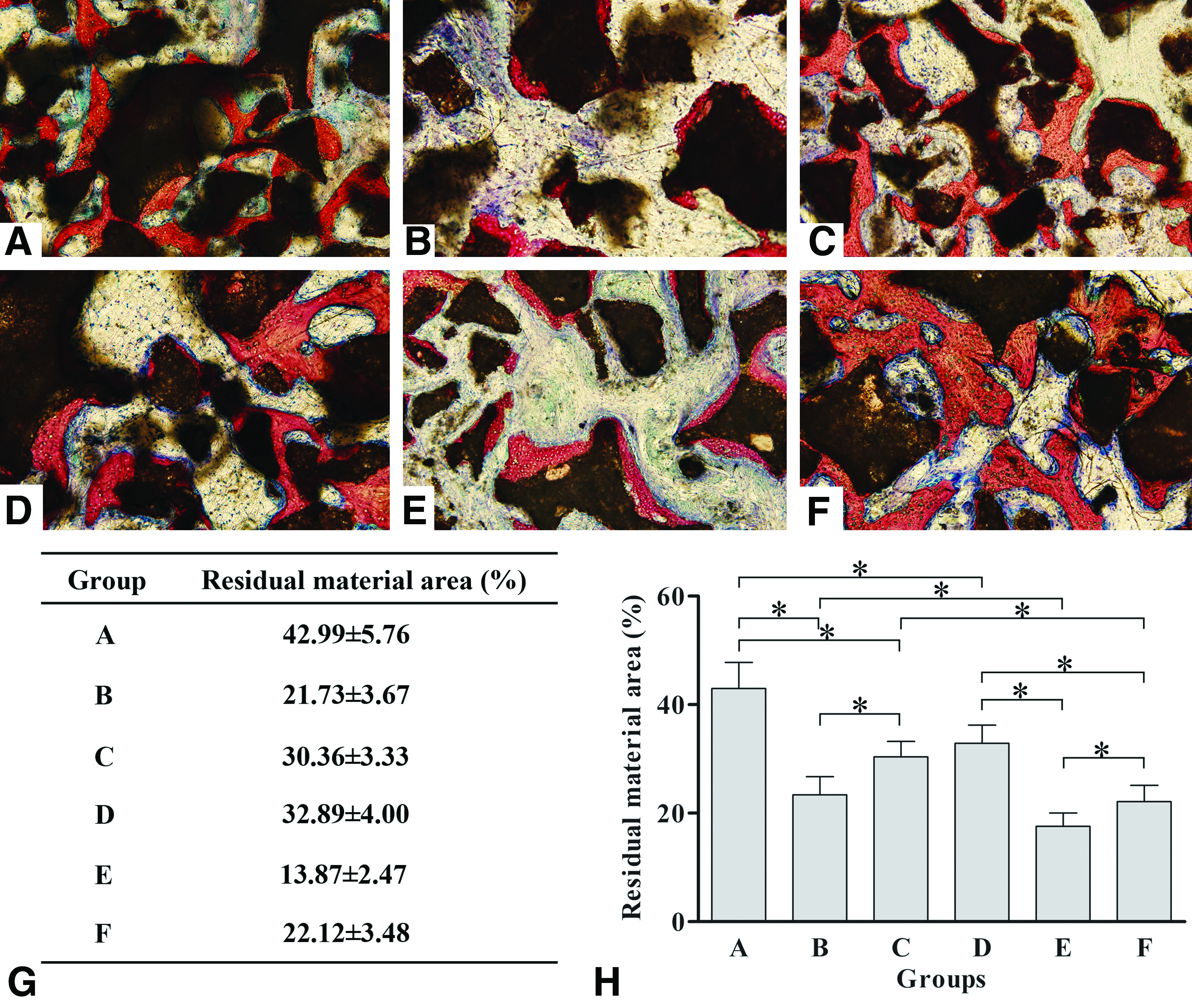
Through the analysis of undecalcified specimens stained with Van Gieson's picro fuchsin (Fig. 7A-F), it was observed that residual scaffolds were surrounded by the newly formed bone in the maxillary sinus augmented space in all six groups. Figure 7G shows that group A had the largest percentage of residual material (42.99±5.76%) compared with group B (21.73±3.67%) and group C (30.36±3.33%) (p<0.05), while group B had the lowest percentage of residual material. The percentage of residual material in group D (32.89±4.00%) was higher than the percentages of group E (13.87±2.47%) and group F (22.12±3.48%) (p<0.05), while the quickest degradation of material was observed in group E. Moreover, the bMSCs seeded on the CPC, MPC, and CMPC materials were observed to accelerate the degradation rate compared to the corresponding groups containing cement material alone. In addition, osteoblast-like cells were seen surrounding the newly formed bone and osteoclast-like multinuclear giant cells were found around the residual material surface (Fig. 8). The analysis of these results suggested that the degradation of CMPC materials could be accelerated by the incorporation of Mg and/or by the combination with bMSCs, which should play an important role in the process of scaffold degradation and bone remodeling.
Microscopic view of bone formation in the maxillary sinus from non-decalcified slides in the CPC, MPC, CMPC, CPC/bMSCs, MPC/bMSCs and CMPC/bMSCs groups (
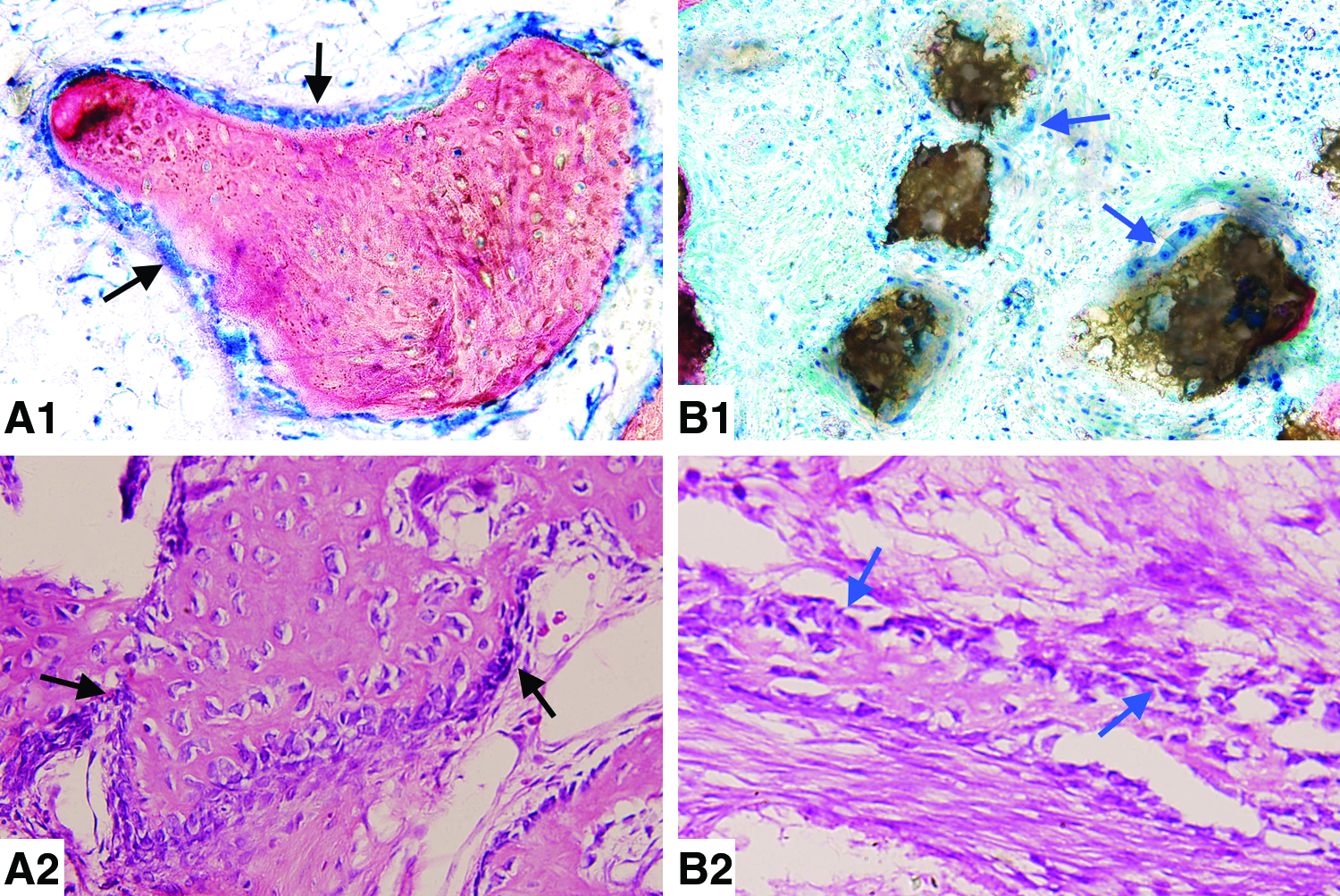
Microscopic view of osteoblast-like cells and osteoclast-like multinuclear giant cells in undecalcified specimens stained with Van Gieson's picro fuchsin (
Fluorochrome labeling analysis
As for the groups sacrificed at week 8, new bone formation and mineralization at 2, 4, and 8 weeks after surgery operation were quantified by calculating the percentage of staining with each fluorochrome (Fig. 9). At 2 weeks after operation, the percentage of TE labeling (yellow) in group C was 1.45±0.30%, which was more than the percentages observed for group A (0.94±0.25%) and group B (0.80±0.26%) (Fig. 10). Moreover, there was a significant difference between group E (1.12±0.30%) and F (1.62±0.30%) (p<0.05), while there was no significant difference between group D (1.38±0.34%) and F. At 4 weeks after the operation, the percentage of AL labeling (red) in group B was 1.20±0.18%, which was less than that in group A (1.93±0.32%) and group C (2.19±0.30%), and the percentage of AL labeling in group E (1.61±0.22%) was lower than the percentages observed for group D (2.61±0.22%) and group F (2.78±0.21%) (p<0.05). Additionally, the percentage of AL labeling in the bMSCs/material groups was higher than that of the groups containing cement materials alone. At 8 weeks after operation, the percentage of CA labeling (green) in group B was 1.54±0.16%, which was less than that in group C (2.06±0.27%); there was no significant difference observed between group A (1.81±0.27%) and C, but the percentage of CA labeling in group F (2.57±0.25%) was more than that of groups C, D (1.92±0.24%) and E (1.67±0.31%) (p<0.05). The analysis of these results shows that the trend regarding the percentage of fluorochrome staining is similar to that of the area of new bone formation, as described above.
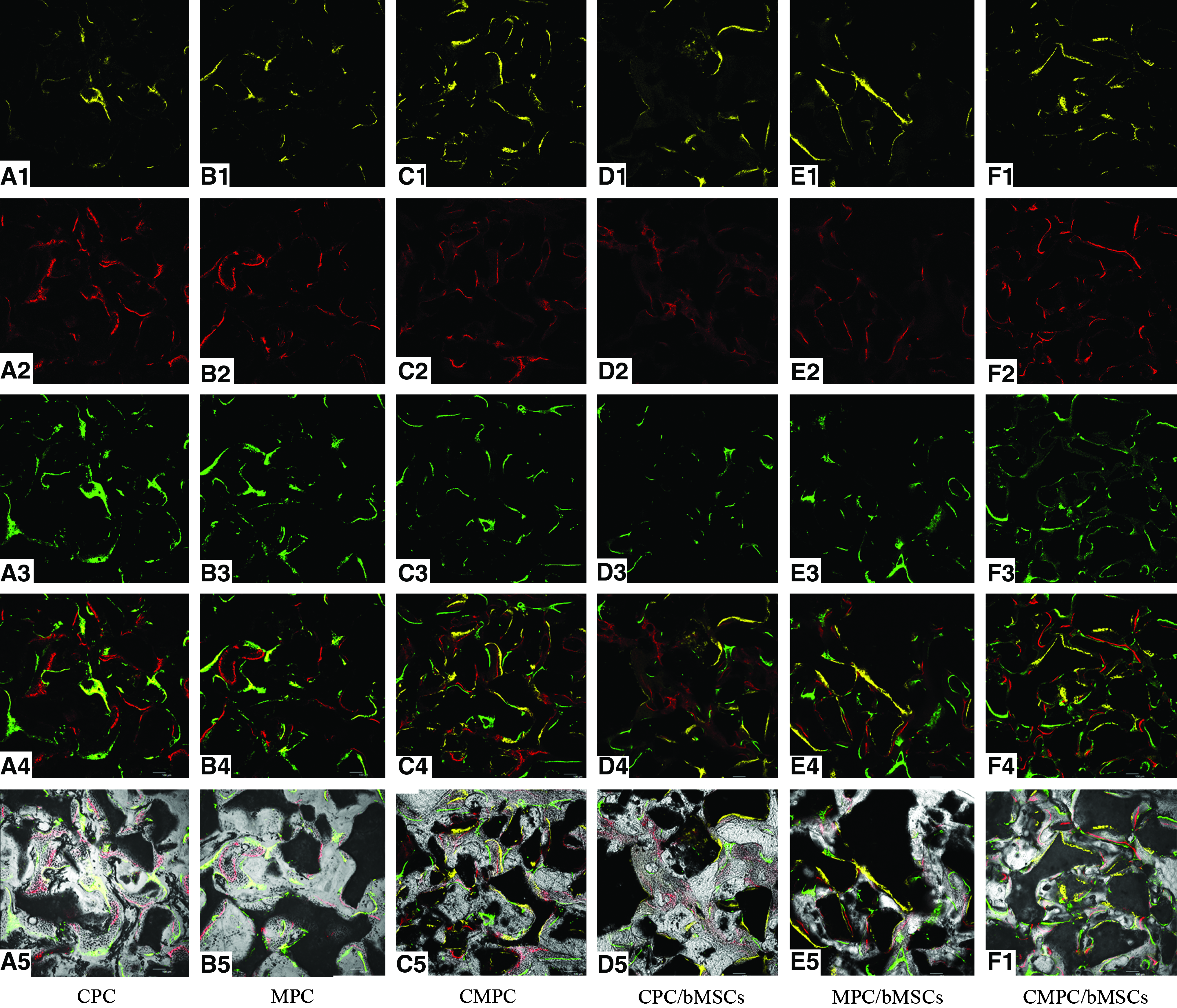
Regarding the groups sacrificed at week 8, sequential fluorescent labeling of TE, AL, and CA was used to determine the rate of bone formation and mineralization at 2, 4, and 8 weeks after operation.
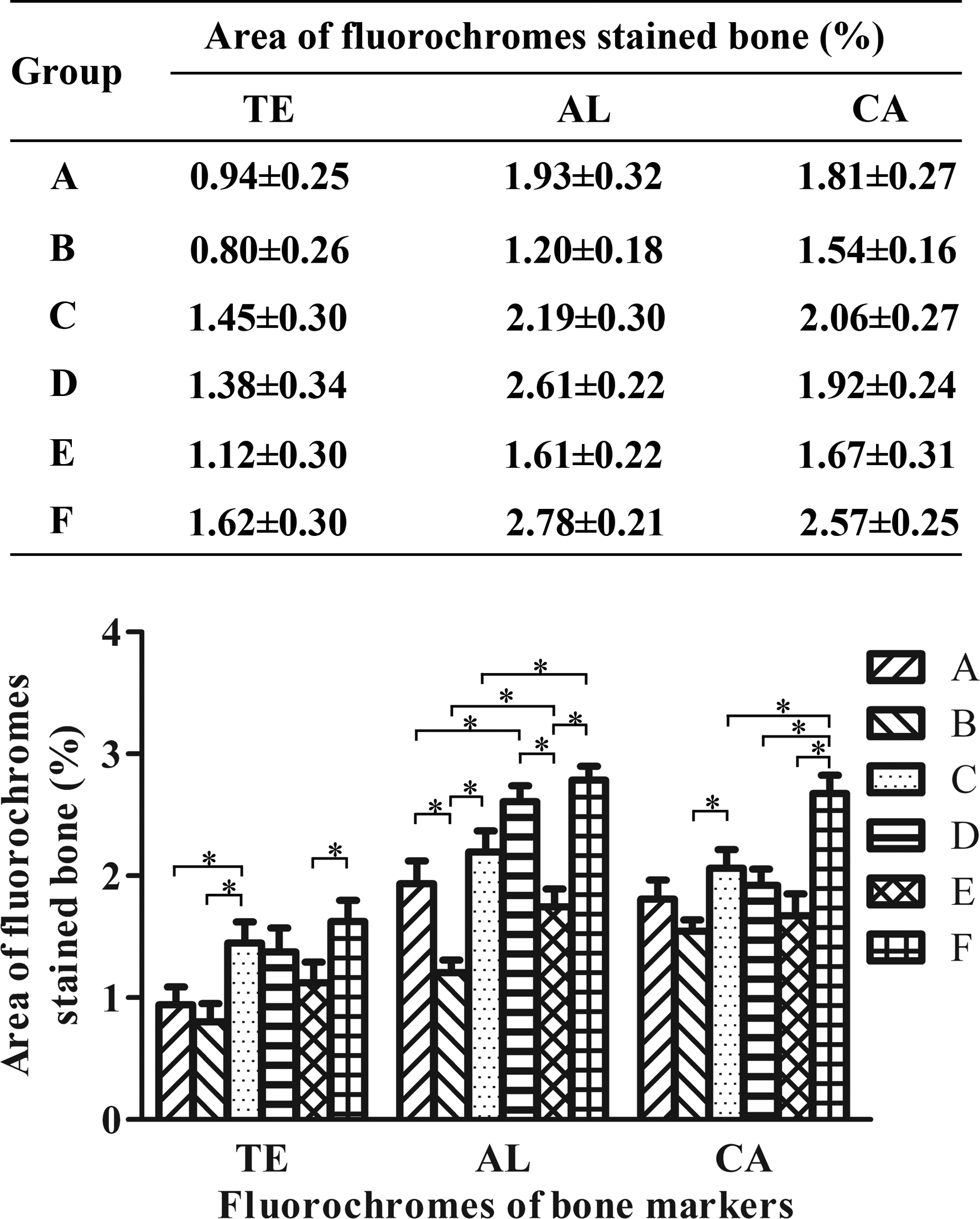
Regarding the groups sacrificed at week 8, the percentage of single fluorochrome staining in maxillary sinus assessed for bone formation and mineralization at 2, 4, and 8 weeks after surgery in the CPC, MPC, CMPC, CPC/bMSCs, MPC/bMSCs, and CMPC/bMSCs groups (* indicates significant differences, p<0.05).
Discussion
The aim of this study was to assess whether a novel CMPC with a chemical composition featuring Ca and Mg ions could enhance the proliferation and osteogenic differentiation of bMSCs and whether CMPC could achieve a better effect on bone regeneration compared with CPC or MPC. In this study, bMSCs were selected as the cell source, which had the capacity to be easily isolated from bone marrow and expanded in vitro to produce large quantities for implantation, 1 Importantly, bMSCs possess the ability to be differentiated into osteoblasts in osteogenic media including dexamethasone, ascorbic acid, and β-glycerolphosphate, and this ability could be further enhanced by certain chemical ions. 29
Cellular responses to a biomaterial, such as attachment, proliferation, and osteogenic differentiation, depend not only on physical properties (surface morphology) but also on the material's chemical composition.30,31 To determine whether the chemical composition of CMPC affects cell behavior, the proliferation and osteogenic differentiation of bMSCs was assayed not only when they were seeded on CPC, MPC, and CMPC, but also when cultured in their extracts. It is known that Ca, Mg, and P ions can be released from CMPC, which is related to bone regeneration; this phenomenon has been further confirmed by the results of ICP-AES in this study.32,33 Additionally, a MTT assay revealed that CMPC could stimulate the bMSCs growth and proliferation compared with CPC. ALP activity and calcium mineralization assay as well as real-time PCR assay on osteogenic genes of ALP, OCN was conducted to demonstrate the enhanced osteogenic differentiation of bMSCs seeded on CMPC or cultured in its extract, and the results revealed that the osteogenic differentiation of bMSCs on CMPC was improved compared to that of bMSCs seeded on MPC. More importantly, the trend regarding the proliferation and osteogenic differentiation of bMSCs seeded on scaffolds or cultured in their extracts was similar. We believe that the chemical composition of CMPC containing Mg, Ca, and P ions plays an important role in the proliferation and osteogenic differentiation of bMSCs. Previous studies have reported that ionic dissolution products containing Mg from bioactive glasses or ceramics could stimulate osteoblast proliferation.35–37 Another study has demonstrated that additional Ca ion supplementation could enhance the mineralization of osteoblasts. 38 We believe that the effect of CMPC on proliferation might be related to Mg ions, while the effect on osteogenic differentiation might be related to Ca ions, although we could not absolutely rule out the influence of structure. Moreover, bMSCs were observed to spread along the material surface and proliferate well after being cultured in vitro. These results suggest that CMPC has good biocompatibility and can facilitate bMSCs adhesion onto its surface. Overall, CMPC achieves better effects on the proliferation of the bMSCs compared with CPC and better stimulates the differentiation of bMSCs compared to MPC, which might be attributed to the release of substances containing Ca and Mg ions from CMPC. However, the mechanism and corresponding signaling pathway is currently far from being fully elucidated and requires further investigation.
A histological and histomorphometrical analysis as well as fluorochrome labeling analysis was conducted to evaluate new bone formation and mineralization. It was observed that porous CMPC could promote new bone formation and mineralization with respect to CPC or MPC. This might be attributed to the enhanced effect on proliferation of resident bMSCs compared to CPC, which could indirectly influence new bone formation, and the enhanced effect on osteogenic differentiation of bMSCs compared to MPC. Throughout the entire observation period, the degree of new bone formation was observed to increase in the CPC/bMSCs, MPC/bMSCs, and CMPC/bMSCs groups compared to the CPC, MPC, or CMPC groups, respectively. The results suggest that the implanted bMSCs played an important role in this respect. During tissue-engineered bone formation, implanted seed cells could promote new bone formation via different pathways, such as cellular osteogenic activity, cell-mediated paracrine stimulation of resident osteoprogenitor cells, or cell-mediated vascular ingrowth. 39 Moreover, the chemical composition of CMPC containing Mg, Ca, and P ions could enhance the proliferation and osteogenic differentiation of implanted bMSCs as well as resident bMSCs and consequently promote the overall effects on new bone formation and mineralization, which might contribute to most of the newly formed bone in the CMPC/bMSCs group.
It is accepted that the biomaterials used for bone regeneration should be resorbable and gradually replaced by newly formed bone in a physiological environment. However, previous studies have shown that the degradation rate of CPC is too slow to match the rate of new bone formation,25,40 which is also confirmed by the results regarding the highest percentage of residual scaffold material presented in this study. At the same time, the percentage of residual material for MPC was the lowest among these groups. As for CMPC, which had the largest new bone formation area, the degradation rate was significantly higher than that of CPC but lower compared to that of MPC. The slower degradation rate of CPC might be attributed to the formation of hydroxyapatite by the hydration of CPC at a relatively low dissolution rate. 41 The degradation of MPC and CMPC is also correlated with their chemical composition. 42 The quick degradation of pure MPC may be attributed to the rapid dissolution of NH4MgPO46H2O, while the degradation of CMPC was accelerated due to the presence of Mg-for-Ca hydroxyapatite. Moreover, the addition of bMSCs could accelerate the degradation of each material. Previous studies have shown that the presence of implanted bMSCs could create a permissive suitable microenvironment for bone formation and mineral resorption, such as through the existence of extracellular matrix (ECM) protein and osteoblasts, which could facilitate multinuclear giant cells adhesion via different pathways, and the materials could be resorbable by organic acids from multi-nuclear giant cells in vivo. 43 Based on the results, the excessively slow degradation rate of CPC with Ca ion composition or the excessively rapid degradation rate for MPC containing Mg ions might limit their final effect on bone regeneration, while CMPC containing both Ca and Mg ions could achieve better effect results for maxillary sinus elevation as a scaffold for bMSCs, which is related to its enhanced effects on cell proliferation and osteogenic differentiation, as well as the appropriate degradation rate to better matching with more newly formed bone.
Conclusion
In this study, it was demonstrated that CMPC featuring Ca and Mg ions could enhance the proliferation of bMSCs with respect to that of CPC and stimulate the differentiation of bMSCs to a greater extent compared to MPC. As for maxillary sinus elevation, CMPC combined with bMSCs exhibited the largest newly formed bone area. It is concluded that CMPC possesses moderate biodegradability and excellent osteoconductivity ability, which may be attributed to its Ca and Mg ion composition. Therefore, the tissue-engineered bone constructed with CMPC and bMSCs might be a better alternative for maxillofacial bone regeneration.
Footnotes
Acknowledgments
This work is supported by the National Basic Research Program of China (973 Program, 2012CB933600(4)), the National Natural Science Foundation of China (30973342), the Program for New Century Excellent Talents in University (NCET-08-0353), the Science and Technology Commission of Shanghai Municipality (10430710900, 10dz2211600), the Shanghai Education Committee (07SG19), and the Doctoral Innovation Foundation of Shanghai Jiao Tong University School (BXJ201127).
Disclosure Statement
No competing financial interests exist.