
Abstract
The objective of this study was to determine whether the local administration of stromal cell-derived factor-1 (SDF-1) using ultrapurified alginate gel (UPAL gel) could improve reparative tissues of osteochondral defects compared with those without treatment. For the investigation, a full-thickness osteochondral defect 4.5 mm in diameter and 3 mm in depth was created in the patella groove of the distal femur in rabbits. Local expression of SDF-1 protein was temporarily upregulated at 1 week after creating the osteochondral defect. The local administration of SDF-1 enhanced the migration of host cells, mainly bone marrow stromal cells (BMSCs), to the site of the osteochondral defect. In vitro cell migration assay supported this result. In the SDF-1 (UPAL gel containing SDF-1) treatment group, the histological scores and the compressive modulus of reparative tissues were significantly improved compared with the no-treatment and vehicle (UPAL gel without SDF-1) groups. On the other hand, SDF-1 did not influence the cellular proliferation and chondrogenesis of BMSCs. Based on the results obtained here, we speculate that SDF-1 enhances the reparative process of osteochondral injuries not through direct effects on the behavior of host cells, but through increased migration of host cells to the injured site. UPAL gel, as a vehicle material, may play an important role in chondrogenesis of recruited cells, mainly BMSCs. The cell-free approach with local administration of SDF-1 may be an effective strategy for developing a minimally invasive technique for cartilage tissue regeneration.
Introduction
One of the possible reasons for the unexpected outcome is the adverse effects resulting from the invasive procedures used in the current ACI technique. The current technique requires a two-stage operation. The first stage is to harvest normal cartilage tissue to isolate chondrocytes. The second one is to implant the isolated cells cultured for 2–5 weeks into the osteochondral defect with periosteal coverage. Further, these processes necessitate a wide arthrotomy for cellular implantation and further exposure to harvest the periosteum.17,19–21
To prevent adverse effects related to the invasive procedures, a novel cellular implantation system without the need for periosteal coverage, and which can be arthroscopically performed, must be established. For this purpose, we developed an in situ forming gel based on alginate as an injectable delivery vehicle for bone marrow stromal cells (BMSCs). 22 The endotoxicity of this naturally occurring material was drastically reduced by the developed technique of ultrapurification. 22 This ultrapurified alginate gel (UPAL gel) has favorable biological effects on in vitro chondrogenesis of BMSCs. 22 Based on the concept of fixing material in the cartilage defect without periosteal coverage, a previous study showed that implantation of autologous BMSCs enhanced cartilage repair in osteochondral defects in rabbits. 23 Our previous results led to a scenario in which, if host BMSCs were effectively recruited to the defects, acellular UPAL gel implantation could improve reparative tissue of osteochondral defects.
Stromal cell-derived factor-1 (SDF-1)/pre-B cell growth-stimulating factor, belonging to the CXC subfamily of chemokines such as CXCL12, acts as a key chemokine of stem cell homing to bone marrow for tissue repair after injury. 24 Unlike other chemokines, SDF-1 is unique in that it binds only to its receptor, CXCR4. A recent study suggested dose-dependent migration potential of human BMSCs in response to stimulation with SDF-1. 25 Regarding musculoskeletal tissue repairs, we showed that an increase in local expression of SDF-1 after ligament injury of rats enhanced the homing ratio of BMSCs to the injured site. 26 Kitaori et al., 27 using a mouse model, showed that SDF-1 was induced in the periosteum of fractured bone and promoted endochondral bone repair by recruiting mesenchymal stem cells to the fracture site. However, to our knowledge, no studies have clarified the functional roles of SDF-1 in the reparative process of cartilaginous lesions.
We hypothesized that the combined administration of SDF-1 and UPAL gel could enhance the repair of osteochondral defects by recruiting host BMSCs to the defect site, even through acellular implantation. The final goal of this study was to determine whether the local administration of SDF-1 using UPAL gel could improve the histological findings and biomechanical properties of reparative tissues in rabbit osteochondral defects compared with those without treatment. The obtained results will be helpful in developing a technique for acellular cartilage tissue engineering, which is a safe and minimally invasive approach, with subsequent tissue regeneration by recruiting host BMSCs.
Materials and Methods
Preparation of alginate gel
An in situ forming material based on UPAL gel with a molecular weight of 1700 kDa (Sea Matrix®; Mochida Pharmaceutical Co. Ltd.) that we developed was used in this experiment. 22 This purified alginate has a quite a low endotoxin level of 5.76 EU/g, compared with that of 75,950 EU/g in commercial-grade alginate (Sodium Alginate 500, 199-09961; Wako). The current material was filter-sterilized through a 0.22 μm pore-size filter and then freeze-dried for packaging in a sterilized vial. After addition of 12.5 mL of distilled water sterilized by filtering through a 0.45 μm filter, 2% UPAL gel was used in this study.
In vitro release assay of SDF-1 protein from UPAL beads
Release studies from UPAL beads were performed in phosphate-buffered saline (PBS, pH 7.4) at 37°C. A 40 μL of UPAL bead containing 0.4 μg SDF-1 was placed in a 24-well plate with 1 mL of PBS per well. At each time point (2, 4, 6, 8, 10, 12, and 14 days) after cultivation, the releasate was collected and stored at −80°C. A fresh 1 mL of PBS was added to the samples and they were re-incubated until the following time point. The mount of SDF-1 protein released from the samples was quantified using ELISA kits (R&D Systems), according to the manufacturer's instructions.
Expression of SDF-1 protein at the site of the osteochondral defect
All procedures involving animals were performed under established ethical guidelines approved by the local animal care committee. Fifteen-week-old female Japanese white rabbits (2.6–2.9 kg) purchased from a professional breeder (Japan SLC) were used for creating an osteochondral defect model. Animals were anesthetized by an intravenous injection of 0.05 mg/kg pentobarbital, followed by isoflurane-in-oxygen gas anesthesia. After intramuscular injection of antibiotics (Penicillin G; Meiji-Seika), the bilateral lower extremities of the rabbits were shaved and draped in a sterile fashion. After a 2 cm anteromedial skin incision was made, the patella was everted through a small medial parapatellar approach. Using a power drill (Rexon), a full-thickness osteochondral defect 4.5 mm in diameter and 3 mm in depth was created in the patella groove of each knee. As a sham operation, we opened the knee joints without creating an osteochondral defect through the same surgical approach. At 3 h, 1 week, 2 weeks, and 4 weeks after operation, animals were euthanized by intravenous injection of an overdose of pentobarbital. The knees were excised with a power saw. To clarify the expression of SDF-1 protein at the site of the osteochondral defect, immunohistochemical staining was carried out with a mouse anti-human/mouse SDF-1 mAb (R&D Systems) that cross-reacted with rabbit tissues obtained at each time point. For immunohistochemical analysis, specimens were fixed with 4% phosphate-buffered paraformaldehyde, decalcified, and embedded in paraffin. A 5-μm-thick section was obtained from the center portion of each defect. In addition, the samples were snap-frozen for Western blotting. The frozen samples were crushed with a hammer, then homogenized in 8 M urea, 50 mM phosphate, 10 mM Tris (pH 8.0) buffer using a motorized homogenizer. EDTA (50 mM) was added to an aliquot of the homogenate. After 24-h incubation at room temperature, the homogenate was centrifuged to obtain the supernatant. Levels of SDF-1 protein were then assessed by Western blotting using a mouse anti-human SDF-1 mAb (1:250, R&D Systems).
In vivo cell homing assessment
To quantitatively evaluate cell homing or migration into the defect site after local administration of SDF-1, the number of cells that migrated into the implanted site of UPAL gel was counted at 7 days postoperatively. The implanted gels were removed using a sharp curette and the obtained specimens were fixed with 4% phosphate-buffered paraformaldehyde for 24 h, embedded in paraffin, cut into 5-μm-thick sections from the center of the gel, and stained with hematoxylin and eosin (H-E) using standard histochemical techniques. The experimental groups, including the vehicle, SDF-1, and AMD3100 groups, are described below.
Rabbit cartilage repair model
The osteochondral defects created by the above procedure were dried and filled with 2% UPAL gel containing each protein. The gel did not flow out of the defect site because of its high viscosity. Without any additional coverage or fixation to the implantation site, the capsule and skin were closed with 4-0 black nylon sutures. The rabbits were allowed to freely move in their cages. A previous study demonstrated that the implanted UPAL gel remained at the surface of similar rabbit osteochondral defects to the current ones while maintaining the initial shape at 2 weeks postoperatively. 22 The articular cartilage defects were divided into four treatment groups (n=10 in each group) as follows: defect, no treatment; vehicle, UPAL gel containing 10 μg/mL bovine serum albumin; SDF-1, UPAL gel containing 10 μg/mL SDF-1 (Miltenyi Biotec, Inc.); and AMD3100, UPAL gel containing 250 μg/mL AMD3100, an antagonist of CXCR4 (Sigma-Aldrich). The concentrations of SDF-1 and AMD3100 were determined by our preliminary study (data not shown).
Macroscopic, histological and immunohistochemical evaluations
At 4 and 16 weeks after operation, animals were euthanized for further investigations. The knee samples were obtained by the method described above and photographed with a digital camera for macroscopic evaluation. The specimens were prepared for histological and immunohistochemical analyses as described above. A 5-μm-thick section was obtained from the center portion of each defect. The sections were stained with safranin-O and H-E. To quantitatively evaluate the reparative tissue in each group, macroscopic and histological findings were scored with the 8-point and 28-point grading scales of Niederauer et al., 23 a modification of the scoring system reported by O'Driscoll. 28 The scores were determined by an independent blinded observer. Immunohistochemical staining was performed with anti-type I and anti-type II collagen antibodies (Fuji Pharm. Lab.). For quantitative evaluation of glycosaminoglycan (GAG) content and type II collagen content, the findings of safranin-O and type II collagen staining were scored using the 3-point grading scales of Mohan's scoring system. 29 To ensure an adverse effect of SDF-1 administration, immunohistochemical staining was performed with matrix metalloproteinase (MMP)-13 antibody (Abcam).
Biomechanical analysis of in vivo samples
Biomechanical testing was performed on the samples obtained from the euthanized rabbits and four slices of normal rabbit cartilage as a control. At 4 and 16 weeks after operation, the mechanical properties of the samples obtained from each group were measured using the axial compression test equipment designed by our laboratory for small samples.22,30,31 A rod with a hemispherical tip (2.5 mm in diameter) was vertically pressed at a crosshead speed of 10 mm/min on the sample placed on a grid. The compression modulus was obtained from the initial slopes of the stress–strain curves.
Preparation of BMSCs
BMSCs were isolated from 15-week-old Japanese white rabbits. Bone marrow was obtained from the femurs and tibias by flushing the shaft using a syringe with a No. 18-gauge needle under sterile conditions. BMSCs were isolated according to the procedure reported by Wakitani et al. 32 The cells at second passage were used for further experiments. In a 37°C, humidified 5% CO2 incubator, the isolated cells were maintained in monolayer culture.
Alginate encapsulation and recovery of cells
Cells were suspended in the UPAL-gel at the desired concentration and dropped from a pipette into CaCl2 solution (Wako). The UPAL-gel-BMSC suspension gelled completely at 10 min after contact with the CaCl2 solution. For the recovery of cells from the alginate gel, alginate beads were secured, washed three times with PBS, and then placed in 50 mM EDTA (Gibco BRL Laboratories) in a 37°C, 5% CO2 incubator. Ten minutes later, cells were recovered by centrifugation at 1500 g for 5 min.
In vitro cell viability assay
To investigate the effects of SDF-1 AMD3100 on cellular viability, BMSCs embedded in UPAL gel beads were cultured in DMEM-HG supplemented with 10% FBS and 1% antibiotics. At 0, 1, 2, 3, and 7 days after encapsulation, cultured beads were dissolved as described above. The number of viable cells at each time was counted with Cell Counting Kit-8 (Dojindo Laboratories). For further investigations, the concentrations of SDF-1 and AMD3100 in the beads were 10 μg/mL and 250 μg/μL, respectively. UPAL gel alone was used as a control.
In vitro cell migration assay
We assessed the influence of SDF-1 on cell migration of BMSCs using the CytoSelect™ 96-well cell migration assay (8 μm, Fluorometric Format; Cell Biolabs) following the manufacturer's instructions.33–35 Briefly, feeder tray wells were filled with 150 μL of medium with or without SDF-1. Confluent cells were harvested and 100-μL aliquots of serum-free medium containing 5×105 cells/mL were added to the wells of the membrane tray (upper tray). Migration assays were run for 8 h at 37°C in a 5% CO2 incubator, after which the medium was removed from the membrane tray and the tray was placed over a harvesting tray containing 150 μL of the cell detachment solution for 30 min at 37°C. The cells were treated with fluorescent dye and measured at 480/520 nm using a SpectraMax M2 Plate Reader (Molecular Devices).
In vitro chondrogenic differentiation of BMSCs in UPAL gel
Forty microliters of UPAL gel beads containing 1×106 BMSCs was placed into each well of 24-well culture dishes. The beads were then cultured in 1 mL of complete chondrogenic medium consisting of DMEM-HG supplemented with 100 μg/mL sodium pyruvate (ICN Biomedicals), 40 μg/mL proline (ICN Biomedicals), 50 μg/mL ascorbic acid-2-phosphate (Wako), 1×10−7 M dexamethasone (ICN Biomedicals), 1% ITS plus mix (Sigma-Aldrich), 1% antibiotics, and 10 ng/mL recombinant human transforming growth factor α3 (R&D Systems), dissolved in 4 mM HCl containing 1 mg/mL bovine serum albumin. The plates were maintained at 37°C in an incubator with the medium changed every 3 days. At 28 days after cultivation, each bead was washed with PBS and fixed with 4% phosphate-buffered paraformaldehyde for 24 h and embedded in paraffin. Then a 5-μm-thick section was cut from the center of the bead. This section was stained with H-E, and safranin-O using standard histochemical techniques. Immunohistochemical staining was performed with anti-type I and anti-type II collagen antibodies.
Data analysis
All data are presented as mean±standard error. Significant differences among three or more groups were assessed by one-way ANOVA followed by multiple-comparison post hoc tests. Comparisons between two groups were performed by unpaired t-tests. Statistical analyses were performed using GraphPad Prism (Version 5.00; GraphPad Software, Inc.). p-Values of less than 0.05 were considered statistically significant. To avoid observer bias, slides were coded before analysis.
Results
Release of SDF-1 protein from the UPAL bead
The release of SDF-1 protein from the UPAL bead to the culture medium was found from 2 to 14 days after cultivation (Fig. 1).

In vitro release kinetics of stromal cell-derived factor-1 (SDF-1) protein from the ultrapurified alginate (UPAL) bead.
Expression of SDF-1 protein after osteochondral injury
Immunohistochemical analysis revealed cells expressing SDF-1 protein in the injury site at 1 week after creation of the osteochondral defect (Fig. 2B, J), whereas the expression was not found at 3 h, 2 weeks, or 4 weeks after injury (Fig. 2A, C, D). After sham operation, no local expression of SDF-1 protein was observed at any time point (Fig. 2E–H). Western blot analysis showed enhanced expression of SDF-1 protein only in the tissue obtained at 1 week after injury, confirming the results of immunohistochemical analysis (Fig. 2Q).

SDF-1 protein expression in rabbit knee.
In vivo migratory effects of SDF-1 on host cells
At 1 week postoperatively, histological findings of the SDF-1 group showed more host cells in the rabbits with UPAL gel implanted into the osteochondral defect than in the other groups (Fig. 3A–F). The quantitative analysis demonstrated that the cell number was significantly higher in the SDF-1 group than in the other groups (n=5 in each group; p<0.01 vs. the vehicle group; p<0.001 vs. the AMD3100 group, Fig. 3G). Although the cell number of the vehicle group tended to increase compared with that of the AMD3100 group, there was no significant difference between the two groups. These results suggested that local administration of SDF-1 enhanced the migration of host cells to the site of the osteochondral defect.
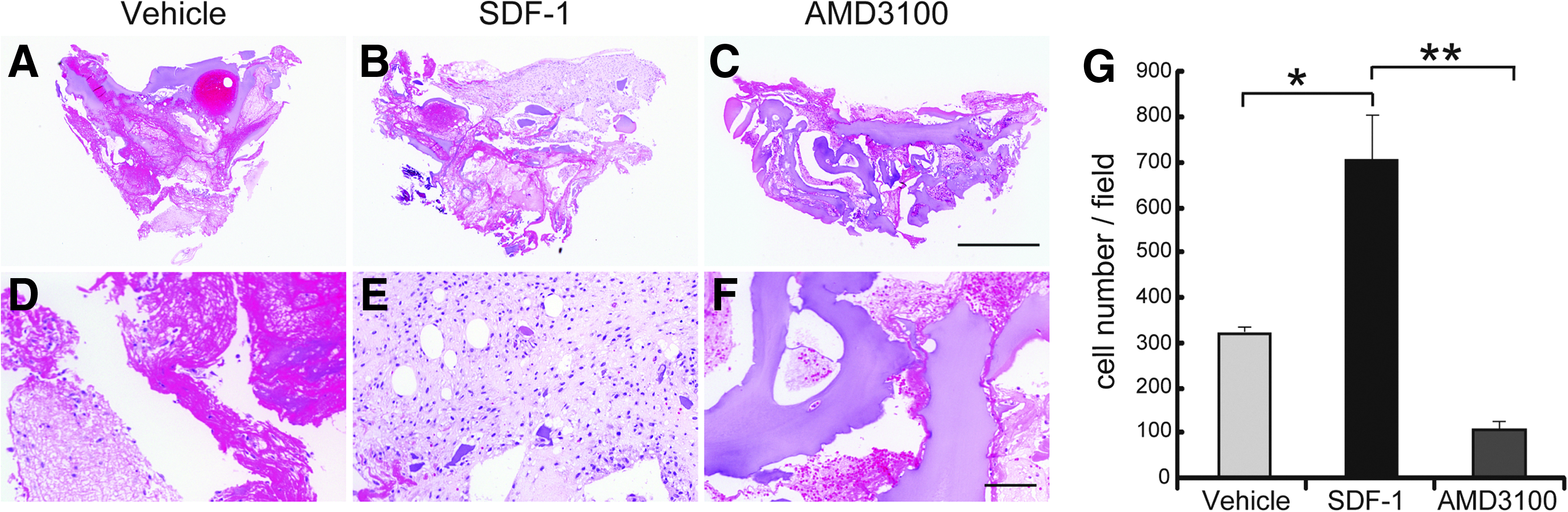
In vivo cell homing assay of the UPAL gel implanted into the osteochondral defect.
Macroscopic morphology
No macroscopic signs indicating infection such as pyogenic fluid or purulent synovitis were found in any knees at any time point. The implanted UPAL gel remained in the osteochondral defects of the patellar groove in the vehicle and AMD3100 groups at 4 weeks postoperatively (Fig. 4B, D). In the defect and AMD3100 groups, the surface of the reparative tissue was somewhat rough, slightly depressed, and poorly integrated with the adjacent cartilage even at 16 weeks postoperatively (Fig. 4A, D, E, H). On the other hand, the smoothness of the surface and the integration with the adjacent cartilage at 16 weeks postoperatively were improved in the vehicle and SDF-1 groups (Fig. 4F, G). The defects in the SDF-1 group at 4 weeks postoperatively were partially filled with firm, glossy white material (Fig. 4C). At 16 weeks postoperatively, the defects were entirely replaced with such cartilage-like tissue (Fig. 4G).
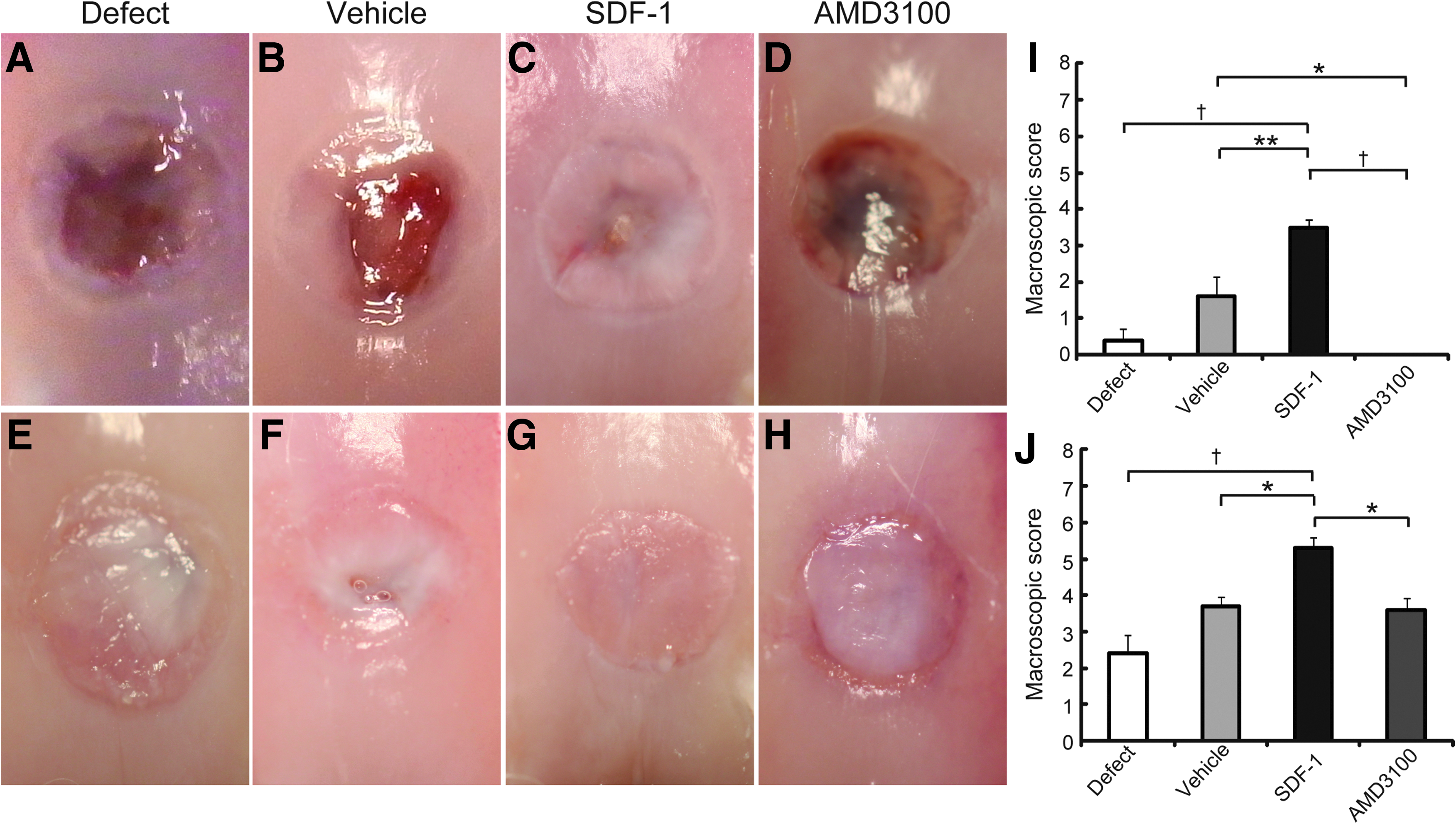
Macroscopic morphology of osteochondral defects at 4 weeks
Mean total macroscopic scores significantly improved from 4 to 16 weeks postoperatively in all groups (n=10 in each group at each time point; p<0.01 in the defect, vehicle, and SDF-1 groups; p<0.001 in the AMD3100 group; Fig. 4I, J). Regarding the comparisons among the groups, the total macroscopic scores at 4 weeks postoperatively were significantly higher in the SDF-1 group than in the other groups (p<0.001 vs. the defect and AMD3100 groups, p<0.01 vs. the vehicle group; Fig. 4I). The scores in the AMD3100 group significantly decreased compared with those in the vehicle group (p<0.05, Fig. 4I). The scores in the SDF-1 group at 16 weeks were also significantly higher than in the other groups (p<0.01 vs. the defect group, p<0.05 vs. the vehicle and AMD3100 groups; Fig. 4J). No other significant differences in the scores were found among the groups.
Histological and immunohistochemical findings
At 4 weeks after operation
The reparative tissue in the defect and AMD3100 groups was replaced with fibrillated fibrous tissues mainly containing type I collagen (Fig. 5A, D, E, H, I, L). On the other hand, the defect sites in the vehicle and SDF-1 groups were partially repaired with hyaline-like cartilaginous tissue containing GAG matrix and type II collagen (Fig. 5B, C, J, K). The reparative tissue in both groups partially included type I collagen (Fig. 5F, G). In the vehicle group, fissures were observed in the defect site (Fig. 5B). No reconstruction of normal subchondral bone structure, a smooth cartilage surface, or a complete tidemark was found in any group (Fig. 5A–D).
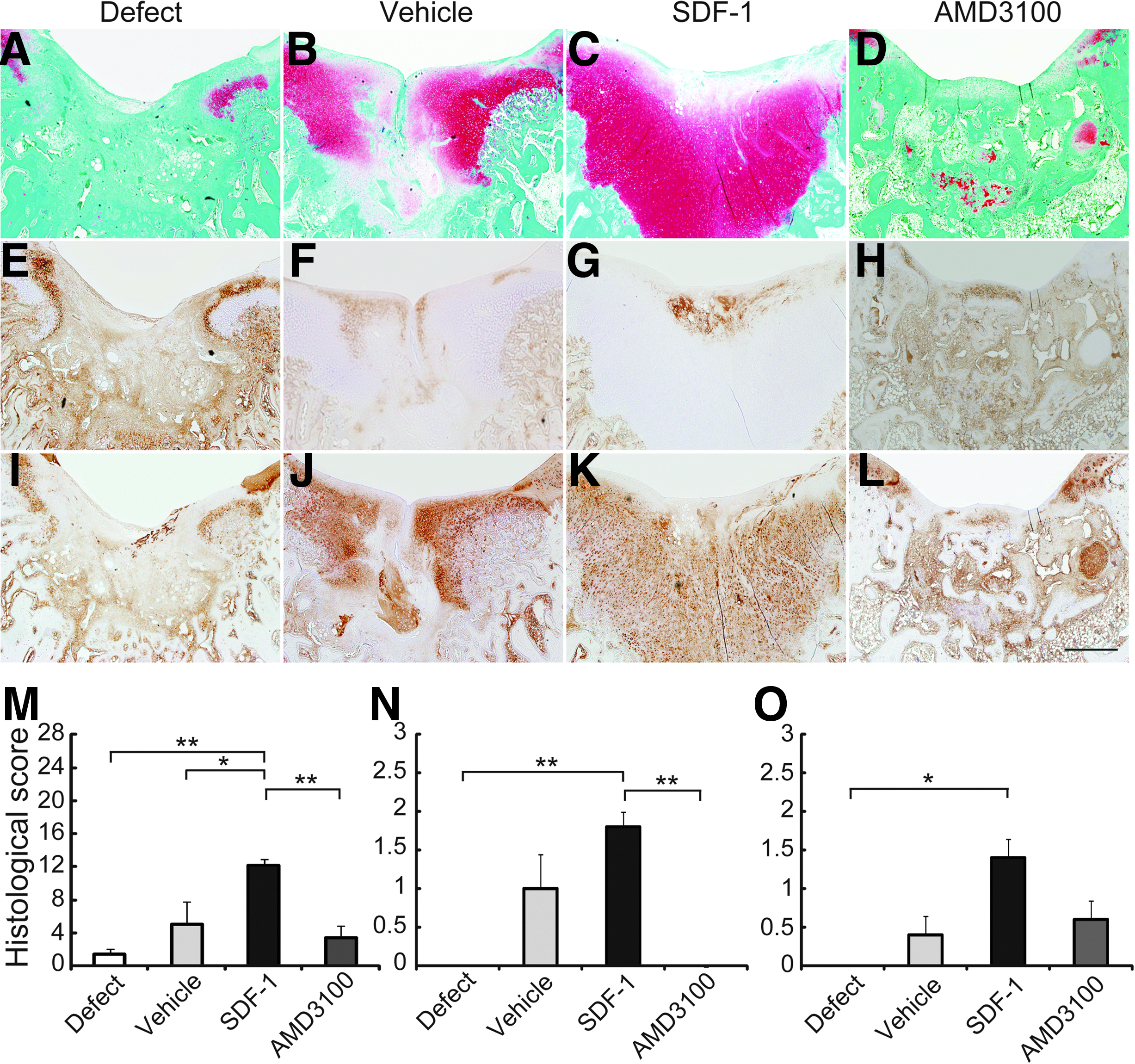
Histological sections of osteochodral defects at 4 weeks after operation. The sections were stained with safranin-O
Mean total histological scores in the SDF-1 group were significantly higher than those in the other groups (n=5 in each group, p<0.01 vs. the defect and AMD3100 groups, p<0.05 vs. the vehicle group; Fig. 5M). No significant differences in the values were found among the other three groups. The scores for GAG content were significantly higher in the SDF-1 group than in the defect and AMD3100 groups (n=5 in each group, p<0.001; Fig. 5N). The values for type II collagen content in the SDF-1 group significantly increased, compared with those in the defect group (n=5 in each group, p<0.01; Fig. 5O).
The reparative tissue in the defect demonstrated strong MMP-13 staining (Fig. 7A). On the other hand, the defect sites in the SDF-1 group showed no apparent MMP-13 staining (Fig. 7B).
At 16 weeks after operation
The defect group showed repair with only fibrous tissues and had some fissures and severely disrupted surfaces (Fig. 6A, E, I). The AMD3100 and vehicle groups demonstrated hypocellular fibrocartilagious repair with weak type I and type II collagen staining (Fig. 6B, D, F, H, J, L). The vehicle clearly enhanced the repair of subchondral bone in the defects (Fig. 6B) compared with the defect and AMD3100 groups (Fig. 6A, D). Fissures were observed at the border between the defect and adjacent cartilage in the AMD3100 group (Fig. 6D), whereas no such findings were observed in the vehicle group (Fig. 6B). On the other hand, the SDF-1 group exhibited nearly normal cartilaginous structures with rich GAG matrix content and strong type II collagen staining, reconstruction of the normal subchondral bone structure, a smooth cartilage surface, and a tidemark (Fig. 6C, K). Type I collagen staining was not found in the cartilaginous layer (Fig. 6G). The neocartilaginous reparative tissue was integrated into the adjacent cartilage and bone (Fig. 6C).

Histological sections of osteochodral defects at 16 weeks after operation. The sections were stained with safranin-O
The total histological scores in the vehicle and SDF-1 groups significantly improved from 4 to 16 weeks postoperatively (p<0.05 in the vehicle group, p<0.01 in the SDF-1 group; Figs. 5M and 6M). The scores at 16 weeks after operation were significantly higher in the SDF-1 group than in the other groups (n=5 in each group, p<0.001; Fig. 6M). The values in the vehicle group were significantly superior to those in the defect group (p<0.01, Fig. 6M). No significant differences in the scores were found between the defect group and AMD3100 group. The SDF-1 group significantly increased the scores for GAG content compared with those of other groups (n=5 in each group, p<0.001; Fig. 6N). The values for type II collagen content were significantly higher in the SDF-1 group than in other groups (n=5 in each group, p<0.001 in the defect and AMD3100 groups, p<0.01 in the vehicle group; Fig. 6O).
The MMP-13 staining in the SDF-1 group appeared to be reduced, compared with that in the defect group (Fig. 7B, D).

Local expression of MMP-13 protein in osteochondral defects at 4 and 16 weeks after operation.
Measurement of mechanical properties
At 4 weeks postoperatively, the compressive modulus in all groups was significantly lower than that of normal cartilage (n=5 in each group, p<0.001, Table 1). There were no significant differences in the value among the experimental groups. From 4 to 16 weeks, the moduli of all groups except the defect group significantly improved (p<0.001 in the SDF-1 group, p<0.01 in the vehicle and AMD3100 groups; Table 1). At 16 weeks postoperatively, the values in the vehicle and AMD3100 groups were significantly superior to that in the defect group (n=5 in each group, p<0.01; Table 1). In the SDF-1 group the modulus was significantly improved compared with the defect group (p<0.001, Table 1) and reached ∼81% of that of normal cartilage. Only the modulus in the SDF-1 group showed no significant difference compared with normal cartilage.
Mean±SEM.
p<0.001 vs. normal knee.
p<0.01 vs. defect at the same time.
p<0.001 vs. defect at the same time.
p<0.05 vs. normal knee.
SDF-1, stromal cell-derived factor-1.
In vitro effects of SDF-1 on BMSC behaviors
In the SDF-1 group in vitro BMSC migration significantly increased compared with the control group (n=16 in each group, p<0.01; Fig. 8A). The cell proliferation assay showed no significant difference at any time point among the experimental groups (n=5 in each group at each time point, Fig. 8B). Histological and immunohistochemical analyses demonstrated no apparent differences in chondrogenesis of BMSCs in UPAL gel beads among the groups (Fig. 8C–H). These results indicated that SDF-1 had no direct effects on cellular proliferation and chondrogenesis of BMSCs.
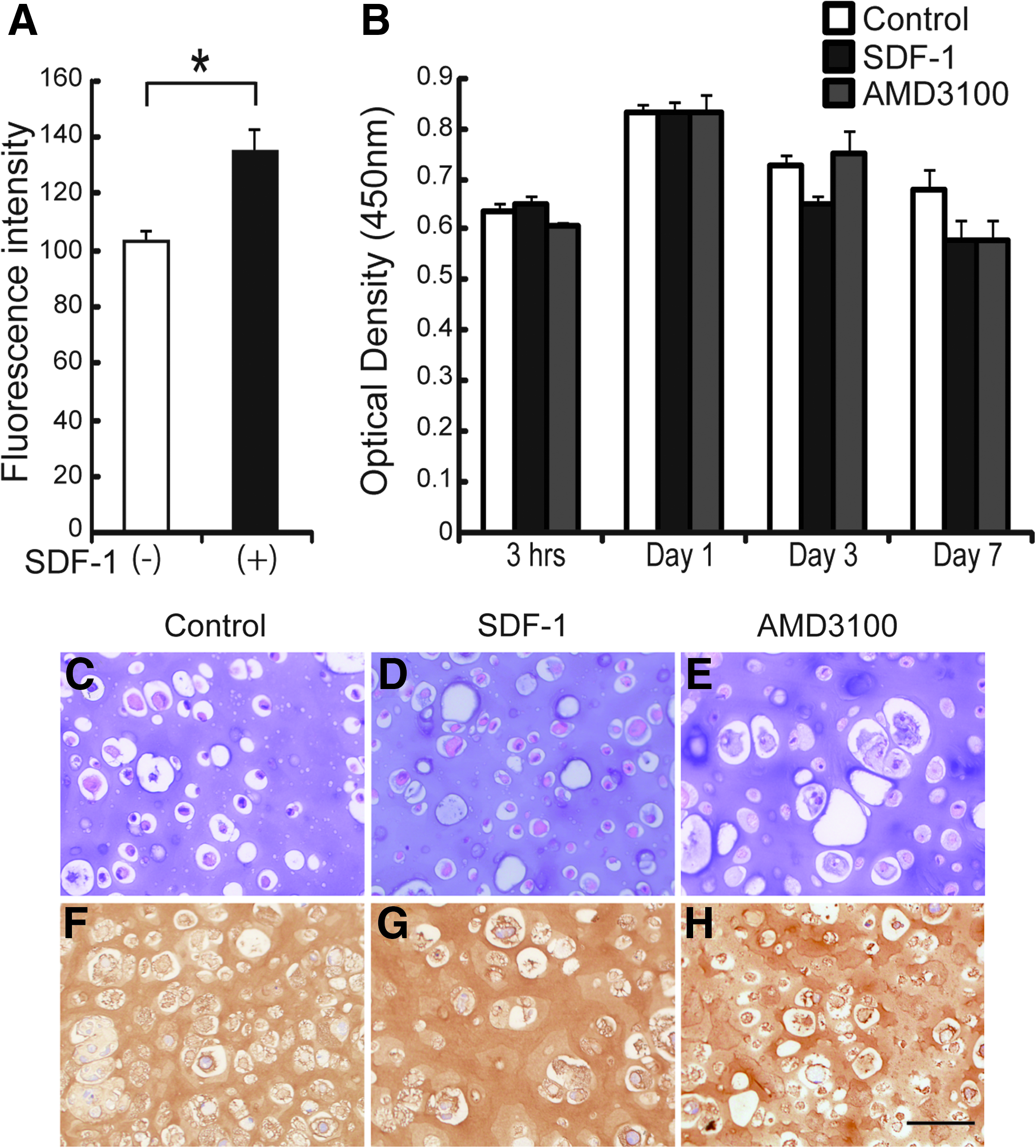
In vitro effects of SDF-1 on bone marrow stromal cell (BMSC) behaviors.
Discussion
Our aim was to determine whether the local administration of SDF-1 using UPAL gel could enhance repair of osteochondral defects in rabbits. The results showed that the SDF-1 treatment (UPAL gel containing SDF-1) significantly improved the histological scores and compressive modulus of reparative tissues compared to other experimental groups, including the vehicle (UPAL gel without SDF-1) group. Regarding an adverse effect of SDF-1 administration, immunohistochemical findings suggested that SDF-1 did not stimulate the expression of MMP-13 in reparative tissues. Therefore, we reasonably concluded that the injection of SDF-1 embedded in the UPAL gel histologically and biomechanically enhanced the reparative process of osteochondral defects.
The assessment of extracellular matrix content, including type II and GAG, in reparative tissues is important to determine the repair with hyaline-like cartilage after the treatment of osteochondral defects. Real-time PCR analyses by Kim et al. 36 showed the upregulated expressions of Type II collagen and aggrecan in rabbit reparative tissues at 8 and 16 weeks after chondrocyte implantation delivered by a heparine-based hydrogel. On the other hand, Hoeman et al. 37 showed that sheep repair tissue at 24 weeks after acellular treatment using chitosan-glycerol phosphate/blood implantation contained nearly twofold more GAG and collagen compared with that from control defects treated with microfracture alone. In our study, the SDF-1 group significantly increased the scores for GAG and type II collagen contents compared with the control defect group at 4 and 16 weeks postoperatively. The studies by Hoeman et al. 37 and the authors demonstrate a potential of hyaline-like tissue repair for cartilaginous lesions by acellular treatment strategies.
The authors, 26 using a rat model, demonstrated that the local expression of SDF-1 was temporarily upregulated, peaking at 2 weeks after medial collateral ligament injury. Kitaori et al. 27 detected high expression of SDF-1 protein in the periosteum of the graft bone on day 2 during the healing of bone grafts in mice. Misao et al. 38 showed upregulation of SDF-1 expression in rabbit myocardial tissues at 7 days after the occurrence of myocardial infarction. On the other hand, Shen et al. 39 reported that the expression of SDF-1 was upregulated until 4 months after a stroke. Regarding the timing of SDF-1 upregulation, the inconsistencies among these tissues and organs may be attributable to differences in cellularity. Cellular and tissue responses to acute cartilage injury are generally classified into three phases as follows: (1) the early phase is characterized by cell death/apoptosis and inflammation (0–6 days after injury); (2) the intermediate phase follows, when a potential balance between catabolic and anabolic responses may exist (6–8 days after injury); and (3) the late phase with repair/remodeling/matrix formation (8–14 days after injury). 40 The current study showed that the transient expression of SDF-1 protein around the injury site occurred at 1 week after surgery. In addition, the local administration of AMD3100, an antagonist of CXCR4, impaired the repair of osteochondral defects. Taken together, these results indicated that SDF-1 played a crucial role in repairing osteochondral defects during the intermediate phase of the reparative process, when anabolic responses are initiated.
The injury created here involves disruption of the articular cartilage with penetration into the subchondral bone. The reparative process of this injury includes formation of a fibrin clot and recruitment of undifferentiated mesenchymal cells into the clot. Then the recruited cells produce reparative tissue that mainly consists of fibrocartilaginous tissue, not hyaline cartilage. To achieve hyaline-like cartilage repair, a reasonable approach is to enhance cellular and/or tissue activities in each reparative phase. Regarding the recruitment of host cells, in the SDF-1 treatment group the number of cells that migrated into the defect site significantly increased at 1 week postoperatively compared with other treatment groups. Our in vitro cell migration assay also showed that SDF-1 significantly increased the migration of BMSCs, supporting the in vivo findings. These results indicated that the chemotactic effect of SDF-1 enhanced the migration of host cells, mainly including BMSCs, to osteochondral defects.
Our previous study demonstrated that UPAL gels clearly enhanced in vitro chondrogenesis of BMSCs. 22 In the current study, the UPAL gel containing SDF-1 beads did not notably improve the proliferation and chondrogenesis of BMSCs in UPAL gel-alone beads. This suggested that there was no direct effect of SDF-1 on chondrogenesis of BMSCs. The authors showed that SDF-1 had no direct effects on cellular behavior of BMSCs in terms of the proliferation, adhesivity, and differentiation to ligament fibroblasts. 26 Jung et al. 41 also reported that SDF-1 had no significant effect on the proliferation of fibroblasts. These previous studies support the current results. Collectively, the results obtained here indicated that SDF-1 influenced the reparative process of osteochondral injuries not through direct effects on the behaviors of host cells, mainly BMSCs, but by increasing their homing rate to the injury site. Regarding cellular differentiation, the implanted UPAL gel may play a crucial role in the chondrogenesis of the recruited host cells. We speculate that these biological effects of both SDF-1 and UPAL gel on the tissue reparative process enhance cartilage tissue repair in the living joint.
Tissue engineering fundamentally combines isolated cells with scaffolds to regenerate damaged tissues. The primary advantage of cartilage tissue engineering and ACI is the development of hyaline-like cartilage rather than fibrocartilage in osteochondral defects. This presumably leads to better long-term clinical outcomes. However, the standard procedure currently performed has considerable limitations. It requires at least two operations, one for tissue harvesting to isolate chondrocytes and the other for chondrocyte implantation. Further, the standard procedure is performed through a wide arthrotomy and has risks of complications related to the periosteal graft such as periosteal hypertrophy,6,19 falling off of the graft site, 42 or intra-articular adhesion. Cell-free approaches like the implantation of naturally occurring or synthetic scaffolds into the defects are based on complementing basic biological repair strategies such as marrow-stimulation techniques and ACI. The procedures can minimize complications by avoiding the harvesting and implantation of cells and of periosteum, and prevent dedifferentiation of isolated chondrocytes during cultivation. In addition, the cell-free approaches make an arthroscopic implantation technique feasible for accessible lesions. A multicenter study of the clinical outcomes after ACI demonstrated that 26% of the procedure-related complications were associated with the open arthrotomy. 6 Cell-free approaches can combine the ability to improve clinical outcomes of cartilage tissue engineering and efficacy in a cost-effective manner by minimizing the adverse effects of the procedures currently performed.
There have been two main cell-free approaches for cartilage tissue engineering. One is to develop a three-dimensional scaffold for implantation,43–45 and the other is to locally apply growth factors, cytokines, or a combination of these proteins.46–48 However, the former strategy has a limitation in the number of cells recruited to the injury site, and with the latter one, a loss of protein activity tends to occur immediately after implantation. These considerations prompted us to develop a novel acellular approach. Our previous study 22 demonstrated that the UPAL gel was completely reabsorbed between 2 and 4 weeks after implantation in living joints. Rabbany et al. 49 reported that alginate patches prolonged the in vivo retention of SDF-1 protein over 2 weeks after surgery. Because heparin and spermine introduced into the alginate material can bind to SDF-1, this protein binds to the material and consequently achieves prolonged in vivo retention in a biologically active form. Our in vitro assessment regarding release kinetics of SDF-1 protein from UPAL gel supports their results.
There are further considerations for the clinical application of our results. First, our evaluation of this treatment strategy was based on the results derived from a rabbit model. Second, in vivo analyses were performed using samples at 4 and 16 weeks postoperatively. Long-term assessments using a large animal model need to be performed to adapt our approach for use in humans.
In conclusion, we succeeded in achieving hyaline-like cartilage repair by local administration of SDF-1 using UPAL gel without cells. The obtained results indicate that UPAL gel enhances chondrogenesis of BMSCs recruited by the chemotactic effect of SDF-1, leading to a novel cell-free approach for cartilage tissue engineering.
Footnotes
Acknowledgments
This study was supported by a Grant-in-Aid for Scientific Research from Japan Society for the Promotion of Science (B-22390285), and “Development of a Novel Injectable Material for the Treatment of Joint Disorders” Science and Technology Incubation Program in Advanced Regions, Japan Science and Technology Agency.
Disclosure Statement
No competing financial interest exists.