
Abstract
In this study, we investigated the efficacy of the transplantation of autologous articular chondrocytes seeded onto a hyaluronan-based scaffold, known as Hyaff®-11, on the treatment of early cartilage lesions in a rabbit osteoarthritis (OA) model. The hypothesis of the study was that this treatment could enhance cartilage repair after OA induction. OA was surgically induced by Anterior Cruciate Ligament Transection (ACLT) in thirty rabbits. Animals were divided into three groups, according to treatment: group 1: ACLT; group 2: Chondrocytes+Hyaff-11; and group 3: Hyaff-11 alone. The animals were euthanized, respectively, at 3 and 6 months after the treatment. Histomorphometrical analyses were performed by means of fibrillation index, cartilage thickness, and subchondral bone thickness evaluations. Histological appearance was scored according to Modified Kraus' Mankin and Osteoarthritis Research Society International (OARSI) scores. Immunohistochemical analyses were carried out for type I and II collagens, MMP-1, and MMP-3. A comparison between groups and follow-up for each outcome was performed with the general linear model with Sidak correction. Histomorphometrical evaluations at 3 and 6 months demonstrated that OA lesions became significantly worse followed by Hyaff-11 treatment, whereas Chondrocytes+Hyaff-11 treatment had the best overall subjective grade. Overall raw histological scores demonstrated a significant improvement with chondro-hyaluronic acid (HA) treatment at 3 months compared with HA in cartilage repair processes. Immunohistochemical analyses displayed a strong positivity for type II collagen in the Chondrocytes+Hyaff-11group at 3 months compared with the HA group. No staining was observed in MMP-3 expression in this group at any experimental point. The use of Chondrocytes+Hyaff-11 for the treatment of early OA lesions produced, already at 3 months, a repair tissue showing better macroscopic, histological, and immunohistochemical results than those observed after Hyaff-11 treatment. Thus, the transplantation of Chondrocytes+Hyaff-11 would seem to be advocated in the very early stage of the OA disease when a precocious action is mandatory.
Introduction
Despite the high prevalence and morbidity of OA, an effective treatment for this disease is currently lacking. Although OA involves the whole joint, cartilage degradation represents the hallmark of the progression and irreversibility of the disease. Restoration of the diseased articular cartilage in patients with OA is, therefore, a challenge of considerable appeal to researchers and clinicians. Cell therapy could provide a permanent, biological solution for the treatment of OA disease. However, the ideal cell candidate and the more suitable scaffold that is used to treat degenerative lesions remains a major challenge. 19 We previously demonstrated that a hyaluronan-based scaffold (Hyaff®-11) (Fidia Advanced Biopolymers/Anika Therapeutics) represents a good biomaterial that is able to allow human chondrocytes re-differentiation,20–22 down-regulate some catabolic factors,23,24 contributing to the regeneration of damaged cartilage in vivo. 25
In our previous work, it was shown that 8 weeks after anterior cruciate ligament transection (ACLT), needed to OA development in an experimental rabbit model, 26 the transplantation of mesenchymal stem cells (MSCs) grown onto Hyaff-11 was efficient in regenerating articular cartilage matrix, particularly at 6 months from the treatment. 27
In the light of these findings, we decided to perform another preclinical study by defining whether the delivery of autologous articular chondrocytes (AC) seeded onto Hyaff-11 is able to enhance the repair of cartilage tissue and decrease the evolution of OA process at an earlier stage compared with the MSC treatment. Mature AC show phenotypical features and secrete a broad spectrum of growth factors that could render them suitable for transplantation.28–30 The results obtainable with chondrocytes instead of MSCs should yield comparative evidence on the use of the two different cell sources in OA treatment and particularly in different OA stages.
To this end, we treated early degenerative cartilage lesions with Hyaff-11 scaffold carrying autologous AC. Animals were euthanized at 3 and 6 months after the treatments, and cartilage tissues obtained from the rabbit condyles were evaluated by performing morphological, histomorphometrical, histological, and immunohistochemical analyses.
Materials and Methods
Scaffold
Hyaff-11 polymer is derived from the total esterification of sodium hyaluronate (80–200 kDa) with the benzyl alcohol on the free carboxyl groups of glucuronic acid along the polymeric chain, leading to an increase in the hydrophobic component of the polymer chain, residence time in vivo, and resistance to hyaluronidase. 31 The material was sterilized by γ-irradiation. As a consequence of the degradation process, the material becomes progressively hydrophilic and hydrated, showing similarity to the soluble native HA polymer with time. In artificial plasma at 37°C, nearly complete hydrolysis of the ester bonds occurs in about 2 months. 32 Studies performed in vivo in rats on the biodegradation of Hyaff®-11 have shown that the material disappears after about 4 months after implantation 33 and in rabbit osteochondral defects, in less than 3 months. 34
Animal experimental design
Animal experimental protocol has been approved by the Ethics and Scientific Committees of Rizzoli Orthopaedic Institute and by the other public Authorities as requested by Italian Law according to EC rules (Law by Decree, 27 January, 1992 n. 116). Thirty healthy, male, adult New Zealand White rabbits (sex: ♂, age: 12 months old, BW: 4.0±0.5 kg) were used in the study. Experimental OA was induced via ACLT procedure35,36 in one knee of one hind limb; in the controlateral knee, a sample of healthy cartilage was harvested to isolate AC 4 weeks from ACLT. An antibiotic (Flumequine, ATI s.r.l.; Ozzano Emilia) and analgesic (Ketoprofene; Rhone-Poulenc-Rorer) therapy was administered immediately after surgery and for 2 days thereafter. Postoperatively, the animals were permitted cage activity without immobilization.
Thirty animals were distributed among different groups as described in Figure 1 and given next:
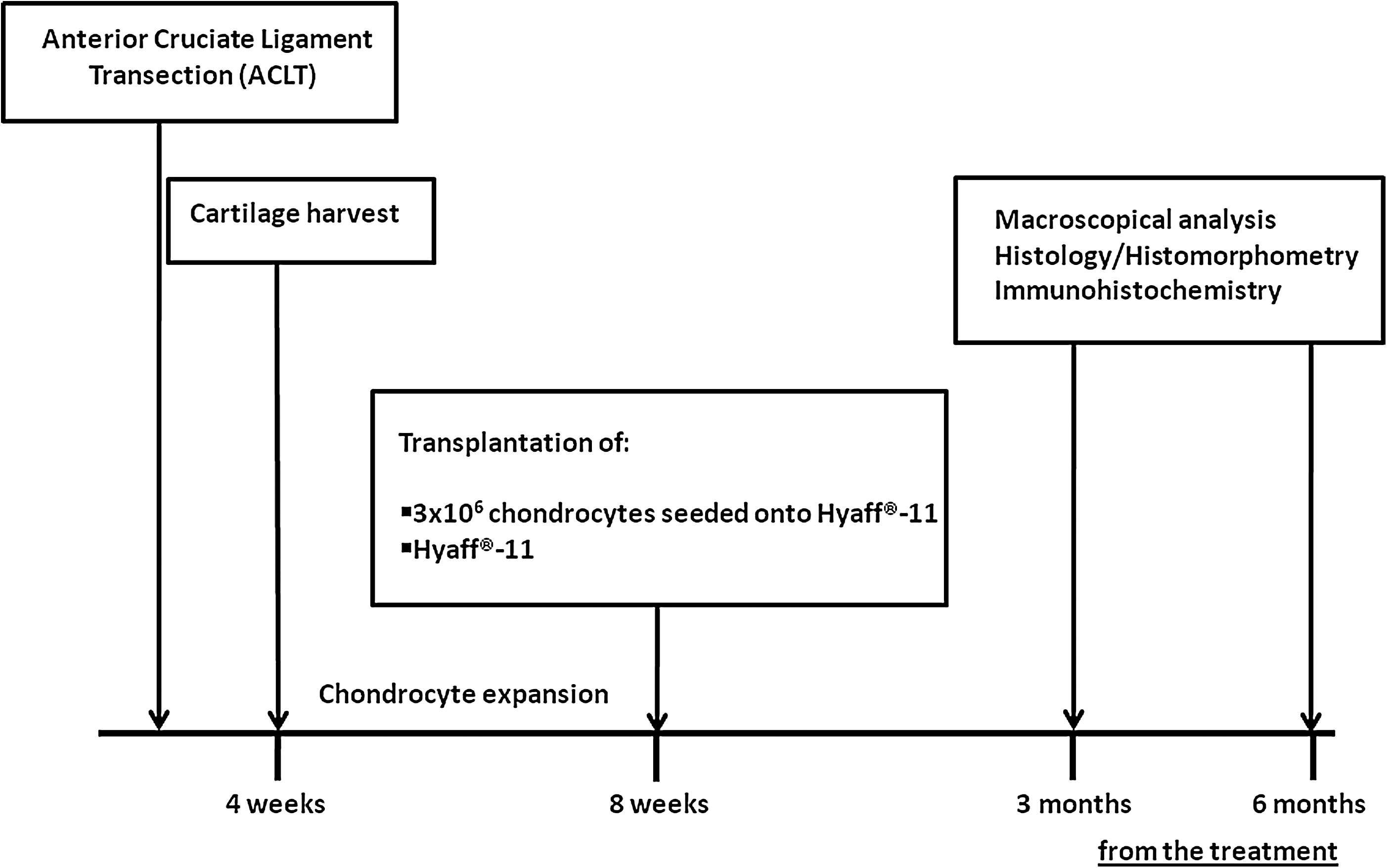
Schematic representation of animal experimental design.
Group I: OA group (six animals)
Articular cartilage of both distal femoral epiphyses submitted to ACLT to induce OA. Two out of the six animals were euthanized at 8 weeks to evaluate the development of OA lesions; the remaining were euthanized at 3 and 6 months from ACLT, respectively, to evaluate the spontaneous repair process.
Group II: (Chondro-HA group) (12 animals)
After 8 weeks from ACLT, articular joints were treated with Hyaff®-11 seeded with 3×106 autologous chondrocytes. These animals were euthanized, respectively, at 3 (six animals) and 6 months (six animals).
Group III: (HA group) (12 animals)
After 8 weeks from ACLT, articular joint was treated with Hyaff®-11. These 12 animals were, respectively, euthanized at 3 (six animals) and 6 months (six animals) from the treatment.
All the animals were euthanized under general anaesthesia by means of an intravenous lethal injection of Tanax (Hoechst Veterinar GmbH). Femoral condyles were explanted and used to perform macroscopic, histo-morphometrical, histological, and immunohistochemical evaluations.
Chondrocyte isolation and culture
Healthy cartilage from femoral condyles was harvested from the rabbit condyles after four weeks from ACLT. AC were isolated by an enzymatic digestion, as previously reported. 24 Briefly, under aseptic conditions, about 0.2 g of cartilage slices were minced and sequentially incubated at 37°C with hyaluronidase (Sigma Chemical Corp.), pronase (Sigma), and collagenase (Sigma) in Dulbecco's Modified Eagle medium (DMEM; Sigma) without Foetal Bovine serum (FBS; Sigma). We obtained about 2×106 cells/g cartilage. Cell number and viability were assessed by eosin. Cells were cultured in DMEM with 10% FBS and maintained at 37°C in a humidified atmosphere and 5% CO2. The cells were first expanded in monolayer cultures for two passages (P2), and then, 3×106 AC/300 μL of the medium (1×107 cells/mL) were passively seeded onto 1.5×1.5 cm2 Hyaff-11 meshes. The constructs were maintained in culture for 9 days to restore chondrocyte phenotype, 20 before the implantation. Collagen I/Collagen II ratio was, respectively, 3 in the matrix synthesized by chondrocytes expanded in the monolayer and 0.3 in those seeded onto Hyaff-11 before the transplantation. Un-seeded Hyaff-11 meshes were prepared just before the transplantation.
Autologous grafting procedure
At 8 weeks, necessary to OA development, knee joints from groups II and III were again opened, patellae were laterally luxated in order to expose the femoral condyles, and Hyaff®-11 meshes un-seeded and seeded with chondrocytes were inserted without any fixation due to their intrinsic adhesive properties.25,27
The implants roughly covered all the articular surface to be reasonably sure that all the injured areas were treated. The patella was repositioned, and the capsule was repaired with 4-0 vicryl broken sutures by checking the grafting position. Finally, the subcutaneous tissues and skin were closed with a broken 5-0 nylon suture.
OA development assessment
A macroscopical assessment from animals of the OA group was performed by India Ink staining (Higgings Waterproof Drawing Ink; Sanford Co.) to assess the OA lesions on femoral condyles. 35 Using a small paintbrush, the India Ink solution was allowed to set for 2 min, and the excess was washed off with a quick rinse of sterile water. Condyles were photographed with a digital camera for analysis.
Cartilage histological assessment and histomorphometrical analyses
Histological and histo-morphometrical analyses were performed on medial femoral condyles from untreated and treated animals. Specimens were fixed in para-formaldheyde 4%, cut into four pieces, and methacrylate embedded. Toluidine Blue/Fast Green (Sigma-Aldrich) and Safranin-O/Fast Green (Sigma) stainings were carried out to perform cartilage histological assessment, as previously reported. 27 To this end, two different semi-quantitative scoring systems were used: Kraus' Modified Mankin36,37 and OARSI 38 scores. Kraus' Modified Mankin score represents the sum of five parameters: articular cartilage structure, Toluidine blue staining, cellularity, osteophyte presence, and tidemark integrity. It has a maximum score of 21 points and a minimum of 0 that translates to a completely normal cartilage. The OARSI score is an index of combined OA grade and OA stage (score=grade×stage), giving a picture of OA severity and extent; it has a maximum score of 24 points and a minimum of 0 that translates to a completely normal cartilage.
Furthermore, a quantitative evaluation of cartilage surface fibrillation index (FI), 39 cartilage thickness (CT), 39 and subchondral bone thickness (SBT) 40 were carried out. Three sagittal sections of severe grade were evaluated and read blindly by two experienced researchers.
All the evaluations were performed with image analysis Kontron KS300 software (Kontron Electronics).
Immunohistochemical evaluations
Immunohistochemical evaluations for type I and II collagens, MMP-1, and MMP-3 were carried out on femoral condyles treated as previously reported. 26 Medial femoral condyles were sectioned in the sagittal plane, perpendicular to the bone.
Sections for type I and II collagens were pretreated with 0.1% pronase (Sigma) in Trizma Base saline (TBS) for 15 min at 37°C. After appropriate blocking steps, the sections were left to react at room temperature (RT) for 1 h with polyclonal mouse anti- type I collagen (Sigma) diluted 1:250 and mouse anti-type II collagen (II-II6B3, Hybridoma Bank, University of Iowa, USA) diluted 1:200 in TBS, washed, and incubated with biotinylated goat anti-mouse and rabbit IgG (H+L) secondary antibody (BioGenex) for 20 min at RT. Then, the samples were treated with a phosphatase-labeled streptavidin (Biogenex) for 20 min at RT, and after washing, the reactions were developed using Fast red substrate (Biogenex). Sections for MMP-1 and -3 were pretreated with peroxidase blocking. The slides were then left to incubate with monoclonal mouse anti-human/rabbit MMP-1 (Chemicon) diluted 1:50 and monoclonal mouse anti-rabbit MMP-3 (Chemicon) diluted 1:50 in TBS followed by incubation with anti-Mouse poly HRP (Anti-Mouse Poly HRP IHC detection Kit; Chemicon). The sections were developed with HRP Kit, biotin-free (Anti-Mouse Poly HRP IHC detection Kit; Chemicon). Negative controls were performed by either omitting the primary antibody (for all the antibodies tested) or using an isotype-matched control. Slides were counterstained with hematoxylin (Gill 3; Bioptica) and mounted with Aquatex®. A semi-quantitative scoring method that assigns immunohistochemistry scores as a percentage of positive cells (the number of positive cells over the total number of cells) has been provided for a complete assessment of protein expression. The scoring analysis was performed by two blinded investigators by using Red/Green/Blue and Hue Saturation Intensity with Software NIS-Elements.
Statistical analysis
Statistical analysis was carried out using the Statistical Package for the Social Sciences (SPSS) software version 15.0 (SPSS, Inc.). All continuous data were expressed in terms of the 95% confidence intervals of the mean. The general linear model with Sidak correction for multiple comparisons was performed to assess the influence of follow-up and the kind of treatment on the different parameters evaluated, such as Kraus' Modified Mankin and OARSI scores, CT, FI, and SBT. Significance was set up at p<0.05.
Results
OA development assessment
The OA group developed varying degrees of OA features. Cartilage degenerative changes were seen particularly in the medial femoral condyle at 6 months. Since the pathology in the rabbit OA model occur particularly in the medial compartment, as observed by India Ink staining (Fig. 2), all the evaluations were performed in the medial femoral condyle.
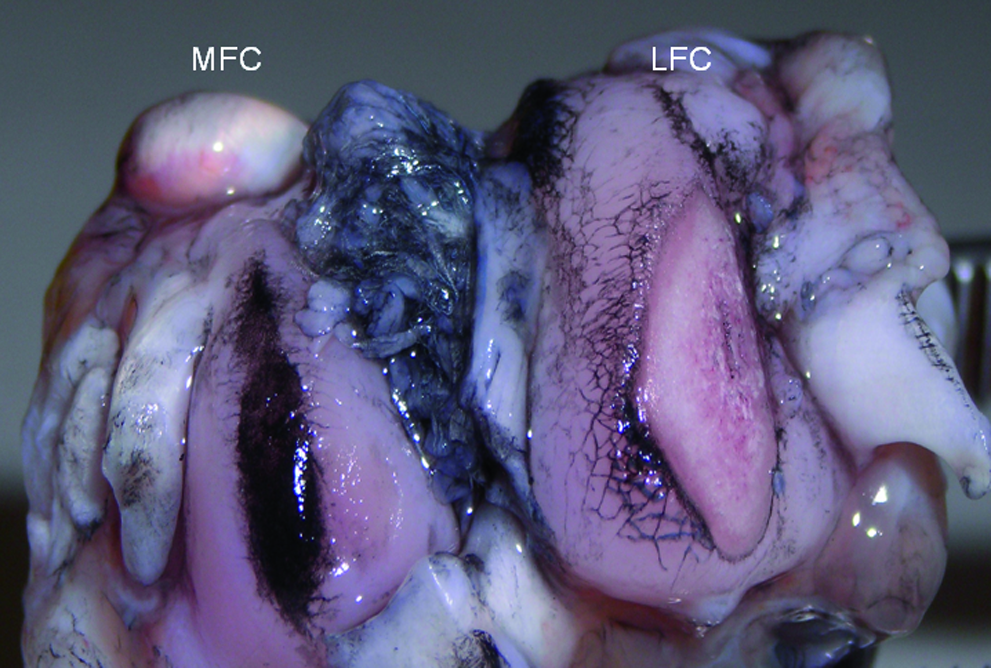
Macroscopic features of India Ink-stained femoral condyles in the rabbit osteoarthritis (OA) model at 8 weeks. Cartilage lesions are more evident in the medial femoral condyle (MFC) than in the lateral femoral condyle (LFC). Color images available online at www.liebertonline.com/tea
Cartilage histological assessment and histomorphometrical analyses
Based on visual assessment of histological staining, cartilage degenerative changes were characterized by chondrocyte and proteoglycan loss; fibrillation and cartilage delamination processes were developed progressively from ACLT surgery (Fig. 3a–d).
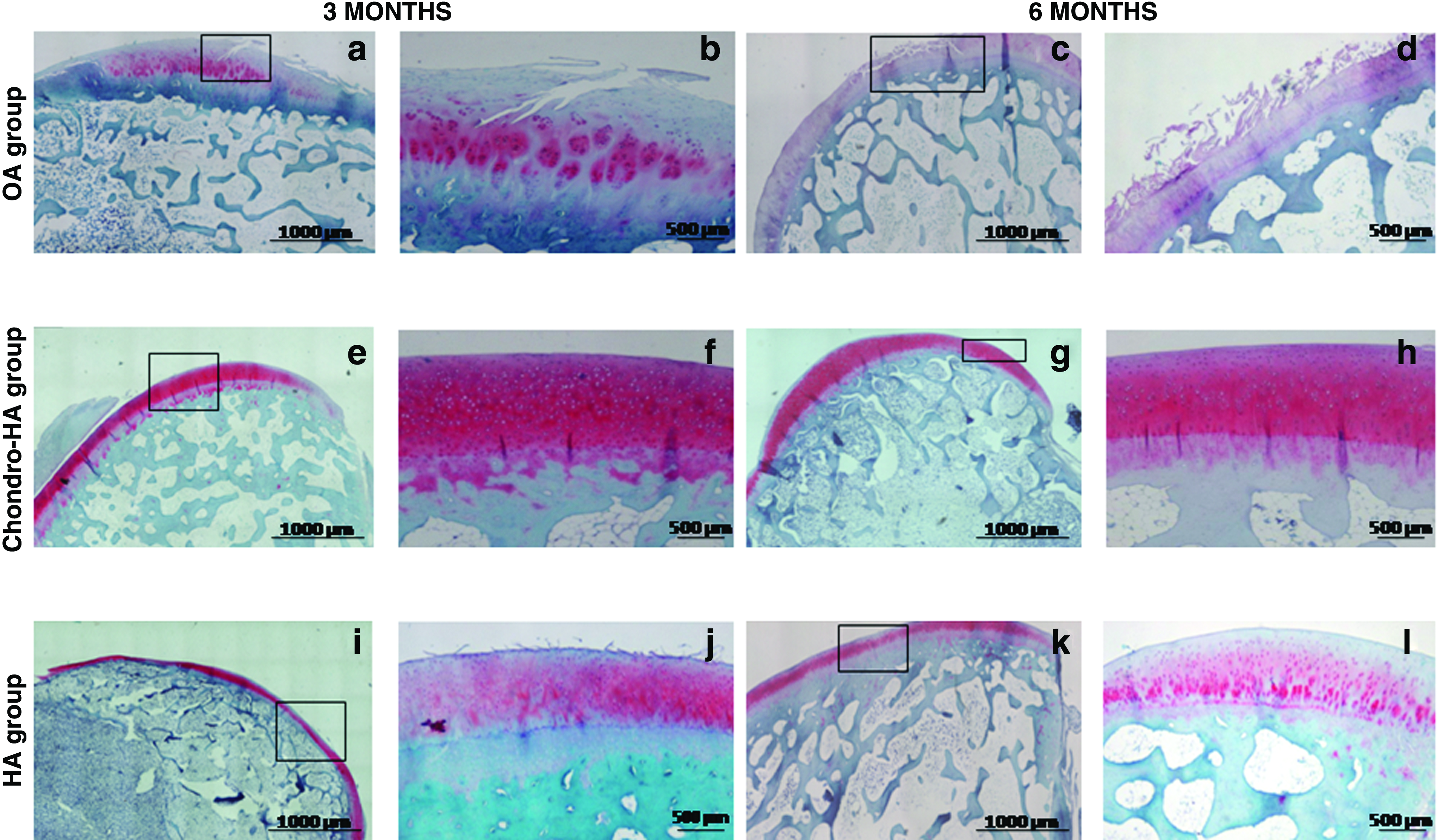
Histological analyses at 3 and 6 months of OA, Chondro-hyaluronic acid (HA), and HA groups. Sections were stained with Safranin-O for articular cartilage matrix proteoglycan assessment and Fast Green for bone and fibrous tissue presence. Sagittal sections from OA group at 3
The chondro-HA group showed cartilage tissue with some hyaline features with a linear arrangement of chondrocytes extending from the subchondral bone toward the surface and a high proteoglycan content already from 3 months (Fig. 3e–h).
The implant of HA in OA knee joints regenerated a tissue in the presence of fibrillation processes and a low content of proteoglycan, particularly in the anterior and posterior areas of the medial femoral condyles than in the condro-HA group just described (Fig. 3i–l).
The impact of chondro-HA and HA treatments on OA knees was estimated by using the histopathological Kraus' Modified Mankin and OARSI scores. Knee joints treated with chondro-HA showed values significantly lower for the Kraus' Modified Mankin score than the OA and HA groups at 3 months from the treatment (p<0.0005); no significant differences were observed at 6 months in the Chondro-HA group (Fig. 4a). The chondro-HA group had values lower for the OARSI score than the OA and HA groups (p<0.0005), particularly at three months; no significant differences were observed in the chondro-HA group at 6 months (Fig. 4b). FI was significantly lower in the chondro-HA and HA groups compared with the OA group at three months (p<0.0005). (Fig. 4d). CT measurements for the OA group decreased at 3 and 6 months form ACLT, while they increased in the chondro-HA and HA groups at 3 and 6 months (Fig. 4c). No significant differences were observed for SBT among the different treated groups at both 3 and 6 months (data not shown).
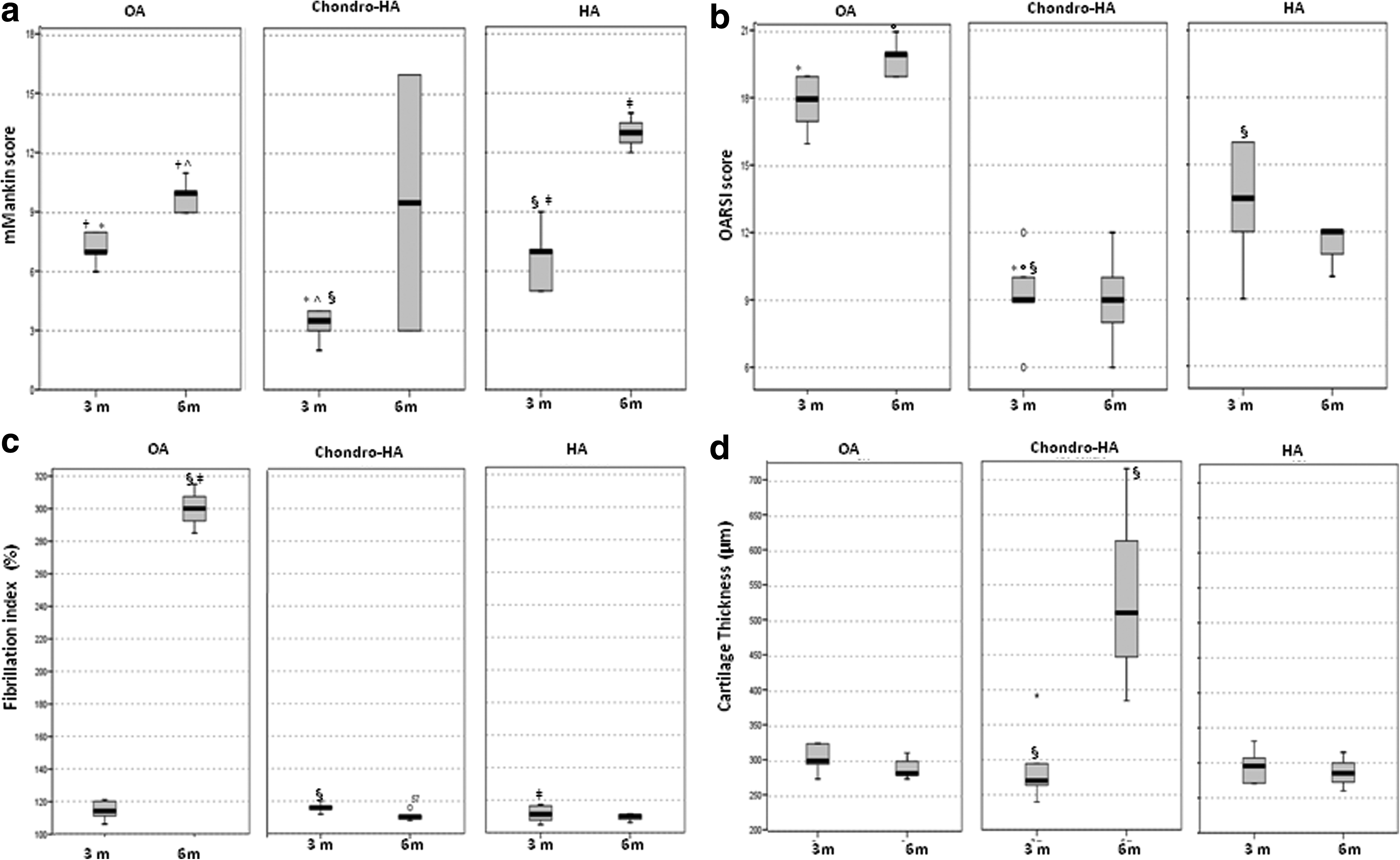
Data are reported in terms of the 95% confidence interval of the mean. The General linear Model with Sidak correction for multiple comparisons was performed to assess the influence of follow-up and treatment for different parameters: mMankin and Osteoarthritis Research Society International (OARSI) scores, fibrillation index (FI), and cartilage thickness (CT). Kraus' Modified Mankin score of OA, chondro-HA and HA groups
Immunohistochemical evaluations
At 8 weeks from ACLT (data not shown), the OA group showed moderate positive cells (80%) for type I collagen in all cartilage zones throughout all regions of cartilage. This positivity continued to increase progressively by 3–6 months (90%–100%) postsurgery.
In comparison, type I collagen expression in the chondro-HA group at the same two time points (3 and 6 months) showed negative staining (Fig. 5c, d). By contrast, type I collagen staining in the HA-group showed moderate positive cells (80%), particularly at 3 months (Fig. 5e), whereas a few positive cells were observed particularly in the middle and deep zones of the central regions of the femur at 6 months (Fig. 5f).
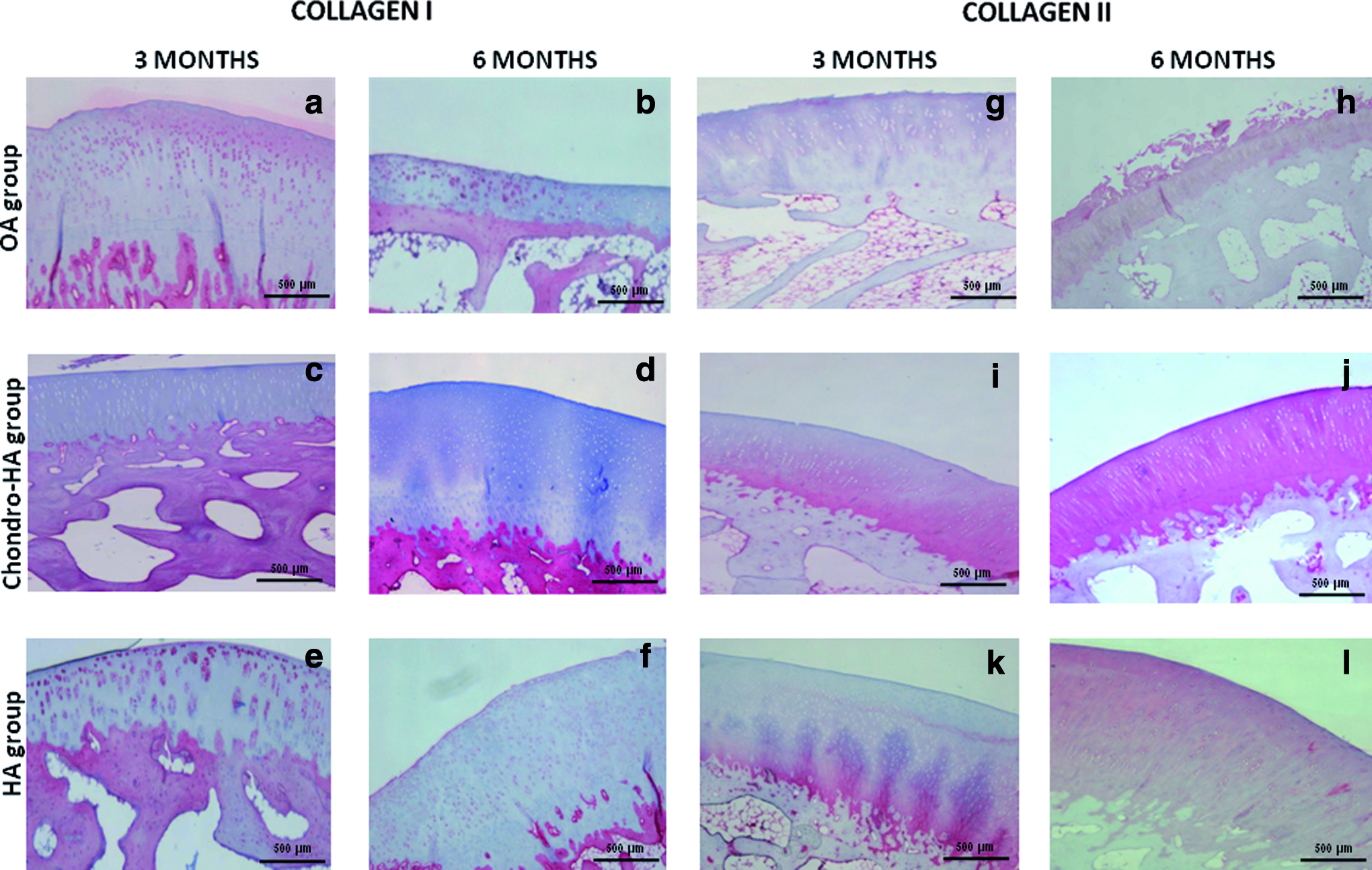
Immunostainings for type I collagen performed in articular cartilage sections from OA, chondro-HA, and HA groups. The reaction was developed using Fast Red chromogen. A strong positivity for collagen type I at the cellular level was found for the OA group at 3 and 6 months (
Type II collagen immunostaining was slightly positive at matrix level 8 weeks from ACLT (data not shown) (10%), became negative at 3 and 6 months in the OA group (Fig. 5g, h). Starting at 3 months of follow-up, positive immunostaining for the chondro-HA group (40%) was detected in the matrix of articular cartilage (Fig. 5i). Marked positive staining intensity for chondro-HA (100%) was observed in the matrix at 6 months from the treatment (Fig. 5j). By contrast, in the HA group, a slight staining for type II collagen located in the deep zone of the articular cartilage was observed (25%) (Fig. 5k). A marked positivity (60%) was always observed at the matrix level at 6 months (Fig. 5l). The collagen I/II ratio was used as a “differentiation index” to evaluate the quality of the repaired cartilaginous tissue. The expression of type II collagen increased 100-fold in the group treated with HA-chondro and 50-fold in that treated with only HA compared with the OA group. Instead, a 90-fold decrease and a 40-fold decrease for type I collagen was observed, respectively, in the group treated with HA-chondro, and only HA compared with the OA group.
In the OA group, MMP-1 immunostaining showed a diffuse dark-brown positivity in chondrocytes of the superficial layer at 8 weeks (data not shown), 3 and 6 months (60%) (Fig. 6a, b). The chondro-HA treated group showed moderate positive cells at both experimental times (50%) evaluated (Fig. 6c, d), and this positivity also remained evident in the group treated with HA alone at both 3 and 6 months (60%) (Fig. 6e, f). As observed in MMP-1, the OA group showed positive cells for MMP-3 localized at the superficial layer at 8 weeks (data not shown), 3 and 6 months (70%) (Fig. 6g, h). Both treated groups were instead negative for MMP-3 at 3 and 6 months (Fig. 6i–l).
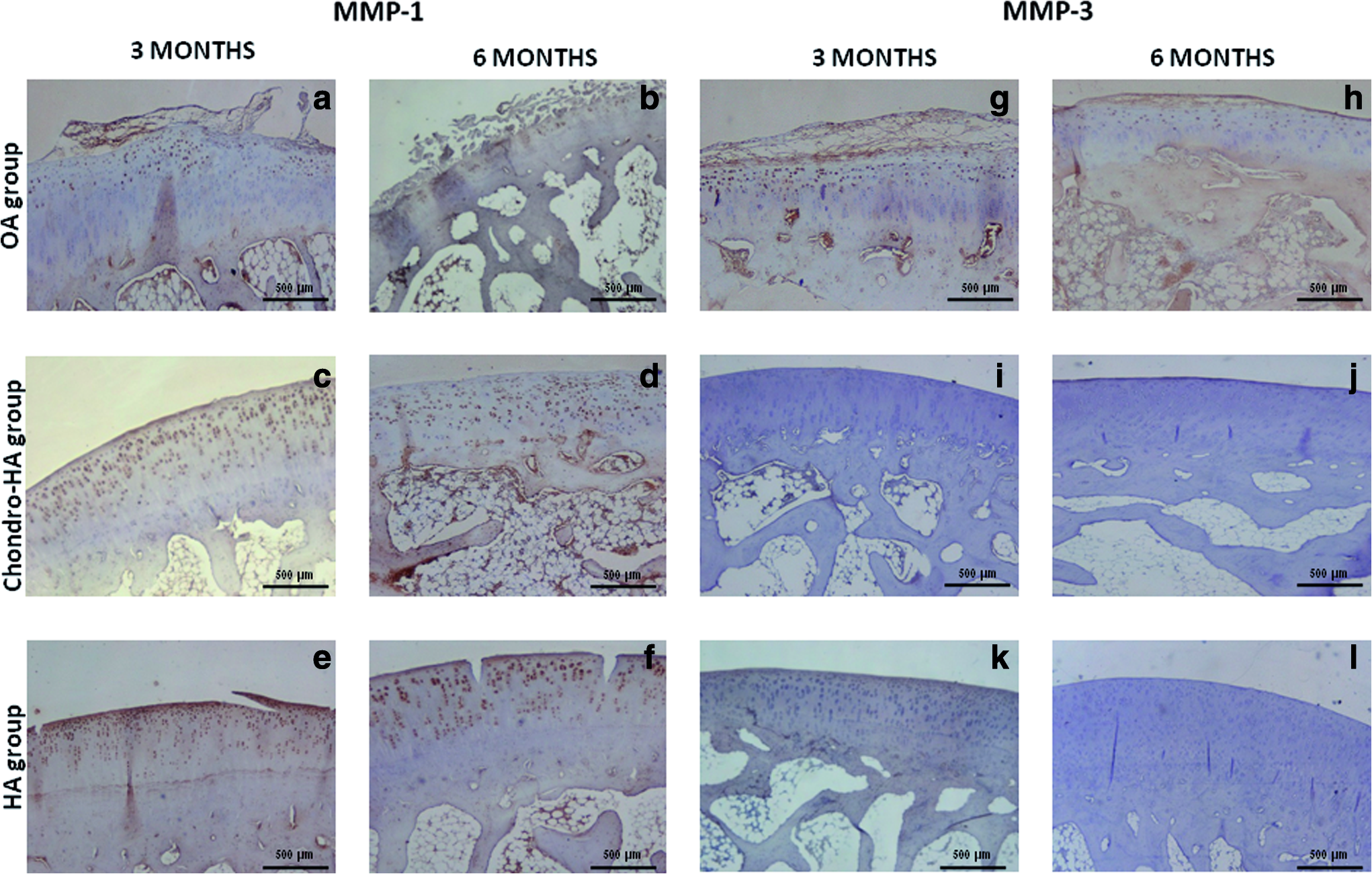
In the OA group, MMP-1 immunostaining showed a diffuse positivity in chondrocytes of the superficial layer at 3 and 6 months
Discussion
OA is a largely diffuse pathology that represents the most widespread cause of physical morbidity and impaired quality of life throughout the industrialized world.2,3 Several joints might be affected by OA, but the sites most commonly affected are knees, hips, fingers, and the lumbar and cervical spine. 1 Given that many questions, particularly those concerning the patho-physiology of OA, remain unanswered, it is not surprising that treatments, either pharmacological or surgical, only partially address the clinical issue.5–9 The current cellular therapies in the joint focus on the repair of isolated cartilage lesions and do not as yet address the widespread damage associated with OA. With continued improvements in early diagnosis of the disease, it is conceivable that cellular therapies may be applied to resurface degenerative tissues, providing a permanent, biological solution in order to avoid and procrastinate prosthesis' interventions.
The major challenges in regenerative medicine for cartilage are the restoration of a biomechanically competent extracellular matrix and the integration of the newly synthesized one within the resident tissue. To address this specific issue, autologous chondrocyte implantation was developed and has paved the way for cell therapy-and biomaterial-assisted cartilage engineering. 41 This technique is now largely used in the United States and other countries by means of suitable and improved scaffolds such as collagen, 42 hyaluronan acid, 43 or poly DL-lactic acid co-glycolic acid. 44 In particular, polymers such as hyaluronan allow the production of TIMPs in chondrocytes, 45 fibroblast adhesion, migration, and cell proliferation46,47 because of its cell surface receptor CD44; moreover, they provide a reduction of several molecules involved in cartilage degenerative diseases, 22 by indicating its possible use to treat early lesions in osteoarthritic patients.
On the basis of these considerations, we investigated, in a previous work, the efficacy of the MSCs seeded onto Hyaff-11 that repair early degenerative lesions in an OA animal model. 26 The findings obtained were encouraging, showing the formation of a new cartilaginous tissue, particularly at 6 months from the treatment, probably due to the secretion of bioactive factors, which, in part, provide a regenerative environment stimulating mitosis and the differentiation of tissue-intrinsic repair and, on the other hand, exert an anti-inflammatory and immunosuppressive action. 48
In the present work, we focused our attention on the use of autologous chondrocytes in evaluating whether the transplantation of differentiated cells might represent a further advantage as cellular therapy for OA care. Moreover, the outcomes of the two different cell therapies could help the choice of the more appropriate cellular type and, at least, could also provide a better understanding of their way of action.
In the current study, we performed a treatment based on the transplantation of condro-HA in the care of early OA lesions surgically induced in a rabbit model and evaluated by means of histomorphometrical, histological, and immunohistochemical analyses. Cartilaginous tissue generated by Hyaff®-11 meshes seeded with chondrocytes displayed abundant glycosamminoglycans content.
The evaluations performed with Kraus' Modified Mankin and OARSI scores confirmed the presence of a tissue with many hyaline cartilage features within 3 months from ACLT, thus at an earlier time compared with MSCs-HA treatment. With regard to FI, the chondro-HA group showed low values at 3 and 6 months, whereas this was not observed using MSCs-HA. CT and SBT values are in agreement with those obtained by using MSCs. Neither signs of inflammation within the joint, nor histological findings of cell reactions were found with the different treatments employed in our animal model. Immunohistochemical evaluations provided evidence of the presence of specific extracellular matrix proteins. In particular, collagen type II, the marker of hyaline cartilage, which was negative after ACLT at 3 and 6 months in the OA group, became positive in the chondro-HA treated group at the same experimental times. The analyses of specimens from cell-seeded implants revealed nearly-normal amounts of type-II collagen at an extracellular level with a percentage very close to a healthy control group (data not shown).
A difference in the treatment performed in our previous work using MSCs has been also observed, 27 where we clearly detected an intense positivity of type II collagen not only at the extracellular level but also within the cells.
From our experience, this last finding reflects a more immature condition of cartilage tissue in a remodeling state, as in a healthy cartilage, the positivity is well evident at the extracellular level. Type I collagen, positive after OA development, became negative in the chondro-HA group as observed in MSC-HA transplantation from 3 months. Our attention was also focused on the expression of MMPs, considering their pleiotropic action as effectors of ECM remodeling, vascular invasion, initiating force leading to endochondral ossification and chondrocyte apoptosis. 49 In particular, our investigations were addressed to MMP-1 and MMP-3, which were absent in the MSCs-HA treated group, while a positivity for MMP-1 was found in the chondro-HA group.
Taken together, our findings provide evidence that both chondrocytes and MSCs combined with Hyaff-11 are valid candidates for OA cartilage repair under the specific experimental conditions utilized. Hyaff-11 alone allowed damaged cartilage to re-synthesize matrix proteoglycans in some cartilaginous zones by exerting a chondro-protective effect, as evident by Safranin-O/Fast Green staining. However, its role is limiting, because OA chondrocytes continue to remain in a flawed homeostasis, thus leading to an incomplete attempt to repair the cartilage damage. Chondro-protective action is enhanced by adding two different cellular types such as AC and MSCs onto Hyaff-11. In vitro and in vivo studies have indicated the pro-inflammatory cytokines, particularly IL-1β and TNF-α, in the destruction of articular cartilage in OA. 50 The major target cell of these cytokines is the chondrocyte, which in OA cartilage shows a dysregulated expression of catabolic and anabolic genes, resulting in imbalanced homeostasis.51,52 The action of AC and MSCs onto Hyaff-11 would seem to take part in several networks interfering with this behavior with an up-regulation and/or down-regulation of some signaling pathways such as Wnt, NF-K beta involved in cartilage repair, secreting anti-inflammatory cytokines, and different growth factors such as transforming growth factor beta (TGFbeta) 1 and IL-17, in the local milieu and/or in the synovial cavity. 53 In particular, implanted autologous chondrocytes would seem to persist into the implantation site, contributing to the structural repair of the tissue by secreting bone morphogenetic proteins and other anabolic factors such as TGFbeta,30,51,54 even if their role in the molecular signaling and subsequent tissue remodeling that leads to mature hyaline cartilage formation still needs to be investigated in detail. With regard to MSCs, some authors reported how the therapeutical potential of these cells, at least in some applications, could be related to paracrine actions with the release of growth factors such as insulin-like growth factor 1, vascular endothelial growth factors, IL 8, angiogenin, and basic fibroblast growth factor that modulate the immune response at different levels, the mobilization and promotion of host cells, and the prevention of an inappropriate fibrotic response.55–57 Ongoing studies in our and other laboratories are aimed at finding early and progressive changes in chondrocyte physiology linked to the OA disease state by means of different technologies as microarrays, RNA interference analysis, and proteomics.
In conclusion, the use of chondro-HA for the treatment of early OA lesions produced, already at 3 months, a repair tissue showing better macroscopic, histological, and immunohistochemical results than those observed after HA treatment. Thus, the transplantation of chondro-HA would seem to be advocated in the very early stage of the OA disease when a precocious action is mandatory.
Further studies are, however, necessary to verify the two different cell treatments in a larger OA animal model, which might fully elucidate the mechanisms of actions that occur in OA repair processes, extending the analyses also in the synovial compartment, to realize any potential clinical application.
Footnotes
Acknowledgments
Thanks are due to Elettra Pignotti for statistical evaluation. The authors are grateful to Patrizia Rappini and Graziella Salmi for assistance in the preparation of the article and to Luciano Pizzi for his technical assistance. This work was supported by grants from Progetto Regione Emilia-Romagna Università “Regenerative Medicine in Osteoarticular Diseases.”
Disclosure Statement
No competing financial interests exist.