
Abstract
Tissue-engineered scaffolds may improve experimental outcomes in cardiac cell therapy by targeted delivery of stem cells and mechanically support an infarcted left ventricular (LV) wall. We transplanted cardiomyocyte-like cells (5×105) with scaffolding via epicardial patching (cell patch, n=17) or a low-dose intramyocardial hydrogel (LD hydrogel, n=18), a high-dose (5×106) intramyocardial hydrogel (HD hydrogel, n=18) or transplanting a serum-free medium control (control, n=13), a blank patch (n=14), and a blank gel (n=16) for targeted cardiomyoplasty in a myocardial infarcted rat model. LV real-time hemodynamics were assessed using a 1.9-F pressure–volume catheter 7 weeks after stem cell transplantation. All mode of scaffold transplantation protected diastolic function by preserving LV wall integrity that resulted in a lower end diastolic pressure–volume relationship (EDPVR) as compared to a control medium-injected group. Moreover, epicardial patching, but not hydrogel injection, reduced ventricular wall stress with a significantly better LV end diastolic pressure (EDP: 5.3±2.4 mmHg vs. 9.6±6.9 mmHg, p<0.05) as compared to control. Furthermore, epicardial patching additionally preserved systolic function by modulating negative remodeling through restricting dilatation of the LV chamber. In comparison to control, an improved ejection fraction in the cell patch group (80.1%±5.9% vs. 67.9%±3.2%, p<0.01) was corroborated by load-independent enhancement of the end systolic pressure–volume relationship (ESPVR: 0.88±0.61 mmHg/uL vs. 0.29±0.19 mmHg/uL, p<0.05) and preload recruitable stroke work (PRSW: 68.7±26.4 mmHg vs. 15.6±16.2 mmHg, p<0.05) in systolic function. Moreover, the cell patch group (14.2±1.7 cells/high-power field vs. 7.4±1.6 cells/high power field, p<0.05) was significantly better in myocardial retention of transplanted stem cells as compared to the LD hydrogel group. Collectively, myocardial transplantation of compliant scaffolding materials alone may physically improve wall mechanics, largely independent of stem cells. However, epicardially grafted cell patch conferred added systolic contractility by improving stem cell retention and cellular alignment leading to improved LV remodeling and geometric preservation postinfarction.
Introduction
Retention of transplanted stem cells following myocardial injection presents a significant challenge to achieving a meaningful therapeutic outcome. It has been reported that only less than 2% of the injected cells are retained in the myocardium. 17 Even though dose-dependent recovery of cardiac function following stem cell transplantation has been demonstrated previously, overall survival of the injected cells remained low. 18 Approaches taken to retain stem cells are likely to be critical to overall functional recovery. Apart from conferring passive mechanical support to the compromised ventricular wall, scaffolding with biocompatible cardiac matrices may precondition stem cells to assimilate more readily into the myocardium. 19 Piao et al. 20 transplanted bone marrow-derived mononuclear cells on poly-glycolide-co-caprolactone scaffolds and Zimmermann et al. 21 seeded neonatal cardiac cells in a collagen/matrigel matrix to improve function in the infarcted rat myocardium. Grafting of the stem cell-seeded collagen scaffold onto the infarcted myocardial scar has been reported in the Myocardial Assistance by grafting a new bioartificial upgraded myocardium (MAGNUM) trial with encouraging outcomes in scar thickness, LV dilatation, and myocardial compliance. 22 Similarly, clinical experience gleaned from the ACORN trial utilizing acellular cardiac supporting device demonstrated the benefit of mechanical scaffolding in heart failure patients. 23
For meaningful myocardial tissue replacement, scaffolding materials should support functional retention of stem cells and provide mechanical support to the weakened ventricular wall. Encouraging outcomes of transplanting human bone marrow-derived stem cells in experimental infarct models have been previously reported.24–26 However, there is limited data on similar contributions of stem cell-seeded scaffolds in myocardial compliance and contractility following AMI. Furthermore, it is unclear if the underlying mechanical property of the scaffolds affects the overall outcome in cardiac cell therapy. We have previously reported that our stem cell-derived cardiomyocyte-like cells (CLCs) showed significant interaction with collagen V matrix in vitro and in vivo.27–29 In the present study, we investigate if grafting CLCs in a collagen-based epicardial patch would confer an added mechanical and functional advantage to transplanting them as an intramyocardial injectable collagen hydrogel in repairing a localized myocardial injury.
Materials and Methods
Recruitment of patients
Forty-eight patients who were scheduled for a cardiothoracic surgery were recruited after informed consent. The study conformed to the Declaration of Helsinki and was approved by the Institutional Review Board of the Singapore General Hospital.
Cell isolation and culture
Approximately 2–5 mL of bone marrow aspirates from the sternum were collected and were depleted of mature blood lineages using the Rosettesep kit (Stem Cell Technologies, Vancouver, Canada) before centrifugation in the Ficoll (Sigma, St. Louis, MO) density gradient. Mesenchymal stem cells (MSCs) were derived and CLCs were differentiated as previously described. 30 Briefly, spindle-shaped early passage MSCs that were maintained in Dulbecco's modified Eagle's medium–low glucose (DMEM-LG) with 10% fetal bovine serum were differentiated in the myogenic differentiation medium (MDM) consisting of 60% DMEM-LG/28% MCDB-201 (Sigma), 10 μg/mL bovine insulin, 5.5 μg/mL human transferrin, 5 ng/mL sodium selenite, 500 μg/mL bovine serum albumin (BSA), and 4.7 μg/mL linoleic acid, 10−4 M ascorbate phosphate and 10−9 M dexamethasone (all from Sigma), and 100 units/mL penicillin G, 100 μg/mL streptomycin sulfate (GIBCO/Invitrogen, Carlsbad, CA), and 10% fetal bovine serum (Stem Cell Technologies). After 2 weeks of differentiation, ∼30% of MDM differentiated cells that expressed multiple cardiac proteins and nascent I-Z-I-like structures with laterally aligned Z-bodies with regular periodicities were termed CLCs.
Cell labeling and scaffold preparation for cell transplantation
CLCs (derived from MSCs of the same patient) were labeled with 1 μM Vybrant Cell Tracker CM-DiI (Molecular Probes/Invitrogen, Carlsbad, CA). Supplementary Figs. S1 and S2 (Supplementary Data are available online at www.liebertpub.com/tea) demonstrate uniformity and specificity of CM-Dil labeled CLCs. Cells (5×105 cells) were seeded onto a collagen sheet (0.75×0.75 cm; Baxter, Deerfield, IL) coated with 10 μg/cm2 of collagen V (Sigma) or infused in a neutralized collagen hydrogel solution constituted with 1.4 mg/mL of rat tail collagen I (Beckon Dickinson, Franklin Lake, NJ) and 0.05 mg/mL of collagen V (Sigma). In another experimental group, 5×106 cells were resuspended into the high-dose hydrogel group. Cell viability was estimated by trypan blue staining using a hemocytometer before cell transplantation.
Rat myocardial infarction model
The animal study was approved by the Singapore General Hospital IACUC committee and conforms with the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health (NIH Publication No. 85–23, revised 1996). Myocardial infarction was created by repeatedly (10 s each for 10 times) cryoinjured the LV free wall of male Wistar rats weighing 200 to 250 g using a liquid nitrogen cooled metal rod of 0.5-cm diameter. Immediately postinfarction, hydrogel solution containing labeled CLCs or the serum-free medium were injected into the peri-infarct regions (4 injection points) of the heart. Alternatively, the cell-seeded patch or the blank patch was overlaid onto the created infarct and anchored with suture. Cyclosporine was administered 3 days prior and daily after cell transplantation as well as in the serum-free medium injected control group at a dose of 5 mg/kg/day. Seven weeks postinfarction, animals were euthanized and heart explanted.
Echocardiography
Transthoracic echocardiography assessments were performed with a 13-MHz linear array transducer (i13L) using Vivid 7 system (GE-Vingmed, Horten, Norway). Cardiac function was assessed at baseline and 6 weeks post-treatment. M-mode tracings were recorded from the parasternal short axis view at the papillary muscle level. Data were analyzed in offline system (Echopac) in a blinded manner. Infarct wall thickness and LV dimensions were measured from 3 consecutive cardiac cycles. LV EF was calculated using the modified Quinones method, 31 while LV fractional shortening (FS) was calculated as (LVIDed-LVIDes)×100%/LVIDed. All data were presented as percentage change from baseline.
In vivo hemodynamic measurement
A 1.9-French microtip variable segmented pressure–volume (PV) conductance catheter (Scisense, Ontario, Canada) was inserted into the right carotid artery and advanced into the left ventricle before sacrifice of animals at 7 weeks post-treatment. The positioning of the catheter was visualized and confirmed by echocardiography guidance. After stabilization for 10 min, signals were continuously recorded at the sampling rate of 1 kHz using a iWorx system (iWorx Systems, Dover, DE) coupled to an Advantage box (Scisense). Manual transient compression of inferior vena cava for derivation of load-independent PV parameters was performed according to Pacher et al. 32 Data were analyzed using iWorx pressure–volume conductance system (Labscribe, iWorx Systems).
Fluorescence microscopy
Frozen tissue sections were fixed in 4% paraformaldehyde, permeabilized with 0.1% Triton X-100, and further blocked in 5% BSA before incubating with primary antibodies, including sarcomeric α actinin and smooth muscle α actin (all from Sigma). This was followed by incubating with Alexa Fluor 488/555-conjugated secondary antibodies (Molecular Probes). Nuclei were stained with 4′,6-diamidino-2-phenylindole (DAPI) before visualized using a fluorescent microscope (Carl Zeiss, Munchen-Hallbergmoos, Germany) and data were analyzed using Axiovision (Carl Zeiss) version 4.6 software.
Microvascular density count
Vascularity in the myocardial tissues was quantified by measuring density of smooth muscle actin stained arterioles as previously described. 33 Range of small arterioles was decided based on reported lower limits of vessels that were most responsive to angiogenic cytokines. 34 Microvessels were subcategorized based on the lumen diameter by smaller or greater than 200 μm. All animals were included in data sampling, and vessels in the infarct borders of myocardium, but not pericardium, were counted.
Apoptosis staining
Apoptosis was determined by the in-situ TUNEL assay kit as described by the manufacturer (Roche, San Francisco, CA). Briefly, dewaxed sections were placed in a plastic jar containing the 0.1 M Citrate buffer (pH 6) and microwave heated. Slides were then blocked in Tris-HCL, 0.1M (pH 7.5) containing 3% BSA and 20% normal bovine serum. TUNEL reaction mixture was added and incubated for 1 h at 37°C in the dark. Converter-AP was then added after slides were washed in phosphate-buffered saline (PBS) thrice and incubated for a further 30 min at 37°C. Slides were then rinsed thrice with PBS and mounted with 70% glycerol and analyzed under the light microscope and DAPI was used to highlight nuclei. Quantification of apoptotic nuclei from randomly selected viewing fields in the peri-infarct zone was carried out using 20×objective and data were normalized against the medium-injected control group.
Estimation of human cells in transplanted rat heart
Transplanted cells that remained in the heart were estimated semiquantitatively by the modified method of Hirata et al. 35 Briefly, the heart was sectioned from the basal segment level below the left auricle to the apex, and tissue sections were screened at every 200 μm to locate transplanted cells. Ten selected sections that contained most cells from the cell patch and hydrogel groups were used for counting using 20×objective with the Zeiss M200 inverted microscope with Axiovision (Carl Zeiss) version 4.6 software. Data were presented as mean number of cells±standard deviation/high power field (HPF).
Detection of human Alu gene and human hTERT gene
Genomic DNA was isolated from explanted hearts using standard phenol/chloroform protocol. Purification of DNA was performed using the DNAeasy® Blood and Tissue Kit (Qiagen, Germantown, PA). DNA concentrations were determined using a NanoDrop 2000 (Thermo Scientific, Asheville, NC). The primers used for amplification includes the following: ALU sense, 5′- GTCAGGAGATCGAGACCATCCC-3′; ALU antisense, 5′- TCCTGCCTCAGCCTCCCAAG-3′ (Sigma) using 5 min at 95°C, 10 s at 95°C; 30 s at 58°C for 40 cycles. Real-time quantitative polymerase chain reaction (PCR) using total genomic DNA against human telomerase reverse transcriptase (hTERT) was performed using the Quantifiler human DNA quantification kit as described by the manufacturer (Applied Biosystems, Foster City, CA).
Mechanical measurement
The atrium and apex portions of the heart were removed transversely. The mid ventricular portion was cut into a strip with the infarct positioned at the center of the measuring machine. The ventricular strips were clamped onto the two measuring drums of the UXF12/UNI adaptor on the Physica MCR101 Rheometer (Anton Paar, Ostfildern, Germany). A prestress of 1 mNm (torque) was applied to straighten the sample and the ventricular strip was stretched and relaxed in a sinusoidal pattern at 1% strain and 1 Hz. All tests were conducted in the PBS environment at room temperature for 20 min. Complex tensile modulus or elasticity |E*| was computed by Rheoplus/32 V3.40 software from the stress and strain relationship. The storage modulus |E′| and loss modulus |E′′| that defined deformation energy stored and deformation energy lost, respectively, and their ratio |E′′|/|E′| representing loss factor tan(δ) were similarly derived to describe the viscoelastic property 36 of the ventricular strips. Similarly, the complex shear modulus, |G*|, was measured by using the 8-mm plate-and-plate measuring system. The ventricular tissue, the patch or the hydrogel were molded into a disc shape with a diameter ∼8 mm and placed between the gaps of the two opposing plates. Gaps between the plates were calibrated to 0.01 N as the measuring plates lightly compressed the two surfaces of the specimen. An oscillating strain sweep test from 0.01% to 100% was subjected to the sample and a |G*| versus strain curve was obtained. The plateau region of the curve was defined as the characteristic complex shear modulus of the sample.
Statistical analysis
The one-way analysis of variance was used to determine statistical significance between groups. A post-hoc comparison using the Dunett t test was employed to determine statistical significance as compared to the medium-injected control group. The Tukey Honestly Significant Difference post-hoc analysis was used to determine statistical significance between treatment groups in relative apoptosis index and transplanted cell count using SPSS version 13 (IBM, Armonk, NY) p<0.05 was considered statistically significant. All data were presented as mean±standard deviation.
Results
Cardiac function–echocardiography
LV echocardiography (Table 1) revealed that only the cell-seeded patch (ΔAWTed: +3.1%±8.3%, p<0.05; ΔAWTes: −4.9%±10.4%, p=ns) and the high-dose (HD) hydrogel (ΔAWTed: +6.1%±9.0%, p<0.05; ΔAWTes: −0.2%±9.0%, p<0.05), but not the low-dose (LD) hydrogel or their blank controls, significantly thickened the infarcted ventricular wall at diastolic and restricted further deterioration at the systolic phase, thereby arresting wall thinning as experienced in the medium control group (ΔAWTed: −7.9%±8.0%; ΔAWTes: −18.1%±18.2%).
Data presented as mean±standard deviation.
p<0.05. Dunnett t-test versus medium control.
AWTed, anterior wall thickness at end distole; LVIDed, left ventricular internal dimension at end diastole; AWTes, anterior wall thickness at end systole; LVIDes, left ventricular internal dimension at end systole; WT, wall thickening; EDV, end diastolic volume; ESV, end systolic volume; EF, ejection fraction; FS, fractional shortening; SVI, stroke volume index; LD, low dose; HD, high dose.
With the exception of the blank gel group that showed worsening of end systolic volume (ΔESV), all experimental groups showed no significant difference in the LV dimension or chamber dilatation. However, stroke volume index (SVI) of the cell patch group (−9.7%±10.9%, p<0.05), but not the hydrogel group, was significantly better preserved than the medium control (−22.0%±11.9%) group. Nevertheless, there was no significant difference in the contractile function in ΔEF and ΔFS among all the experimental groups.
Cardiac function–PV hemodynamics
Consistent with better ventricular wall integrity, LV PV catheterization (Table 2) confirmed that the cell patch (5.3±2.4 mmHg, p<0.05) and blank patch (3.2±2.7 mmHg, p<0.005) groups reduced wall stress as demonstrated in lower end diastolic pressure (EDP) as compared to the medium injection group (9.6±6.9 mmHg). Furthermore, the end diastolic pressure–volume relationship (EDPVR) in all experimental groups was uniformly better than the medium injection group. However, only the cell patch (p<0.05), but not other experimental groups, reduced the end-systolic volume (ESV: 59.8±23.0 μL, p<0.05) as compared to medium injection (114.3±33.9 μL). Consistently, only the cell patch group (80.1%±5.9%, p<0.01) improved the systolic performance by enhancing EF as compared to the medium control group (67.9%±3.2%). The enhanced systolic contractility in the cell patch group was further confirmed by the load-independent measurement of the end systolic pressure–volume relationship (ESPVR: 0.88±0.61 mmHg/μL vs. 0.29±0.19 mmHg/μL, p<0.05) and preload recruitable stroke work (PRSW: 68.69±26.38 mmHg vs. 17.55±16.18 mmHg, p<0.05).
Data presented as mean±standard deviation.
p<0.05.
p<0.01.
p<0.005 versus medium control.
HR, heart rate; SV, stroke volume; CO, cardiac output; SW, stroke work; ESP, end systolic pressure; dP/dtmax, maximal rate of left ventricle pressure change; EDP, end diastolic pressure; dP/dtmin, minimal rate of left ventricle pressure change; dV/dtmax, peak left ventricle filling rate; Tau-Weiss, time relaxation constant; ESPVR, end systolic pressure–volume relationship; EDPVR, end diastolic pressure–volume relationship; PRSW, preload recruitable stroke work.
Integration of transplanted CLCs
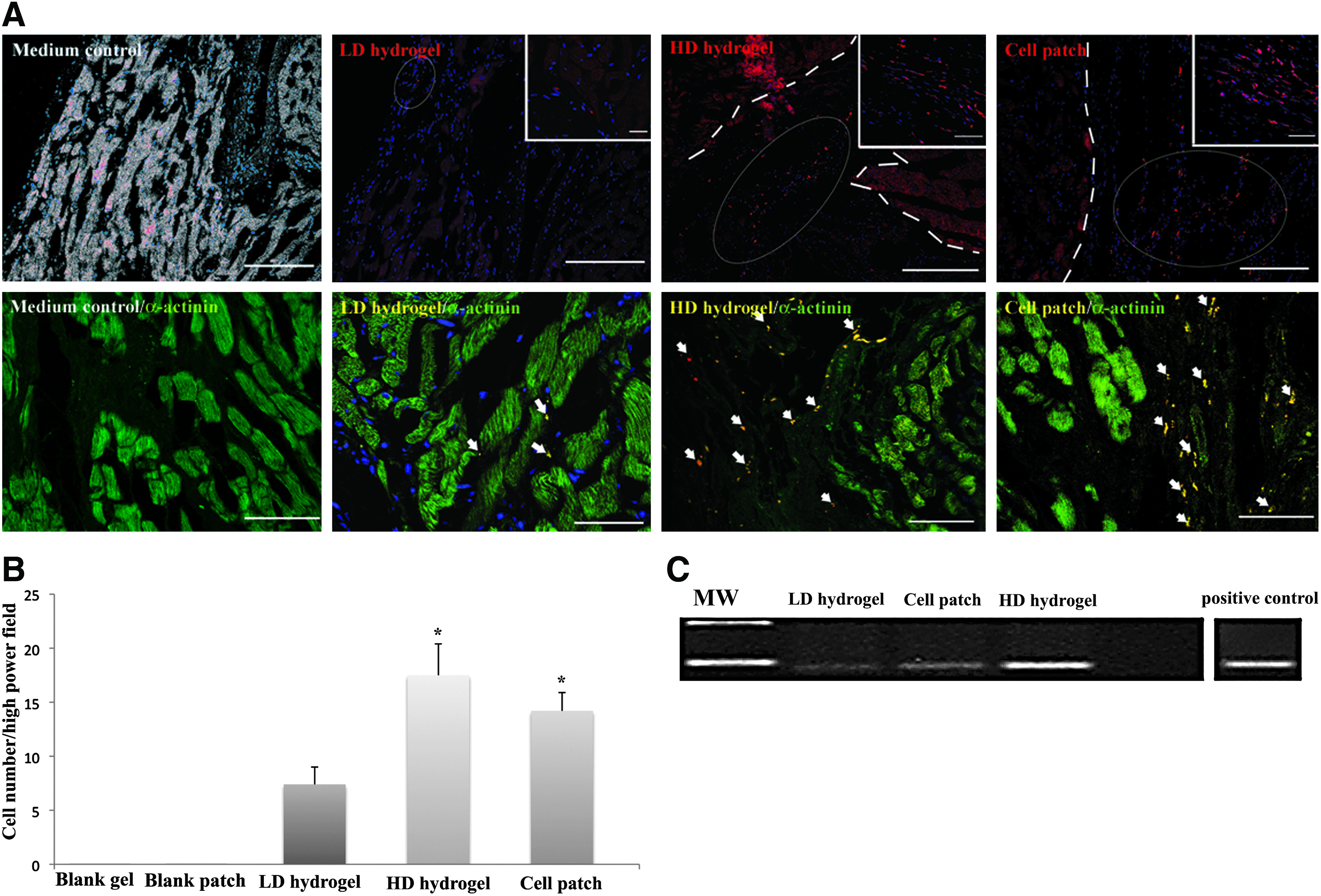
Immunofluorescence staining showed that CLCs survived well in the host myocardium. However, majority of the transplanted cells remained close to the peri-infarct sites (Fig. 1A, top panel), even though some cells in the HD hydrogel and cell patch groups were aligned in parallel to the axis of host muscle fibers (insets in Fig. 1A). Furthermore, few isolated cells were localized in close proximity to α-actinin-stained host muscle fibers, but the transplanted cells were absence of sarcomeric cross-striations (Fig. 1A, bottom panel). Semiquantitative counting of the transplanted cells showed that there were significantly more surviving cells remained in the host myocardium in the cell patch (14.2±3.7 cells/HPF, p<0.05) and HD hydrogel (17.4±4.3 cells/HPF, p<0.05) groups as compared to the LD hydrogel (7.4±1.9 cells/HPF) group 7 weeks following cell transplantation (Fig. 1B). Consistently, detection of human Alu gene by PCR confirmed the dose-dependent presence of human cells in the transplanted rat heart with the HD hydrogel showed the highest presence of human Alu gene followed by the cell patch group with the least in the LD hydrogel group (Fig. 1C). Similarly, quantitative real-time TaqMan PCR targeting against human telomerase reverse transcriptase (hTERT) gene confirmed the presence of higher number of human cells in the cell patch and HD hydrogel groups as compared with the LD hydrogel group (Fig. 1D).
Mechanical property of transplanted scaffolds strengthens infarcted wall
Mechanical measurements of the blank patch (9.37±2.79 kPa) expectedly showed a considerably higher shear modulus than the blank gel (0.012±0.001 kPa), although it was lower than those of intact heart (16.59±0.57 kPa) that was comparable to previously reported values of 10 to 20 kPa 37 for rat myocardium. Similarly, the cell-seeded patch (1.01±0.14 kPa) revealed a higher modulus than the cell-infused hydrogel (0.012±0.001 kPa) early after cell seeding, although such differences dissipated subsequently (Table 3).
p<0.05 versus blank patch.
p<0.001 versus intact heart.
p<0.05 versus intact heart.
ND, not determined.
The rheometric measurement of mechanical integrity of the ventricular wall (Fig. 2) revealed that wall integrity of the medium-injected group (81.2±18.3 kPa, p<0.001) was significantly compromised as compared to the intact healthy myocardium (195.4±15.0 kPa). In comparison, wall integrity of the cell patch (116±24.9 kPa), LD hydrogel (120.5±10.5 kPa), HD hydrogel (107.7±20.0 kPa) groups and blank patch (118.8±41.1 kPa) as well as blank gel (132.1±23.4 kPa) groups was comparable to the intact healthy myocardium (Table 3). Furthermore, mechanical compliance of the ventricle in the form of tan(δ) as demonstrated by differential storage and loss tensile moduli of the infarcted wall was better preserved in the cell patch (0.097), LD hydrogel (0.095), and HD hydrogel (0.098) groups as compared to the medium control (0.107) group, whereby only the medium injected group was significantly lower than the intact healthy myocardium in both the storage modulus (85.2±8.4 kPa vs. 194.7±14.9 kPa, p<0.001) and loss modulus (9.1±0.2 kPa vs. 16.8±0.9 kPa, p<0.05) (Table 3).
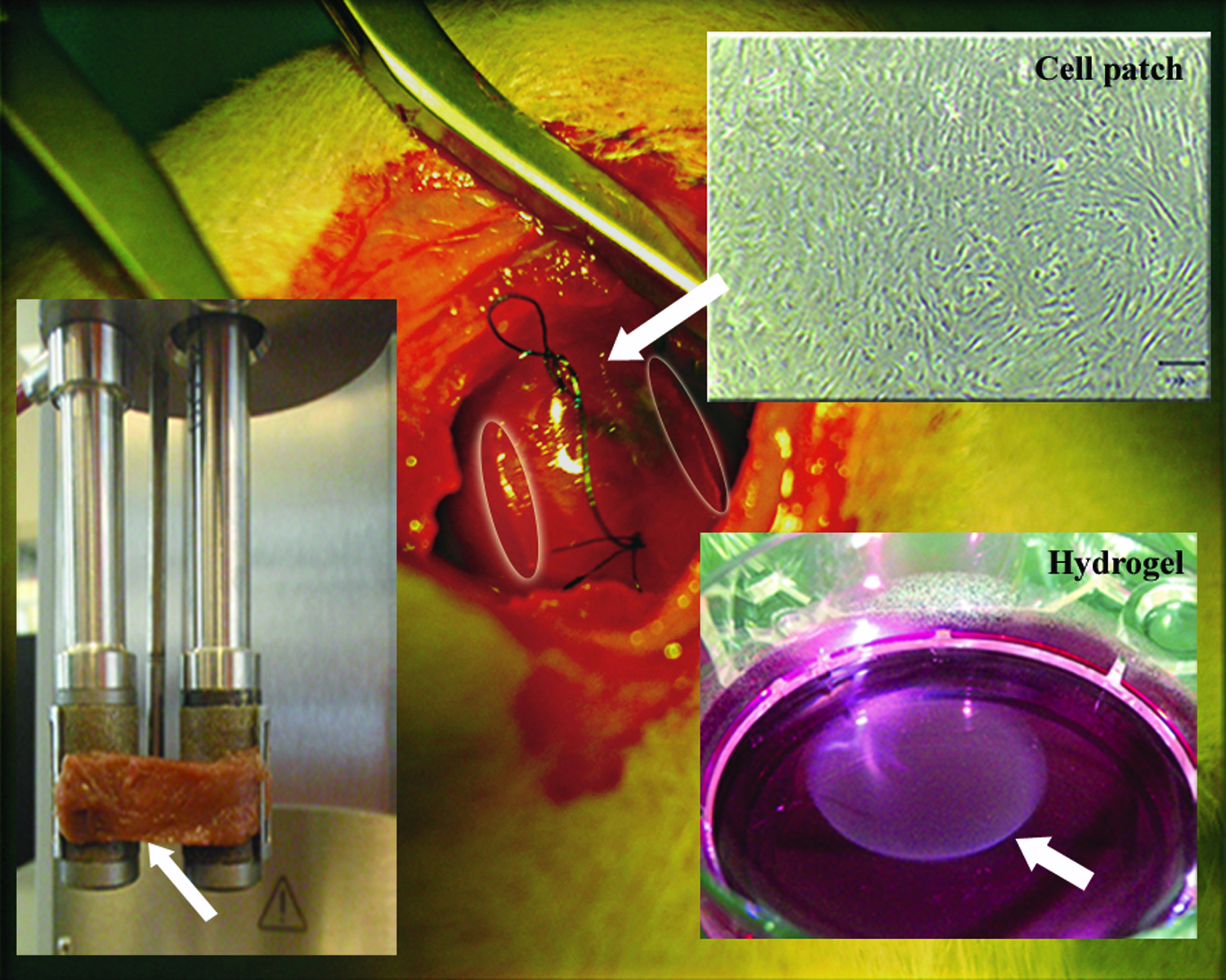
Left ventricular (LV) thoracotomy showing grafting of the cell patch onto the infarcted myocardium. White arrow indicates placement of the cell patch on the rat epicardium. Upper right inset showing the phase-contrast image of the CLC-seeded cell patch before cardiac grafting. Lower right inset with white arrow shows circular hydrogel formed in vitro demonstrating a well-formed gel capable for embedding CLCs. Lower left inset with white arrow shows rheometric assessment of the excised rat LV infarcted myocardium postsacrifice. Color images available online at www.liebertpub.com/tea
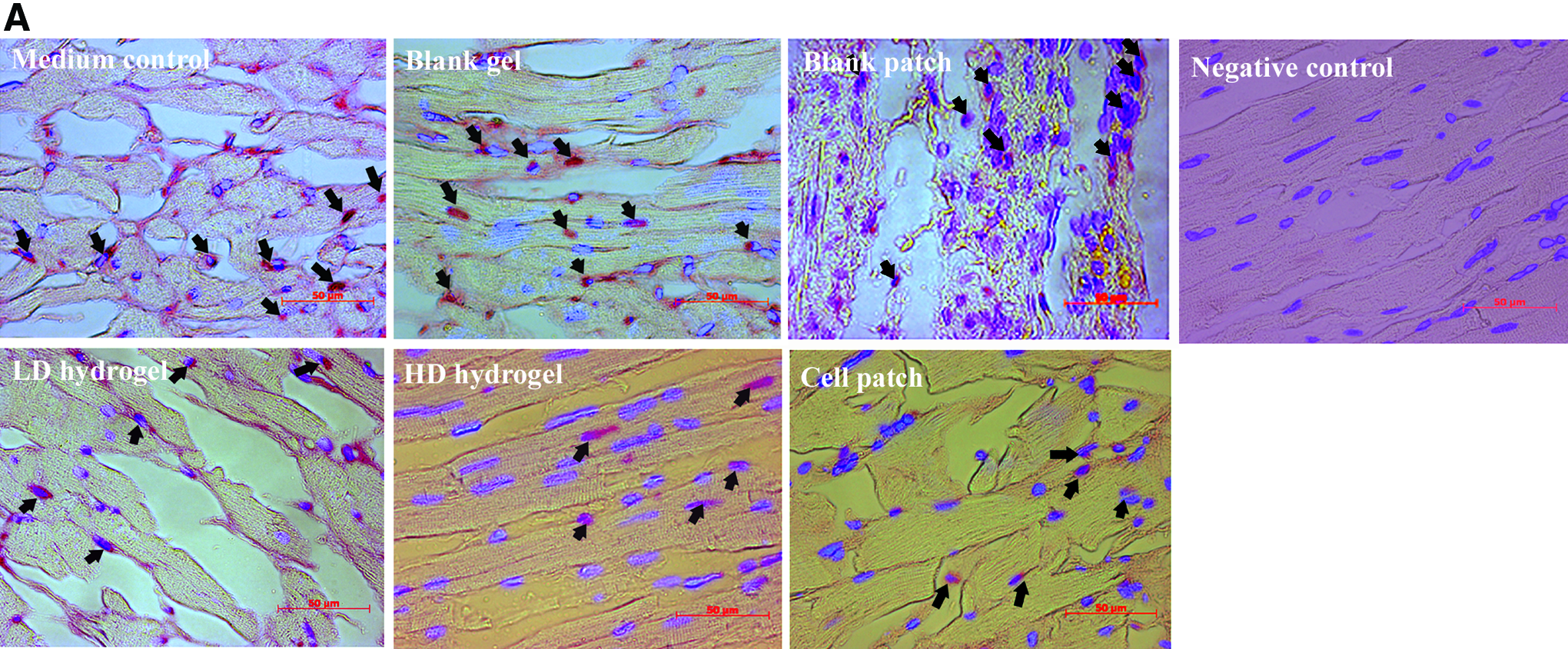
Transplantation of the cell patch (0.33±0.17, p<0.05), the LD hydrogel (0.20±0.16, p<0.05), and the HD hydrogel (0.34±0.26, p<0.05) resulted in a significantly reduced apoptosis in the infarct as compared to the blank patch (1.09±0.29) and blank gel (1.06±0.30) groups (Fig. 3A, B). However, there was no noticeable difference in the microvascular density count of both small (<200 μm diameter)-and large (>200um diameter)-sized arterioles in all the experimental groups as compared to the control group (Table 4 and Fig. 4).
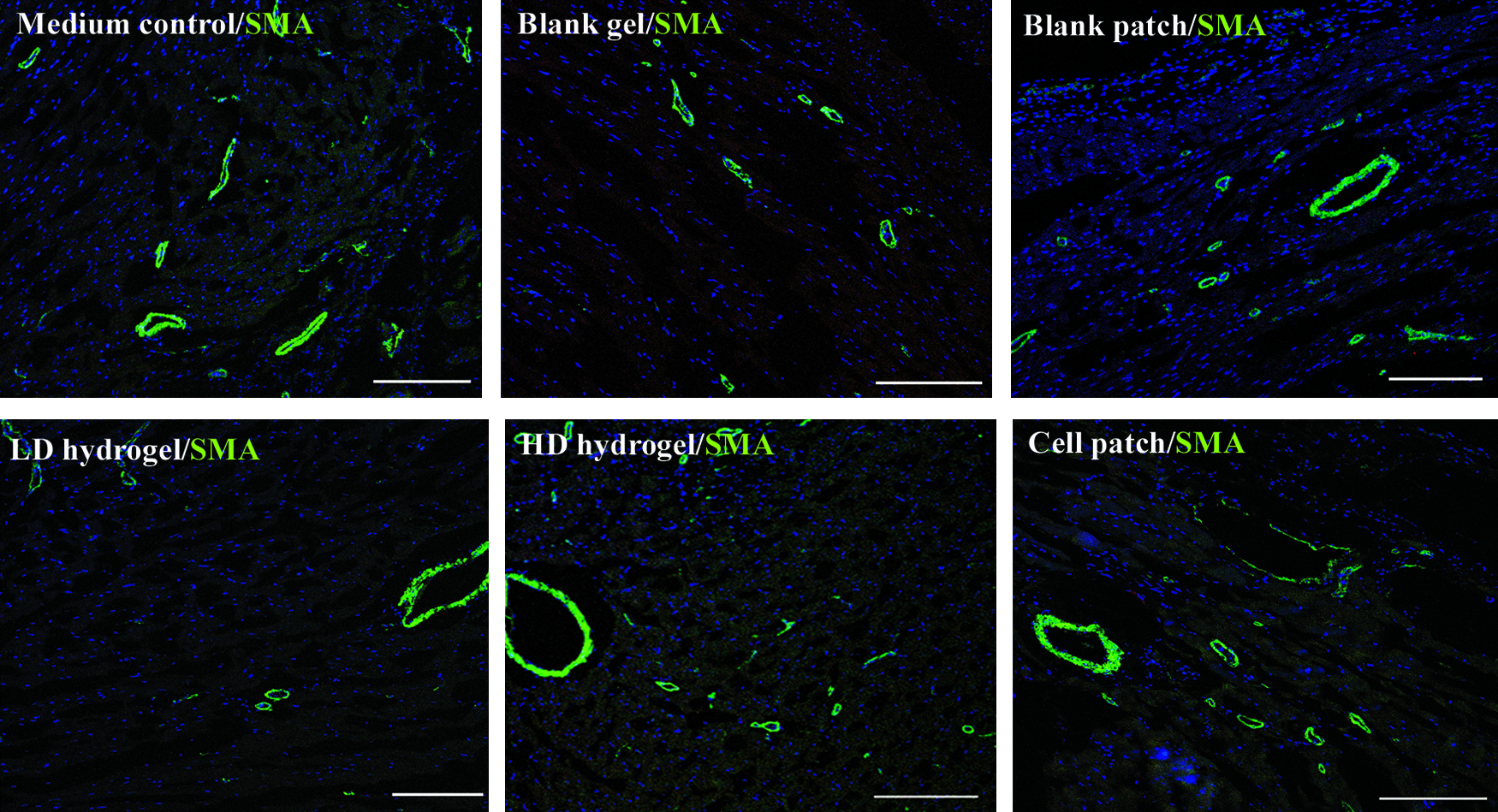
Comparable vascular angiogenesis in the cell transplanted groups and the control groups indicates low angiogenic potential of CLCs. SMA: α-smooth muscle actin; scale bar: 200 μm. Color images available online at www.liebertpub.com/tea
NS, not significant.
Discussion
Tissue-engineered scaffolds may improve experimental outcomes in cardiac cell therapy by targeted delivery of stem cells and mechanically support areas at risk postinfarction. Both the epicardial patch and the intramyocardial hydrogel exerted beneficial effects in the current study by maintaining myocardial compliance and preserving infarct wall integrity of the myocardium. This was evident by improved EDPVR (Table 2) and enhanced ventricular compliance and mechanical elasticity of the infarcted wall (Table 3). The beneficial effect of the acellular scaffold alone was consistent with previous published reports that showed better mechanical property 11 and improved LV remodeling 12 following transplantation. Nevertheless, better EDPVR observed in our acellular scaffold groups (blank patch or blank hydrogel) did not translate to additional improvements in systolic parameters, whereas only CLC-populated scaffolds (cell patch or HD hydrogel) were found to improve systolic indexes. This indicates that the presence of CLCs post-AMI by cryoinjury uniquely contributed to systolic contractility that was consistent with our previous observations in the subacute MI rat ligation model, 18 although no difference in EDPVR was observed in that study.
Despite similar numbers of CLCs being transplanted, the cell patch group resulted in a better cardiac function as compared to the LD hydrogel group. Functional benefits observed by the cell patch may have been driven by better cellular retention, even though no additional benefits in myocardial angiogenesis or antiapoptosis were observed in the cell patch group. Furthermore, the cell patch group contributed to a superior cardiac performance despite similar cellular retention achieved as in the HD hydrogel group in which 10-fold higher cell numbers were injected. This indicated that epicardial patching may impart cell-independent mechanical advantages to functional preservation as compared to intramyocardial injection. It is unclear if initial mechanical stability (1.01 kPa vs. 0.01 kPa) conferred by the underlying patch material as compared to the hydrogel group (Table 3) had any role in better survival of patch-seeded CLCs early after myocardial transplantation. Nonetheless, the overall low cell numbers remaining in both our patch and hydrogel groups indicated that large numbers of transplanted cells were lost after transplantation.
Contrary to other stem cell-populated cardiac patches that were reported to increase vascular angiogenesis as the main benefit in functional improvements,38,39 no such angiogenic effect was observed in CLC-populated scaffolds in our study. This could be attributed to a more differentiated nature of our CLCs as compared to stem cells utilized in previous studies. Instead, benefits of the cell patch were evident by restrained negative LV remodeling and reduced ventricular wall stress as demonstrated by moderated ESV and EDP, respectively. Such findings are consistent with experience from the ACORN trial, whereby external epicardial mesh was effective in maintaining ESV postinfarction. 40
Mechanical elasticity of the infarct wall at sacrifice attained similar recovery among the cell patch, the blank patch and LD hydrogel groups (Table 3), despite differing in vitro mechanical strength initially. This indicated that transplanted cells may only have a minimal role in recovery of the mechanical property of the infarcted wall. However, the differing mechanical property of the cell-seeded patch in comparison to the blank patch indicated that the seeded CLCs actively remodeled collagen fibers, and such activity may contribute to postinfarct remodeling of extracellular matrices (ECM) toward beneficial LV remodeling. Furthermore, the cell-seeded patch resulted in a more favorable LV compliance as demonstrated by smaller mechanical tan(δ) index (Table 3). This may in part explain the inability of the blank patch group in recovering EF and ESPVR despite favorable effect on EDPVR of transplanted left ventricle (Table 2). Consistently, such ECM remodeling by transplanted stem cells has been reported to link to recovery of cardiac function postmyocardial infarction.37,41
Functional recovery in the cell patch group was confirmed by a significantly better hemodynamic measurement of EF (p<0.01), ESV (p<0.05), SVI (p<0.05), and infarct wall thickness at diastole (AWTed, p<0.05) as compared to the medium-injected control. Furthermore, superiority of cell patch epicardial transplantation over HD hydrogel intramyocardial injection was reinforced by the load-independent measurement of ESPVR (p<0.05) and PRSW (p<0.05), which further supported a unique role of epicardial patching of CLCs in enhancing efficiency of systolic contractility in the infarcted myocardium. Interestingly, transplanting the blank patch alone was as effective as the cell patch in reducing wall stress as demonstrated by moderated EDP (Table 2), although no other cardiac benefits were apparent without the presence of cells. This confirmed the unique benefits conferred by an epicardial approach in scaffolding stem cells, which was consistent with the previous report of epicardial grafting of adipose-derived stromal cell sheets, 42 although no comparison to the acellular scaffold was performed in that study. Such mechanical stabilization of the stressed regional wall was consistent with previous observations, whereby scaffolding materials alone could affect cardiac mechanics, but not necessarily translated to improvement in global contractile function. 16
Despite cell patch-transplanted CLCs contributed to specific augmentation of contractile hemodynamics, systolic recovery remained disproportional to the relatively low numbers of cells found in the heart. While the two-dimensional cell patch utilized in the current study has a limited surface area for transplanting higher cell volume, it was unlikely that cell-mediated myocyte replacement alone could be responsible for the recovery of global cardiac function. As revealed by better ESV and EDP, the combined antiapoptotic effect of CLCs with a compliant epicardial patch may alleviate chamber dilatation 43 and reduce wall stress by thickening of the infarcted wall as predicted by Laplace's Law. 44 Such improvements in ventricular wall mechanics may stabilize mechanotransduction signals to restore stress-induced apoptosis and normalize changes to mechanoelectrical properties of surviving myocytes. 16 Furthermore, better preservation of structural architecture of the ventricular wall in the form of laminar shearing and extension throughout cycles of systole and diastole are crucial in regional mechanical function. 45 The cell patch approach with its preorganized monolayered cell–cell connections and more aligned cellular orientation demonstrated in the infarct may better preserve this aspect of architecture than the enzymatic prepared hydrogel injection approach, since interspersed distribution of interstitial collagens by scattered injection of cell-infused gel matrix may increase stiffness 46 or arrhythmias, 17 although such an adverse outcome was not apparent in our current study at 7-week post-transplantation. Such implications of cell-seeded scaffolds may continue influencing ventricular remodeling chronically, even if the underlying scaffold and transplanted cells are unlikely to persist in the rat myocardium over a longer term. Similar observation was reported previously in a rodent infarction model that received human MSCs. 47
In comparison to the hydrogel approach, more superior endogenous repair and endogenous stem cell mobilization by the patch approach may serve as an alternative mechanism in functional improvement; such a population, however, was rarely observed in previous experience with collagen patches, 15 although the Sca-1 antibody-conjugated collagen patch that captures circulating stem cells has been recently reported to enhance cardiac tissue repair. 48 Furthermore, increased adrenergic sensitivity and reduced myocyte hypertrophy by an epicardial supporting device similar in concept to the current cell patch approach were previously demonstrated. 40
Collectively, myocardial transplantation of compliant scaffolding materials alone may physically improve wall mechanics, largely independent of stem cells. However, the epicardially grafted cell patch conferred added systolic contractility by improving stem cell retention, and cellular alignment leading to improved LV remodeling and geometric preservation postinfarction.
Footnotes
Acknowledgments
This study was funded by the research grant from the National Medical Research Council of Singapore and the SingHealth Foundation.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.