
Abstract
We developed a novel injectable type I collagen/hyaluronic acid/fibrinogen (COL/HA/FG) composite gel that encapsulated synovium-derived mesenchymal stem cells (SDSCs) for the repair of damaged articular cartilage. We first analyzed the suitability of the composite gel as a three-dimensional injectable cell carrier in vitro. In an in vivo rabbit model, the COL/HA/FG composite gel displayed the potential to regenerate and repair osteochondral defects in the knee. Culture of the SDSCs encapsulated COL/HA/FG composite gel in a chondrogenic medium resulted in high viability of the SDSCs and high expressions of type II collagen, aggrecan, and sox 9 mRNA. Moreover, glycosaminoglycans and type II collagen were accumulated within the extracellular matrix. In the animal model, the SDSCs encapsulated COL/HA/FG composite gel produced a hyaline-like cartilage construct. Twenty-four weeks after transplantation, the defects had been repaired with hyaline cartilage-like tissue that was densely stained by safranin-O and immunostained by a type II collagen antibody. This data suggest that the SDSC-encapsulated COL/HA/FG composite gel can be a good therapeutic candidate/strategy for repairing of damaged articular cartilage.
Introduction
In addition to the selection of a cell source, the vehicle used for the delivery of the cells also is crucial in cell-based therapy for tissue regeneration. Injection of a MSC suspension can lead to improved cartilage healing. 10 However, direct transplantation of MSCs may lead to cell leakage during the healing process, preventing the formation of hyaline cartilage. 11 Injectable hydrogel-type scaffolds that mimic the chondrogenic environment of MSCs have become a major research in the field of articular cartilage regeneration.12,13 Furthermore, they facilitate the transport of nutrients to cells encapsulated in a hydrogel-type scaffold. Among them, collagen (COL), fibrinogen (FG), and hyaluronic acid (HA) have been utilized as typical extracellular matrices for cartilage regeneration.14–17 More recently, the combined use of two or more biomaterials has been explored to utilize to benefits of each biomaterial, including COL/HA, 18 fibrin/HA, 19 and COL/fibrin. 20 The results from the combined gels have indicated their feasibility as supports for cell proliferation without loss of cartilage regeneration potential. A combination, gelatin/chondroitin/HA tri-copolymer, has demonstrated potential in cartilage tissue engineering.21,22 Therefore, when the advantages of the three materials are ideally combined, the hybrid biomaterials could be an attractive scaffold to support better cell survival, proliferation, differentiation, and matrix synthesis, leading to the reconstituted hyaline architecture of cartilage. The present study explored this possibility. SDSCs encapsulated collagen/hyaluronic acid/fibrinogen (COL/HA/FG) composite gel was assessed for its feasibility as an injectable cell carrier for its suitability in a three-dimensional environment. Also, we determined the potential of the composite gel to regenerate and repair osteochondral defects in rabbits.
Materials and Methods
Preparation of COL/HA/FG composite gel
FG (71.5–126.5 mg/mL, Greenplast kit; Green Cross) was dissolved in an aprotinin solution (1100 Kallikrein inhibitor units [KIU/mL]; Green Cross), which was a protease inhibitor typically added to slow fibrinolysis. The FG solution was mixed with COL (COL/FG; 3%, RMS Innovations), HA (HA/FG; 10 mg/mL, LG CI), respectively, and with both COL and HA. The different mixture ratios of composite gel are described in Table 1. The COL/HA/FG solution was loaded into syringe A of a Duploject syringe support system (included in the Greenplast kit; Green Cross). Thrombin (4.9–11.1 mg/mL) containing 40 mM CaCl2 was loaded into syringe B. Upon mixing, the two solutions almost instantaneously formed a gel; for each sample, the total volume of the gel was about 200 μL. The gels were transferred to six-well culture plates.
COL/HA/FG, collagen/hyaluronic acid/fibrinogen.
Enzymatic degradation time assay of the COL/HA/FG composite gel
To mimic an in vivo degradation profile, the COL/HA/FG composite gels (200 μL) of various mixture ratios were incubated in 2 mL phosphate-buffered saline (PBS) containing lysozyme (1 mg/mL; Sigma-Aldrich) at 37°C at the predetermined time intervals (day 1, 3, 5, 7, 10, 14, 21, and 28). Weight loss of the initially weighed gel (W0) was monitored as a function of the incubation time in PBS at 37°C. At specified time intervals, the gels were removed from the PBS and weighed (Wt). The remaining gel weights were expressed (%) as (Wt/W0)×100.
Isolation and expansion of rabbit SDSCs
All the experimental procedures involving the use of animals were in accordance with the NIH Guide for the Care and Use of Laboratory Animals and the procedures were approved by the Ethics Committee of the Seoul National University Hospital. Synovial tissues were harvested aseptically from the knees of New Zealand white rabbits (8-month-old males weighing 3.5–4.0 kg) under anesthesia. The synovial tissues were finely minced in PBS and then digested with 0.02% collagenase (Sigma-Aldrich) at 37°C. After filtering through 70-μm cell strainers, the released cells were washed and resuspended in a culture medium (high glucose DMEM; Gibco) supplemented with 10% fetal bovine serum (Gibco) and 1% antibiotic–antimycotic solution (Gibco), and were plated at 2×104 cells in 150-mm-diameter culture dishes (Nunc) at 37°C in a humidified 5% CO2 atmosphere. The medium was changed after 2 days to allow cell adhesion and to remove the nonadherent cells. When the cells reached 80%–90% confluence after 14 days (passage 0), they were washed twice with PBS and detached by incubation with trypsin–EDTA (0.25% trypsin, 0.53 mM EDTA; Life Technologies) for 5 min, and then they were washed twice with the culture medium. The resuspended cells in the growth medium were plated at 2×104 cells/150 mL.
Culture of SDSCs in COL/HA/FG composite gel
When the cells of the second passage reached 80%–90% confluency, they were trypsinized using 0.25% trypsin/EDTA and counted using a hemocytometer. After centrifugation, the cell pellets were resuspended at a concentration of about 2×107 cells/mL in the prepared COL/HA/FG solutions (COL/HA/FG-3 and COL/HA/FG-4) according to the procedure described above. The COL/HA/FG composite gels containing the SDSCs were transferred to six-well culture plates and cultured in a chemically defined chondrogenic medium consisting of a low-glucose DMEM supplemented with 100 μM ascorbate-2-phosphate, 100 μg/mL pyruvate, 40 μg/mL proline, 100 nM dexamethasone, antibiotic–antimycotic solution, and an ITSTM + premix universal culture supplement. After 24 h of incubation at 37°C in an atmosphere of 5% CO2, the medium was replaced with a chondrogenic medium supplemented with 100 ng/mL of bone morphogenetic protein-2 and 10 ng/mL of transforming growth factor-beta 1. The plates were maintained at 37°C in an incubator with a medium change every 3 days.
Cell proliferation and viability assay
The proliferation assay was carried out using the 3-(4,5-dimethylthiazol-2yl)-5-(3-carboxymethoxyphenyl)-2-(4-sulfophenyl)-2H-tetrazolium, inner salt (MTS) assay available in a commercial kit (Promega) according to the manufacturer's instructions. At day 1, 7, 14, and 28 of cultivation, the SDSCs encapsulated within the COL/HA/FG composite gels were digested with 100 μL of 0.1% collagenase (Sigma-Aldrich) for 3 h at 37°C in a 5% CO2 atmosphere in the low-glucose DMEM containing 1% antibiotic–antimycotic solution and 20 μL of CellTiter 96® AQueous One Solution Reagent (Promega) that contained the MTS tetrazolium compound and an electron coupling reagent (phenazine ethosulfate). After incubating for 1.4 h at 37°C in a 5% CO2 atmosphere, the absorbance of the formazan product was measured at a wavelength of 490 nm using a VersaMas 96-well plate (microplate spectrophotometer; Molecular Devices Corp.). The viability of encapsulated SDSCs within the COL/HA/FG composite gel was assessed using the Live/Dead Viability kit (Molecular Probes) according to the manufacturer's instructions. Samples at day 1, 7, 14, 21, and 28 after cultivation were treated in a solution containing 2 mM ethidium homodimer-1 and 4 mM Calcein AM in PBS for 40 min. After washing in PBS, thin slices of the stained samples were prepared on glass slides and they were observed using a fluorescence microscope. Live cells were visualized by a green color and dead cells were visualized by a red color.
Determination of the glycosaminoglycans content
The dimethylmethylene blue (DMB) method was used for the detection of the total glycosaminoglycan (GAG) contents in the COL/HA/FG composite gels. At day 0, 14, and 28 after cultivation, the COL/HA/FG composite gels containing the SDSCs were digested for 12 h with a papain solution (200 μg/mL papain, 5 mM L-cysteine, 100 mM Na2HPO4, and 50 mM EDTA) at 55°C. After centrifugation, 50-μL aliquots of the papain-digested extracts were pipetted into each well of 96-well plates and 250 μL of the DMB dye solution was added. The absorbance of these extracts was determined using an ELISA reader at 530 and 590 nm, and were compared to the absorbance of standard chondroitin-6-sulfate. The total GAG quantities per sample were then normalized by their DNA contents as determined using an indole assay. After the DMB assay, the COL/HA/FG composite gels were treated with 100 μL of 1 N NaOH and 100 μL of indole reagent and then incubated for 10 min at 100°C. The absorbance of these solutions was determined at 490 nm.
Reverse transcription–polymerase chain reaction and quantitative real-time PCR analysis
Total mRNA was isolated using a RNeasy mini kit (Qiagen). RT was conducted on 1 μg of RNA using a First strand cDNA synthesis kit (Fermentas Life Sciences). PCR amplification of the resulting cDNA was performed using AccuPower® PCR PreMix (Bioneer). cDNAs were subjected to PCR amplification in the presence of the following specific primer sets: 5′-CGTGGTGACAAGGGTGAGAC-3′ and 5′-TAGGTGATGTTCTGGGAGGC-3′ for type I COL, 5′-TTCAGCTATGGAGATGACAATC-3′ and 5′-AGAGTCCTAGAGTGACTGAG-3′ for type II COL, 5′-CCCTTTTTGCTGCTAGTATCC-3′ and 5′-CTGTTGTCCAGGTTTTCCTGGCAC-3′ for type X COL, 5′-TGAGGAGGGCTGGAACAAGTACC-3′ and 5′-GGAGGTGGTAATTGCAGGGAACA-3′ for aggrecan, 5′-CCCGATCTGAAGAAGGAGAGC-3′ and 5′-GTTCTTCACCGACTTCCTCCG-3′ for Sox9. PCR fragments were normalized with the levels of glyceraldehyde-3-phosphate dehydrogenase (GAPDH; 5′-ATTGTTGCCATCAATGACCC-3′ and 5′-AGTAGAGGCAGGGATGATGTT-3′). PCR reactions were allowed to proceed for 30 cycles. PCR products were separated by 1.5% agarose gel electrophoresis, and DNA bands were visualized with ethidium bromide. Signals were observed using a Gel Doc 2000 low light imaging system (BioRad). A densitometric computer program (TINA; Raytest Isotopenmeßgerate) was used to scan the reverse transcription–polymerase chain reaction (RT-PCR) agarose gel after photographic documentation. The program measured the relative mean density after correcting for background density, and the expression of marker genes was calculated as the percentage of the expression of GAPDH.
RNA isolation and cDNA synthesis for real-time PCR were performed as described above. For the SDS 7000 system reactions, a master mix of the following components was prepared to the indicated end concentration and then analyzed on an ABI Prism 7000 Sequence Detection System (Perkin-Elmer Applied Biosystems): 6.25 μL water, 1.25 μL primer (9 μM), and probe (2.5 μM) and 12.5 μL TaqMan PCR 2×master mixture (Perkin-Elmer Applied Biosystems). Five microliters of complementary DNA was added as a PCR template. The PCR conditions were as follows: after the initial activation of uracyl-N-glycosylase at 50°C for 2 min, AmpliTaq Gold was activated at 95°C for 10 min; the subsequent PCR condition consisted of 45 cycles of denaturation at 95°C for 15 s and annealing extension at 60°C for 1 min per cycle. During the PCR amplification procedure, the amplified products were continuously measured by determination of the fluorescence emission. The levels of the target gene expression were analyzed using the 2-ΔΔCT method and they were normalized to a human GAPDH endogenous control (VIC/MGB Probe, Primer Limited; Perkin-Elmer Applied Biosystems), and the levels were presented as the relative expression. The PCR primer and probe sets for type I COL (CCGATGGCTTCCAGTTCGAGTACGG), type II COL (GGCGACGGCCCCCACGCCCACTCGC), type X COL (ACTGCAAGGAGAGCCAGGGTTGCCA), aggrecan (GATGGAGGGTGAGGTCTTTTACG), and sox 9 (CCTCGGGAAGCTCTGGAGACTGCTG) were designed using the Primer Express software (Perkin-Elmer Applied Biosystems).
Surgical procedure
New Zealand white rabbits (8-month-old males weighing 3.5–4.0 kg) were anesthetized with an intramuscular injection of ketamine hydrochloride (35 mg/kg; Yuhan) and xylazine hydrochloride (5 mg/kg; Bayer), and anesthesia was maintained with isoflurane. The knee joints were approached through medial parapatellar incisions, and the patella was reflected laterally to expose the femoral articular surface of the patellofemoral joint of rabbits. A full-thickness osteochondral defect 4 mm in diameter and 3 mm in depth was made in the patellar groove of the distal femur using a hand drill with a depth stop. Before transplantation, the joints were thoroughly rinsed with sterile saline. The harvest of synovial tissues was performed 2 weeks before the joint surgery in the rabbits, and then isolated SDSCs were cultured in the DMEM medium. Because SDSC transplants would be autologous, careful monitoring of individual animal source was maintained at all times during SDSC processing. Sixty rabbit knee joints were divided into three groups as follows. The osteochondral defect in the left knees of the control group (n=20) was not treated with the COL/HA/FG-4 composite gel; they served as sham controls. The osteochondral defect in knees (right or left) of the Gel group (n=20) was filled with the COL/HA/FG-4 composite gel (150 μL/defect). The osteochondral defect in the right knees of the Gel/SDSC group (n=20) was filled with the COL/HA/FG-4 composite gel loaded with autologous SDSCs (2×107 cells/mL, 150 μL/defect). The COL/HA/FG-4 composite gel, with or without loaded autologous SDSCs, and thrombin solution were injected using a dual syringe with a 23-gauge needle into the left or right knee until the defect was filled. These COL/HA/FG-4 composite gels gelled and bonded to the adjacent cartilage and bone within about 5 min after injection. The soft tissue over the defect and the skin were closed with nylon sutures. Postoperatively, all the rabbits were allowed to move freely in the cage. The rabbits were sacrificed with an overdose of ketamine solution at 4 and 24 weeks after the surgery (n=8 at each time point).
Macroscopic examination
After sacrifice at 4 and 24 weeks, the knee joints were opened, the area of the femoral defect was photographed, and gross examination was performed. Digital images were taken using a Canon EOS-450D digital camera (Canon Korea Consumer Imaging, Inc.). The gross appearance of the defects was assessed by three blinded independent researchers using an established eight-point grading scale. 23
Histological and immunohistochemical examination
The entire knee was dissected after macroscopic observation, and the femurs were fixed in 10% buffered formalin for 5 days, and decalcified with Decal Rapid decalcifying agent (National Diagnostics) for 2 days, dehydrated with a graded series of ethanol solutions, and then embedded in paraffin. Sagittal sections (5-μm thick) were stained with hematoxylin and eosin (H&E) and safranin-O/Fast Green. The stained sections were subsequently analyzed under a model BX 51bright-field microscope (Olympus). The histomorphologic findings (n=8 at each time point) for each section were evaluated in a blinded manner and independently scored by three investigators according to the O'Driscoll histological grading scale. 24 The total score ranged from 0–28 points, with a lower score indicating better repair of tissues.
For the immunohistochemistry, serial sections were used for the detection of type II COL. The sections were deparaffinized with xylene, rehydrated through a decreasing gradient of ethanol solutions, and rinsed three times with PBS. The endogenous peroxidase activity was blocked with 0.5% hydrogen peroxide in methanol, and the sections were washed in 0.1% bovine serum albumin in PBS. The sections were then treated with 500 U/mL testicular hyaluronidase (Sigma-Aldrich). Nonspecific staining was reduced by incubation with horse serum. The sections were incubated overnight at 4°C with the antibody against type II COL (dilution 1:100). Antibody binding was visualized by using the Vectastain avidin–biotin peroxidase complex kit (Vector Laboratories) in combination with the diaminobenzidine solution according to the manufacturer's instructions. The sections were counterstained with hematoxylin. As a negative control, the primary antibody was omitted from the immunohistochemical protocol.
Statistical analysis
All the results are reported as the mean±standard deviation. The Mann–Whitney U test was used to determine the statistical significance of the differences in the mean values between the different groups. All of the analyses were performed using SPSS 12.0 for Windows software (SPSS). p-values<0.05 were considered to be significant.
Results
Degradation assay of COL/HA/FG composite gels
Degradation rate of the FG gel, the HA/FG and COL/FG composite gels (200 μL) was evaluated in PBS containing lysozyme at 37°C at predetermined time intervals. As shown in Figure 1A, weight loss of the FG gel was significantly delayed compared with that in the HA/FG and COL/FG composite gels (*p<0.05) and remained at about 31.5%±4.59% of the initial weight at 28 days. Both the HA/FG and COL/FG composite gels lost their weights in PBS very rapidly during 14 days, at which only 35.9%±5.67% and 37.2%±5.38%, respectively, of the initial weights were preserved. After 14 days, the degradation of these gels decreased slowly, and their weights remained at 21.30%±4.91% and 22.24%±3.81%, respectively, of the original gel weight at 28 days. Degradability of the COL/HA/FG tri-composite gels was performed in PBS containing lysozyme at 37°C as shown in Figure 1B. The COL/HA/FG composite gels containing more FG showed a slower rate of weight loss than the COL/HA/FG composite gels with less FG. The curves shown in the figure could also be divided into two groups. In the first group with a low amount of FG, the weight loss of the COL/HA/FG-1 and -2 composite gels increased sharply and was ∼10.7%±3.52% and 12.1%±3.67%, respectively, after 28 days. In the second group with a high amount of FG, the weight loss ratio between the COL/HA/FG-3 and -4 composite gels was slightly increased, and the value of weight loss was less than that in the first group after 28 days (29.3%±3.81% and 29.5%±6.92%, respectively, **p<0.01: first group vs. the second group). The results of in vitro degradation indicated that the degradation of COL/HA/FG composite gels depended on the extent of FG. The results supported the idea that both the COL/HA/FG-3 and the COL/HA/FG-4 composite gels can be an appropriate SDSC delivery vehicle.
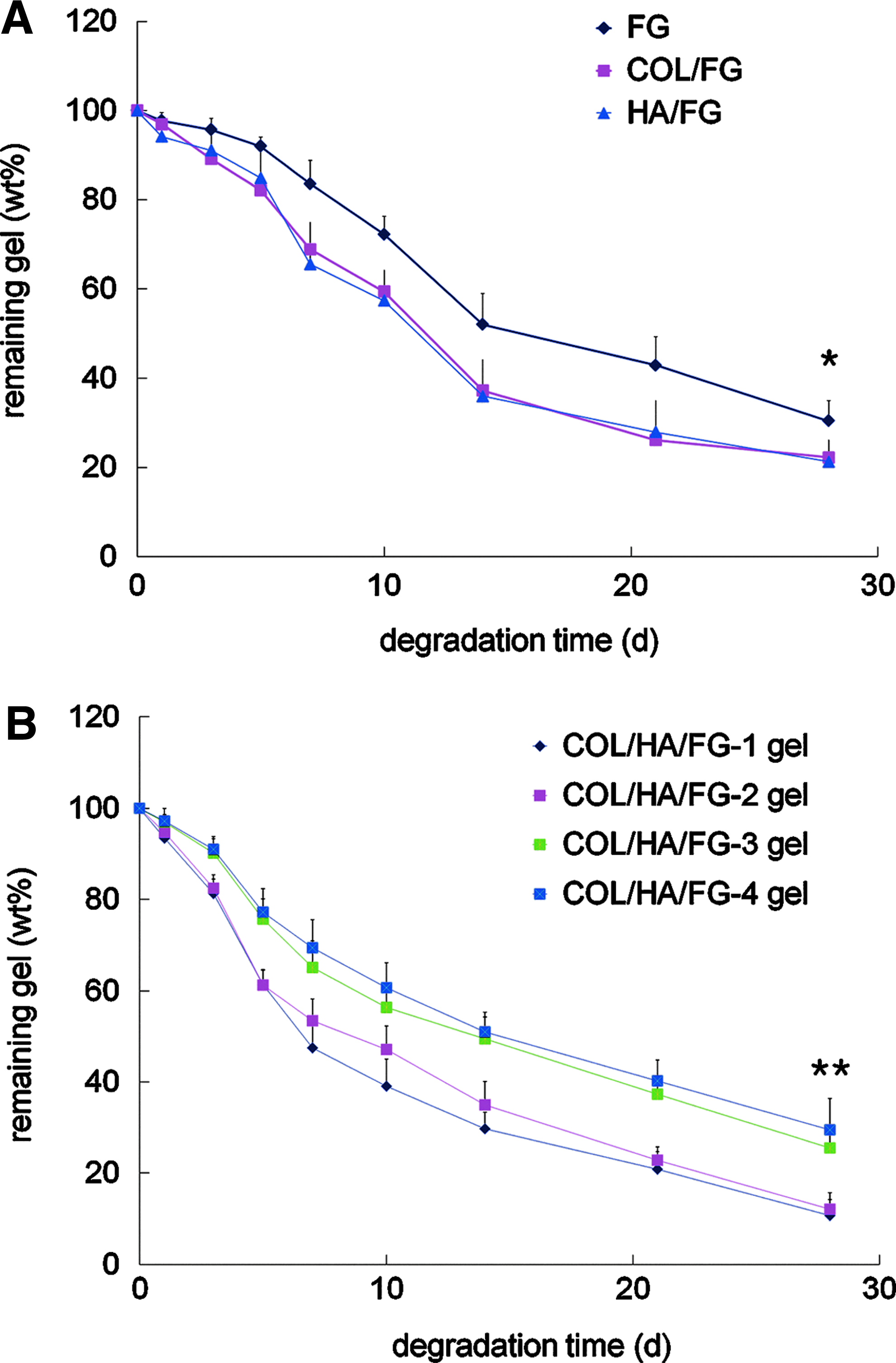
In vitro degradation of composite gels.
Proliferation and viability of SDSCs
The proliferation of the SDSCs encapsulated in both the COL/HA/FG-3 composite gel and the COL/HA/FG-4 composite gel was evaluated by the MTS assay at day 1, 7, 14, 21, and 28 after cultivation (Fig. 2A). The proliferation rate of SDSCs in the COL/HA/FG-3 composite gel was similar to that of SDSCs in the COL/HA/FG-4 composite gel. The number of SDSCs showed a relatively slow increase up to day 14, and thereafter decreased marginally up to day 28; the difference was not statistically significant. The viability of SDSCs encapsulated in the COL/HA/FG-4 composite gel was confirmed by the Live/Dead stained assay at day 1, 7, 14, 21, and 28 after cultivation (Fig. 2B). Fluorescence staining revealed a uniform distribution of the cells throughout the COL/HA/FG-4 composite gel and high cell viability (>95%, green color) for 14 days after encapsulation, which indicated that the gel was nontoxic to the encapsulated SDSCs. The cell viability inside the COL/HA/FG-4 composite gel started to decrease after 14 days; the percentage of viable cells was ∼92%±4.1% of the entire cell population in the COL/HA/FG-4 composite gel at day 28 of cultivation. Cell viability in both the COL/HA/FG-3 and the COL/HA/FG-4 composite gels was not significantly different (data not shown).

Proliferation and appearance of encapsulated rabbit SDSCs.
Gene expression analysis
Figure 3A shows the mRNA expression patterns of SDSCs encapsulated in the COL/HA/FG-3 and -4 composite gels at day 28 after cultivation, as determined by RT-PCR. In the COL/HA/FG-4 composite gel group, the expression of type II COL and sox 9 mRNA were significantly increased, but the gene expression of type X COL was markedly decreased as compared to that in the COL/HA/FG-3 composite gel group. On the other hand, the expression of the genes encoding type I COL and aggrecan showed a slight decrease, but the difference was not statistically significant. The mRNA expressions of chondrogenesis-related genes were confirmed by real-time PCR in the COL/HA/FG-4 composite gel group (Fig. 3B). When cultured in the COL/HA/FG-4 composite gel, the expression of the genes encoding type II COL, aggrecan, and sox 9 was significantly increased from day 14–28 after cultivation. At 28 days after cultivation, the gene expressions of type II COL, aggrecan, and sox 9 were increased 1.4-fold, 11-fold, and 18.6-fold, respectively, compared to that on day 0 (***p<0.001). The expression of the genes encoding type I COL was slightly increased at day 14, but was decreased at day 28 after cultivation. On the other hand, the gene expression of type X COL was slightly increased from day 14–28 after cultivation. However, the difference between these gene expressions was not statistically significant.

Results of gene expression analyses.
GAG content and immunohistochemistry
The ratio of GAG to DNA, a chondrogenic differentiation index, showed that the GAG synthesis from the SDSCs encapsulated in the COL/HA/FG-3 and -4 composite gels was significantly increased at both days 14 and 28 as compared to that on day 1 after cultivation (***p<0.001). The COL/HA/FG-4 composite gel group also had greater GAG accumulation by day 28 compared to day 14 samples (*p<0.05). The GAGs' contents (μg of sGAG/μg of DNA) at 28 days were 2.87±0.58 in the COL/HA/FG-3 composite gel group and 3.47±0.44 in the COL/HA/FG-4 composite gel group (Fig. 4A). The specimens of the aforementioned COL/HA/FG-4 composite gel group were examined for lacunae formation and accumulation of sulfated GAGs by safranin-O staining (Fig. 4B) at 28 days after cultivation. The H&E stained images are not presented in Figure 4B because the distribution of lacunae was also observed in the safranin-O stained images. When the SDSCs encapsulated in the COL/HA/FG-4 composite gel were cultured, the formation of cartilage-specific lacunae around the cells was apparent. The extracellular region was strongly stained by the characteristic red of safranin-O, indicating the presence of a proteoglycan-rich matrix. Similar to the safranin-O staining results, intense immunostaining for type II COL was observed. The results supported the suggestion that the COL/HA/FG-4 composite gel strongly supports chondrogenic differentiation of SDSCs.
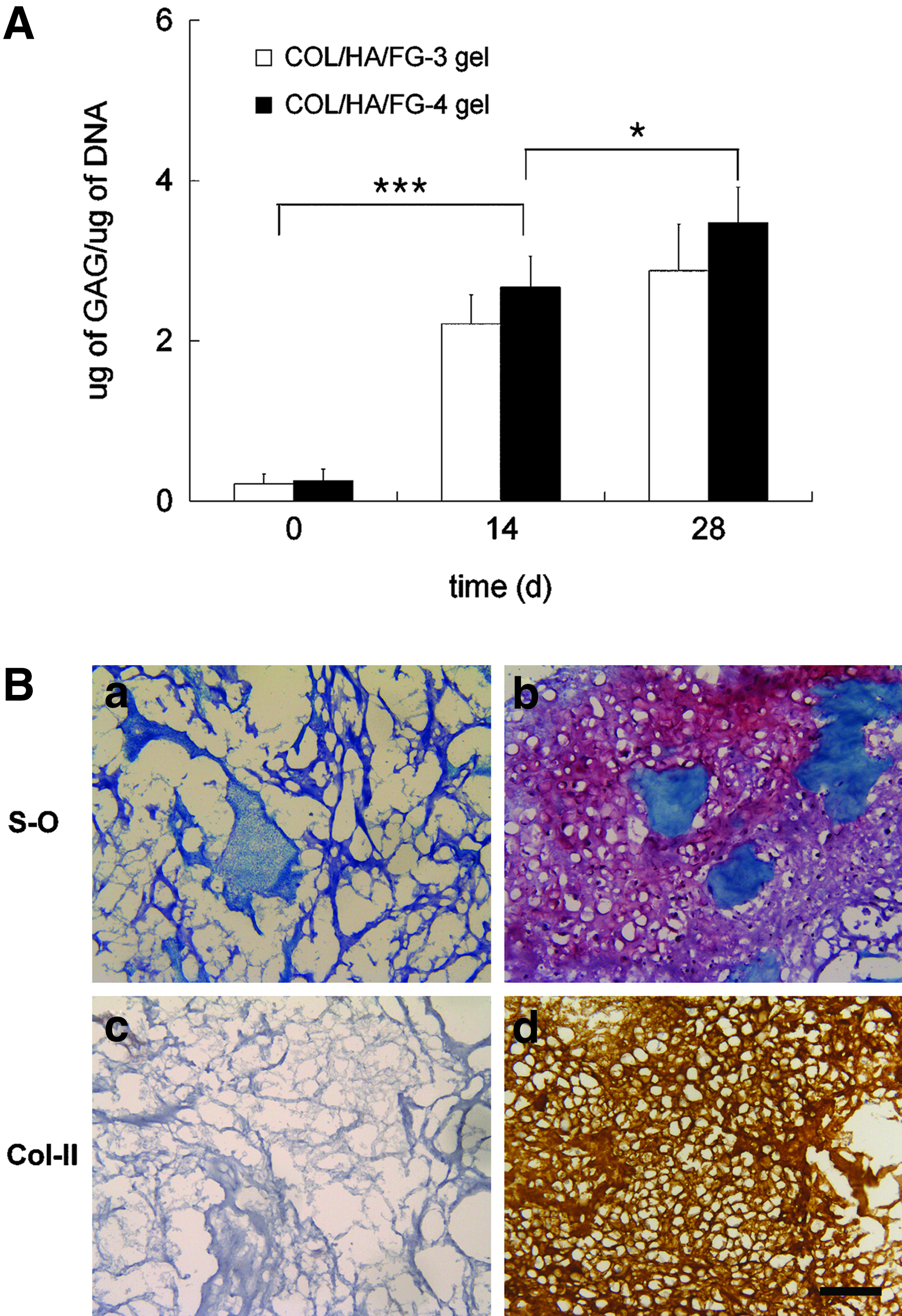
GAG/DNA, histology, and immunohistological data of encapsulated rabbit SDSCs.
Macroscopic findings from in vivo experiments
Postoperatively, the joints and incision areas in all the experimental groups appeared normal on gross examination, and no adverse immune reaction or infection was confirmed throughout the experiments. The representative gross appearance of the repaired tissue at 4 and 24 weeks after surgery is shown in Figure 5A. At 4 weeks after the surgery, the regenerated areas of the control groups were red or dark brown. Irregular tissue with depressions was noted and the margin of the defect was clearly differentiated from the surrounding normal cartilage (Fig. 5A-a). In the Gel and the Gel/SDSC groups, the repaired tissue was filled with smooth, white tissue, which was distinguished from the margins of the intact cartilage (Fig. 5A-b, 5A-c). At 24 weeks after the surgery, the defect of the control groups was only covered with white tissue, which was not cartilage-like in appearance. This white tissue was barely distinguishable from the surrounding normal cartilage and had irregular surfaces. In addition, there was a depression in the center of the repaired surface (Fig. 5A-d). In the Gel and Gel/SDSC groups, the repaired tissue became opaque and was completely integrated into the surrounding normal cartilage. It was difficult to discern the boundary between the host tissue and the repaired tissue. In some cases of the Gel group, the central area of the defect was slightly depressed (Fig. 5A-e). Yet, the defect in the Gel/SDSC group was filled with the repaired tissue that resembled hyaline cartilage (Fig. 5A-f).

Examination of osteochondral defect repair.
Macroscopic scores of the in vivo experiments
The macroscopic scores for the control group, the Gel group, and the Gel/SDSC group were 1.33±1.03, 4.33±1.03, and 5.00±0.89 at 4 weeks and 3.83±1.47, 5.50±1.87, and 7.00±1.10 at 24 weeks, respectively. Regarding the comparison among the experimental groups, the total macroscopic scores at 4 weeks postoperatively were significantly higher in the Gel and Gel/SDSC groups than in the control group (*p<0.05). At 24 weeks, the values in the Gel and Gel/SDSC groups were significantly higher as compared with those in the control group (**p<0.01: the Gel/SDSC group vs. the control group, *p<0.05: the Gel group vs. the control group, Fig. 5B).
Histological findings
At 4 weeks after the surgery, the surface of the regenerated tissue remained concave in both the control and experimental groups. The untreated groups were characterized by fibrous tissue and blood clots stemming from the perforated marrow vasculature. Undifferentiated spindle-shaped cells appeared at the periphery of the defect, and the center of the defect showed a blood clot with eosinophilic staining (Fig. 6a–c). The findings of the Gel and Gel/SDSC groups were similar to those of the control group. The defects showed the transplanted gel at the center of the regenerated tissue. In the Gel/SDSC group, at higher magnification, many elongated cells located near the trabecular bone surface were gradually surrounded and replaced by cartilaginous tissue, which was gradually replaced by the appositional growth of the subchondral bone (Fig. 6d–i, see also Appendix Fig. A1).
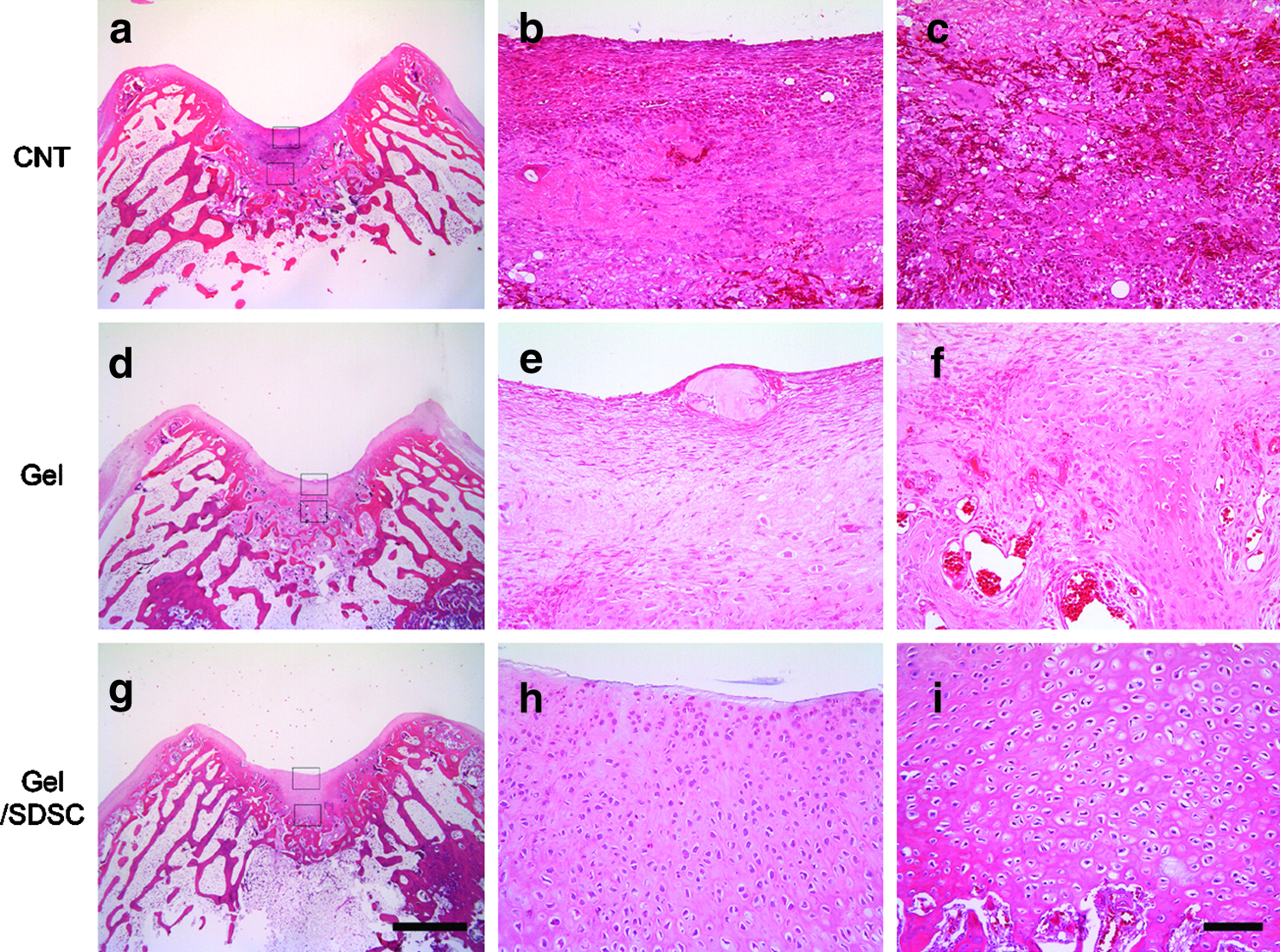
Histological appearance of the defects on the trochlear groove (4-mm diameter) at 4 weeks after surgery (H&E stain). The defect in the control group was almost filled with undifferentiated spindle-shaped cells and blood clots with eosinophilic staining
At 24 weeks after the surgery, none of the cases in the control group healed completely with hyaline-like cartilage. The surface of the regenerative tissue was irregular and the regenerative tissue varied from fibrous to fibrocartilaginous tissue. The repaired tissue was obviously thicker than the surrounding cartilage and it had incomplete integration with the surrounding cartilage. The subchondral plate had not been reconstituted properly; the defect tissue extended down to the subchondral space. Furthermore, at high magnification, compared with the surrounding articular cartilage, the round cells in the repaired tissue were clustered and the arrangement seemed to be more irregular (Fig. 7a–c). In the Gel group, the transplanted area was mostly repaired by cartilage-like tissue, although the surface region of the repaired tissue exhibited a fibrocartilage-like appearance. The subchondral bone was well-reconstituted, and the defect tissue did not extend down to the subchondral space. High magnification of the defect revealed that the interface between the adjacent tissue and the repaired tissue showed a lack of integration of the repaired tissue. The round cells appeared to have an irregular arrangement in the repaired tissue (Fig. 7d–f). In the Gel/SDSC group, the transplanted area was mostly repaired by a cartilage-like tissue with a thickness equivalent to that of the surrounding original cartilage. At higher magnification, complete integration was observed at the border between the regenerative tissue and the adjacent host original cartilage. The cells had a columnar alignment, and were similar in morphology to normal chondrocytes. The deeper portion of the defects had been almost completely replaced by bone, and the subchondral bone and tidemark were well remodeled without loss or alteration of the overlying articular cartilage (Fig. 7g–i).
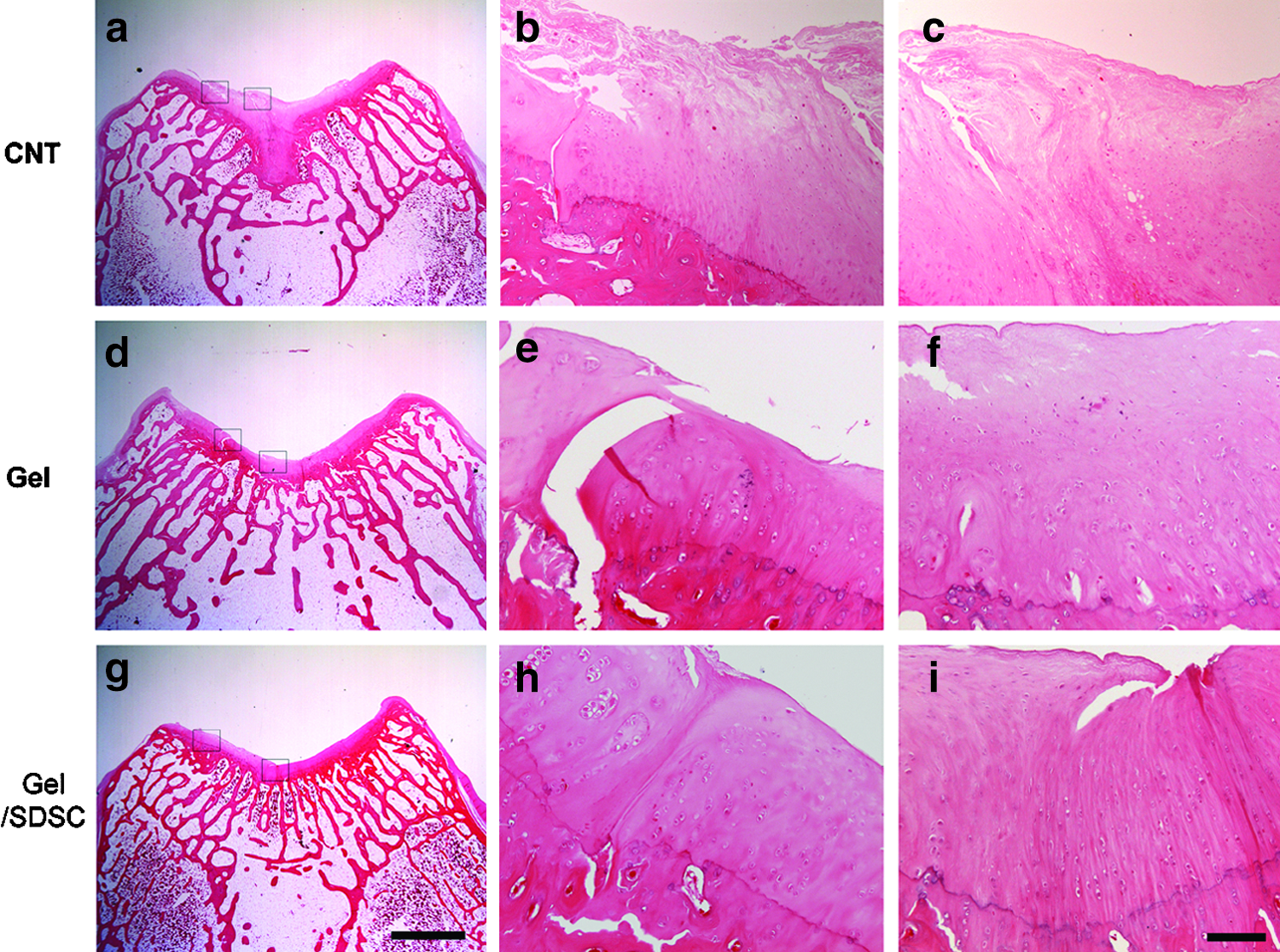
Histological appearance of the defects on the trochlear groove (4-mm diameter) at 24 weeks after surgery (H&E stain). None of the cases in the control group healed completely with hyaline-like cartilage
Histochemical and immunohistochemical findings from in vivo experiments
As assessed histochemically, in the control group, the cartilage tissue developed in the subchondral bone area and it occupied less than two-thirds of the whole defect, and was negative for safranin-O (Fig. 8a) and type II COL (Fig. 8d) staining at 24 weeks. However, in the Gel and Gel/SDSC groups, the newly formed cartilage tissue on the whole defects had an appearance of hyaline cartilage that was densely stained by safranin-O (Fig. 8b, c) and type II COL immunostaining (Fig. 8e, f).
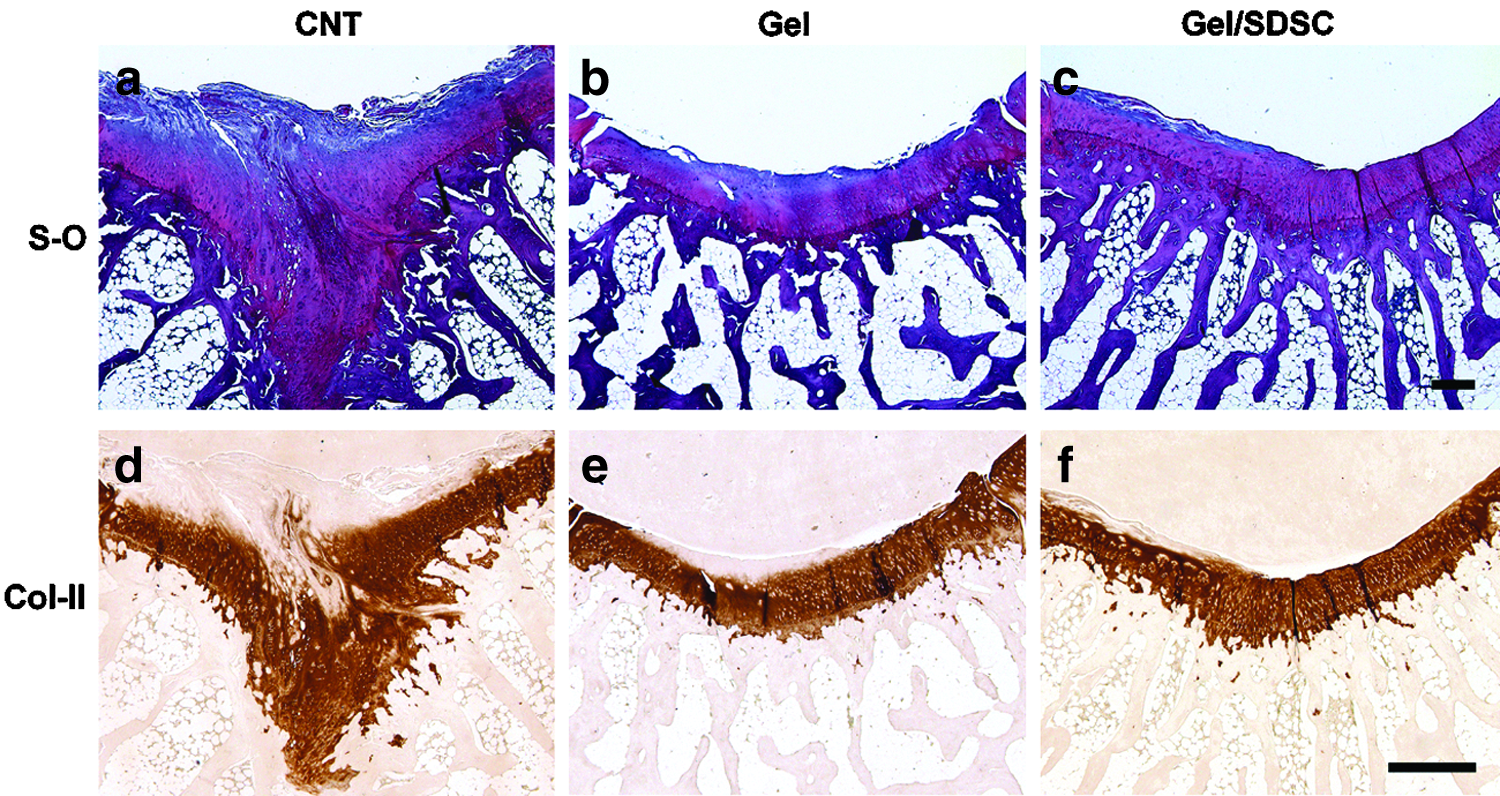
Histochemical and immunohistochemical appearance of the defects on the trochlear groove (4-mm diameter) at 24 weeks after surgery. In the control group
Microscopic scores of the in vivo experiment
The O'Driscoll histological scores for the control group, Gel group, and Gel/SDSC group were 4.50±1.80, 8.33±2.94, and 10.00±2.36 at 4 weeks and 13.00±2.76, 19.67±2.88, and 23.17±2.23 at 24 weeks, respectively. At 4 weeks after the operation, the total histological scores in the Gel group were significantly higher than those in the control group (*p<0.05, **p<0.01, respectively, Table 2). Among the categories in the scoring system, the surface regularity in the Gel/SDSC group was significantly superior to that in the control group (**p<0.01). From 4–24 weeks postoperatively, the total histological scores in all groups tended to improve with statistical significance. The total histological scores at 24 weeks were significantly higher in the Gel and Gel/SDSC group than in the control group (Table 2). Regarding the comparisons of each category, the scores of the Gel/SDSC group were significantly higher than those of the control group in 7 of 11 categories.
The treatment groups that showed significant improvement compared with that of the control at p<0.05 and p<0.01 were marked with a and b. X, statistical analysis was not performed because the standard deviation of at least one group is zero.
CNT, control; SDSCs, synovium-derived mesenchymal stem cells.
Discussion
The aims of this study were to determine the in vitro and the in vivo effectiveness of an injectable COL/HA/FG composite gel encapsulated with SDSCs to enhance the healing of the rabbit osteochondral defect.
Previous studies have indicated that SDSCs are a promising cell source for the repair and regeneration of articular cartilage.8,9,25 Unlike chondrocytes, the use of SDSCs is not prevented by the limited availability of healthy articular cartilage or an intrinsic tendency of the cells to lose their phenotype during expansion, and the use of SDSCs avoids the morbidity caused by damage to the donor-site articular surface. Synovium may serve as a source of MSCs that are mobilized following injury, and the MSCs migrate to the wound site where, they participate in the repair response. After partial-thickness chondral defects were created in the rabbit articular cartilage, a continuous layer of MSCs extending from the synovium was found to contribute to cartilage regeneration. 26 We have previously shown that the SDSCs can be expanded in culture and differentiated into the desired lineage with the application of specific growth factors. 27 Although the reparative potential of SDSCs and bone marrow-derived MSCs (BM-MSCs) is similar, an in vivo chondrogenic assay demonstrated that SDSCs produce more cartilage matrix than BM-MSCs.8,9 Furthermore, SDSCs can proliferated much faster than BM-MSCs when cultured with autologous human serum. 28 To regenerate damaged articular cartilage, it is necessary to identify an appropriate cell source that is easily accessible, can be expanded to large numbers, and has chondrogenic potential. Therefore, we believe that SDSCs are the most clinically promising source of stem cells to develop new strategies for cartilage regeneration. SDSCs have recently been explored as an alternative cell source for cartilage regeneration and repair because of their chondrogenic potential and their ease of isolation from sources, such as joints, without damage to the native cartilage tissue.8,9 In an in vitro study, we showed that the reconstructed tissue derived from the SDSC-encapsulated COL/HA/FG composite gel resembles native hyaline cartilage both biochemically and histologically.
In recent attempts to regenerate the articular cartilage, injectable hydrogel-type scaffolds have been shown to be an effective culture system for chondrogenic differentiation of MSCs because these scaffolds have mechanical and structural properties that are similar to components of the extracellular matrix.29,30 Of the various scaffold materials, COL is a predominant component of the extracellular matrix in bone and cartilage, and it helps regulate cell growth and differentiation. Due to its biocompatibility, COL has been used as a scaffold in constructing a three-dimensional cell culture system, and has demonstrated its ability to maintain a chondrocytic phenotype. 11 Previous studies have shown that MSCs embedded in COL type I gels are able to undergo chondrogenic differentiation in vitro and in vivo.31,32 Furthermore, a cartilage defect was partially repaired when autologous culture-expanded MSCs engineered in a COL type I gel were transplanted into an osteoarthritic knee. 16 Thus, COL is essential for maintaining the homeostasis of MSCs, and it could possibly be a good candidate as a scaffold for a three-dimensional culture system of MSCs. However, previous results using the type I COL gel showed limited repair with incomplete integration of the neocartilage with the surrounding cartilage as well as high variability within groups. In addition, cysts formed in the subchondral bone, which the authors attributed to a lack of mechanical support from the COL gels. 33 HA is a major component of the cartilage ECM and is expected to provide a favorable environment for chondrogenesis of MSCs. 34 The pivotal role of HA on chondrocytes and cartilage metabolism have been reported, including cell attachment, proteoglycan organization, and differentiation.35,36 In addition, HA might modulate the degradation rate of fibrin because FG can specifically bind to HA. 37 Its biological properties and rapid degradation makes HA an ideal candidate for the development of new biomaterials. 18 Fibrin is another class of tissue-derived natural material that can be utilized to a three-dimensional scaffold. Fibrin is a protein that is involved in the clotting of blood, and it is formed by polymerization of FG in the presence of thrombin. Various studies have reported the use of a fibrin gel as a cell delivery matrix for generating a new cartilage matrix.38,39 Moreover, FG promotes the proliferation and gene expression of MSCs. 40 However, weak mechanical properties, shrinkage of the gel, and early degradation of fibrin have been problematic. 17 Recently, it has become common to combine two biomaterials to utilize the advantages of each biomaterial. For example, the addition of HA to COL I gels increased markers of cartilage formation by encapsulated chondrocytes in a subcutaneous implantation model. 41 Fibrin gels mixed with HA provide a favorable environment for chondrocytes to maintain a stable phenotype and to synthesize cartilage ECM in nude mice. 42 Furthermore, fibrin gels with COL allow stable graft fixation in a chicken model of cartilage repair. 43 However, previous reports have indicated that a gel scaffold composed of both HA and fibrin drastically shrank within a few days. 44 Therefore, to improve the quality of the gel, we added type I COL to the HA/FG gel. With this new gel composition, we observed no shrinking effects. Furthermore, the COL/HA/FG composite gel showed superior chondrogenesis, as indicated by the real-time PCR results, GAG content and immunohistochemical staining for higher expression of type II COL.
Hydrogel-type scaffolds have the ability to be injected into the defect as a solution and to form a gel immediately after injection, thus they can be easily applied to the irregular defect in a minimally invasive manner.10,45 In the present study, the mixture of SDSCs and the COL/HA/FG composite gel solution were immediately permeated into the defect, gelled within 5 min, and then bonded to the adjacent cartilage and cancellous bone. Such rapid gel formation is mediated by chemical reactions between FG and thrombin. Besides that, the COL/HA/FG components used in these applications appeared to gel without damaging the cells. After gelation, the scaffolds need to be maintained for several weeks so that cells can support the physical structure. Thereafter, when the tissues are regenerated, the scaffolds should be degradable. An inappropriate degradation rate of scaffolds would substantially affect cell survival and activity. 12 Thus, the degradation properties of materials are also important because they determine the changes in the structural and physical properties of the gels. Variation of FG concentration can generate gels with different mechanical properties and stability. 46 A previous study reported two different types of fibrin gels controlled by the concentration of FG. At higher FG concentration, the fibrin gels became rigid gels with small pores. In contrast, at lower FG concentration, they were composed of loose gels with a larger pore size. 47 The present study shows that the degradation properties of the COL/FG/HA composite gel can be controlled easily by altering the FG component of the gels (Fig. 1). Thus, stabilization of the SDSC-encapsulated COL/HA/FG composite gel by addition of high concentration of FG is a feasible method for three-dimensional formation of cartilaginous tissue in vitro. However, the low level of FG may have resulted in higher rates of polymer degradation and may be responsible for the inability of the tissue-engineered cartilage to maintain its contour. During this study, we observed that the SDSC-encapsulated COL/HA/FG-1 and -2 composite gels were dissolved too early, before cartilaginous tissue formation could occur (data not shown). The present results of in vitro degradation suggest that the degradation of the COL/FG/HA composite gel depends on the extent of FG. In the animal study, the transplanted COL/HA/FG composite gel had almost disappeared by 4 weeks postoperatively, suggesting that the degradation of gel may require 4 weeks after transplantation. The in vivo degradation study showed good agreement with the in vitro study.
Among the different types of scaffolds, injectable hydrogel-type scaffolds are of interest for the encapsulation of cells to mimic the three-dimensional environment of cells, thereby facilitating the transport of nutrients to the cells encapsulated in the hydrogel-type scaffolds.48,49 Additionally, a three-dimensional environment involving cell/cell or cell/matrix interactions is required for proper chondrogenic differentiation. Our subsequent objective was to determine whether our COL/HA/FG composite gel could be a suitable scaffold for supporting the chondrogenic differentiation of SDSCs. When placed in chondrogenic conditions, SDSCs cultured within COL/HA/FG composite gels were still able to undergo chondrogenic differentiation. The major chondrocyte phenotypic markers (type II COL, aggrecan, and sox 9) were expressed at the mRNA level. Moreover, sulfated GAGs and type II COL accumulated within the extracellular matrix. These data demonstrate that the COL/HA/FG composite gel is a biomaterial that provides a three-dimensional environment that is able to support the in vitro chondrogenic differentiation of SDSCs. Consequently, the combination of COL/HA/FG may mimic the cartilage extracellular matrix, providing a chondrogenic environment for the encapsulated SDSCs.
Although injectable hydrogel-type scaffolds that are composed of two materials have been examined for regenerating damaged articular cartilage,45,38,50 they have not yet been adopted except for subcutaneous injection of gel into the backs of mice. 51 To determine whether the SDSC-encapsulated COL/HA/FG composite gel could be an appropriate device for articular cartilage repair, we created osteochondral defects in rabbits and then treated them with this gel construct. The control defects that were left empty displayed the formation of fibrocartilaginous repair tissue, which had inferior mechanical properties than the healthy cartilage. Interestingly, the SDSC-encapsulated COL/HA/FG composite gel led to the formation of repair tissue that produced GAG and type II COL. Furthermore, this repair tissue displayed a specific tissue organization resembling that of the native articular cartilage. No immunological or inflammatory reactions were encountered after transplantation throughout the experiment. Thus, in part, COL/HA/FG composite gel contributed to the successful cartilage regeneration in this study. However, the effects of transplanted SDSCs on regenerated cartilage after transplantation remain unknown as the fate of these cells was not investigated in this study. Therefore, we need to further investigate the biomechanical roles of these SDSCs. We only performed a histological evaluation of the repaired tissue for up to 24 weeks after transplantation. Further, biochemical or biomechanical analyses of the reparative cartilage for longer time periods will be necessary. We think that it will be necessary to compare our findings with those of a control group treated with a contemporary technique, such as microfracture, as the next step of our study.
Conclusions
The aim of the present study was to fabricate and characterize a novel biocompatible hydrogel composed of type I COL, HA, and FG that may be used as an injectable cell carrier for cartilage repair. We have demonstrated that SDSCs are able to differentiate toward the chondrogenic lineage in vitro when cultured within the COL/HA/FG composite gel. Transplantation of the COL/HA/FG composite gel containing SDSCs led to the repair of osteochondral defects in rabbits. Therefore, these results demonstrate that the SDSC-encapsulated COL/HA/FG composite gel can be a good therapeutic candidate/strategy for the restoration of damaged or diseased articular cartilage. Additionally, this cell–gel combination product has the potential to be delivered by an arthroscope, which is advantageous for its clinical application in damaged or diseased articular cartilage.
Footnotes
Disclosure Statement
No competing financial interests exist.