
Abstract
Soft tissue defects resulting from trauma, tumor resection, or congenital causes provide a challenging problem to reconstructive surgery and tissue engineering. Current therapeutic procedures lack the ability to induce rapid formation of neovascularization. Therefore, to date, no adequate application for the reconstruction of soft tissue defects is available. We have previously shown that bioactive factors extracted from adipose tissue (adipose tissue extract [ATE]) induce both adipogenesis and angiogenesis in vitro. These bioactive factors were incorporated into hyaluronan (HA) hydrogel, and the ATE-HA implant-induced angiogenesis and adipogenesis were studied. The developed implant was shown to gradually release the bioactive factors, and the presence of the implant in human adipose stem cell culture was able to induce adipogenic differentiation as evaluated by Oil-red-O staining. In animal experiments, the implants were placed under dorsal subcutis of rodents. Either rat- (rATE, allograft) or human- (hATE, xenograft) derived ATE was incorporated into implants. Local inflammation reactions, angiogenesis, and adipogenesis were followed from 1 week to 40 weeks. Angiogenesis was assessed by microvessel density analysis; adipogenesis was assessed by automated image analysis, and immunological effects by immunostaining and counting inflammatory cells. The key requirements for soft tissue replacement—host compatibility, bioactivity, and sustainability—were all achieved with the novel ATE-HA implant. This acellular implant induced microvessel induction early after implantation and adipose tissue deposition from 12 weeks onward as well as subcutaneous tissue volume increase. The ATE-HA implant was replaced by mature adipose tissue with capillaries, nerve bundles, and healthy connective tissue without local inflammation or capsule formation. The large fat pads remained in tissue until the end of the follow-up time, for 9 months. No adverse effects were detected at the site of implantation, and according to irritating ranking, the ATE-implant was considered to have excellent biocompatibility. The results demonstrate that an acellular HA hydrogel implant induces significant increase in adipogenesis and angiogenesis in vivo compared to the plain HA implant, and ATE has excellent potential for use in tissue engineering for sustained reconstruction of soft tissue defects.
Introduction
Current therapeutic procedures for soft tissue replacement include filling the defects with synthetic or natural biomaterials, using autologous fat grafts or stem cell therapy.2,8–10 Synthetic materials induce unwanted allergic reactions, and fat grafts have drawbacks such as resorption of transplants. 10 Stem cell therapy is promising, although time consuming, and only autologic transfer of cells is possible.9,10 The adequate induction of angiogenesis is a prerequisite for successful adipose tissue reconstruction.11–13 It was recently reported that in tissue-engineered vascular grafts, the neovasculature was solely derived from the host cells via vascular remodeling, not from implanted cells.14,15 The cells of the tissue-engineered vascular graft actually promoted the host tissue regeneration instead of themselves differentiating into the vessels. 16 The key inductive molecules would therefore be sufficient for adequate induction of vascular development. 15 In fact, an acellular soft tissue substitute that would induce its own replacement would be advantageous to soft tissue engineering.14,17,18 Inductive adipogenesis would not require stem cell harvest from the patient, and an acellular alternative would prevent severe immune responses and could allow the alloplastic use of the implant.1,17,19–24 Several studies have already been performed to provide a suitable microenvironment for the formation of blood vessels and adipose tissue without the need to transplant cells. This has been tried by incorporating growth factors or extracellular matrix proteins into biomaterials.14,17,20,25–28 The controlled release of multiple angiogenic factors has shown to promote tissue regeneration at the site of the implantation.14,29,30 However, the creation of the optimal environment for inductive adipogenesis has been difficult, especially in long-term. 8 Overall, all current therapy approaches for soft tissue induction, mostly due to inadequate vascularization,13,28,31 fail to produce long-term satisfactory and repeatable results, 8 and therefore the sizes of the tissue-engineered implants are limited.31–33
Adipose tissue is known to be a very active endocrine organ and an excellent source of growth factors and cytokines,30,34,35 and it can be thought to bear excellent potential for adipose tissue induction. 34 We have recently characterized and developed the process to extract growth factors and cytokines from adipose tissue (the adipose tissue extract [ATE]), and have shown that ATE is capable of inducing effectively both angiogenesis and adipogenesis in vitro, and has therefore potential to be used in soft tissue engineering. 34
The main objective of the current study was to create an acellular implant by incorporating ATE into a biodegradable biomaterial that would release these angiogenic and adipogenic substances locally in tissue. The ATE was combined with hyaluronan (HA) hydrogel and implanted subcutaneously in rodents. HA is a glycosaminoglycan and a natural component of the extracellular matrix that takes part in binding growth factors and cytokines, 9 is known to modulate inflammation and tissue reparation 36 and to promote angiogenesis,37,38 and is therefore considered a very potential material for soft tissue engineering. 36 HA has been previously used, for example, for inducing formation of bone and cartilage 26 and soft tissue.8,31 Several FDA-approved injectable HA hydrogel materials are already in clinical use, and the adverse reactions of HA derivatives have been minimal.39,40
In the current study, the local effects after implantation of the grafts, inflammation reactions and induction of adipogenesis and angiogenesis, were followed. The efficacy and immunological effects were evaluated both short term and long term (from 1 to 40 weeks) in vivo, and both from allograft (rat ATE-HA implant in rat) and xenograft (human ATE-HA implant in rat). The present study shows that acellular HA implant with ATE induces significantly more angiogenesis and adipose tissue formation in tissue than the control HA implant. The ATE implants are regarded as nonirritant, and the effects of implantation are sustained, at least for 9 months.
Materials and Methods
The adipose tissue samples were obtained from surgical operations with informed consents at the Tampere University Hospital, Tampere, Finland, in accordance with the Ethics Committee of the Pirkanmaa Hospital District, Tampere, Finland (R03058). All animal experiments were performed according to the Finnish animal protection laws and approved by the Department for Social Welfare and Health Services of the State Provincial Office of Western Finland.
ATE preparation
Human adipose tissue specimens were obtained as subcutaneous tissue samples from surgical operations, and rat as subcutaneous fat adipose tissue specimens were obtained from sacrificed rats. Adipose tissue was cut into small pieces and transferred into 50-mL tubes (Sarstedt). Equal volume of the Dulbecco's Modified Eagle's Medium Nutrient Mixture F-12 (DMEM/F12; Gibco, Invitrogen), without supplements was added into the tube and left for 24 h for growth factor secretion at 37°C in a CO2 incubator. The tube was gently shaken during incubation. The extracts were collected, centrifuged at 12,000 rpm for 5 min, and sterile-filtered through a 0.22-μm filter (Sarstedt). The aliquots were stored at −20°C before use.
Measurement of protein concentration
ATE samples, collected at 24 h, and phosphate-buffered saline (PBS) samples, from the protein release study, collected at several time points were analyzed for the total protein concentration with the BCA protein Assay Kit (Pierce Biotechnology).
Preparation of implants
The resulting sterile ATE, either from (1) human, hATE, or from (2) rat, rATE, was mixed with HA (nonanimal-derived partially cross-linked hyaluronic acid Restylane; Q-Med) in such a ratio that the implant contained 57% ATE and 43% HA hydrogel. As a control implant, HA with incorporated PBS was used, with corresponding volumes of HA (43%) and PBS (57%). The final human ATE concentration in the implant was 1.48 mg/mL of hydrogel (148 μg in each implant), and the final rat ATE concentration in the implant was 0.75 mg/mL of hydrogel (75 μg in each implant).
Isolation and culture of human adipose stem cells
Stem cells were isolated as described previously.34,41–43 Briefly, human adipose tissue specimens were cut into pieces and enzymatically digested with 0.05% collagenase I (Invitrogen). The digested tissue was centrifuged at 600 g for 10 min and filtered through 100- and 40-μm filters (Sarstedt). Human adipose stem cells (hASCs) were seeded and cultured in DMEM/F12 supplemented with 1%
Protein release studies
The protein release from the implants was tested by incubating the implants in PBS at 37°C up to 3 weeks. The 48-well plate inserts (Scaffdex Oy) were filled with HA-ATE hydrogels, prepared as described above, and put on the top of PBS-filled 48-well plate wells (Nunc). Aliquots of PBS were collected at predetermined time points and analyzed for total protein concentration with BCA protein Assay (Pierce Biotechnology).
Adipose stem cell differentiation with bioactive HA implant
To study the adipogenic effect of bioactive implants in cell culture, hASCs were plated in 48-well plates at early passages (p1–p3) at a density of 10,000 cells/cm2. Cells were seeded and cultured in the hASC culture medium as described above. The next day, the hATE implants were created as described above. The 48-well inserts (Scaffdex) were filled with hATE-HA hydrogel and placed into cell culture wells. The medium was changed twice during the study. Cells were cultured for 6 days and examined for lipid accumulation with Oil-red-O (ORO; Sigma) staining.
ORO staining
Lipid accumulation was assessed at 6 days after the onset of the differentiation experiment by using ORO staining. ORO staining was performed as described previously. 34 Briefly, hASCs were fixed with 4% paraformaldehyde (Sigma) for 20 min, incubated with 60% isopropanol for 2 to 5 min, and stained with 3:2 diluted and filtered 0.5% ORO stock solution (Merck & Co., Inc.; prepared in 100% isopropanol) for 5 min. Images were taken with the Nikon Eclipse TS-100 microscope (Nikon) equipped with the Nikon DS Camera Control Unit DS L-1 (Nikon). The images were processed with Adobe Photoshop CS3 software (Adobe Systems) and Corel Draw software 10.0 (Corel Corporation).
Animal model of acellular soft tissue induction
Twenty-six male Sprague-Dawley rats (weight 325±75 g, average age of 8 weeks) were housed per 2, with 12 h light and 12 h darkness, and fed pelleted diet and water ad libitum. Rats were anesthetized with a mixture of Domitor (medetomidin hydrochloride; Orion Pharma) 1 mg/mL (0.5 mg/kg) and Ketalar (ketamin hydrochloride; Pfizer) 10 mg/mL (75 mg/kg). Three different types of hyaluronic acid implants, each incorporated with different substances, were created as described above. About 100 μL of the resulting gel mixture was immediately injected with a 1-mL syringe and a 27-gauge needle (Terumo Europe) into dorsal subcutis of rat. Implants were carefully injected in between the upper subcutis and the muscle layer into rat dorsal subcutis. Three animals in each time point were used (n=3); three constructs per rat were implanted, and the places of implants were varied in different time points. The injected implant was ∼8 mm in diameter. Implants were left under subcutis for 1, 4, 12, 20, or 40 weeks, after which animals were sacrificed. The remaining implant and its surrounding tissue were carefully cut from the implant site in the dorsal subcutis and further processed for histological analysis.
Hematoxylin and eosin staining
The histological specimens were cut into 1-mm2 pieces and fixed in 4% paraformaldehyde overnight, dehydrated with a graded ethanol series, and embedded in paraffin. Specimens were cut into 5-μm-thick slices with a microtome (Microm HM 430, Microm GmbH) and stained with hematoxylin and eosin (H&E) for histology. Briefly, samples were deparaffinized by treating them three times for 5 min each with xylene (VWR International, LLC) and after that with graded laskeva ethanol series. The samples were stained for 10 min with Mayer Hematoxylin or Papanicolauslösung 1a Harris' Hämatoxylinlösung (Merck KGaA), rinsed with tap water 10 min and with distilled water 2 min, then stained with 1% eosin for 15 s, and rinsed with tap water and further with distilled water. The samples were then dehydrated with 94% and 100% ethanol, treated 3×5 min with xylene, and mounted with Entellan (Merck KGaA) for storage. Images were taken with a Nikon Microphot FXA microscope (Nikon) connected to a Sony DXC-S500 camera control unit and Sony Twain Driver Software 1.0 (Sony Europe Limited) and further processed with Adobe Photoshop CS 3 software (Adobe Systems) and Corel Draw software 10.0. (Corel Corporation). The microscopic images from H&E-stained subcutaneous tissue slices were merged with Canon Photo Stitch 3.1 (Canon).
Immunohistochemistry
The histological specimens were cut into 1-mm2 pieces and fixed in 4% paraformaldehyde overnight, dehydrated with a graded ethanol series, and embedded in paraffin. Specimens were cut into 3- or 5-μm-thick slices with a microtome (Leica DM2000; Leica Instruments GmbH or Microm HM 430; Microm GmbH, respectively). Samples were deparaffinized with xylene (VWR International, LLC) 3×5 min each, rehydrated with graded ethanol series, and washed with distilled water.
For anti-von Willebrand Factor and for anti-Neurofilament-68 staining (anti–vWF produced in rabbit; Sigma; 1:5000 and anti-NF-68 produced in mouse; Sigma; 1:500, respectively, both 4°C overnight), tissue samples were treated 15 min with 0.5% hydrogen peroxide (Mallinckrodt Baker, Inc.) in methanol (Mallinckrodt Baker, Inc.), microwave oven-treated 10 min in a preboiled 0.01 M sodium citrate buffer, pH 6.0, cooled 20 min in a sodium citrate buffer, and treated with the Histostain Plus Broad Spectrum Detection Kit (Zymed Laboratories, Inc., Invitrogen). The color was developed with a DAB Substrate kit (Zymed Laboratories) for 5 min. The samples were counterstained for 5 s with Mayer Hematoxylin and mounted with Entellan (Merck KGaA).
For anti-CD3 staining (CD3 [Clone SP7] rabbit monoclonal antibody; Thermo Fisher Scientific; 1:100, 90 min at room temperature), the samples were microwave oven-treated 2×7 min in 10 mM Tris–HCl, 1 mM EDTA, pH 9.0., cooled for 20 min in Tris–EDTA buffer, and then treated with the DAKO EnVision™ + System, HRP kit (DakoCytomation). For anti-CD79a staining (mouse anti-human Cd79a; AbD Serotec, MorphoSys AG; 1:500, 4) and for anti-CD68 staining (monoclonal mouse anti-rat CD68; AbD Serotec, MorphoSys AG; 1:100, in 0.1% BSA in TBS, 4°C overnight), samples were treated with the Mouse on Rat HRP Polymer Kit (Biocare Medical). The color was developed with the DAKO Cytomation Liquid DAB Substrate Chromogen System (Dako), and samples were counterstained with Papanicolauslösung 1a Harris' Hämatoxylinlösung (Merck) and mounted with Pertex (HistoLab Products Ab).
The results were analyzed with a Leica DM 2000 microscope (Leica) from five different fields from three animals per each time point. Images were taken with a Nikon Microphot FXA microscope (Nikon) connected to a Sony DXC-S500 camera control unit and Sony Twain Driver Software 1.0 (Sony Europe Limited) and processed for publication with Adobe Photoshop software CS3 (Adobe Systems), Corel Draw software 10.0 (Corel Corporation), and Canon Photo Stitch 2.0. (Canon).
Determining the capillary density
The number of formed capillaries was calculated microscopically from three animals per time point (each containing three different types of implants), and from five different random high-power fields (hpf, 400×) in each implant at the implant–tissue interface with a Leica DM 2000 microscope (Leica Microsystems GmbH). The capillaries were confirmed to be stained positive for vWf, and the capillaries needed to have lumen that was visible in hpf (400× magnification). Both capillary proliferation and larger arteriole-like and venule-like vessels were counted.
Automated quantitative analysis of the adipose tissue formation
To quantitate the adipose tissue formation in rat subcutis, an automated computer-assisted analysis tool was earlier developed for fat deposit detection. The applicability of the analysis tool for quantification of fat and for evaluating the differences in the fat accumulation between time has been previously described. 44 Briefly, before analysis, the samples were stained as described above in H&E staining. H&E-stained slides were photographed with a Nikon Microphot FXA microscope (Nikon) connected to a Sony DXC-S500 camera control unit and Sony Twain Driver Software 1.0 (Sony Europe Limited) and analyzed with the analysis tool without any preprocessing to the images. The analysis tool estimates the area of fat coverage by segmenting the hue component of the image with dual thresholding. Size constraints were applied to remove small, fractioned areas and excessively large areas, which typically belong to background. Finally, the user was allowed to modify the segmentation result by removing any possible false detection and by adding missing areas. Adding of new areas was implemented using the seeded region growing where the user gives the seed point and the area grows around this point. 44
Measurement of the tissue expansion
The H&E-stained histological specimens were measured with a Nikon TS-100 microscope using Nikon TS Elements software. The total vertical height of the rat dorsal subcutis sample (from the muscle layer to the epithelial layer) was measured from each implant from two different sites at a 40-week time point.
Evaluation of the local immunological effects of implantation
The local biological effects were quantitatively scored after immunohistochemical staining as described previously45,46 and according to the International Organization of Standardization (ISO) Standard ISO-10993:6–2007 “Tests for local effects of implantation,” when applicable. The response was evaluated per hpf (400×) from five different fields and from three different animals per time point. The inflammation score criteria were (as modified from ISO 10993-6:2007) as follows: 0=no cell type detected; 1=rare; 1–5/hpf (except for giant cells, 1–2/hpf); 2=5–10/hpf (except for giant cells, 3–5/hpf); 3=heavy infiltrate; 4=packed. The final average irritating ranking (as described in ISO 10993-6:2007) was obtained from the average of overall scores.
• nonirritant (0.0–2.9)
• slight irritant (3.0–8.9)
• moderate irritant (9.0–15.0)
• severe irritant (>15)
The final active inflammatory changes were multiplied by two to get the final irritation ranking.
Statistical analysis
All statistical analyses were performed and graphs processed with GraphPad Prism 5 (GraphPad Software, Inc.). Samples were subjected to one-way analysis of variance followed by appropriate post-tests; for the capillary formation and adipose tissue formation, Tukey's and Dunnett's post-tests, and for tissue thicknesses, Tukey's post-test. The results were considered significant when *p<0.05, **p<0.01, and ***p<0.001.
Results
Protein release from the implants
The protein release of the designed implants was tested by incubating the implants with PBS as well as incubating the implants with ASCs. The ATE-containing implants were shown to release protein when incubated in PBS up to 3 weeks, whereas control implants did not show any protein release. The results are seen in Figure 1A. The protein released from the implants was able to induce adipogenesis in hASC culture as stained with ORO after 6 days of culture (Fig. 1B).
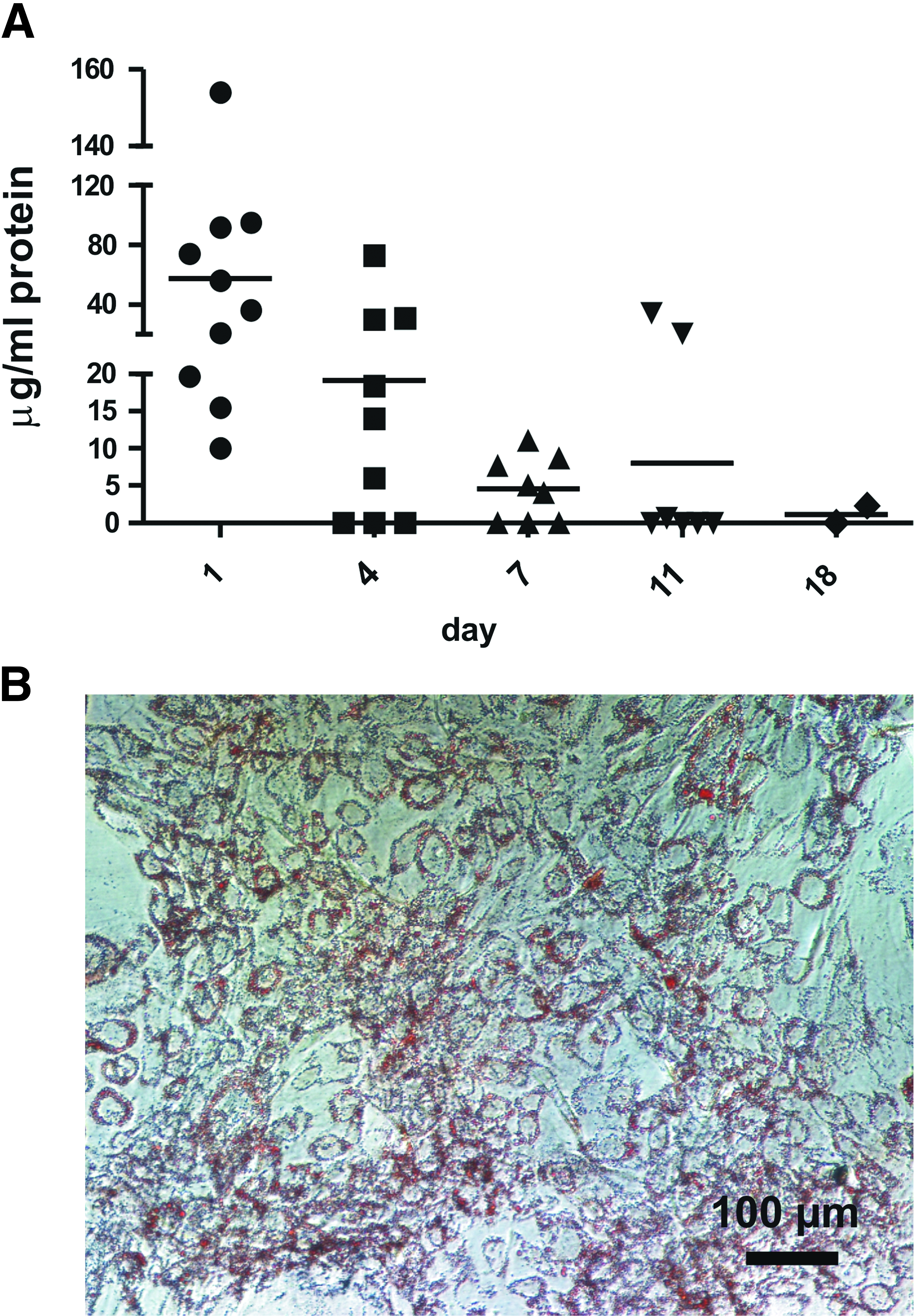
The HA hydrogel protein release.
Histological evaluation of the local effects of implantation in tissue
The effects of implantation were evaluated with local tissue histology after H&E staining. The evaluated time points were 1, 4, 12, 20, and 40 weeks. The results are shown in Figure 2.

The rat subcutaneous tissue histology at 1, 4, 12, 20, and 40 weeks after implantation of the rATE-HA implant, hATE-HA implant, or control (plain HA) implant.
At 1 week, cell penetration into all of the implants was seen. Capillary proliferation with small newly formed capillaries was extensively present with both rATE-HA and hATE-HA implants (Fig. 2B, C, respectively) at the implant–tissue interface. In rATE, also larger arteriole-like and venule-like vessels were seen next to the implant (Fig. 2B). The vessels were higher in number as well as in the diameter with rATE-HA and hATE-HA implants, compared to controls. Very small adipose tissue deposits, indicating triglyceride accumulation, were also seen (Fig. 2B). The control implant did not present any relevant tissue changes (Fig. 2A).
At 4 weeks, the tissue histology resembled that of 1 week. Vast capillary infiltration was seen with both rATE-HA and hATE-HA implants at the implant–tissue interface, close to the degrading hydrogel, and several arteriole-like and venule-like structures and a lot of small fat deposits were seen. Close to the implant, large vessels were also present. Only few larger capillaries were detected in the control implant (Fig. 2D).
At 12 weeks, few larger vessels and small fat deposits were seen in the control HA implant (Fig. 2G). In rATE-HA implant, dense, large, well-vascularized fat pads were already seen (Fig. 2H). Capillaries were evenly distributed throughout the fat tissue. The newly formed fat pads were often seen to be located apart from the native fat tissue, at the initial implant injection site. Inside the fat pads, vascularization and nerve bundles were visible. The hATE-HA implant (Fig. 2I) was histologically similar to the rATE-HA implant; however, the amount of fat was more extensive in the rATE-HA implant than in the hATE-HA implant.
At 20 weeks, the tissue histology was similar to 12 weeks, except that more adipose tissue had accumulated in the rATE-HA (Fig. 2K) and hATE-HA (Fig. 2L) implants. More adipose tissue was seen in the rATE (Fig. 2K) than in the hATE (Fig. 2L). The rATE-HA implants had induced large fat pad formations, seen as several layers of adipose tissue. All implants, the rATE-HA implant, hATE-HA implant, and control implant, were still present in tissue, and they were equally degraded.
At 40 weeks, the control implants were completely degraded. These implants had induced some adipogenesis, more than was seen in the control tissue. Two of the rATE-HA implants (out of three animals) were degraded completely. The degradation of the control implant was faster than the rATE-HA and hATE-HA implants. The hATE-HA implant degradation rate was decreased compared to other implants, as all of the implants still partly remained in tissue at 40 weeks. However, no capsule formation was seen, only a narrow layer of fibrosis occasionally. The large fat pad formations, seen also already at 20 weeks, and induced especially by rATE-HA implants, were present at 40 weeks, and the adipose tissue seen was well vascularized. The histology of the newly formed mature adipose tissue was similar to normal tissue in all implants at 40 weeks, when tissue histology was compared between the control implant (Fig. 3A), rATE-HA implant (Fig. 3B), and hATE-HA implant (Fig. 3C). The accumulated adipose tissue in the implants resembled that of the endogenous tissue with a densely packed structure and hexagonal-shaped cells, accompanied with blood vessels.

The comparison of adipose tissue histology in H&E-stained images between rATE-HA implant
When tissue thicknesses were microscopically evaluated, the HA implant (Fig. 3D, rATE-HA implant) was shown to induce increase in thickness of subcutis at 20 weeks compared to control implant (Fig. 3E) and control tissue (Fig. 3F). The change in tissue thickness was evaluated by measuring the thickness of the subcutis from histological samples at 40 weeks. The results are shown in Figure 3G. As statistically evaluated, all implants induced a significant increase in tissue thickness at 40 weeks compared to control tissue (control implant **p<0.01; hATE-implant ***p<0.001; rATE-implant ***p<0.001). At 40 weeks, the tissue thickness was significantly higher in the rATE implant and the hATE implant (both ***p<0.0=1), compared to the control implant.
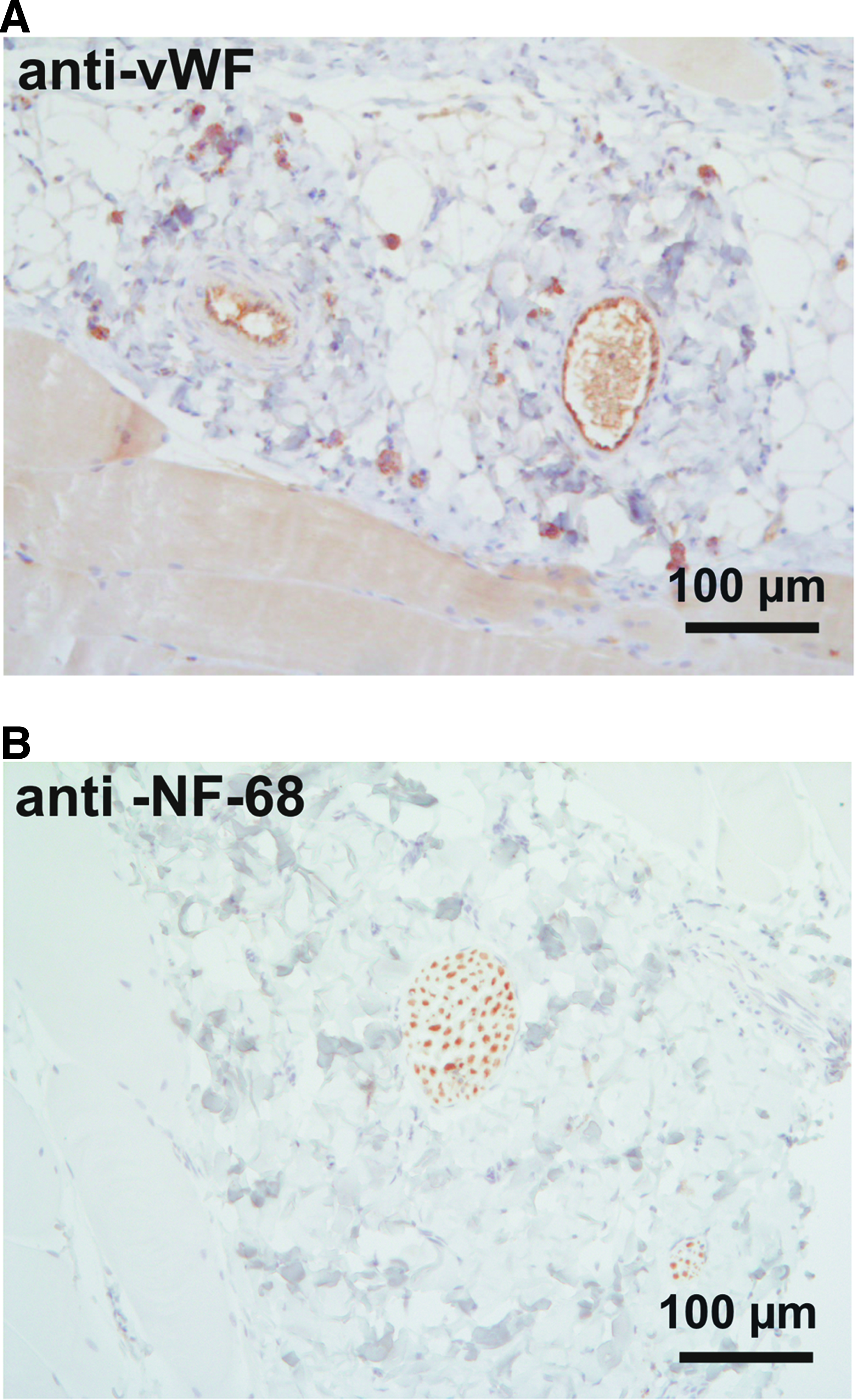
The capillary proliferation was confirmed with anti-von Willebrand factor staining at 4 weeks (Fig. 4A), and tissue innervation, seen often from 12 weeks onward as nerve bundles, was confirmed with antineurofilament 68 staining (Fig. 4B). Nerve bundles were not detected at earlier time points, but often at 12 to 40 weeks.
Quantification of angiogenesis and adipogenesis in vivo
Capillary density was evaluated from five different microscopic hpf (400× magnification) at 1 and 4 weeks (e.g., before adipose tissue accumulation) by calculating the capillaries manually under microscope. The results are shown in Figure 5A. The statistical analysis was performed at both time points between different implants (significancy shown in Fig. 5A as asterisks) as well as by comparing each implant to their 1-week control (significancy shown in Fig. 5A as hash signs). Both capillary proliferation and larger arteriole-like and venule-like vessels were counted. The overall number of vessels was highest at 1 week. The control implant blood vessel number was very similar at both time points. The hATE-HA implant induced significantly higher capillary proliferation at 1 week (p<0.05) and at 4 weeks (p<0.001), compared to the respective control implants.
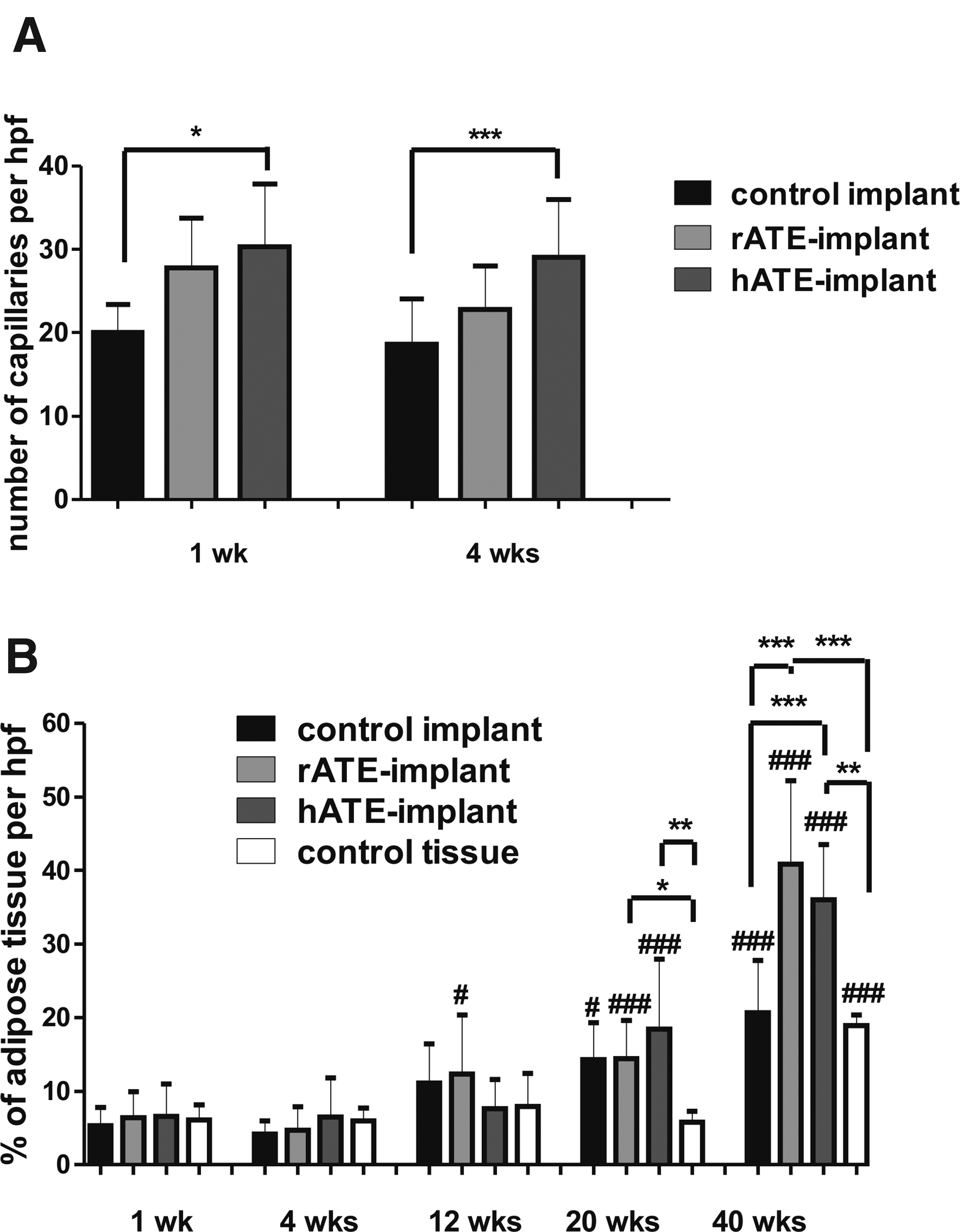
The quantification of angiogenesis and adipogenesis after implantation of ATE-HA implants.
The adipose tissue was quantified with a specific analysis tool designed for the purpose and published previously. 44 The statistical analysis was performed at each time point between different implants (shown in Fig. 5B as asterisks) as well as by comparing each implant to their 1-week control (shown in Fig. 5B as hash signs). The number of adipose tissue (% from microscopic image, 40× magnification) was increased during the time; however, until 12 weeks, there was no significant increase in adipose tissue accumulation. At 12 weeks, the rATE-HA implant contained significantly more adipose tissue than the rATE-HA implant at 1 week (p<0.05). At 20 weeks, all (control implant, rATE-HA implant, and hATE-HA implant) had more adipose tissue than respective treatments at 1 week (p<0.05, p<0.001, and p<0.001, respectively). Moreover, at 20 weeks, the rATE-HA implant and the hATE-HA implant had induced more adipose tissue accumulation than control tissue (p<0.05 and p<0.01, respectively). At 40 weeks, all implants, as well as control tissue, contained more adipose tissue than respective treatments at 1 week (all highly significant, p<0.001). However, at 40 weeks, the rATE-HA and hATE-HA implants had induced significantly more adipose tissue accumulation than the control implant (p<0.001 with both implants) or control tissue (p<0.001 and p<0.01, respectively).
Immunological effects of implantation
The evaluation of immunological effects of implantation was modified from ISO-10993:6-2007. The results are scored and summarized in Table 1. To be able to perform irritating ranking as described in ISO 10993-6:2007, the active inflammatory changes were multiplied by two. Similar inflammatory scoring is also described previously.45,46 The irritation ranking was evaluated solely by immunological effects, not with induction of vascularization or fatty infiltrate, as these were the desired effects of implantation. No serious adverse tissue effects occurred. Some inflammatory cell infiltration was seen in earlier time points. At week 1, the control implant showed moderate B-cell and mild macrophage infiltration, as well as the rATE-HA and hATE-HA implants showed mild infiltration of B-cells and macrophages. The polymorphonuclear cell infiltration was minimal throughout the study. During the time course, the control implant inflammatory effects were decreased and were completely disappeared at 40 weeks, when also the implant had degraded completely. The rATE-HA and hATE-HA implants were both present at 40 weeks, hATE-HA in each sample and rATE-HA occasionally, and they still showed some inflammatory cell infiltration at the time. No granuloma, fibrous capsule formation, giant cells, or necrosis were seen in any of the samples. Implants were seen to be often surrounded by a narrow band of fibroblasts, but after implant was degraded, no signs of fibrous bands were seen. Normal fibroblast proliferation was often seen, and it was accompanied with capillary proliferation. According to the evaluation of local immunological effects, the implant was considered to be nonirritant compared to the control implant.
The response has been evaluated per high-powered field (hpf, 400×) from five different fields surrounding the implant and from three different animals in each time point.
The inflammation score criteria were (as modified from ISO 10993-6:2007)
0=no cell type detected,
1=rare, 1–5/hpf (except for giant cells, 1–2/hpf),
2=5–10/hpf (except for giant cells, 3–5/hpf),
3=heavy infiltrate,
4=packed
The average irritating ranking (as described in ISO 10993-6:2007) was as follows:
• nonirritant (0.0–2.9)
• slight irritant (3.0–8.9)
• moderate irritant (9.0–15.0)
• severe irritant (>15)
Negative difference was recorded as zero.
ATE, adipose tissue extract; HA, hyaluronan; ISO, International Organization of Standardization.
When statistically evaluated, none of the implants were found to be more irritating than others. The CD3- (T-cell) positive cell count was significantly higher in the rATE-HA implant at 1 week than with any other implant and in any other time point (p<0.001) as well as in the hATE-HA implant at 1 week compared to implants at 20 weeks (p<0.05) and 40 weeks (p<0.01). The CD68- (macrophage) positive cell infiltration was significantly higher in the control implant at 1 week and at 20 weeks compared to the control implant at 40 weeks (p<0.01 and p<0.001, respectively). Moreover, the rATE-HA and hATE-HA implants had significantly more macrophage infiltration at 1 week compared to the respective implants at week 40 (p<0.05 and p<0.01, respectively). The control implant had significantly more CD79a-positive cells at week 1 than at week 20. The polymorphonuclear cell count remained low in all implants throughout the study.
Discussion
Soft tissue engineering is a prominent research area, as soft tissue defects and chronic wounds are a medical and economic challenge to the healthcare system, and the demand is increasing every year.4,5 The ideal soft tissue replacement should induce rapid vascularization, induction of adipogenesis, and induce a permanent effect in tissue. 2 However, the current applications have shown only modest success, for example, some vascularization, but hardly any adipose tissue formation, 14 and the optimal adipose tissue substitute remains to be discovered.
Our approach for the induction of capillary proliferation and adipose tissue accumulation was to create an in vivo-like environment for soft tissue formation as possible. In our previous work, we demonstrated that extracted factors from adipose tissue (ATE) induce angiogenesis and adipogenesis in vitro. 34 ATE is able to induce adipogenesis at ≥200 μg/mL protein and angiogenesis at ≥450 μg/mL protein. 34 ATE is a mixture of a wide variety of components of mature adipose tissue, of which the most abundant are, for example, vascular endothelial growth factor, fibroblast growth factor 2, adiponectin, angiogenin, interleukin 6, leptin, and insulin-like growth factor-binding protein 6. 34 These factors are known to have an inductive role on adipogenesis and/or angiogenesis (reviewed in Szasz and Webb). 47 In the present study, we demonstrate that both the induction of microvessels and adipose tissue can be effectively and permanently induced with these adipose tissue-derived factors in vivo. The key requirements for soft tissue replacement, as listed by Choi et al, 2 are host compatibility, bioactivity, and sustainability, all of which were achieved with the novel ATE-HA implant.
The ATE-HA implant induced extensive capillary proliferation early after implantation, and the induction was significantly higher than the control implant. The induction of vascularization during the first 4 weeks was well in line with the protein release rate of the implants detected in vitro. The human ATE induced slightly more capillary formation than rat ATE in rat subcutaneous tissue. This may have been due to the higher concentration of hATE in the implant compared to rATE (rATE implant contained 75 μg protein and hATE implant 148 μg protein). However, as the rat ATE was overall slightly more efficient in adipose tissue accumulation in rat tissue than human ATE, one explanation may be that human factors act differently in rat adipose tissue remodeling than allogenic (rat) factors. In fact, it is known that there are differences between rodent and human adipose tissue. 48 In adipose tissue, key adipokines have differences in function in humans and rodents, as reviewed in Wang et al. 49 From 12 weeks upward, when also adipose tissue started to accumulate, the histology of the newly formed tissue vasculature resembled that of endogenous adipose tissue. The growth factor-induced neovascularization was extensive early after implantation compared to endogenous tissue, but during adipogenesis, the vessels were remodeled. During angiogenesis stimulus in tissue, the endothelial cells start to proliferate toward the stimulus, and a number of immature capillaries are formed. During vessel remodeling, the vessels that cannot become perfused are regressed, 50 resulting in normal tissue restoration. Similarly, the ATE-implant induced formation of adipose tissue with vasculature that was histologically comparable to the endogenous fat tissue. It is an important finding that ATE is able to induce efficient tissue restoration with normal vascular remodeling.
The adipose tissue deposition was abundant and microscopically observed as dense fat pads from 12 weeks onward with ATE-HA implants (significant increase compared to control tissue), and also, the subcutaneous tissue volume was increased. However, due to variation between animals, the adipose tissue increase was not statistically significant compared to the control implant, until at 40 weeks. The timing of adipose tissue appearance in ATE implants most likely reflects the release properties of the biomaterial used in the study. The inductive factors are first released by diffusion from the implant; however, later on, the factors are released simultaneously with the degradation of the material. The inductive effect could be possibly reached sooner, if a higher concentration of ATE was used, or moreover, different type of hyaluronic acid or other biomaterial was used. However, this remains to be further tested.
The rat ATE was overall slightly more efficient in adipose tissue induction in rat tissue than human ATE. However, both the rATE-HA implant and the hATE-HA implant were replaced by newly formed adipose tissue that had histological features of normal adipose tissue; capillaries, nerve bundles and normal connective tissue, and the fat pads remained in tissue until the follow-up time (9 months). Already at a 20-week time point, the 100 μL rat ATE implant had induced even a sevenfold increase in fat accumulation compared to control tissue (∼0.4-mm fat layer in control tissue vs. even 2.8-mm fat layer in the rat ATE implant), and almost 2.5-fold induction compared to the control implant (∼1.2-mm fat layer in the implant). Both ATE implants induced significantly thicker tissue than the control implant at 40 weeks. The sustained effect in this extent has not been demonstrated previously by any of the applications tested, neither with hASC-seeded scaffolds nor with acellular scaffolds. For example, in a previous study by Hemmrich et al., 37 blood vessels were formed, but hardly any mature fat was seen by 12 weeks postimplantation. In a 24-week study by Tsuji et al, 51 only modest de novo adipogenesis was seen. Overall, previous studies show some adipose tissue formation, but no vascularization, 52 or limited longevity of the adipose tissue 20 and not enough information on long-lasting (over 3-month) effects.52–54
Tissue fillers like hyaluronic acid are known to contribute to angiogenesis and adipogenesis,36–38 and this was also seen in our study, as the control implant did increase both capillary and adipose tissue formation in some extent. However, at 40 weeks, when the control implant had degraded, the control implant had not induced any more adipose tissue than what was seen in control tissue. There was an increase in the tissue thickness in the control implant, which was however often contributed by the connective tissue formation induced by the control implant. Therefore, the control implant did not induce mature adipose tissue formation, although mild adipose tissue induction compared to normal tissue. The control tissue also represented a significant change in adipose tissue accumulation between week 1 and 20 and/or 40 weeks. It is a well-known phenomenon and a normal feature presented in laboratory animals that laboratory animals gain weight during time when they get older.
The key feature of a soft tissue substitute, the good biocompatibility, 2 was achieved with the ATE-HA implant. No adverse reactions or fibrous capsule formation occurred, and when the local inflammatory cell response of the implants was observed, ATE-HA implants did not show increase in irritating effects over the control HA implant. At 1 week postimplantation, the T-cell marker CD3 was increased in the rATE-HA and hATE-HA implants, and on the other hand, the B-cell marker CD79a in the control implant and macrophage infiltration in all implants. This is most probably due to the tissue damage caused by the injection of the implant into the subcutaneous space. We cannot exclude the possibility that hyaluronic acid itself induces inflammatory cell infiltration; however, ATE does not have any additional effect on the number of inflammatory cells, and therefore can be considered to be biocompatible and safe. In fact, macrophage infiltration is reported to be intrinsic for adipose tissue formation.55–57 Macrophages are known promote angiogenesis,36,58 hASC differentiation into endothelial cells, 45 and even to transdifferentiate into adipocytes. 55 It is also noteworthy that there was no difference with the immunological reaction between allogenic (rat ATE in rat) and xenogenic (human ATE in rat) implants, indicating that the ATE is well tolerated.
The angiogenesis-/adipogenesis-inducing effect in rats was demonstrated with quite low doses of ATE. Each rATE implant contained 75 μg protein and each hATE implant 148 μg protein. In the current study, the injectable implant was administered only once, at the onset of the study. Repeated administration and increased dose of ATE could even enhance the inductive effect. As the potential cytokines are injected locally, the overall doses of adipogenic and angiogenic factors required are reduced. However, the optimal dose and efficacy, and administration schedule of ATE, are currently under further investigation, as the right combination of factors is known to be crucial,28,30 rather than the maximal dose. The effects of simple ATE substance, if used without incorporation into scaffold, are currently under study, as well as the systemic toxicity of high concentrations of ATE. It also remains to be resolved whether the range of indications of ATE could be broadened, that is, whether the inductive effect of ATE applies to other tissues than soft tissue.
We have developed a new acellular approach to soft tissue engineering. ATE combined with HA hydrogel is able to induce vascularization and soft tissue formation in tissue. The key requirements for soft tissue replacement—host compatibility, bioactivity, and sustainability—are all achieved with the novel ATE-HA implant. The blood vessel induction in tissue is rapid, and the newly formed adipose tissue remains at least for 40 weeks and is histologically comparable to the native mature adipose tissue. The implant presents no immunological risks even when used in a xenogenic manner, and therefore is an important tool in creating an allogenic soft tissue substitute for patients. This bioactive implant is a potential replacement for the current soft tissue products to overcome the challenge of vascularization and to restore soft tissue permanently.
Footnotes
Acknowledgments
We sincerely thank Ms. Mirja Hyppönen, Ms. Marja-Leena Koskinen, Ms. Sari Leinonen, and Ms. Hilkka Mäkinen for excellent technical assistance. We thank Heikki Kupi, M.D., Ph.D., for providing us with HA hydrogel and Tiina Mäkelä, B.Sc., for the help in the analyses. Funding for the project was provided by the Biomaterial and Tissue Engineering Graduate School of Finnish Ministry of Education, the Competitive research funding of the Pirkanmaa Hospital District (EVO9G189 and EVO 9H212), as well as Pirkanmaa Cultural Foundation.
Disclosure Statement
No competing financial interests exist. Patent is pending (WO/2010/026299).