
Abstract
Following the coordinated efforts of five established scientific organizations, this report describes the novel cellular therapy activity in Europe for the year 2010. One hundred six teams from 27 countries responded to the cellular therapy survey, 69 teams from 21 countries provided data on 1010 patients using a dedicated survey; 37 teams reported no activity. These data were combined with an additional 260 records reported by 37 teams in 15 countries to the standard European group for Blood and Marrow Transplantation (EBMT) database. Indications were graft-vs.-host-disease (GvHD; 26%; 11% autologous), musculoskeletal disorders (25%; 93% autologous), cardiovascular disorders (20%; 100% autologous), epithelial disorders (16%; 44% autologous), autoimmune diseases (11%; 55% autologous), and neurological disorders (2%; 62% autologous). Autologous cells were predominantly used for musculoskeletal (39%) and cardiovascular (32%) disorders, whereas allogeneic cells were mainly used for GvHD (58%) and epithelial disorders (23%). The reported cell types were mesenchymal stem/stromal cells (MSC; 49%), hematopoietic stem cells (28%), chondrocytes (10%), dermal fibroblasts (4%), keratinocytes (1%), and others (8%). In 63% of the grafts, cells were delivered following ex vivo expansion, whereas cells were transduced or sorted respectively in 10% or 28% of the reported cases. Cells were delivered intraorgan (45%), intravenously (31%), on a membrane or gel (20%) or using 3D scaffolds (4%). Compared with last year, the number of teams adopting the dedicated survey was 1.25-fold higher and, with few exceptions, the collected data confirmed the captured trends. This year's edition specifically discusses scientific, clinical, regulatory, and commercial aspects related to the use of cell therapy for the repair of cartilage defects.
Introduction
Information available in public databases (e.g., www.clinicaltrial.gov) is critical to establish a map of the planned or ongoing trials, but does not allow identifying the precise number of patients treated with specific cells at a defined point in time. Published results of clinical studies are keys to evaluate the primary endpoints, but only marginally represent the total number of performed trials. Databases organized by working groups on specific areas (e.g., by the European group for Blood and Marrow Transplantation [EBMT]) have the main advantage of including data on the patient outcome, but can hardly be extended to the public domain, where sharing of critical information may conflict with confidentiality issues or commercial interests.
Since 2008, a complementary program has been established by the European sections of the Tissue Engineering and Regenerative Medicine International Society (TERMIS-EU), the International Society of Cellular Therapy (ISCT), and the International Cartilage Repair Society (ICRS) in a joint initiative with the EBMT and the European League Against Rheumatism (EULAR).5,6 The program is organized in the form of a survey, collecting the number of patients being treated in Europe by novel cellular therapies, sorted by specific therapeutic indications, cell types used, and cell processing/delivery modes. The absence of patient assessment data, the yearly publication of the data, and the possibility offered to the participating teams to query more specific information offers an open and flexible platform to establish and disseminate the status in the field of novel cellular therapies in Europe.
Here, we report the results of the third survey edition for the activity in 2010, with a comparison to the previously identified trends and a specific discussion on the field of cell-based cartilage repair procedures.
Patients and Methods
Definitions
For the purpose of this survey, novel cellular therapies include the use of cells other than HSC or of HSC for uses other than reconstitution of the hematopoietic system. The term HSC, which is often ambiguously used in the field of novel cellular therapies, indicates a mixture of stem and progenitor cells predominantly of the hematopoietic lineage. Donor lymphocyte infusions, often used in relapsing patients after HSC transplantation, are considered to be an integral part of the HSC transplant procedure and are excluded. The term “Epithelial disorders” is also used to include parenchymal diseases, as for example, diabetes or liver insufficiency.
Data collection and validation
Participating teams were requested to report their data for 2010 by indication, cell type and source, donor type, processing method, and delivery mode. The survey followed the traditional principles of the EBMT, concentrating on numbers of patients with a first cellular therapy. Members of the four participating societies from 47 countries (39 European and 8 affiliated countries) were contacted for the 2010 report (EBMT survey). The non-European countries affiliated with the EBMT were Algeria, Iran, Israel, Jordan, Lebanon, Saudi Arabia, South Africa, and Tunisia. For EBMT teams not using the extended questionnaire, information on cellular therapies was limited to numbers of HSC for nonhematopoietic use, mesenchymal stem/stromal cell (MSC)-based therapies (later identified to be almost exclusively related to treatment of graft-vs.-host-disease [GvHD]), and donor type. Extended questionnaires, in the format displayed in Supplementary Figure S1(Supplementary Data are available online at www.liebertpub.com/tea), were collected by paper forms or electronically. Quality control measures, for EBMT members only, included several established independent systems: confirmation of validity of the entered data by the reporting team, selective comparison of the survey data with MED-A data sets in the EBMT ProMISE data system, cross-checking with the National Registries, and onsite visits of selected teams. No quality control system could be yet applied for the non-EBMT reporting teams.
Transplant rates
Transplant rates, defined as the reported numbers of patients receiving cellular therapies or the number of teams reporting treatments per 10 million inhabitants, were computed for each country, without adjustments for patients who crossed borders or received treatment in a foreign country. Population numbers were obtained from the 2010 U.S. census office database (www.census.gov).
Results
Participating teams
One hundred six teams in 27 countries (24 European and 3 affiliated countries) responded to the novel cellular therapy survey; 69 teams (21 countries) reported performing novel cellular therapies with detailed information on indication, cell source and type, donor type, processing, and delivery mode, while 37 teams reported no activity. The remaining 37 teams from 15 countries (13 European and 2 affiliated countries) reported using the standard EBMT transplant activity survey, allowing to include only limited information. Data were thus received from a total of 23 countries. Teams that responded with activity are listed in the Appendix in alphabetical order by country, city, and EBMT center code (if applicable), along with the total number of reported novel cellular therapies.
Number of novel cellular therapies and disease indications
According to the received reports, 1142 patients were treated with novel cellular therapies, 504 (40%) with allogeneic and 766 (60%) with autologous cells (Table 1). Main indications were GvHD (26%; 11% autologous), musculoskeletal disorders (25%; 93% autologous), cardiovascular disorders (20%; 100% autologous), epithelial disorders (16%; 44% autologous), autoimmune diseases (11%; 55% autologous), and neurological disorders (2%; 62% autologous).
HSC, hematopoietic stem cells; MSC, mesenchymal stem/stromal cell; GvHD, graft-vs.-host-disease.
More detailed information on specific indications was obtained from 1010 patients. Among the musculoskeletal disorders, cartilage and bone repair were the most frequently reported indications. Among the cardiovascular disorders, peripheral artery disease, myocardial ischemia, and heart failure were the main reasons for a cellular therapy. Skin reconstruction, diabetes, and cornea repair were the three main reported indications for epithelial/parenchymal disorders. Among autoimmune disorders, gastrointestinal diseases and multiple sclerosis represented the predominant indications. The number of patients treated for neurological indications was rather limited and mostly confined to Huntington's disease. The number of reports of patients treated for GvHD needs to be combined with that reported in the EBMT standard form, for a total of 336 cases (Table 1).
Cell type, source and donor type
Of the 353 HSC treatments, 93% were autologous transplants and 59% were used to treat cardiovascular diseases (Table 1). All 125 chondrocyte transplants were autologous, whereas all 19 keratinocytes and 50 dermal fibroblasts transplants were allogeneic. Of 627 MSC-based therapies, 61% were allogeneic. The donor type was associated with the disease indication: autologous cells were predominantly used for musculoskeletal (39%) and cardiovascular (32%) disorders, whereas allogeneic cells were mainly used for GvHD (58%) and epithelial (23%) disorders (Fig. 1). In the detailed survey, MSC were mainly obtained from bone marrow (63%) or adipose tissue (25%) and mostly used to treat GvHD (38%), musculoskeletal (31%), and autoimmune disorders (14%). For the HSC treatments, cells were derived from the bone marrow (90%) or peripheral blood (10%).

Percentage of indications for novel cellular therapies in Europe in 2010, sorted by donor type. Data used for this chart were derived from the extended questionnaire and the standard European group for Blood and Marrow Transplantation (EBMT) survey sheet. GvHD, graft-vs.-host-disease.
Cell processing and delivery mode
Of all the grafted products reported in detailed form, 63% required cell expansion, 10% were transduced cells, and 28% were sorted (Table 2). Nonexpanded cells were used to treat 83% of neurological, 82% of cardiovascular, 37% of musculoskeletal, 26% of epithelial, and 30% of autoimmune disorders, while GvHD was exclusively treated with expanded cells. Cell sorting was applied for 70% of autoimmune, 44% of epithelial, 42% of cardiovascular, and 14% of musculoskeletal disorders. Transplanted cells were genetically transduced for 69% of autoimmune, 18% of epithelial, 3% of cardiovascular diseases, and 1% of the GvHD treatments.
Data only from extended questionnaire.
About one half (45%) of the cell grafts was delivered intraorgan, 31% intravenously, 20% on a membrane or gel, and 4% using a 3D scaffold (Table 3). Cells were delivered intraorgan for 85% of cardiovascular, 58% of neurological, 49% of musculoskeletal, 40% of autoimmune, and 39% of epithelial disorders. Intravenous delivery was reported for all GvHD treatments and predominantly for autoimmune (60%), epithelial/parenchymal (21%), and cardiovascular (13%) disorders. The use of a membrane or a gel for cell delivery was reported almost exclusively for epithelial (39%) or musculoskeletal (38%) treatments. A 3D scaffold was used only for musculoskeletal indications (13%), in particular cartilage or bone repair.
Data only from extended questionnaire.
Transplant rates and active teams
Reported cellular therapies were performed in a limited number of countries and with different intensity. Figure 2 displays the reported cellular therapy transplants per 10 million inhabitants in the different European and EBMT-associated countries. High transplant rates (i.e., >100 per 10 million population) were reported in Belgium, the Republic of Belarus, Slovenia, and Switzerland. The number of teams reporting novel cellular therapies was also mapped in the different European and EBMT-associated countries after normalization to the inhabitant numbers (Fig. 3). The number of reporting teams per 10 million inhabitants was higher than 4 in Belgium, Finland, Israel, Slovenia, and Switzerland.

Number of novel cellular therapies per 10 million inhabitants reported in Europe in 2010. Data used for this chart were derived from the extended questionnaire or the standard EBMT survey sheet.
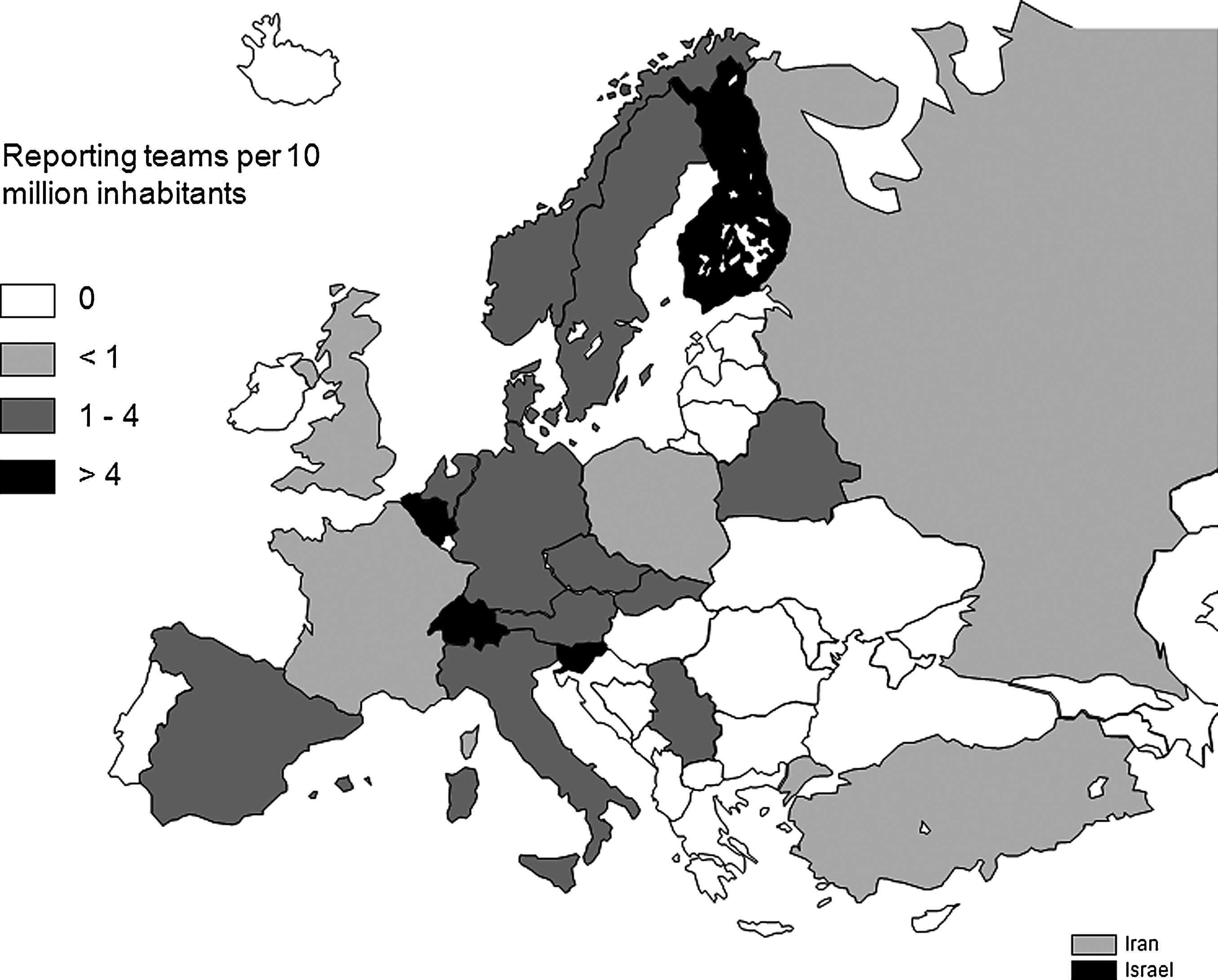
Number of teams per 10 million inhabitants reporting novel cellular therapies in Europe in 2010. Data used for this chart were derived from the extended questionnaire or the standard EBMT survey sheet.
Discussion
Compared with the data collected for patients treated in the previous years,5,6 the present report confirms the main identified trends, with a few remarkable differences. Although the percentages of treatments using autologous versus allogeneic cells were almost identical to those from 2008 and 2009, comparative analysis of specific categories indicates that the distribution of autologous or allogeneic cell transplantation for different indications has not yet reached a consolidated trend (Fig. 4). The discrepancies are more evident in the field of cardiovascular diseases, due to the predominant treatment of ulcers with allogeneic cells in 2009, and of epithelial/parenchymal disorders, due to the variable source of cells used for skin reconstruction. The remarkable absence of reports on the use of allogeneic cells for cardiac-related disorders in Europe is in line with the list of ongoing trials officially registered at www.clinicaltrials.gov and summarized in a recent study. 7 The fact that most ongoing trials for cardiac-related disorders outside Europe use allogeneic cells 7 highlights that the present report may be not representative of a geographically global scenario for what concerns donor types within specific categories, probably due to a combination of cultural, regulatory, and/or commercial issues.

The percentage of cases treated with expanded cells, requiring dedicated Good Manufacturing Practice facilities and compliance to a rigorously defined quality management system, slightly but steadily increased from 51% in 2008 and 59% in 2009 to 63% in 2010. This may indicate that the manufacturing groups are positively reacting to the tighter regulatory framework for Advanced Therapy Medicinal Products introduced in 2008 by the European Medicines Agency (EMA; www.ema.europa.eu). The use of transduced or sorted cells progressively increased from 2008, possibly reflecting the recognition that specific biological processes need to be targeted by enhancing expression of defined genes or implanting more homogeneous cell phenotypes. With regard to the cell delivery modes, the 2010 data confirmed that the use of a 3D scaffold remains confined within the field of musculoskeletal diseases, although in this area the percentage of use decreased by 50% from 2009. This figure is in line with the higher challenges in establishing “tissue engineering” procedures in the clinical practice, compared with the more conventional cell delivery modes.
This year's focus: cell therapy for cartilage repair
In cartilage regeneration, the use of cell therapy has been established for over 20 years.8,9 This extensive experience has been beneficial to the cell therapy field as a whole to recognize the importance of identifying proper clinical indications and of validating the tools for outcome evaluation, and to experience the challenges of the treatments that are mainly economical and logistical. In Europe, cellular therapies were placed under the guidance of advanced therapeutical medicinal products by the EMA. The necessary trial data for registration have increased the current clinical knowledge and allowed more evidence-based treatment selection and development of well-established algorithms for patient profiling.10,11 The time between cartilage damage, the occurrence of symptoms and initiation of treatment is of direct influence on treatment outcome. 12 So-called “old defects” in a chronic stage, treated in an environment of disturbed joint homeostasis, show significantly worse clinical outcome at 5-year follow-up. Thus, the initial concept of applying cell therapy after failure of other treatments is being replaced by earlier intervention with application of advanced imaging methods for more active early diagnosis.
Since the new regulatory pathway and framework have been established in 2008, the first product has been approved (ChondroCelect; Tigenix, Leuven, Belgium) and others are in the process of acquiring such approval (MACI, Genzyme; Sanofi, Kopenhagen, Denmark). The next step will be to place these products within a clinical setting that most effectively exploits them. Given the general economic challenges in Europe, it seems clear that innovative healthcare solutions need to take into account the economic downturn and associated financial restrictions of healthcare systems. More and more we will be asked to apply innovative solutions in an initially limited market, to generate well designed prospective cost benefit and risk analyses. This will be most likely applied in selected cell therapy centers and should be providing data to a central European prospective registry (i.e., ICRS EuroCart), which will allow for reporting collaboratively on the outcome of these essential developments.
The data from the current survey indicate a rise from 7% in 2009 to 21% in 2010 in the use of nonexpanded cells. This seems to be a signal of the desire to limit the complexity and the morbidity of two-stage surgical procedures. The development of one-stage procedures alleviates the need for double surgery and extensive waiting time between biopsy and graft delivery. Currently, only autologous chondrocyte-based therapy has a clinically proven track record. However, the focus is shifting toward the use of MSCs from diverse sources to be applied in one-stage procedures with or without addition of growth factors, bone marrow concentrates, and other cell types and/or biomaterials. 13
Another interesting observation from this survey is the use of membranes or gels as delivery substances. Their rise from 12% in 2009 to 38% in 2010 clearly demonstrates the increased acceptance of biomaterials but may also reflect the demand for higher reliability of delivery, appropriate cell dosing, and possibly arthroscopic or minimally invasive graft delivery, for which injectables or synthetic carriers are essential. These changes will progress most likely to a level where injectable and malleable biomaterials will be used in all procedures, replacing the need for additional harvesting of patient's own tissue (e.g., periosteal flap) for the application of the cell product.
What will be the next developments in cell-based cartilage repair? The application of cell therapy to the treatment of critically sized defects or in osteoarthritis is a great challenge and would have considerable impact on the field.14,15 Another challenge is the need to establish registered products for specific indications based on multiple prospective randomized trials and in turn to address the large financial and regulatory burden these trials produce. The associated risk is to slow down the implementation of innovation and to exclude the smaller initiatives, thus creating a bias toward large pharmaceutical companies, which may or may not be desirable. Broader and more standardized clinical trials/use of cell-based grafts will require to introduce manufacturing paradigms inspired from other well-established biotechnology sectors, for example an automated production within closed bioreactor systems. 16 Finally, a European harmonization of guidelines of eligibility for reimbursement by health insurances will have to be targeted. Most professional orthopedic organizations agree on a clinical treatment algorithm for cartilage defects and this professional consensus should be the guide for policy makers and healthcare providers.17–19
Conclusions
The progressive increase in the number of reporting teams using the dedicated form and the number of total treatments being claimed (respectively 25% and 11% from the previous year) indicates that the inter-society program of the survey on novel cellular therapies is becoming a reference platform for access to information that is not available in public databases or scientific publications. Nevertheless, we are aware that several active teams in Europe have not reported treatments and therefore, the data in this survey represent an underestimation of the actual number of novel cellular therapies and groups involved. The use of a more organically structured query form, which has been introduced for the collection of 2011 data, together with the planned headhunting for active teams not yet reporting treatments, are expected to further consolidate the program. Moreover, while published and registered studies provide a complementary type of information, released with a different timing as compared with this survey, we expect that only an integrated use of the different instruments will allow to effectively monitor changes and trends in cell-based therapeutic strategies.
Footnotes
Acknowledgments
We greatly appreciate the cooperation of all participating teams and their staff (listed in the ![]() ) and the engagement of the different working groups and their highly committed representatives, namely TERMIS-EU (Sarah Wilburn), ISCT-Europe (Francesco Lanza), ICRS (Stephan Seiler), EBMT (Alejandro Madrigal), and EULAR. We are grateful to Dietlinde John for her database support and to Anke Wixmerten for her help in editing the collected data. The work was supported in part by the European Leukaemia Net LSH-2002-2.2.0-3. EBMT is supported by grants from the corporate members: Amgen Europe, Gilead Sciences UK, Miltenyl Biotec GmbH, Schering-Plough, Celegene International SARL, Genzyme, Fresenius Biotech GmbH, CaridianBCT Europe NV, Therakos, Cephalon, F. Hoffmann-La Roche Ltd., Gentium SpA, Pierre Fabre Médicament, Alexion Europe, Pfizer, Merck Sharp and Dohme, Chugai Sanofi–Aventis, Novartis, Hospira, and MacroPharma.
) and the engagement of the different working groups and their highly committed representatives, namely TERMIS-EU (Sarah Wilburn), ISCT-Europe (Francesco Lanza), ICRS (Stephan Seiler), EBMT (Alejandro Madrigal), and EULAR. We are grateful to Dietlinde John for her database support and to Anke Wixmerten for her help in editing the collected data. The work was supported in part by the European Leukaemia Net LSH-2002-2.2.0-3. EBMT is supported by grants from the corporate members: Amgen Europe, Gilead Sciences UK, Miltenyl Biotec GmbH, Schering-Plough, Celegene International SARL, Genzyme, Fresenius Biotech GmbH, CaridianBCT Europe NV, Therakos, Cephalon, F. Hoffmann-La Roche Ltd., Gentium SpA, Pierre Fabre Médicament, Alexion Europe, Pfizer, Merck Sharp and Dohme, Chugai Sanofi–Aventis, Novartis, Hospira, and MacroPharma.
Disclosure Statement
There are no conflicts of interest to declare. Writing of the article was the sole responsibility of the authors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.