
Abstract
Stem cell therapy represents a potential novel additional therapy for acute myocardial infarction. Cardiac applications of stem cell therapy are now undergoing clinical trials though many properties, including localization, possible adhesion, and infiltration of the injected stem cells in the myocardium, have not been studied in detail even in vitro. To study these mechanisms in a controlled microenvironment, we developed a model where mesenchymal stem cells (MSCs) were transported into live, cultured cardiac explants for further co-culture. About 10×103 porcine MSCs were injected into freshly excised and isolated cardiac explants of the pig. The explants were present in the culture medium for up to 7 days, with the time course of viability of the myocardial tissue, and the migration and the localization of the injected MSCs were analyzed with histological and immunohistological stainings. The myocyte structure was observed to be well preserved, and proliferation of capillaries and myofibroblasts was detected at the explant periphery. There were injected MSCs localized in the capillaries and in contact with the endothelial cells. The migration range and the number of adherent MSCs increased over time, suggesting active movement of MSCs in the explant. Our results suggest that this cardiac explant culture model is a feasible method for studying the effects of stem cells in the myocardium in vitro.
Introduction
It is known that when used in conjunction with AMI, stem cell therapy, for example, with bone marrow-derived mesenchymal stem cells (MSCs) can reduce the extent of inflammation and the number of apoptotic myocytes in the infarct border zone through.4,5 In addition, stem cell transplantation also diminishes the amount of fibrosis and induces angiogenesis. 6 The positive effect of MSC transplantation is postulated not only to be a consequence of stem cell proliferation and differentiation of the transplanted MSCS into functional cells but also to a great extent due to paracrine effects. Previously it was thought that the predominant effect was mediated through stem cell differentiation into myocytes and vascular cells, but now it is assumed that the immunomodulatory growth factors secreted by the MSCs play a key role. At present, several delivery routes such as intracoronary, intramyocardial, and intraventricular transplantation methods have been used.7–9 Direct injection of the stem cells into the myocardial tissue targets them to the target area, but there are doubts whether the infarcted myocardial tissue is a truly viable environment to allow stem cell survival. 1
The types of cell therapy used in myocardial repair can be subdivided into two different approaches. Implantation of in vitro engineered tissue constructs is one alternative approach with adult stem cells representing a most promising cell source for regenerative medicine. 10 In particular, the plasticity of adult stem cells strongly favors their use in tissue engineering. There are studies revealing the potential of bone marrow mononuclear cells to differentiate into cardiomyocyte-like cells. 11 Implantation of isolated cells into myocardium is widely used, but detailed information about how transplanted stem cells adapt to their new microenvironment remains unclear. An in vitro study has revealed that the presence of anti-inflammatory cytokines in the platform can support the growth of human MSCs. 12 Despite the clinical stem cell therapy studies now being conducted, neither the development nor the immediate outcome of the MSCs after myocardial injection has been reported, possibly due to technical difficulties.8,13
The purpose of this study was to develop an in vitro model to simulate the myocardium environment under tissue stress and to study in detail the behavior of the injected MSCs in cardiac tissue. We compared the properties of two different cardiac explant models and used several microscopy techniques to study the localization of the injected MSCs and the structural changes in the MSCs and the surrounding tissue. The pig was chosen as the laboratory animal because of its size and its other tissue-level similarities to humans in regard to their cardiovascular system and the availability of the myocardial tissue and stem cell material.
Materials and Methods
Animals
The animals were maintained and the procedures were performed in accordance with the European Convention for the protection of vertebrate animals being used for experimental and other scientific purposes (ETS 123, Council of Europe 2006) and the European Union recommendation on guidelines for the accommodation and care of animals used for experimental and other scientific purposes (2007/526/EC). The study was approved by the Finnish Animal Ethics Committee.
Seven healthy female landrace pigs (8–10 weeks of age) were used in this study. The animals were sedated by intramuscular injection of ketamine hydrochloride (350 mg) and midazolam (45 mg). A peripheral catheter was inserted into a vein to allow administration of drugs and fluids.
Isolation of mononuclear stem cells
The animals were sedated and placed in the supine position. To harvest mononuclear cells from the bone marrow, 2×10 mL of bone marrow was aspirated from beneath the tibial tuberosity into a syringe containing 5000 IU of heparin and delivered to the laboratory for isolation. The bone marrow aspirate was diluted to 1:6 in phosphate-buffered saline (Sigma-Aldrich) and then subjected to a density-gradient centrifugation (Ficoll-Paque Plus; Amersham Biosciences) to exclude granulocytes and erythrocytes. After collecting mononuclear cells from the interphase, they were washed three times with phosphate-buffered saline.
Culture of stem cells
Mononuclear cells were plated for 2 days with hematopoietic and other nonadherent cells being washed away during medium changes. On the basis of adhesive properties of the MSCs, they were then collected and expanded in culture and labeled. The plastic-adherent cells were cultured in Minimum Essential Medium Eagle alpha modification supplemented with 10% fetal calf serum (Promo Cell), 100 U/mL penicillin, 0.1 g/L streptomycin, 20 mM HEPES, and 2 mM L-glutamine (all reagents from Sigma-Aldrich unless otherwise indicated). Half of the medium was replaced twice a week during culture with the cells being passaged (passage 2–4) when they reached confluence.
Characterization and functionality of stem cells
Pig MSCs were characterized with flow cytometry after incubation with conjugated antibodies (Acris Antobodies) recognizing the cell surface antigens. We could not perform all of the tests required by the International Society for Cell Therapy due to insufficient and inappropriate availability of antibodies for pig cells. More than 95% of the cultured cells were positive for CD105, CD44, CD29, and CD46, while less than 2% of the cells were positive for CD45 and CD31 (data not shown). The antibody treatments and flow cytometry were performed as previously described. 14
To confirm the viability of the MSCs, Annexin 5 and propidium iodide tests were performed according to the manufacturer's (BD Biosciences) instructions as previously described. 14 The viability tests for MSC before injection to myocardium revealed only a small number of apoptotic cells (≤3%) (data not shown).
The effect of ultrasmall super paramagnetic iron oxide (USPIO) labeling on cellular proliferation rate was assessed by culturing control cells and MSCs and analyzing them with the (3-(4,5-dimethylthiazol-2-yl)-2,5-)diphenyltetrazolium bromide assay (tetrazole, MTT; Sigma-Aldrich) according to the manufacturer's instructions. Briefly, 500 cells/well were plated in six replicate wells per sample, cultured for 3, 7, and 10 days and incubated for 2 h with MTT (0.5 mg/mL) at 37°C. The cells were lysed in dimethylsulfoxide and absorbance was read at 550 nm against 650 nm.
The cultured MSCs were confirmed to have differentiation potential toward osteogenic and adipogenic lineages. Briefly, adipocytic differentiation was induced with adipogenesis-inducing medium (Minimum Essential Medium Eagle alpha modification supplemented with 2% fetal calf serum [Promo Cell], 100 U/mL penicillin, 0.1 g/L streptomycin, 10 μg/mL insulin [Novo Nordisk], 0.1 μM dexamethasone, 0.1 mM indomethasine, and 2 mM L-glutamine [all reagents from Sigma-Aldrich unless otherwise indicated]). The cells were cultured for 3 weeks, after which the cells were fixed with 3% paraformaldehyde and stained with 0.2% Sudan III (Sigma-Aldrich) in 50% isopropanol and evaluated according to their morphology with the osteoblast differentiation test being performed as previously described. 14
Labeling of stem cells
Fluorescent Vybrant CM-DiI dye- and super paramagnetic iron oxide (SPIO) labeling were used to detect the injected MSCs in the histological studies. Two different labeling methods were used in order to ascertain that labeling does not affect the MSCs and infiltration results. Vybrant CM-DiI dye labeling was conducted according to the manufacturer's instructions (Invitrogen). SPIO labeling (39 mg/mL ferucarbotran corresponding to 36 mM of iron) was performed by incubating the stem cells overnight with Resovist (Bayer) in 37°C. After labeling, the MSCs were washed twice with PBS and trypsinized. The total of MSC amount was counted and suspended in a saline solution to a density of 10×103 (group 1) or 100×103 (group 2 explants) MSCs in 30 μL.
Preparation of cardiac explants
After heparin administration (500 IU/kg), the sedated pigs were sacrificed with an intravenous injection of pentobarbital (60 mg/kg) and the hearts were removed under sterile conditions. The ventricles were placed for 15 min in a special buffer that was designed to maintain the viability of the tissue. The buffer was composed of glutamine acid 70 mM, taurine 15 mM, KCl 30 mM, glucose 11 mM, KH2PO4 10 mM, MgCl2 0.5 mM, Hepes 10 mM, and Egta 0.5 mM. Titration of the buffer to pH 7.3 was achieved with KOH. A biopsy needle (Kai Medical) was used to prepare cardiac explants from the ventricles and to standardize the size of the explants to 6×8 mm (226 mm3).
Cardiac explants and stem cell delivery: control group, group 1, and group 2
Two different in vitro cardiac explant culture models were developed, and therefore the explants were divided into three groups: the control group, group 1, and group 2.
The control group consisted of 20 explants, and in this case 30 μL of saline was injected in a standardized manner into the center of the explants using a 27G×¾ needle and a 1 mL syringe. Group 1 consisted of 60 explants. A total of 10×103 of allogenic DiI- or SPIO-labeled stem cells in a volume of 30 μL were injected into the explants in the same standardized manner as in the control group (Fig. 1). Both the control group and group 1 explants were transported into 24-well plates containing Minimum Essential Medium Eagle alpha and supplements as described earlier.
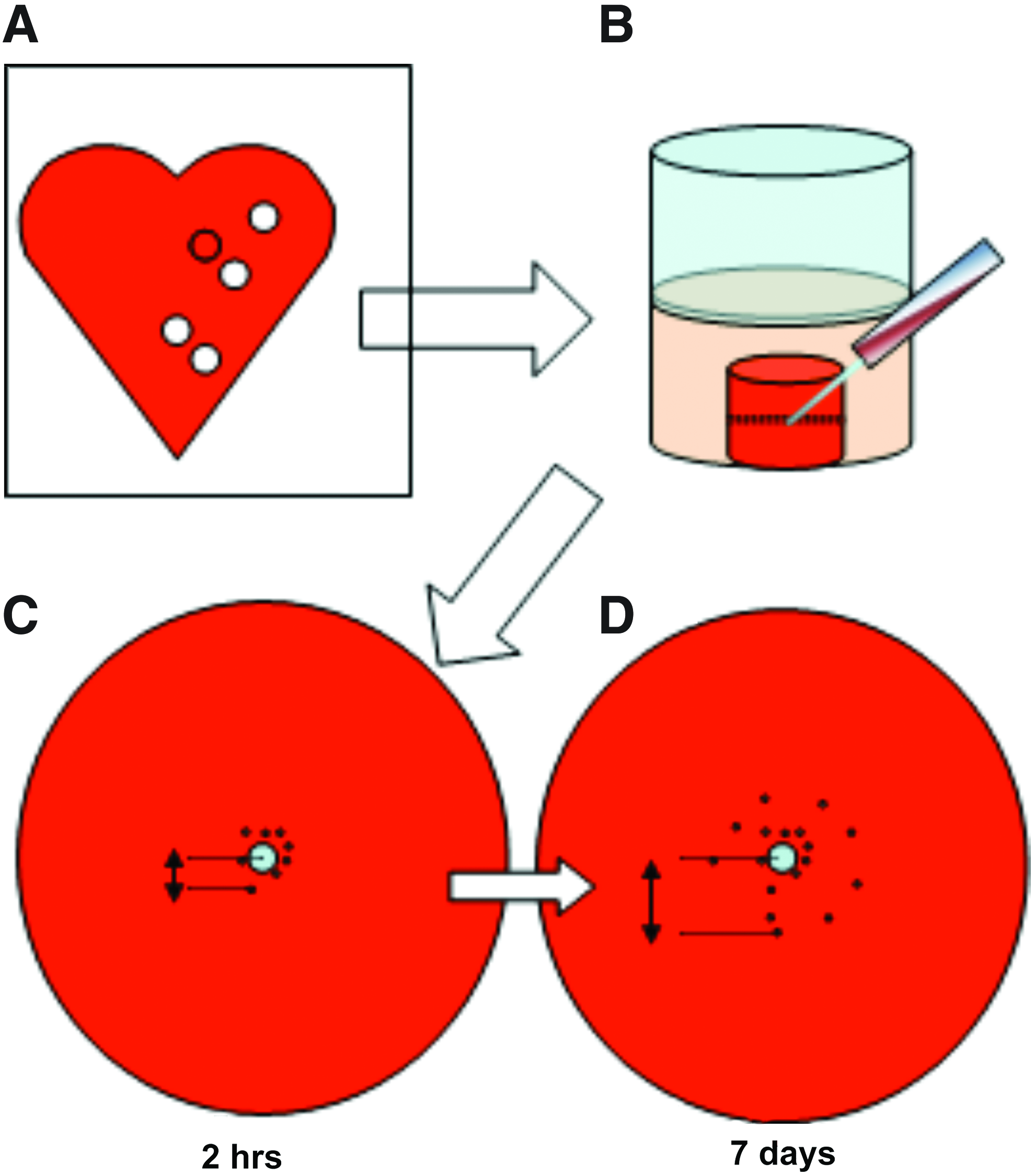
Method to study stem cell invasion by using in vitro cardiac explant culture model.
For the control group and group 1, the method for recognition of the center of the entry point was clarified in detail by conducting pilot experiments and different dyes, for example, methylene blue, were used as were microspheres. The dyes were not reliably visible, and the microspheres induced a dormant effect in the injected cells causing interference with the migration process. Thus, it was concluded that careful sectioning of the sample must be done in order to recognize the center of the entry point from the histological samples.
Group 2 consisted of 48 explants. The group 2 explants were set into the inserts of the Millicell-96 Cell Culture Insert Plate (Millipore). A total of 100×103 of DiI- or SPIO-labeled MSCs in a volume of 30 μL were carefully placed onto the top of the cardiac explants via a syringe. Both the explant in the insert and the culture media were set into the chamber. The cardiac explants fitted snugly and filled the whole upper well such that the SPIO or fluorescent DiI dye-labeled stem cells could not be flushed away from the surface of the cardiac explants.
Culture media were replaced daily from each explant group. At every time point (2 h, 48 h, 72 h, 7 days), six cardiac explants were taken from the culture media and fixed in formalin.
Histochemistry and immunohistochemistry
The cardiac explants were fixed in 10% formaldehyde and embedded in paraffin. Tissue samples were sectioned (4 μm) and deparaffinized.
Histological stainings of hematoxylin and eosin (H&E), Prussian blue, and Mallory's phosphotungstic acid hematoxylin (PTAH) was conducted using standard protocols. In brief, for the Prussian blue staining, sections were incubated for 30 min in 2% potassium ferrocyanide, which labels intracellular iron of the SPIO-labeled MSCs as a blue color. PTAH highlights muscle striata, fibrin and nuclei in blue, and elastic fibers as a deep brownish or red color.
Immunohistochemical stainings against α-smooth muscle actin (α-SMA), desmin, and a platelet/endothelial cell adhesion molecule (PECAM-1) was used in order to clarify the localization of the injected MSCs and to specify the different cell types. α-SMA detects myofibroblasts as well as vascular smooth muscle cells and the pericytes that surround the capillaries. Desmin labels both striated (skeletal and cardiac) and smooth muscle cells. PECAM-1 was used to identify endothelial cells. Cell proliferation was assayed with Ki67 immunohistochemical staining. Ki-67 detects a protein expressed by the cells in the proliferative phases, that is, G1, G2, M, and S of the cell cycle. For α-SMA and desmin, the Dako Envision Kit (Dako) was applied for the IHC with a 30 min incubation for the primary antibody. For PECAM-1, a Goat Kit was used with a 60 min incubation for the primary antibody. The sections incubated with PBS instead of the primary antibody were used as the negative control. Ki-67 antibody was detected with a polymer-based system using automated Leica Bond III Tissue stainer (Leica Microsystems) according to the manufacturer's instructions. The list of the antibodies, dilutions, and antigen retrieval methods used in this study are shown in Table 1.
Microwave heat treatment; bTris-EDTA buffer, pH 9.0; cCitrate buffer, pH 6.0.
α-SMA, α-smooth muscle actin; PECAM-1, platelet/endothelial cell adhesion molecule.
Analysis of histochemistry and immunohistochemistry
H&E was used to investigate the viability of the explants by studying the morphology of the different cell types and by searching for signs of myocyte striation, apoptosis, degeneration, and edema.
Prussian blue was used to detect the SPIO-labeled stem cells and to evaluate their localization inside the explants. SPIO-labeled MSCs were evaluated according to their color intensity, shape, and size with Prussian blue staining. The possible intravascular localization of the stem cells was examined as well as their adherence to the endothelium or myocytes. The criteria for the adherence of a stem cell to the endothelium were defined as a positive staining reaction for Prussian blue and an elongated shape of a stem cell adjacent to an endothelial cell or myocyte.
Fluorescence microscopy was used to detect DiI dye-labeled stem cells and to evaluate their localization inside the explants. DiI dye-labeled stem cells were assessed according to their size, shape, and color intensity. However, due to technical challenges, it proved impossible to measure the migration range using DiI dye.
The infiltration range of the stem cells from the injection site into the cardiac explant was assessed in a light microscope. The site of the injection was defined by a star-shaped cleft in the middle of the explant. Quantification of the infiltration range was done by measuring the maximal distance from the center of the injection site into the furthest stem cell. A commercial computer program was used for quantification (Scientific Image Analysis, MCID_m4 3.0 Rev 1.1).
Possible intravascular localization of the stem cells and characterization of the different cells types were specified by immunohistochemical stainings. The presence of endothelial cells in arterioles and capillaries was recognized by positivity for PECAM-1 and a positive smooth muscle layer or a rim of pericytes stained positively for α-SMA. Cells positive for desmin were interpreted as being muscle cells. Spindle-shaped cells positive for α-SMA but negative for desmin and PECAM-1 were designated being myofibroblasts. 15
Finally, quantification of the capillary structures in the control group and group 1 was conducted. The quantity of the capillary proliferation at the marginal zone was estimated at 7 days with a commercial computer program (Scientific Image Analysis, MCID_m4 3.0 Rev 1.1). The proportional area of the cell coverage was counted based on PECAM-1 staining with 10 images from the marginal zone of each explant being analyzed.
Statistical analysis
Statistical analysis was performed with the SPSS statistical program (SPSS SmartViewer version 15.0, SPSS, Inc.). According to the Kolmogorov–Smirnov's normality test, an independent samples t-test could be used to evaluate both adhesion and invasion of the MSCs. All results are presented as mean and standard deviation. A p-value less than 0.05 was considered as statistically significant.
Results
Function of stem cells
We tested the effect of USPIO labeling on the viability of the cultured pig MSCs using MTT and functional tests (data not shown). In agreement with other reports, we could not find any detrimental effect on long-term MSC viability caused by this label.16,17
Changes in the morphology of the explants
Control group and group 1
There was no difference in the myocardial histology between the control group and group 1 and the structure of the myocytes was well preserved in both groups after 7 days in the culture. The PTAH staining revealed organized actin filament structures at all time points (Fig 2A, B). After 7 days, there was degeneration, swelling, and apoptosis of endothelial cells in the center of the explants (Fig. 2D, E). At this time point, half of the biopsies in the control group and all the biopsies in group 1 were also surrounded by spindle-shaped cells which were positive for α-SMA but negative for desmin and PECAM-1 (Figs. 2G, H and 3A, B, D, E, J, K). In addition, there was budding of PECAM-1-positive endothelial cells and capillaries at the marginal zone of the explants at the 7 day time point (Fig. 3G, H). The proportional area of the PECAM-1-positive staining was analyzed to quantify the extent of capillary proliferation at the marginal zone but no statistically significant differences were observed (results now shown).

Histological findings of the cardiac explants after 7 days in the culture.
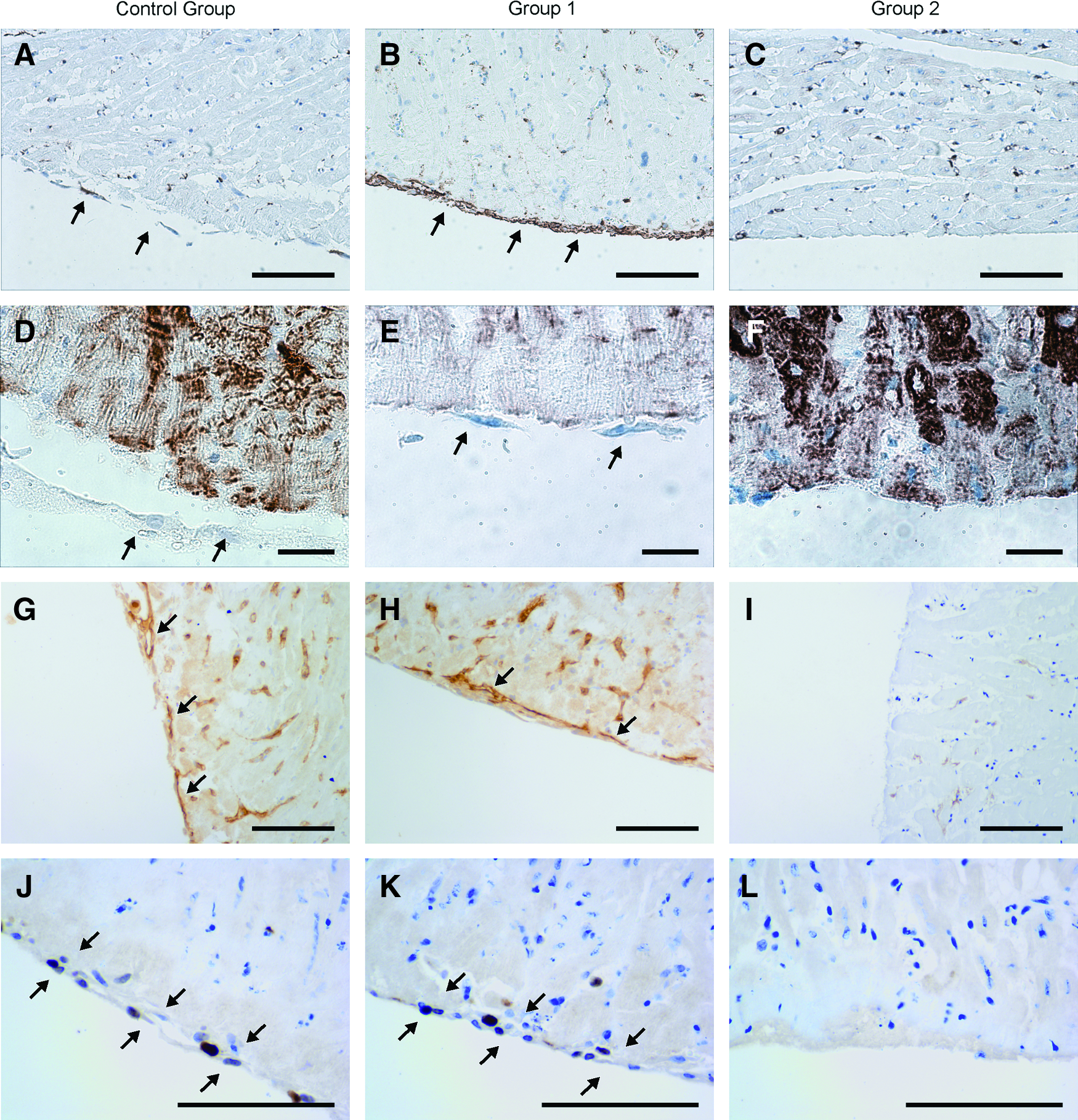
Immunohistological findings of the cardiac explants after 7 days in the culture.
Group 2
In group 2, there was variable and often extensive extracellular edema and degeneration of the myocytes in the explants after 7 days in the culture (Fig. 2C). There was also vacuolization, edema, and degeneration of endothelial cells, even total destruction of the capillaries (Fig. 2F). No proliferation of spindle-shaped cells or capillaries was observed at the marginal zone at the 7 day time point (Fig. 2I and 3C, F, I, L).
MSC localization and morphology
Control group and group 1
In group 1, Dil- or SPIO-labeled MSCs were injected into the center of the cardiac explants. The function of the MSCs was not affected by the labeling methods and changes were observed in the morphology and localization of MSCs examined with both labeling techniques.
MSCs were mainly localized in slit-like spaces, some of which could be identified as capillaries with PECAM staining. The injected MSCs often remained in aggregates but also single cells were observed. Injected MSCs were found outside the initial injection site in all explants, and the distance from the injection site increased during the follow-up (Fig. 4A–D). However, the exact localization of the SPIO-labeled MSCs was much easier to define compared to that of the Dil-labeled MSCs; thus, it was possible to measure the distance of the MSCs from the injection point at 7 days; only the SPIO-labeled MSCs were evaluated. The results indicate that there was a significant difference in the range of migration between the time points of 2 h (mean 1193 μm, SD 288 μm) and 7 days (mean 1384 μm, SD 255 μm; p=0.02). The maximal ranges at the different time points are shown in Figure 4E.
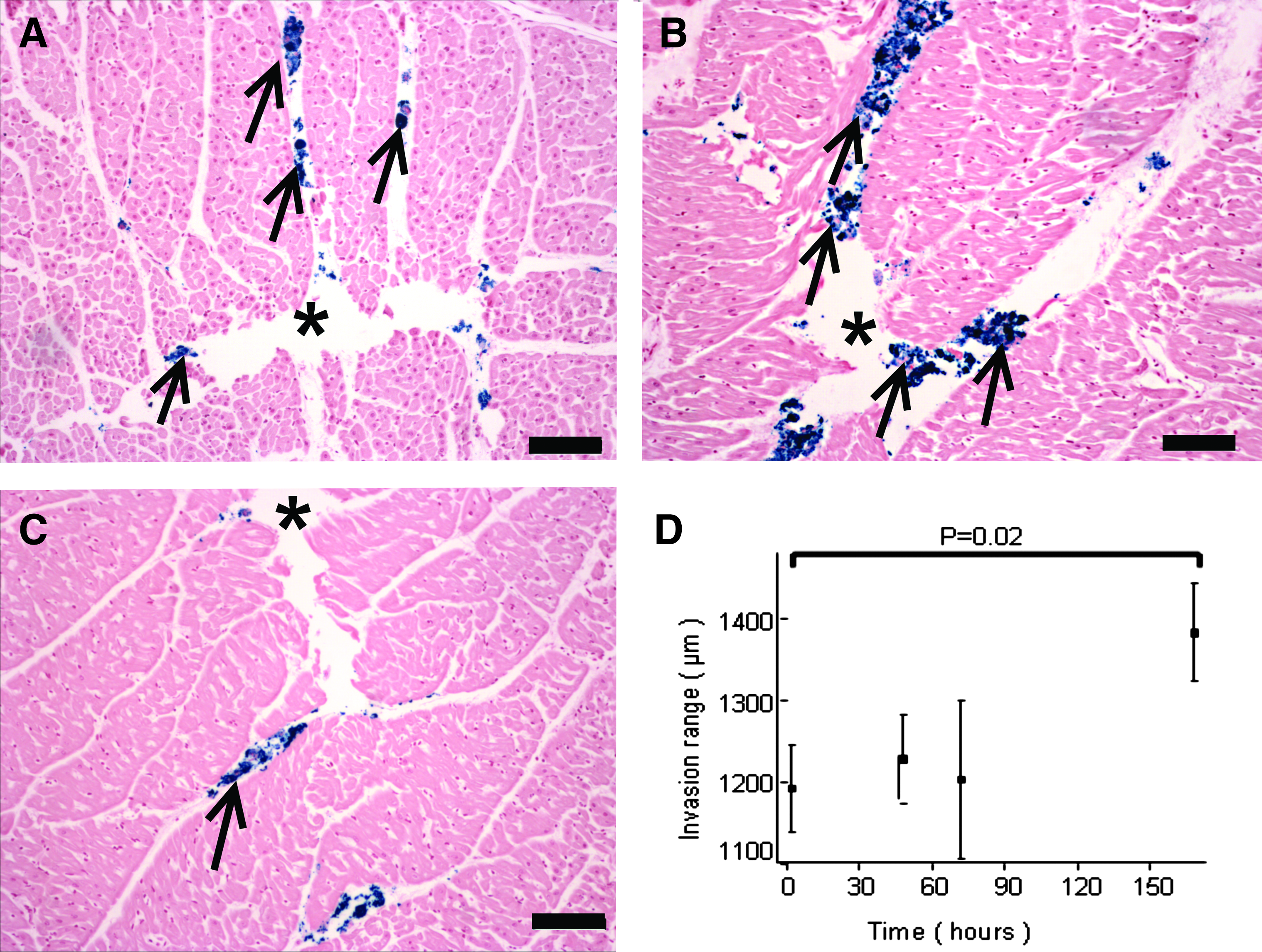
Distance of the super paramagnetic iron oxide (SPIO)-labeled stem cells from the injection site at different time points in group 1. Stem cells were directly injected into the center of the cardiac explants and Prussian blue staining was used to detect the injected stem cells (arrows). Injection sites (*) and infiltrated stem cells (arrows) at different time points
There were changes observed in the morphology of the MSCs. Some of the MSCs became elongated and flattened and localized parallelly along capillary endothelial cells or myocytes (Fig. 5A–C). This change in morphology and localization was observed in both DI- and SPIO-labeled stem cells and at all time points. Already after 2 h, there were single stem cells in close contact with myocytes and endothelial cells, but the number of stem cells in contact with endothelial cells or myocytes increased during the follow-up period. There was a statistically significant (p<0.05) difference in the number of the SPIO-labeled stem cells in contact with endothelium or myocytes between the time points of 2 h (mean 1.43, SD 1.342) and 7 days (mean 4.00, SD 0.816). The number of the SPIO-labeled stem cells in contact with endothelium or myocytes at 2 h, 48 h, 72 h, and 7 days are shown in Figure 5D.

Morphological change of the injected stem cells in the cardiac explant culture model.
Group 2
In group 2, MSCs were placed on the surface of the explant. No significant stem cell migration deeper into the explant was observed, and after 7 days, 85% of the DI-labeled stem cells were still on the surface.
Discussion
We have developed a new explant model with which to examine MSCs in myocardium in vitro, and as far as we are aware, this study is the first to reveal the fate of injected stem cells in myocardial tissue by using a cardiac explant culture model. The aim of the study was to monitor the location and possible adaptation of the MSCs after injection into live myocardial tissue. Since the myocardial tissue explants have no circulation and their intake of oxygen and nutrients depends on diffusion, our model also possibly simulates myocardial tissue stress.
The size of the explant was selected after pilot experiments as one that allowed the maximal dimension without any significant decay of cardiomyocytes. In the 6-mm-diameter cardiac explants, the morphology of the myocytes was fully preserved in both the controls and group 1. This indicates that myocytes remain viable during the culture, and diffusion can supply enough of nutrients to explants. In addition, after the preparation, the cardiac explants did not respond to electric stimulation by contraction (data not shown). We conclude that the myocytes remain viable in a dormant state that requires less energy, which is analogous to the in vivo myocardial tissue reaction observed in MRI and ultrasound. 18 In this dormant state, the myocytes are resting and remain viable but are not able to contract. This phenomenon can partially explain the good preservation of the myocytes in our explants.
Degeneration and apoptosis of endothelial cells was observed in the center of the cardiac explants in all of the study groups (Fig. 3). In an effort to confirm endothelial apoptosis or induction of apoptosis, we initially utilized caspase-3 and/or TUNEL, but despite several attempts, TUNEL or caspase-3 did not function when applied to the myocardial tissue of the pig. However, endothelial cell apoptosis was readily and reliably recognized by an experienced pathologist based on the presence of apoptotic bodies, which are a hallmark of apoptosis. 19 Endothelial cell degeneration and apoptosis are associated with a number of diseases and conditions, and in our study setting the degeneration and apoptotic activity of the endothelium in the control group and study group 1 are possibly a nonspecific finding due to the mechanical manipulation of the myocardial tissue. 10 It is also possible that the endothelial cells are more sensitive to tissue hypoxia than the myocytes. However, in the explants placed in the inserts, there was true capillary degeneration.
At the 7-day time point there was capillary budding partly forming a rim-like structure of newly formed endothelial cells at the marginal zones of both controls and group 1 explants. This was interpreted as being real capillary proliferation and confirms that the endothelial cells are capable of regeneration also in the explant culture model (Fig. 3). In addition, there was a rim of spindle-shaped cells at the margins of the biopsies at the 7-day time point in the control group and group 1 explants. These cells were positive for α-SMA but negative for desmin and PECAM, and they were interpreted as being myofibroblasts. 15 The viability of the myocytes and the adaptation of the endothelial cells and fibroblasts/myofibroblasts to the explant culture conditions are evidence that our cardiac explant culture model is a feasible method for simulating myocardial tissue in vitro.
It was observed that the explants placed into the inserts in group 2 had deteriorated after 7 days in culture. There was extensive extracellular edema, degeneration of capillaries, and the muscle striation was poorly preserved (Fig. 2C, F). Furthermore, no myofibroblast or capillary proliferation at the margins of the explants was seen (Fig. 2I and Fig. 3C, F, I, L). Evidently, culture of the explants in an insert prevents nutrient diffusion into the explants and diminishes their viability. When the explants are placed tightly into the insert, this may also produce a mechanical barrier that hinders proliferation of new cells. Overall, the findings from group 2 suggest that the use of inserts is not beneficial for culturing cardiac explants.
Our data show that the injected MSCs were localized in slit-like spaces within the myocardium, some of which were lined by endothelial cells, and thus they were identified as capillaries. With the progression of time, MSCs were found farther from the initial injection site evidence for active migration. In group 1, both the SPIO- and DI-labeled MSCs soon came into contact with the endothelium and the myocytes. These MSCs were elongated and flattened (Fig. 5), and the change in their localization and morphology was interpreted as being due to an adherence of the MSCs to the mesenchymal cells. 9 With time, both the migration range and the number of adherent MSCs increased, but the first signs of MSC adhesion appeared already at 2 h after injection. The migration and adhesion of the injected MSCs indicate that the transplanted stem cells remain viable for several days even in vitro. Our findings also indicate that the MSCs quickly adapt to their new biological environment and actively interact with myocardial tissue immediately after their transplantation. Steingen et al. used several in vitro models to demonstrate transmigration and the invasive characteristics of MSCs and demonstrated that MSCs transmigrate quickly underneath the endothelial cell monolayer within 240 min in vitro. 9 This finding is consistent with our results of MSC adhesion occurring 2 h after injection.
The fact that the number of adherent MSCs increases with time indicates that the MSCs remain viable and active for up to 7 days after transplantation in to myocardial tissue. Active migration of MSCs presumably enables therapeutic paracrine effects of the MSCs to spread widely throughout the myocardial tissue. It is assumed that immunomodulatory growth factors secreted by MSCs play a key role in the remodeling process after AMI. 20 Injection of MSCs after AMI diminishes fibrosis, reduces myocyte apoptosis, and induces angiogenesis, which consequently diminishes scar formation and infarction size and improves cardiac function. 13 In ischemic myocardial tissue, the MSCs have been reported to promote angiogenesis and decrease cardiomyocyte apoptosis after transplantation into the infarcted area.13,21,22 In addition, the effects of the stem cell therapy can be improved by special treatments and gene modification of the transplanted stem cells. 17 For example, overexpression of the chemokine receptor CCR1 has been shown to enhance the migration, survival, and engraftment of MSCs. Treatment with PDGF-BB seems to prevent later loss of transplanted bone marrow cells, presumably by inhibition of apoptosis.23,24 Our data suggest that the loss of the beneficial effects is not due to apoptosis or incapacity of the transplanted cells but rather to be a consequence of the hostile, inflammatory tissue environment in which the cells must operate in vivo.
AMI evokes an ischemic injury and decreased myocardial function. A considerable number of studies have shown that intramyocardial injection of MSCs after AMI can improve cardiac function.22,25,26 Direct intramyocardial injection seems to contribute to the measurable release of cardiac biomarkers (e.g., CK-MB) associated with myocardial damage. However, direct injection does not cause any ECG changes or ventricular arrhythmias. 27 Thus, the intramyocardial injection can be considered as a feasible transplantation method for stem cells. However, although the intramyocardial injection method is currently being used in clinical trials, there is little data on the immediate outcome of the injected cells in the microenvironment.28,29
The cardiac explant culture model is an in vitro preparation that has numerous limitations compared to the in vivo situation. The model simulates to some degree the lack of nutrients and oxygen; hence, it can also simulate tissue stress. However, the lack of immunomodulatory cells normally derived from the circulatory system naturally limits the extent of inflammation present in the explants. Therefore, the possible anti-inflammatory effects of stem cells and their interaction with inflammatory cells cannot be studied in this in vitro model without adding them artificially into the preparation. In vivo, the blood and lymph circulation and muscle contraction would presumably also improve the migration of MSCs. It is noteworthy that even though the in vitro model lacks these factors, MSCs still were able to migrate deep into the cardiac explant during the follow-up. Hence, one obvious improvement to our model would be to collect the myocardial tissue explants at various time points after experimentally induced infarction, which would allow homing of endogenous inflammatory cells in a controllable manner.
This study focused on investigating the immediate outcome of intramyocardially injected MSCs and the development of a new cardiac explant model. We have also shown that our model is suitable for studying labeling methods for MSCs. This model can be developed further by incorporating chemical and biological modifications, such as controlling for the presence of inflammatory cells or cytokines or modifying the oxygen level. Hence, this in vitro model may allow studies that are not possible to be conducted in vivo. In conclusion, our cardiac explant culture model is a feasible method for studying myocardial tissue in vitro and determining the outcome and adaptation of MSCs after injection into cardiac tissue.
Footnotes
Acknowledgments
The study was supported by Finnish Foundation for Cardiovascular Research and the state subsidy for the University hospital of Oulu. The staining protocol for PECAM was kindly proposed by Tuomas Rissanen, MD, PhD, Kuopio University Hospital. The skilful assistance of Ms. Lissu Hukkanen, Ms. Mirja Vahera, Ms. Erja Tomperi, Ms. Riitta Vuento, and Mr. Hannu Wäänänen is kindly acknowledged.
Disclosure Statement
Research project was sponsored by Finnish Foundation for Cardiovascular Research and the state subsidy for the University Hospital of Oulu. No competing financial interests exist.