
Abstract
Anterior cruciate ligament (ACL) reconstruction with the hamstring tendon graft takes a long time, as the tendon graft needs to heal at the site of the bone–tendon integration in the created bone tunnels. Several reports have shown the therapeutic effects of simvastatin on bone formation with neovascularization. The aim of this study was to test the hypothesis that enhanced angiogenesis and osteogenesis by locally applied simvastatin promotes tendon–bone healing after ACL reconstruction. Rabbits received ACL reconstruction with hamstring tendon graft and were implanted with either simvastatin-conjugated gelatin hydrogel or gelatin hydrogel alone in their bone tunnels, and then bone regeneration and neovascularization at tendon–bone interface and biomechanical properties were assessed. Histological analysis at week 2 demonstrated that tendon–bone healing was significantly greater with angiogenesis and osteogenesis in the simvastatin-treated group than in the control group. Computed tomography at weeks 2 and 4 showed a significantly smaller tibial bone tunnel in the simvastatin-treated group. Biomechanical testing at week 2 demonstrated a significant increase in ultimate failure load in the simvastatin-treated group. This study suggested that local administration of low-dose simvastatin-conjugated gelatin hydrogel promotes the tendon–bone healing via its effect on both angiogenesis and osteogenesis at an early phase in a rabbit model, but does not affect biomechanical property in long-term after ACL reconstruction.
Introduction
Simvastatin, an inhibitor of the competitive 3-hydroxy-3-methyl-glutaryl coenzyme A reductase, is a convenient and economical drug, which has been widely used to treat hyperlipidemia. In recent years, it has been reported that statins possess pleiotropic effects that include improvement of endothelial effect,18,19 anti-inflammatory effect,20,21 and stimulation of angiogenesis.22,23 Additionally, since Mundy et al. found that statins could have an anabolic effect on bone formation both in vitro and in vivo by activating the promoter of the BMP-2 gene, 24 many observations and experiments investigating the favorable effects of statins on bone formation have been reported.24–29 In our previous study, Fukui et al. reported the efficacy of low-dose simvastatin for bone fracture healing stimulated by enhanced osteogenesis and angiogenesis. 29 Although several reports have shown a certain therapeutic effect of simvastatin on bone formation with neovascularization,24,25,27,30 systemic administration of simvastatin minimized these positive effects due to clearance in the liver, suggesting the need for high-dose administration that may then cause systemic adverse side effects.
To overcome the problem of low efficacy/frequent side effects by high doses of simvastatin treatment, we utilized biodegradable gelatin hydrogels as a tool for drug delivery for tendon–bone healing in ACL reconstruction. We aimed to test the hypothesis that enhanced angiogenesis and osteogenesis by local administration of low-dose simvastatin-conjugated gelatin hydrogel promote tendon–bone healing after ACL reconstruction.
Materials and Methods
Gelatin hydrogel
Simvastatin was provided by Merck & Co., Inc. The procedure for producing simvastatin-conjugated gelatin hydrogel has been described previously.28,29 Briefly, in the first step,
Surgical procedures
This animal experiment was approved by the Institutional Animal Care and Use Committee of Kobe University. Forty-two skeletally mature Japanese White Rabbits (Kitayama Labs) weighing between 3.0 and 3.5 kg were used in this study. All animals underwent bilateral ACL reconstruction under general anesthesia with an intravenous pentobarbital sodium solution (Kyoritsu-seiyaku, 30 mg/kg body weight). The bilateral limbs were disinfected before skin incisions were made. After subcutaneous injection of 3 mL of 1% lidocaine, the medial parapatellar approach was used to expose the knee joint. The native ACL was exposed and completely transected. The bone tunnels were created with the use of a 2.5-mm-diameter drill in the femur and tibia referred to as the insertion of the native ACL. An ipsilateral semitendinosus tendon was harvested as a graft, and gelatin hydrogel was wrapped by the tendon graft as much as possible not to disturb tendon–bone healing. The tendon graft with gelatin hydrogel was advanced though the tunnel. The amount of simvastatin applied to each bone tunnel was 125 μg in both femur and tibial bone tunnels. A total of 250 μg of gelatin hydrogel incorporating simvastatin was implanted in the right knees, and the gelatin hydrogel alone was implanted into the bone tunnels in the left knees to serve as the control group (Fig. 1). The dose of simvastatin was determined by a previous study assessing the effect on osteogenesis and angiogenesis. 29 The end of the graft was sutured at manual maximum tension to the periosteum and surrounding soft tissue using 4-0 Ethibond sutures (Ethicon, Inc.) at 90° of knee flexion. The retinacular incision and wound were closed in layers with 3-0 nylon sutures (Alfresa Co.). Postoperatively, the animals were then returned to their cages and permitted to bear full weight.
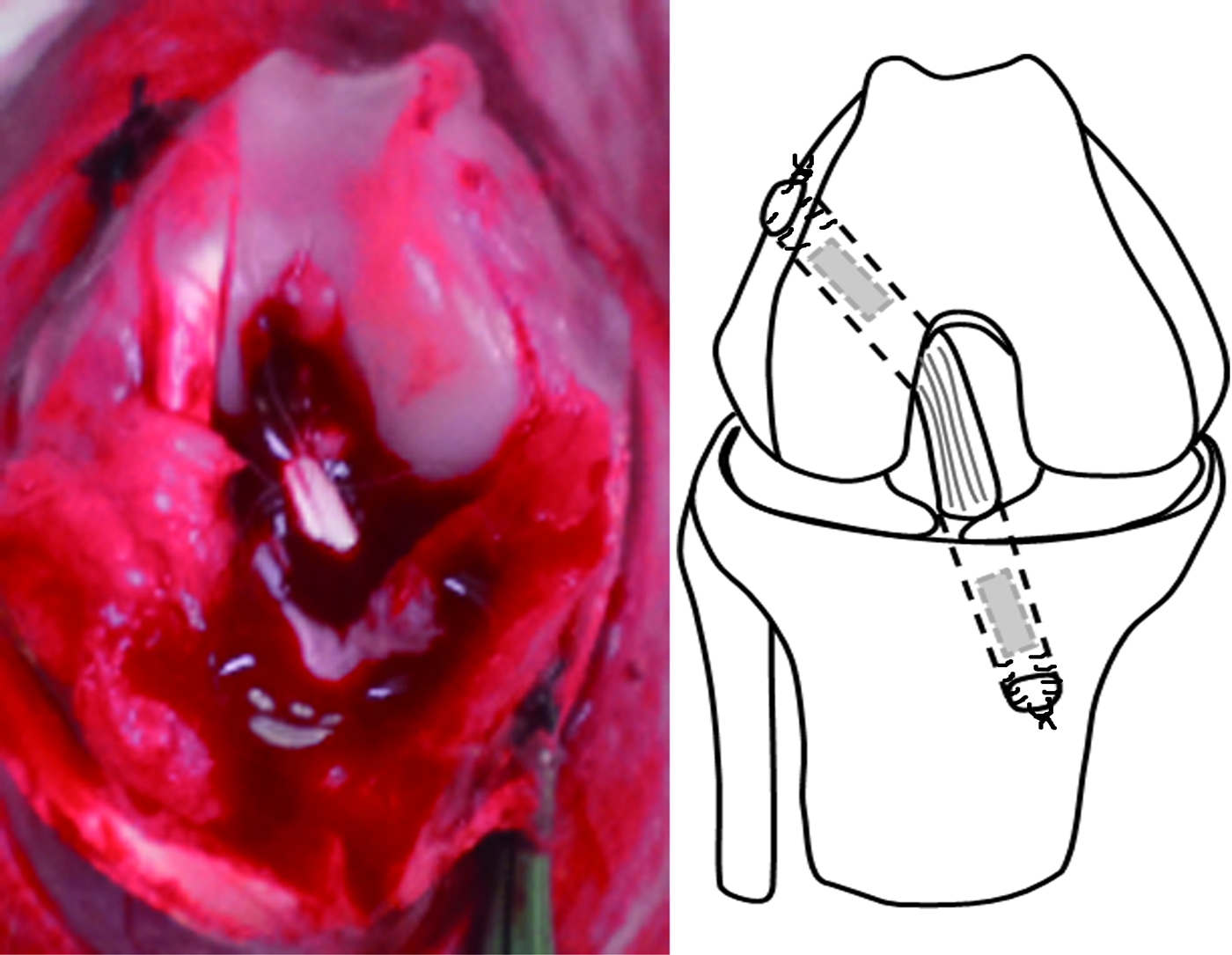
Surgical procedure of anterior cruciate ligament (ACL) reconstruction in this study. The hamstring tendon graft was passed though the bone tunnel. The proximal and distal ends of the graft were fixed to the periosteum using 4-0 Ethibond sutures. The gelatin hydrogels were implanted into both bone tunnels. Color images available online at www.liebertpub.com/tea
Each animal was sacrificed with the lethal injection of pentobarbital at either 2, 4, or 8 weeks after surgery for assessment: 21 rabbits for the histological assessment, 18 rabbits for the biomechanical assessments, and 3 rabbits treated with bevacizumab (Table 1).
The figures are expressed number of experimental animal.
Histology
Immediately after sacrifice, the specimens were fixed in 4% paraformaldehyde in 0.1 M phosphate-buffered saline (PBS) for 24 h. After each sample had been decalcified in 10% ethylenediaminetetraacetic acid with PBS at room temperature for 2 weeks, it was dehydrated with a graded alcohol solution and embedded in paraffin wax. The samples were sectioned parallel to the longitudinal axis of the tibial tunnel. For conventional light microscopy, sections were cut at 5 μm and stained with hematoxylin and eosin. Russell-Movat pentachrome stain was also performed to see the tendon–bone interface with light microscopy (n=5, at each group at each time point).
Immunohistochemical staining for evaluating angiogenesis
To assess angiogenesis at the tendon–bone interface, sections were prepared from paraffin-embedded samples at week 2 (n=5 at each group). Immunohistochemical staining for isolectin B4 (Vector Laboratories) as an endothelial cell marker was visualized with fluorescence, and the capillary density was morphometrically evaluated as the average value in five randomly selected fields (250 μm×250 μm) of the tendon–bone interface from each animal. Capillaries were recognized as tubular structures positive for isolectin B4. The two investigators performing immunohistochemical analysis were blinded to the animal treatment.
Immunohistochemical staining for evaluating osteogenesis
To analyze osteogenesis at the tendon–bone interface, osteocalcin was immunohistochemically stained (n=5 at each group). Briefly, sections were deparaffinized according to the standard procedures. Sections were treated with proteinase K (S3020; Dako) for 10 min at 37°C. Primary mouse anti-osteocalcin monoclonal antibody (Thermo Scientific) diluted 1:200 in a CanGet Signal® immunoreaction enhancer solution (TOYOBO) was placed on the section overnight at 4°C. Slides were washed with PBS after incubation for 2 h at room temperature with a fluorescent-labeled goat anti-mouse secondary antibody (Alexa Fluor® 546 goat anti-mouse IgG) diluted 1:500 (4 μg/mL) in a CAN GET SIGNAL® immunoreaction enhancer solution.
Bone tunnel evaluation by micro-CT
The femur–ACL graft–tibia complex (n=6 at each group at each time point), with a femur length of 45 mm and a tibia length of 60 mm, was harvested from each knee immediately after sacrifice and frozen at −30°C until testing. Before testing, the specimen was thawed overnight at room temperature. The areas of the vertical plane of the axis of the bone tunnel at 5-mm depth from the tibial joint surface were measured using microcomputed tomography (micro-CT, 250-μm slice thickness; ALOKA LaTheta Laboratory CT). The areas were estimated with image analysis software (ImageJ; National Institutes of Health). The areas were measured an average of three times.
Biomechanical study
After measuring the area of the bone tunnel, the biomechanical study was performed (n=6 for each group at each time point). All soft tissue, except for the ACL graft, was removed by sharp dissection. The knee was potted at 45° of flexion with the bone tunnel oriented parallel to the testing axis (Fig. 2). All mechanical testing was conducted using a tensile sensor (AG-I SHIMAZU Co.). Before the tensile test was conducted, preloading of 1N for 1 min and cyclic preconditioning of the constructs between elongation limits of 0 and 0.75 mm were applied. Immediately after preconditioning, the ultimate load to failure (N) was recorded in uniaxial tension at 10 mm per minute. The stiffness (N/mm) was calculated from the slope of the linear region of the load-deformation curve.
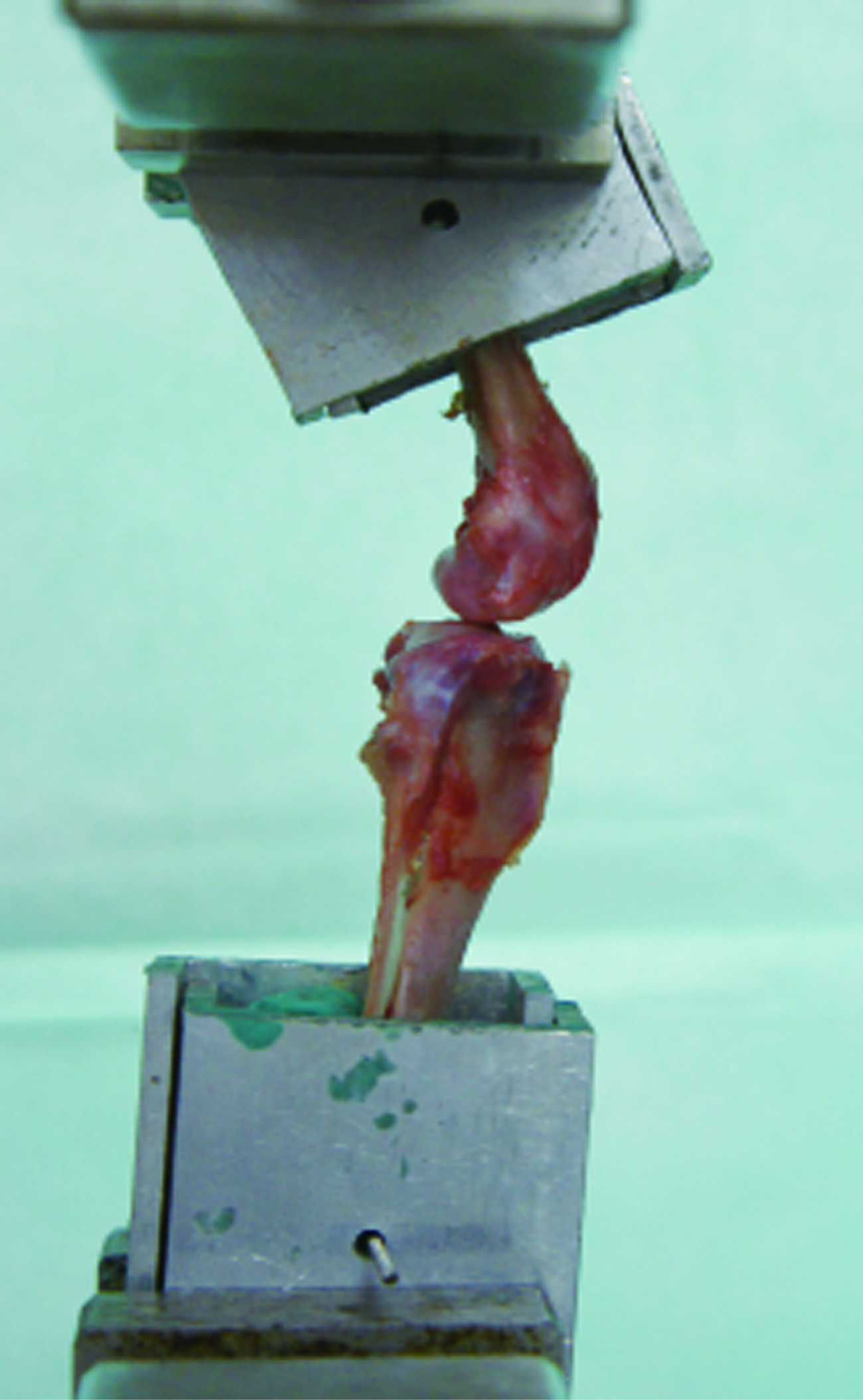
The specimen was fixed and oriented for tensile testing, so the pullout loads were applied with the knee at 45° of flexion. Color images available online at www.liebertpub.com/tea
Real-time polymerase chain reaction analysis
Immediately after sacrifice at week 2, bone–tendon interface samples (the bone tunnel and its surrounding tissue) were extracted as cylindrically shaped pieces 3.5 mm in diameter using the Mosaicplasty kit (ACUFEX; MosaicPlasty Precision, Smith & Nephew) and frozen in liquid nitrogen (n=6 for each group). The tissues were homogenized in TRIzol reagent (Invitrogen) with a T-18 ULTRA-TURRAX homogenizer (IKA Werke) immediately after the harvest. Total cellular RNA was extracted from the harvested tissue using the acid guanidinium thiocyanate–phenol–chloroform method. After the RNA extraction, RNA was cleaned up using the RNeasy Mini Kit (Qiagen). mRNA transcription (in duplicate) was quantified using the Applied Biosystems StepOne™ Real-time polymerase chain reaction (RT-PCR) System (Applied Biosystems). RT-PCR reactions (20 μL) contained 0.1 μM forward primer, 0.1 μM reverse primer, and 1 μL of cDNA template from RT reaction, and 12.5 μL 10× Master Mix for Power SYBR green master mix (Applied Biosystems). Reaction conditions were as follows: 10 min at 95°C, followed by 40 cycles at 95°C (15 s), and 60°C for 1 min. The level of each target gene was normalized to the levels glyceraldehyde-3-phosphate dehydrogenase (GAPDH, a housekeeping gene) and expressed relative to the levels of the control group at each timepoint (DDCT methods; Applied Biosystems). All primers used in this study were mRNA specific (on different exons and crossing over to introns) and designed for RT-PCR analysis of gene expression using Primer 3 and Primer designing tool (NCBI). Primers for GAPDH were designed to the forward sequence 5′-CCACCTTGTGAAGCTCATTTCCT- 3′ and the reverse sequence 5′-TCGTCCTCCTCTGGTGCTCT- 3′. Primers for vascular endothelial growth factor (VEGF) were designed to the forward sequence 5′-CCTTGCCTTGCTGCTCTACC-3′ and the reverse sequence 5′-AGGTTTGATCCGCATGATCTG-3′. All primers were obtained from Invitrogen.
Inhibition of neovascularization
To investigate the hypothesis that neovascularization is essential for tendon–bone healing, we used an anti-VEGF monoclonal antibody, bevacizumab (Avastin; Genentech, Inc.). Three rabbits subjected to ACL reconstruction with simvastatin were intravenously administered 100 mg bevacizumab at postoperative day 3. 31 At postoperative 2 weeks, biomechanical assessment and bone tunnel evaluation by micro-CT were performed.
Statistical analysis
All values were expressed as mean±SEM. The biomechanical property, capillary density, osteoblast density, and expression of VEGF between control groups and simvastatin-treated groups were compared using Student's t-tests. The inhibition of neovascularization was statistically analyzed using analysis of variance, followed by post-hoc testing with a Tukey procedure. A probability value<0.05 was considered significant.
Results
Histological assessment
Specimens at 2 weeks
There was a less-organized fibrous tissue and a very little new bone formation containing chondroid cells between the edge of the trabecular bone and the tendon in the control group at week 2 (Fig. 3A and 3B). In the simvastatin-treated groups, there was aligned connective tissue, newly formed woven bone, and cartilage in the tendon–bone interface.

Histological evaluation of the tendon–bone interface of a specimen from each group at 2, 4, and 8 weeks after surgery (
Specimens at 4 weeks
The fibrous connective tissue was aligned, and the woven bone covered the edge of the trabeculae between tendon and bone in both groups. There was more aligned chondroid-like cell and matured interface in the simvastatin-treated group than in the control group. The collagen fiber anchored toward the woven bone and integrated along the tendon was more advanced in the simvastatin treatment group.
Specimens at 8 weeks
The fibrous connective tissue at the tendon–bone interface was narrow and unclear in both groups. A more aligned and layered cartilage zone was observed that incorporated the adjacent bone and tendon in the simvastatin treatment group.
Assessment of osteogenesis and angiogenesis
Endothelial cells staining with isolectin B4 in tissue samples collected 2 weeks after surgery revealed enhanced angiogenesis in the area of tendon–bone integration in the simvastatin-treated group. Neovascularization assessed by the capillary density was significantly increased in the simvastatin-treated group than in the control group (statin, 112.0±6.9 vs. control, 72.0±5.8/mm2; p<0.01, n=5) (Fig. 4). Osteoblast stained with anti-mouse osteocalcin in tissue samples collected 2 weeks after surgery also revealed augmentation of osteogenesis in the area of new bone formation in the simvastatin-treated group. Osteogenesis assessed by osteoblast density was significantly enhanced in the simvastatin-treated group compared with the control group (simvastatin, 495.3±32.9 vs. control, 272.0±28.3/mm2; p<0.001, n=5) (Fig. 5).

Histological analysis of the tendon–bone interface. Representative fluorescent vascular staining for isolectin B4 (IB4) in 2-week specimens in the control and simvastatin groups (magnification,×200). Capillaries are indicated in green, and the average number of capillaries was significantly higher in the simvastatin group than in the control group. Color images available online at www.liebertpub.com/tea
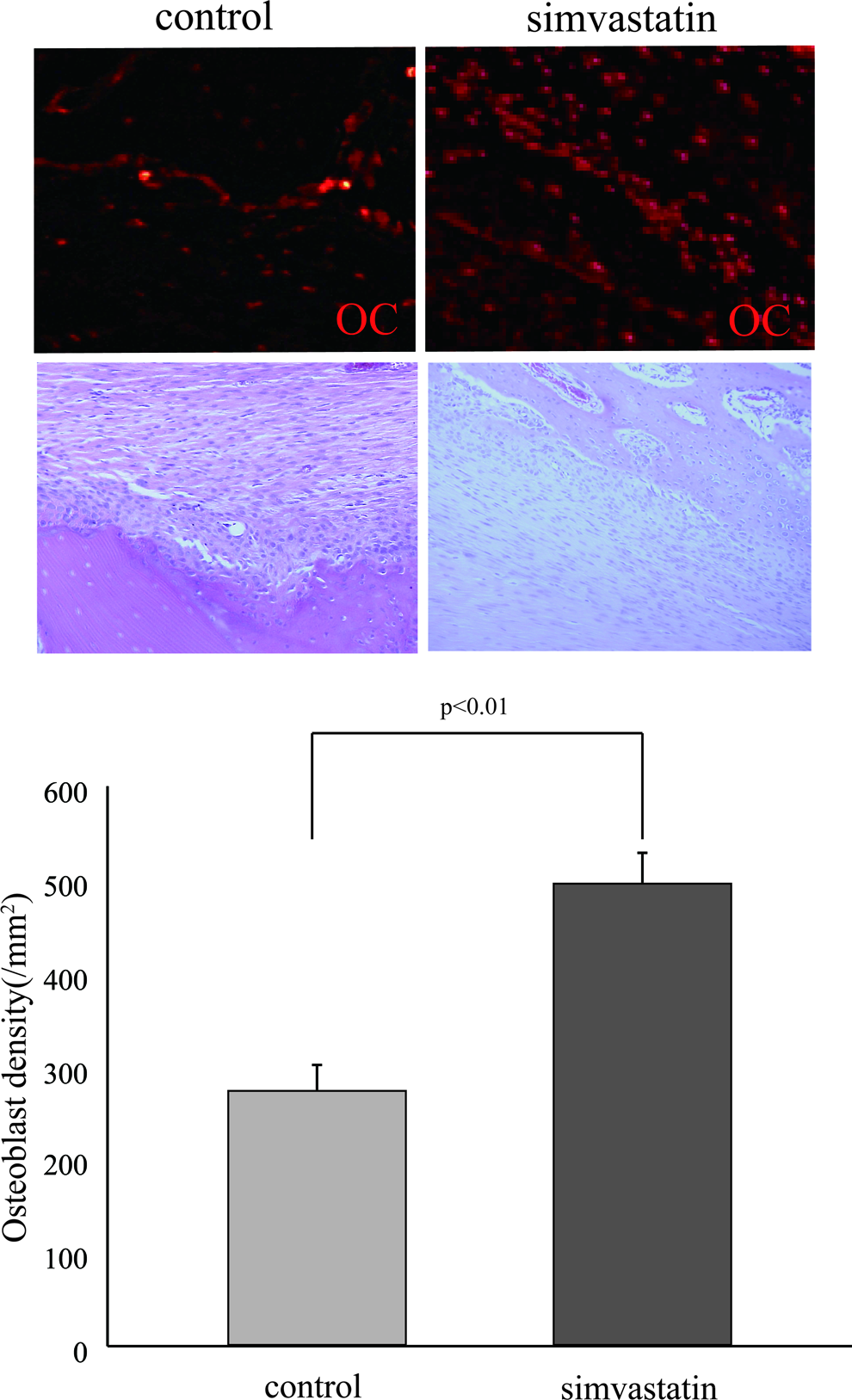
Histological analysis of the tendon–bone interface. Representative fluorescent vascular staining for osteocalcin (OC) in the 2-week specimens in the control and simvastatin group (magnification,×200). Osteoblasts are indicated in red, and the average number of osteoblasts was significantly higher in the simvastatin group than in the control group. Color images available online at www.liebertpub.com/tea
Bone tunnel evaluation
The averages of the bone tunnel area in the simvastatin-treated group were significantly smaller than in the control group at weeks 2 and 4 (week 2: simvastatin, 3.25±0.33 vs. control, 4.13±0.28/mm2; p<0.05, n=6; week 4: simvastatin, 1.61±0.14 vs. control, 2.71±0.31/mm2; p<0.01, n=6) (Fig. 6A and 6B). At week 8, the averages of the bone tunnel area showed no significant differences between the two groups (simvastatin, 0.94±0.03 vs. control, 1.61±0.14/mm2; p=0.06, n=6).
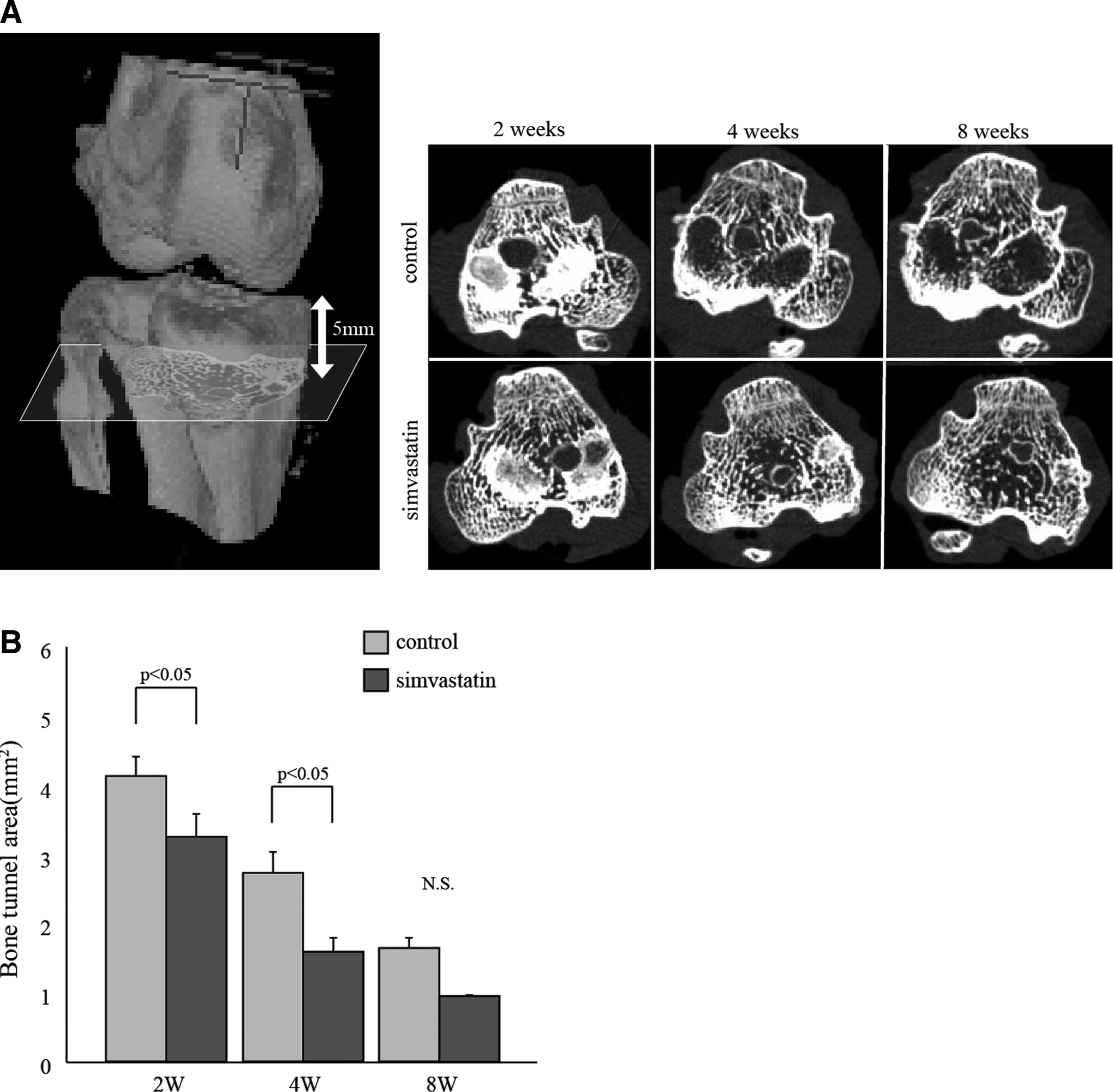
Micro-CT scans at each group and time point.
Biomechanical testing
The average load to failure in the simvastatin-treated group was significantly greater than in the control group at week 2 (simvastatin, 32.5±2.3 vs. control, 21.6±3.8 N; p<0.05, n=6). At weeks 4 and 8, there were no significant differences in the average load to failure between the two groups (week 4: simvastatin, 35.5±1.6 vs. control, 33.4±3.5 N; p=0.68, n=6; week 8: simvastatin, 38.4±6.8 vs. control, 36.7±2.3 N; p=0.73, n=6) (Fig. 7A). There were no significant differences in stiffness between the two groups at each time point (week 2: simvastatin, 12.8±1.6 vs. control, 8.9±2.1 N/m; p=0.22, n=6; week 4: simvastatin, 13.6±1.2 vs. control, 11.1±2.9 N/m; p=0.43, n=6; week 8: simvastatin, 16.3±3.8 vs. control, 15.3±1.5 N/m; p=0.76, n=6) (Fig. 7B).
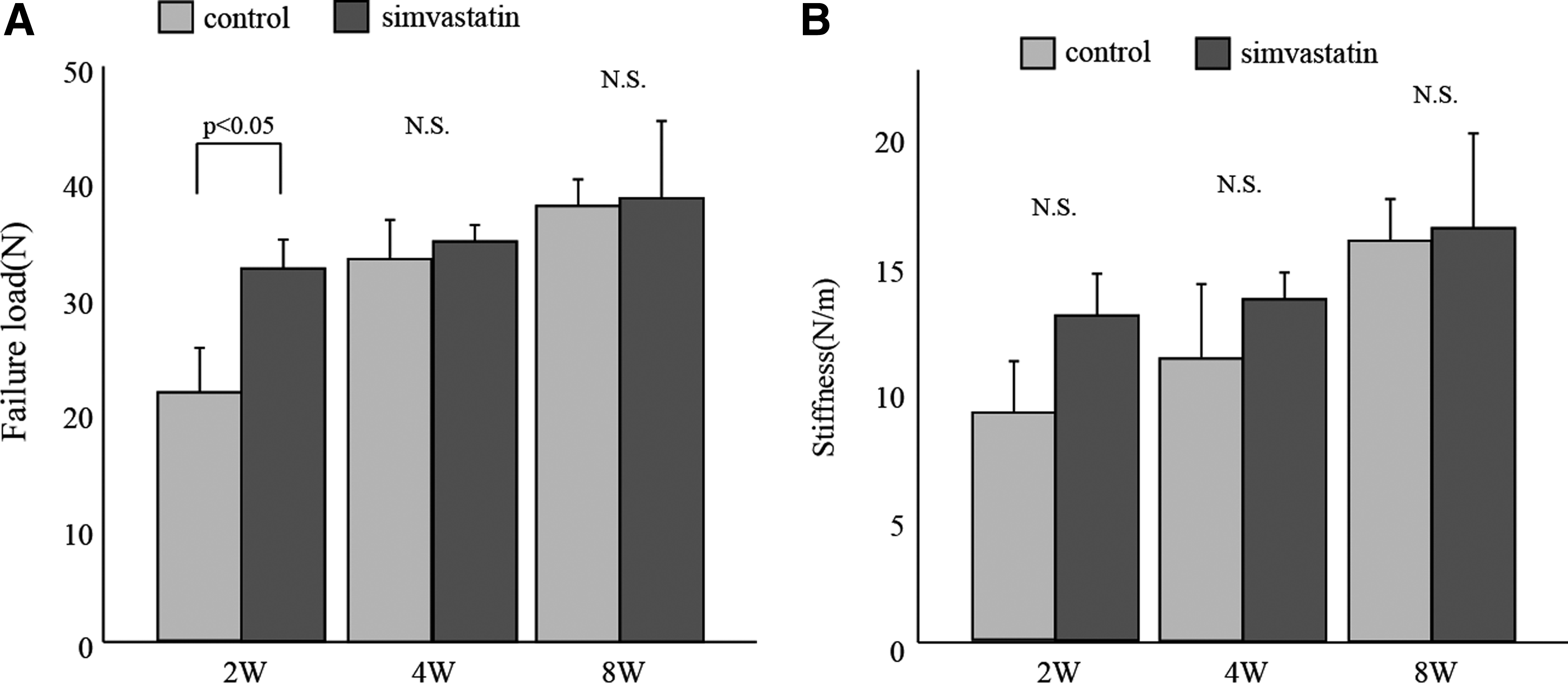
The femur–ACL graft–tibia complex (n=5 at each group at each time point) was used for biomechanical testing using a tensile sensor.
As the assessment of failure mode, five grafts in the control group and two grafts in the simvastatin-treated group failed by totally pullout from the bone tunnel, and one graft in the control group and four grafts in the simvastatin-treated group were torn-off inside the bone tunnel at week 2. Two were torn-off inside the bone tunnel, and the others failed at midsubstance in both groups at weeks 4 and 8.
RT-PCR analysis
At week 2, the simvastatin-treated group showed significantly higher VEGF gene expression than the control group (control group 1.000±0.192; simvastatin group 1.738±0.216; p<0.05) (Fig. 8).
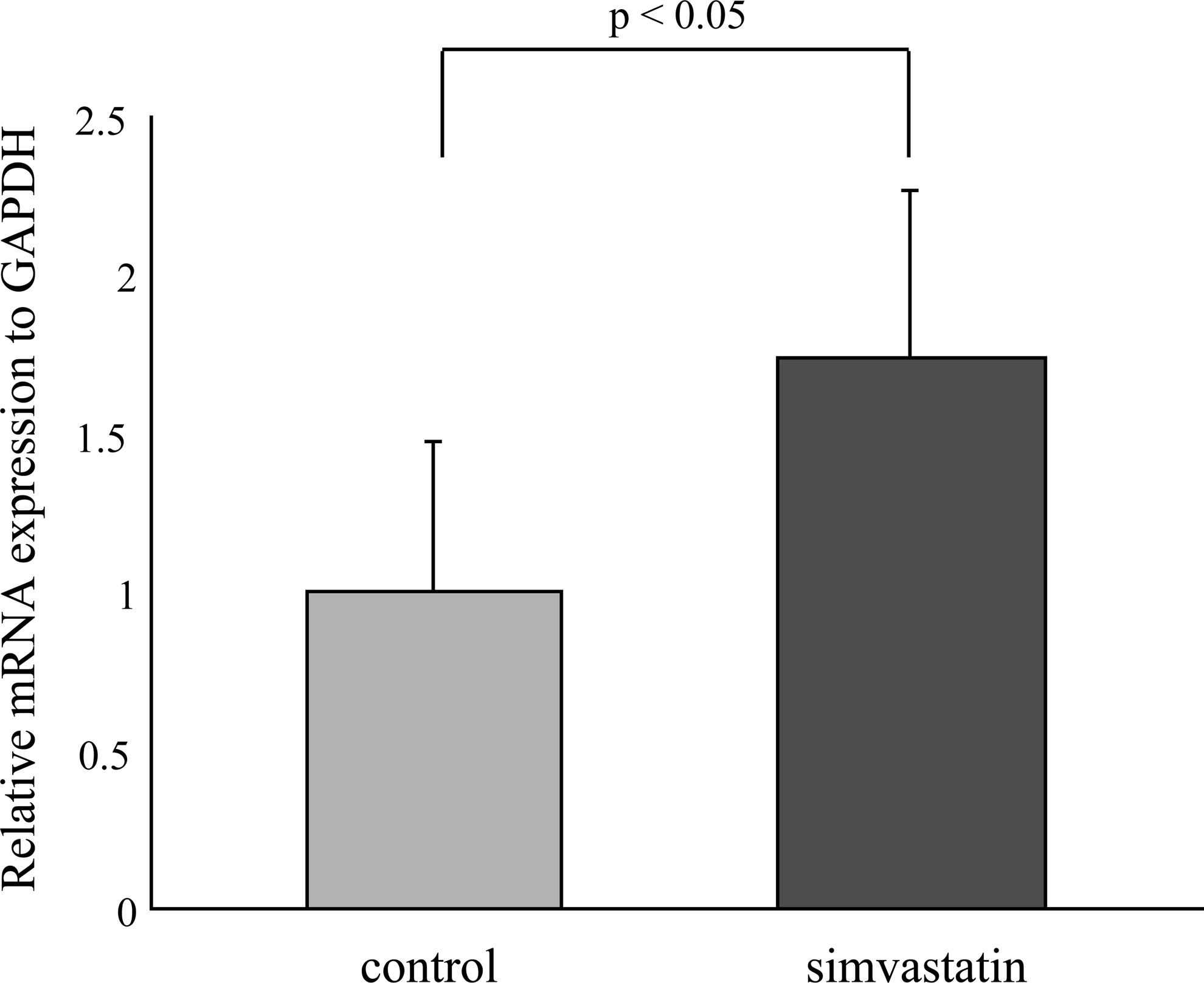
Real-time polymerase chain reaction product. Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) rations for vascular endothelial growth factor (VEGF). The mRNA expression in the tibial bone tunnel was compared between the control and the simvastatin-treated groups. Specimens in the simvastatin-treated group had significantly increased VEGF/GAPDH at week 2 (n=6).
Inhibition of neovasularization
The average bone tunnel area was significantly larger in the bevacizumab-injected group than in the control and simvastatin-treated groups at week 2 (simvastatin, 3.25±0.33 vs. control, 4.13±0.28 vs. bevacizumab, 5.15±0.25/mm2, respectively p<0.01, n=6) (Fig. 9).The average load to failure and stiffness in the bevacizumab-injected group were significantly lower than in the simvastatin-treated group (failure load; simvastatin, 32.5±2.3 vs. control, 21.6±3.8 vs. bevacizumab, 21.5±2.9 N, respectively, p<0.05, n=6; stiffness; simvastatin, 12.8±1.6 vs. control, 8.9±2.1 vs. bevacizumab, 6.3±0.8 N/m; respectively, p<0.05, n=6).
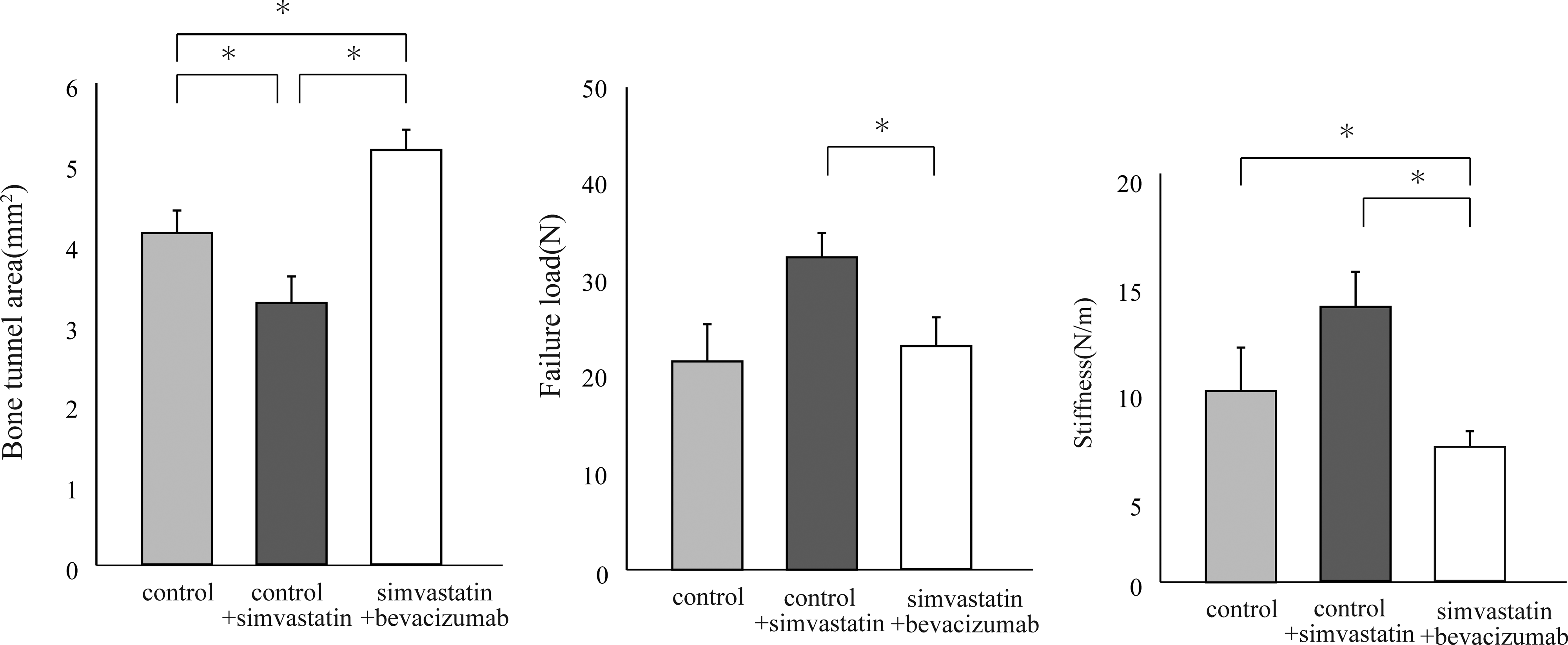
The average bone tunnel area was significantly larger in the bevacizumab-injected group than in the control and simvastatin-treated groups at week 2 (n=6). The average load to failure and stiffness in the bevacizumab-injected group were significantly lower than in the simvastatin-treated group. *p<0.05.
Discussion
In the present study, we elucidated the effectiveness of low-dose simvastatin-incorporated gelatin hydrogel for early tendon–bone healing in ACL reconstruction using a rabbit model. Histological, radiological, and biomechanical assessment at the site of the tendon–bone interface provided early and strong healing. This is the first reported study demonstrating a therapeutic strategy using simvastatin for ACL reconstruction surgery.
Reconstructed tendon grafts in the bone tunnels are separated from their vascular supply; therefore, the ingrowth of new blood vessels is an essential step in the process of tendon graft remodeling. In addition, neovascularization is essential for bone regeneration around the tendon graft and tissue regeneration at the tendon–bone junction.14,32–34 Wang et al. applied an extracorporeal shockwave after ACL reconstruction in a dog model and demonstrated that angiogenesis was essential for tendon–bone healing by detecting strong VEGF expression in the tendon–bone junction. 34 In the meantime, the positive effects of simvastatin on VEGF release during wound healing using diabetic mice were also reported. 23 In addition, Kanazawa et al. reported that VEGF is highly expressed at postoperative week 2 in an in vivo ACL reconstruction animal model. 35 These studies supported our findings that neovascularization and increased VEGF expression at the tendon–bone interface promoted by simvastatin were demonstrated in the 2-week specimens. Endothelial progenitor cells (EPCs) were recognized to respond to tissue ischemia and injury as well as cytokines by mobilizing the bone marrow into the peripheral blood, migrating to regions of neovascularization to differentiate into mature endothelial cells, and further promote vasculogenesis. 36 Among the various cytokines and drugs, statins were also reported to promote the proliferation, migration, and survival of endothelial cells and bone marrow-derived EPCs, and therefore enhance angiogenesis.37,38 Recently, Fukui et al. reported that statins induced angiogenesis by increasing EPCs, and this effect on bone formation contributes to the improvement of fracture healing using a psuedoarthrosis model. 29 Similarly, in our study, angiogenesis and osteogenesis were enhanced by low-dose simvastatin administration in the ACL reconstruction model.
Previous studies have shown that osteoinductive agents accelerated osteointegration to the tendon graft, and osteointegration improved the mechanical properties at the tendon–bone interface.10,11,39 Rodeo et al. reported a narrower interface zone in BMP-treated specimens, indicating better graft incorporation. 10 The current study showed that histologically simvastatin promoted bone ingrowth into the tendon–bone interface at week 2 and determined the quantity of the bone tunnel area. Osteocalcin is a well-known marker of terminal osteoblast differentiation influencing bone mineralization, and the finding of high osteoblast density in the simvastatin-treated group also indicated the effectiveness of simvastatin on osteogenesis. The ultimate failure load in the simvastatin-treated group was larger than the control group at 2 weeks, but there were no difference between the two groups at 4 and 8 weeks. This was because a consistent regeneration of the direct insertion with a fibrocartilage layer at the tendon–bone interface was not obvious at an earlier phase. Tendon–bone healing is classified into two types: one shows layered chondral formation at tendon–bone interface that resembles normal ligament–bone insertion, and this type mainly plays a role to mechanical strength; and the other type shows fibrous insertion where tendon and bone directly come in contact with each other. 8 Both types need osteogenesis at the tendon–bone interface. Fibrous insertion appears at early phase, and layered chondral formation takes a long time to mature and accomplish higher mechanical strength. The chondral tendon–bone healing was more seen in the simvastatin-treated group at weeks 4 and 8, but incompletely matured chondral healing could not strengthen biomechanical properties. Meanwhile, fibrous healing where tendon and bone come in contact with each other was seen in histological findings and bone tunnel evaluation in the simvastatin-treated group at week 2. That is why the failure load in the simvastatin-treated group was significantly greater than in the control group at week 2. The ACL reconstruction model in the study was used on the assumption that hamstring tendon grafts were fixed with a suspensory fixation devise. It is well known that the suspensory fixation devise causes bone tunnel widening after ACL reconstruction, because the fixation point is farther away from the aperture than the interference screw, and micromovement occurs at the tendon–bone interface.40,41 In this study, mechanical property could not be reinforced by simvastatin in long term, but simvastatin promoted tendon–bone healing at early stage, and prompt bone infiltration into the tendon–bone gap could predict to prevent bone tunnel enlargement and tension loss of the graft in the bone tunnel. These could be a ground to encourage quicker rehabilitation after ACL reconstruction.
In this study, we also demonstrated the important role of angiogenesis on tendon–bone healing, as intravenously injected antiangiogenetic agent prevented bone formation and weakened biomechanical properties. The mean bone tunnel area in the bevacizumab-injected group was less than that in the simvastatin-treated and control groups. Although the biomechanical property in the bevacizumab-injected group was significantly decreased compared to the simvastatin-treated group, there was no difference between the control and bevacizumab-injected groups. This was explained by the fact that there was insufficient bone formation and less contact at the tendon–bone interface in the 2-week specimens in the control and the bevacizumab-injected groups. Bevacizumab totally inhibited the beneficial effects of simvastatin on tendon–bone healing. The results demonstrated that the positive effect of simvastatin on tendon–bone healing was associated with increased angiogenesis and osteogenesis, whereas an inhibition of VEGF did decrease not only angiogenesis but also osteogenesis in promoted healing at the tendon–bone junction. These findings suggest that angiogenesis plays a more important role in tendon–bone healing than osteogenesis.
There are some limitations in this study. Only a single dose of simvastatin was applied in a small number of animals. In a future study, a dose–escalation study should be investigated in a large number of animals to find whether the treatment is effective in a dose-dependent manner or not. The results might be some specific effects, so that repeating the experiment in a larger animal would be worthwhile to put a practical clinical use. Both hind limbs simultaneously received ACL reconstruction. To simulate the healing process in the clinical setting, a one-sided operation should be performed.
In conclusion, the local administration of low-dose simvastatin-conjugated gelatin hydrogel promotes tendon–bone healing at an early stage via angiogenesis and osteogenesis, but does not affect the biomechanical property in long term. This convenient and economical method may enable a new strategy for the promotion of recovery after ACL reconstruction.
Footnotes
Acknowledgment
The authors thank Ms. Minako Nagata and Ms. Kyoko Tanaka from the Kobe University for excellent technical assistance.
Disclosure Statement
No competing financial interests exist.