
Abstract
Myocardial restoration using tissue-engineered grafts to regenerate the ischemic myocardium offers improved donor cell retention, yet a limited cell survival resulting from poor vascularization needs to be addressed. A cell type derived from the subamnion, namely, cord-lining mesenchymal stem cells (CL-MSC), has recently been identified. Here we present a restorative strategy that combines a fibrin graft containing human CL-MSC and omental flap providing, thereby, cell-, structural-, and angiogenic support to the injured myocardium. The graft consisted of a mixture of 2×106 CL-MSC-GFP-Fluc and fibrin. Myocardial infarction (MI) was induced in nude rats and following confirmation of ensued heart failure with echocardiography 2 weeks after injury, therapeutic intervention was performed as follows: untreated (MI, n=7), CL-MSC graft (CL-MSCG, n=8), CL-MSCG and omental flap (CL-MSCG+OM, n=11), and omental flap (OM, n=8). In vivo bioluminescence imaging at 1, 3, 7, and 14 days post-treatment indicated comparable early donor cell viability between the CL-MSCG and CL-MSCG+OM. Treatment with CL-MSCG+OM improved the myocardial function as assessed by the measurement of end-diastolic left ventricular (LV) pressure (3.53±0.34 vs. 5.21±0.54 mmHg, p<0.05), contractility (+dP/dt, 3383.8±250.78 mmHg vs. 2464.9±191.8 mmHg, p<0.05), and the relaxation rate (−dP/dt, −2707.2±250.7 mmHg vs. 1948.7±207.8 mmHg, p<0.05), compared to MI control 6 weeks after ischemic injury. Furthermore, evidence of a 20.32% increase in the ejection fraction was observed in CL-MSCG+OM rats from week 2 to 6 after injury. Both CL-MSCG and CL-MSCG+OM led to an enhanced cardiac output (p<0.05), and attenuated the infarct size (35.7%±4.2% and 34.7%±4.8%), as compared to MI (60.7%±3.1%; p<0.01 and p<0.001, respectively). All treated groups had a higher arteriole density than controls. Yet, a higher amount of functional blood vessels, and a 20-fold increase in arteriole numbers were found in CL-MSCG+OM. Altogether, CL-MSCGs supplemented with vascular supply have the potential to repair the failing, chronically ischemic heart by improving myocardial revascularization, attenuating remodeling, and ameliorating cardiac dysfunction.
Introduction
While cardiac tissue-engineered approaches to repair the ischemic myocardium offer improved donor cell retention compared to intramyocardial cell injections, a drawback faced by cardiac patches aiming at postischemic myocardial repair is limited donor cell survival resulting from poor vascularization within thick constructs. Omental wrapping or omentopexy, a classical technique introduced in the mid-1930s to treat myocardial ischemia by promoting revascularization from a pedicle with omental vessels to coronary arteries, 12 has recently been reintroduced in the cardiac tissue engineering setting to promote neovascularization in myocardial grafts. Omentopexy has been used to cover various types of cardiac patches in situ, including scaffolds seeded with MSC in a rat model, 13 and a fibroblast growth factor (FGF)-hydrogel sheet covering the area of myocardial ischemia in rabbits. 14 Likewise, a porous alginate scaffold seeded with neonatal rat cardiomyocytes and a cocktail of prosurvival and angiogenic factors has been prevascularized in the omentum for 7 days before implantation onto the infarcted heart of allogeneic rats. 15 Strategies using an omental flap encompassing a three-layer MSC sheet in rats, 16 and skeletal myoblast sheets in pigs 17 have also been recently described. In general, omentopexy combined with cardiac patches or cell sheets resulted in improvement of heart function and increased scar thickness thereby attenuating LV dilation, while enhancing donor cell viability and vascular density.13,15–17 In this study, we tested the hypotheses that a fibrin graft containing cord-lining mesenchymal stem cells (CL-MSCG) constitutes a suitable restorative device, and that the combination of CL-MSCG with a vascularized omental flap has a superior ability to regenerate the chronically infarcted myocardium. To our knowledge, this is the first study to utilize CL-MSC for myocardial repair.
Materials and Methods
Cell culture
Human umbilical CL-MSC isolated from the subamnion of the umbilical cord were provided by CellResearch Corporation Pte Ltd., 4 and maintained in proprietary serum-free media (PTT-4) containing the DMEM-F12-CMRL1066 (GIBCO®, Life Technologies Corporation) with supplement of albumin, insulin, the basic FGF (bFGF), transforming growth factor beta 1, and leukemia inhibitory factor (All supplements were purchased from R&D System, Inc.). CL-MSC were subcultured upon reaching confluency of 80%–85% by mechanically lifting the cells from the surface of the tissue culture flask using a cell lifter (Costar®, Corning®). Human cardiac myocytes-adult (ScienCell Research Laboratories) were cultured in the cardiac myocyte medium. Human dermal fibroblast-adult (Gibco®, Life Technologies Corporation) were maintained in the medium 106 with low serum.
Construction of CL-MSCG
The sterile fibrin matrix (Tisseel; Baxter Healthcare Corporation) was prepared following the vendor's instructions and used as a scaffold material to construct the CL-MSCG. For in vitro studies, either 0.5×106, 1×106, or 2×106 CL-MSC transduced with the green fluorescent protein and firefly luciferase (CL-MSC-GFP-Fluc) (see Supplementary Materials and Methods; Supplementary Data are available online at www.liebertpub.com/tea) in serum-free media were mixed with the fibrin matrix (1:4) to a final volume of 250 μL, and plated into eight-well chamber slides (Lab-Tek™II Chamber Slide™; NUNC A/S) to produce 10×8×2.5-mm grafts. For in vivo studies, a mixture of 2×106 CL-MSC-GFP-Fluc in DPBS and the fibrin matrix with the same dilution and final volume was plated. Subsequently, the mixture was allowed to polymerize for 30 min at room temperature. Grafts were then covered with 0.4 mL serum-free media and placed in an incubator under CO2 at 37°C. The medium was exchanged daily.
Rat model of MI and restorative therapy
All experiments were approved by the Institutional Animal Care and Use Committee (IACUC) of the National University of Singapore and carried out in accordance with established guiding principles for animal research. Male NIH Nude Rats (250–300 g; Taconic) were used for our experiments. Left-thoracotomy and pericardectomy followed by left anterior descending coronary artery (LAD) ligation were performed as previously described. 18 An acute evidence of MI was assessed by direct observation of myocardial blanching and ECG changes. Postoperative care was done as previously described. 18 Animals were randomly assigned a therapeutic procedure 2 weeks after MI and upon confirmation of the fractional area change (FAC) ≤40% by echocardiography. In animals receiving a CL-MSCG and omental flap (CL-MSCG+OM, n=11) and those only having an omental flap (OM, n=8), an upper mid-laparatomy was performed concurrently to a left-thoracotomy, and the greater omentum was mobilized from the abdomen to the thoracic cavity via a small cut in the diaphragm. 19 Next, the omental flap (conserving a vascular pedicle) was wrapped onto the LV scar area with or without a patch, respectively. The patch and the greater omentum were attached to the recipient heart using fibrin glue (Tisseel). In animals that only received a CL-MSCG (n=8), the patch was implanted epicardially without omentum wrapping. MI animals (injury control, n=7) did not receive any treatment after 2 weeks of LAD ligation.
Echocardiography
Transthoracic echocardiograms were performed in all animals at baseline (before surgery), and 2 and 6 weeks following MI (i.e., 4 weeks after treatment) by a blinded investigator (L.H.L.), using a Vivid 7 Dimension ultrasound system (GE VingMed) equipped with a broadband 10S transducer operating at up to 11 MHz. 18 Diastolic and systolic LV wall thickness and internal dimensions were obtained from M-mode recordings of the LV in the parasternal short-axis view. LV volumes were calculated using a modified Teichholz formula described elsewhere. 20 The LV ejection fraction (EF%) was calculated as [(LV end-diastolic volume−LV end-systolic volume)/LV end-diastolic volume]×100. The FAC was measured from 2D images of the LV in short-axis and calculated as FAC%=[(end-diastolic area−end-systolic area)/end-diastolic area]×100. Offline measurements of LV dimensions and areas were made from three consecutive cardiac cycles using EchoPac software (version BT06; GE VingMed).
In vivo bioluminescence imaging
To investigate in vivo donor cell viability of the implanted cells within 3D grafts, we performed bioluminescence imaging (BLI) using a Xenogen-IVIS® Lumina imaging system (Caliper Life Sciences, PerkinElmer) as previously described.18,21 All rats from the CL-MSCG and CL-MSCG+OM group were imaged on days 1, 3, 7, and 14 days postepicardial patch implantation. Regions of interest corresponding to the location of the peak photon emission were generated using Living Imaging Software version 3.2.
Additional materials and methods can be found in Supplementary Materials and Methods.
Statistical analysis
Data are presented as mean±standard error of mean. To test for statistically significant differences, between-group comparisons of echocardiographic indexes were performed using a 2-way ANOVA with repeated measurers followed by pairwise comparisons by the Bonferroni's post-test. The ANOVA model included control versus treatment and baseline versus 2 and 6 weeks after MI as factors, as well as the interaction between the two factors. For other comparisons, one-way ANOVA followed by the Bonferroni's post hoc test and the unpaired Student's t-test were used when appropriate. Differences were considered significant when p<0.05. All statistical analyses were performed using GraphPad Prism® software version 5.04 for Windows (GraphPad Software).
Results
Phenotypic and functional characteristics of CL-MSC
Multilineage differentiation potential of CL-MSC was confirmed, as cells were easily differentiable toward chondrogenic, adipogenic, and osteogenic lineages (Supplementary Fig. S1A). Lentiviral transduction efficiency studies revealed that 75% of CL-MSC were green fluorescent protein (GFP)-positive. In agreement with the minimal criteria for defining multipotent MSC established by the International Society for Cellular Therapy, 22 expression of MSC markers >95% (CD73, CD90, and CD105) by CL-MSC-GFP-Fluc was evidenced through flow cytometry (Supplementary Fig. S1B). Also, we confirmed that CL-MSC-GFP-Fluc were negative (<2%) for hematopoietic stem cell (CD34, CD45, and CD117) and endothelial cell (CD31) markers (Supplementary Fig. S1B). CL-MSC-GFP-Fluc were also positive for the stem cell markers Oct3/4 (96.36%±2.36%; Supplementary Fig. S1C, S1G) and Nanog (80.95%±2.53%; Supplementary Fig. S1D, S1G). Interestingly, CL-MSC-GFP-Fluc also expressed the early cardiac stem cell markers NKX2.5 (87.92%±1.71%) and GATA4 (71.52%±2.52%) as evidenced by immunohistochemistry (Supplementary Fig. S1E–G) and Western blotting (Supplementary Fig. S1H, I).
In vitro donor cell viability within CL-MSCG
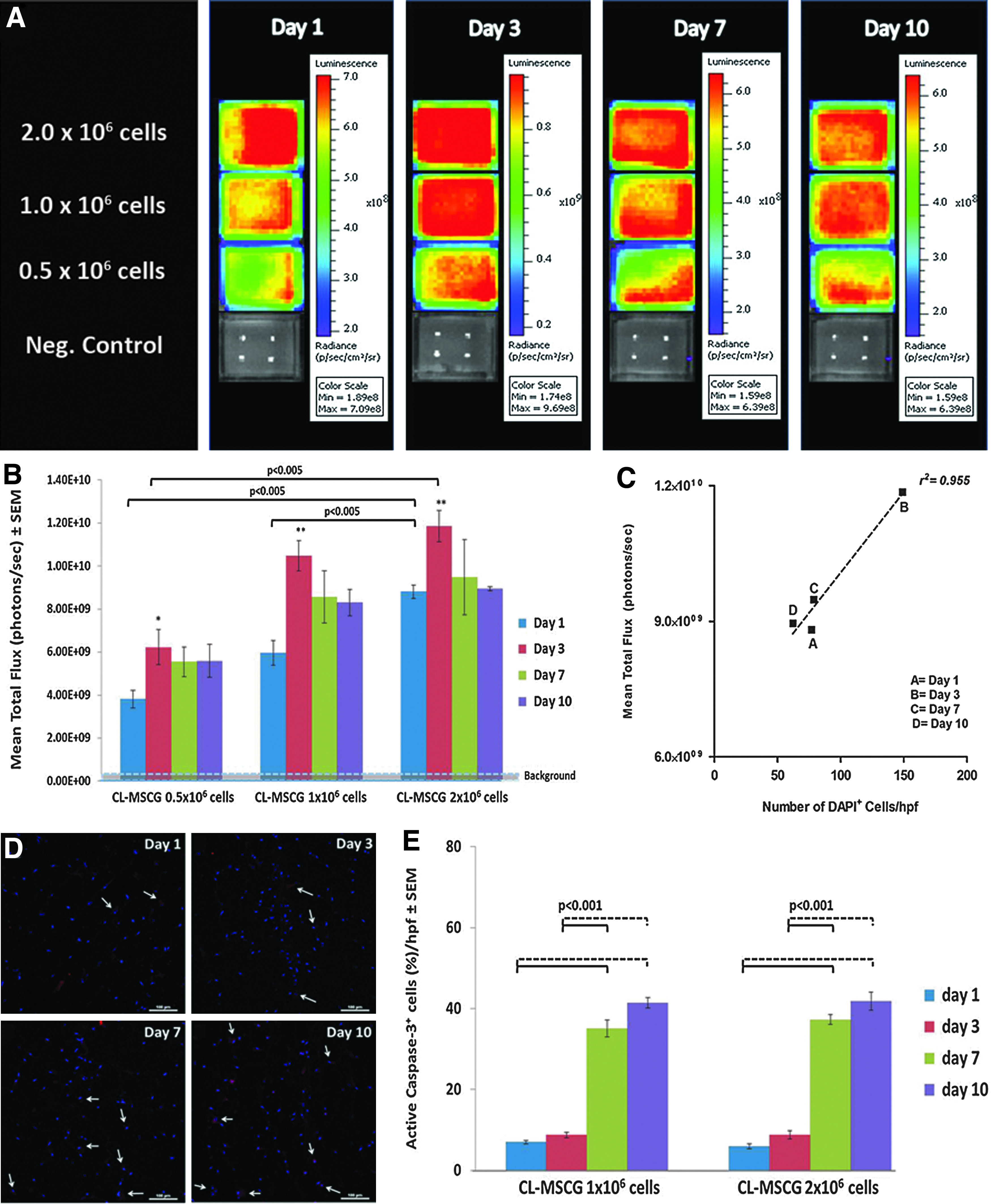
In vitro BLI revealed a significant increase in cell bioluminescent baseline signals from day 1 to 3 in the CL-MSCG containing 0.5×106 cells (p<0.05), 1×106 cells (p<0.01), and 2×106 cells (p<0.01) followed by a gradual decrease to baseline by day 10 in culture (Fig. 1A, B). The CL-MSCG with 2×106 cells showed significantly larger bioluminescent signals after 1 day in culture (p<0.005 vs. 1×106 cells/graft and p<0.005 vs. 0.5×106 cells/graft) and after 3 days in culture (p<0.005 vs. 0.5×106 cells) (Fig. 1A, B). There was a good correlation between mean bioluminescence (mean total photon flux) and the histological mean cell number (DAPI+ cells) in grafts containing 2×106 cells across the different time points in vitro (r2=0.955) (Fig. 1C); hence, we chose to construct grafts for in vivo studies with this cell number.
In vitro donor cell viability within CL-MSCG.
Active caspase-3 staining was used to assess donor cell apoptosis in the CL-MSCG. The percentage of apoptotic (active caspase-3+) cells in the CL-MSCG containing 1×106 and 2×106 cells was comparable between day 1 (6.99%±0.41% and 5.92%±0.58%, respectively), and day 3 in static culture (8.73%±0.67% and 8.81%±0.98%, respectively). Still, there was a sharp increase in the number of apoptotic cells at day 7 (35.07%±2.14% and 37.28%±1.20%, respectively), and day 10 in culture (41.41%±1.26% and 41.84%±2.25%, respectively), when compared to day 1 and 3 (p<0.001) (Fig. 1D, E). Since fewer apoptotic cells were found during the first 3 days in culture, we used grafts that had been only 1 day in culture for the in vivo studies.
Postischemic therapy with CL-MSCG and omental flap in a rat model
A CL-MSCG (Fig. 2A) combined with omental flap wrapping was implanted onto infarcted heart tissue (CL-MSCG+OM, n=11) (Fig. 2B), as we envisioned that the omentum's vasculature would provide an immediate source of blood vessels to the graft enhancing thereby donor cell survival and cardiac function. To endorse any beneficial effect of omental wrapping on the ability of the CL-MSCG to improve heart function, we implanted grafts containing CL-MSC without omentum (CL-MSCG, n=8). Likewise, we used omental wrapping alone without the epicardial patch (OM, n=8) to confirm that vascularization alone is insufficient for myocardial repair and the paracrine factors derived from CL-MSC are necessary. Untreated infarcted animals were used as injury controls (MI, n=7). Only rats displaying a FAC ≤40%, as assessed by echocardiography 2 weeks after MI, were included in this study.

In vivo donor cell viability in grafted CL-MSCG
Prospective evaluation of donor cell survival in vivo indicated a progressive decrease in cell signals from day 1 to 14 after graft implantation. Photon emission was significantly decreased in both CL-MSCG and CL-MSG+OM groups from day 1 (7.55×107±1.34×107 and 6.46×107±1.0×107 photons/s, respectively), day 3 (4.04×107±6.84×106 and 3.05×107±6.51×106 photons/s, respectively; p<0.01), day 7 (1.28×107±3.78×106 and 4.45×106±1.62×106 photons/s, respectively; p<0.0001), and day 14 (6.84×105±3.33×105 and 1.48×105±3.13×104 photons/s, respectively; p<0.0001). Early in vivo donor cell survival was comparable between both groups at any time point (Fig. 2C–E). Immunofluorescence staining 4 weeks after treatment revealed that some GFP+ cells could be detected within the epicardial graft of animals from both the CL-MSG (Fig. 2F) and CL-MSG+OM groups (Fig. 2G). These donor CL-MSC remained within the graft or were found aligned on top of the epicardium, without evidence of migration toward the ischemic area (Fig. 2F, G). Also, there was no evidence of in situ differentiation of CL-MSC into mature cardiomyocytes, as expression of alpha sarcomeric actin was not detected (data not shown).
LV function and structure assessment by echocardiography
Transthoracic echocardiography 2 weeks after induction of MI confirmed the presence of LV remodeling and deterioration of heart function, as a significant increase in LV internal dimensions both in systole and diastole, as well as a decrease in LV thickness and marked declines in EF and fractional shortening (FS) were found in all groups compared to baseline (Supplementary Table S1). Of note, animals assigned to the CL-MSCG group had a more severe decrease in wall thickness before treatment. (Fig. 3 and Supplementary Table S1).

Echocardiographic evaluation of LV remodeling and function of infarcted untreated rats (MI), OM-, CL-MSCG-, and CL-MSCG+OM-treated rats, before (baseline), 2 and 6 weeks after myocardial injury.
Evaluation 4 weeks after treatment revealed that therapeutic intervention with the CL-MSCG supplemented with omental flap (CL-MSCG+OM) led to an improvement of wall thickness, since values in diastole increased and were comparable to baseline and values in systole were significantly increased compared to week 2 in the same animals (p<0.01). CL-MSCG+OM treatment significantly increased wall thickness in diastole and systole compared to MI (p<0.0001), OM (p<0.05 and P<0.01, respectively), and CL-MSCG (p<0.05 and P<0.01, respectively) groups, 6 weeks after injury (Fig. 3 and Supplementary Table S1). CL-MSCG-treated animals also displayed an improvement in LV wall thickness in systole and diastole from week 2 to 6 after MI. Treatment with CL-MSCG and CL-MSCG+OM attenuated further LV dilation from 2 to 6 weeks after MI. Consequently, MI and OM groups had increased LV internal dimensions in systole from week 2 to week 6 after MI (p<0.05). Moreover, cardiac dysfunction was ameliorated 6 weeks after injury in CL-MSCG+OM animals, as FS was higher in this group compared with infarct control and OM rats (p<0.05, respectively). FS remained stable in CL-MSCG rats from week 2 to 6 after infarction. LVEF in CL-MSCG+OM animals (47.01%±2.02%) was higher than that observed in MI (37.75%±2.26%, p<0.05), and OM (37.24%±3.37%, p<0.05) after 6 weeks of MI (i.e., 4 weeks after treatment). No statistical significance in EF was found between CL-MSCG- and CL-MSCG+OM-treated animals at 6 weeks post-MI (Fig. 3 and Supplementary Table S1). Moreover, CL-MSCG+OM-treated rats displayed a 20.32% increase in EF from week 2 to 6 after MI, while CL-MSCG treatment induced a 2.04% increase in EF. In contrast, a negative change in EF was observed from week 2 to 6 after injury in both MI and OM-treated animals (−5.58% and −17.34%, respectively).
Hemodynamic measurements
Hemodynamic analyses carried out 4 weeks after treatment (Table 1) showed significantly lower LV-end diastolic pressure in the CL-MSG+OM group compared to MI (3.53±0.34 vs. 5.21±0.54; p<0.05). CL-MSCG+OM-treated rats displayed improved contractility (increased dP/dt max) and a better LV relaxation rate (lower dP/dt min) compared to untreated rats (p<0.05, respectively). The cardiac output was higher in both CL-MSCG- and CL-MSCG+OM-treated rats compared with MI rats (p<0.05). Stroke volume (SV) was also increased in these groups, but only a significant higher SV was observed in CL-MSCG+OM relative to MI animals (p<0.05).
Statistical significance is indicated as follows:*ap<0.05 vs. MI; **ap<0.01 vs. MI; #p<0.001 vs. MI; *bp<0.05 vs. OM; *cp<0.05 vs. CL-MSCG; **cp<0.01 vs. CL-MSCG; **dp<0.01 vs. CL-MSCG+OM.
CL-MSCG, cord-lining mesenchymal stem cell graft; OM, omental flap; MI, myocardial infarction; LVEDP, left ventricular end-diastolic pressure; BPM, beats per minute; IRP, isovolumetric relaxation period.
LV infarct size and vascularization
Treatment with CL-MSCG and CL-MSCG+M led to smaller scar size compared to untreated hearts (p<0.01 and p<0.0001, respectively), as assessed by a measurement of the percentage of the LV cross-sectional area containing fibrosis (Table 2). On the other hand, the scar size in the OM group was comparable to MI. Consistent with an echocardiographic evaluation, CL-MSCG+OM-treated hearts displayed more conserved LV dimensions in comparison to MI hearts (Fig. 4). The implanted CL-MSCG alone or in combination with omental flap engrafted to the epicardium of the scarred myocardium. The LV wall of all treated hearts appeared thicker than untreated hearts. This increase in thickness was due, in part, to the presence of the epicardial graft and the omental flap in the CL-MSCG and OM groups (Fig. 4). In contrast, the increased wall thickness in the CL-MSCG+OM group was associated with the presence of a viable myocardium. Furthermore, abundant blood vessels were observed both within the remains of the CL-MSCG and/or the wrapped omentum.
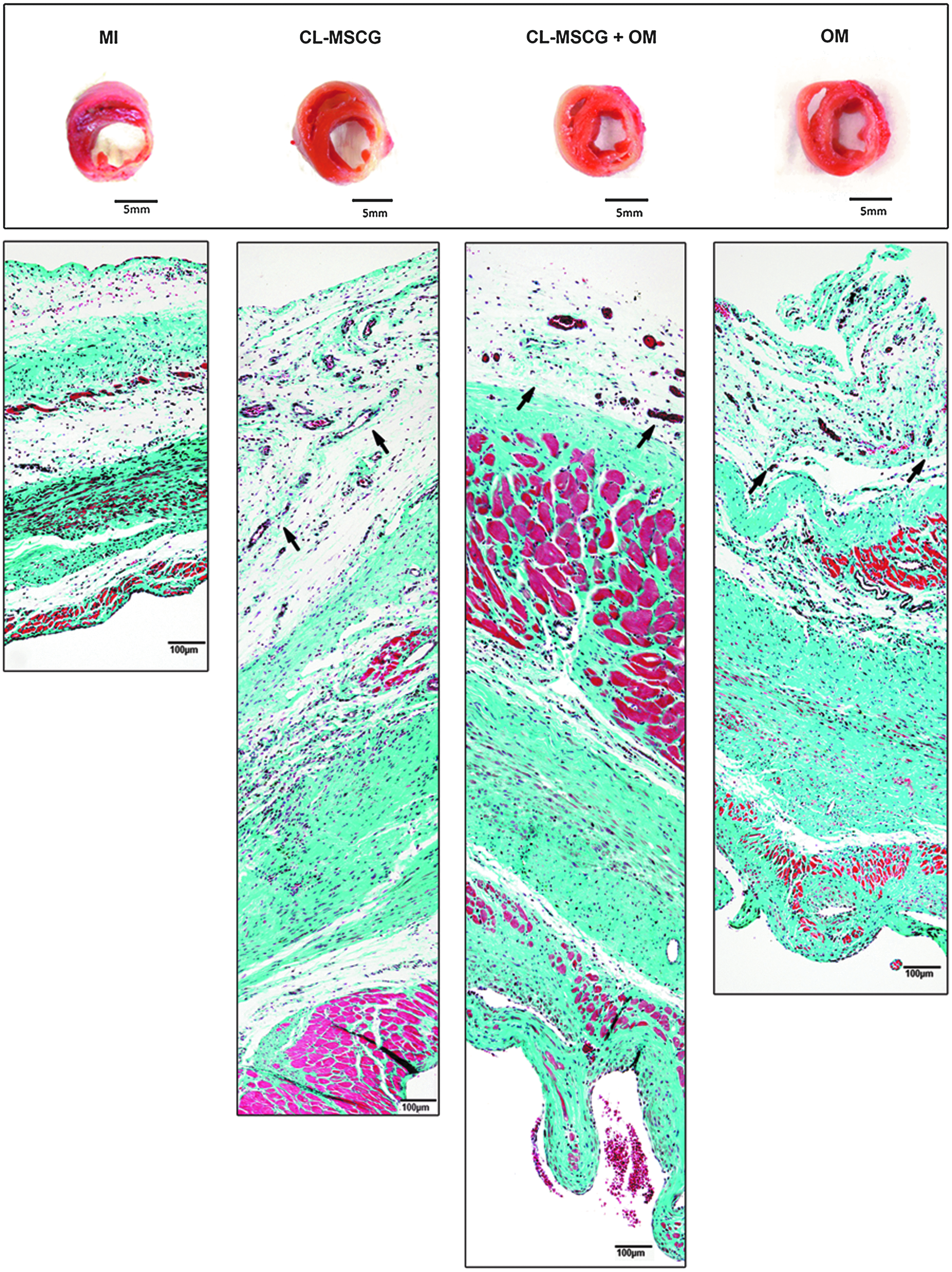
Morphology of explanted hearts 4 weeks after treatment. Top panel: Midventricular cross section of infarcted untreated rats (MI), CL-MSCG-, CL-MSCG+OM-, and OM-treated rats, 4 weeks after treatment (i.e., 6 weeks after myocardial injury). CL-MSCG+OM-treated hearts displayed more preserved LV dimensions in comparison to MI hearts, whereas the wall thickness appears higher in all treatment groups with a better enhancement in CL-MSCG+OM hearts. Lower panel: Reconstruction of the LV wall using Masson's trichrome staining micrographs taken in the scar area (100×) confirmed enhancement of wall thickness in all treatment groups. However, this increase seems to be due to the presence of the graft in the CL-MSCG or the omentum in OM hearts. In contrast, there is a considerable amount of viable myocardium in the CL-MSCG+OM- treated hearts along with reduced collagen deposition. Abundant blood vessels are observed within the graft area of CL-MSCG and CL-MSCG+OM. Black arrows indicate the joint between the epicardium and the graft and/or the omental flap.
Left ventricular scar size determined by midline length measurement on Masson's trichrome-stained sections.
Statistical significance is indicated as follows: **ap<0.01 vs. MI; ***ap<0.001 vs. MI.
Four weeks after treatment, CL-MSCG+OM hearts had a greater amount of DiI+ functional blood vessels in the LV scar area per 100× field (17.6%±0.5%) compared to untreated MI (6.3%±0.8%, p=0.0004), CL-MSCG (8.4%±0.7%, p=0.001), and OM (12.8%±0.6%, p=0.003) (Fig. 5A–E). Quantification of blood vessel density on Masson's trichrome-stained sections showed similar results to our analysis using DiI, as the CL-MSCG+OM group exhibited a higher blood vessel density (5.8±0.9 blood vessels/hpf) compared to all the other groups (1.8±0.3 blood vessels/hpf, p<0.001 vs. MI; 3.3±0.5 and 3.3±0.4 blood vessels/hpf, p<0.05 vs. CL-MSCG and OM respectively; Fig. 5F). This higher degree of vascularization consisted of both formation of capillaries and arterioles. In this analysis, CL-MSCG and OM groups also had increased total blood vessel density than MI (p<0.05). Although all treated hearts displayed a higher arteriole density compared to untreated hearts, the combination of the CL-MSCG and omental flap had a superior impact on arteriogenesis with a 20-fold increase in the arteriole density compared to MI (p<0.01). Likewise, a higher amount of RECA+ blood vessels were observed within the LV scar area of all treatment groups, particularly in CL-MSG+OM animals (Supplementary Fig. S2). It is possible that the results for DiI analysis and vascular density measured in histological sections differ in the CL-MSCG group due to the different numbers of rats analyzed, as DiI perfusion was only performed in 3 animals per group.
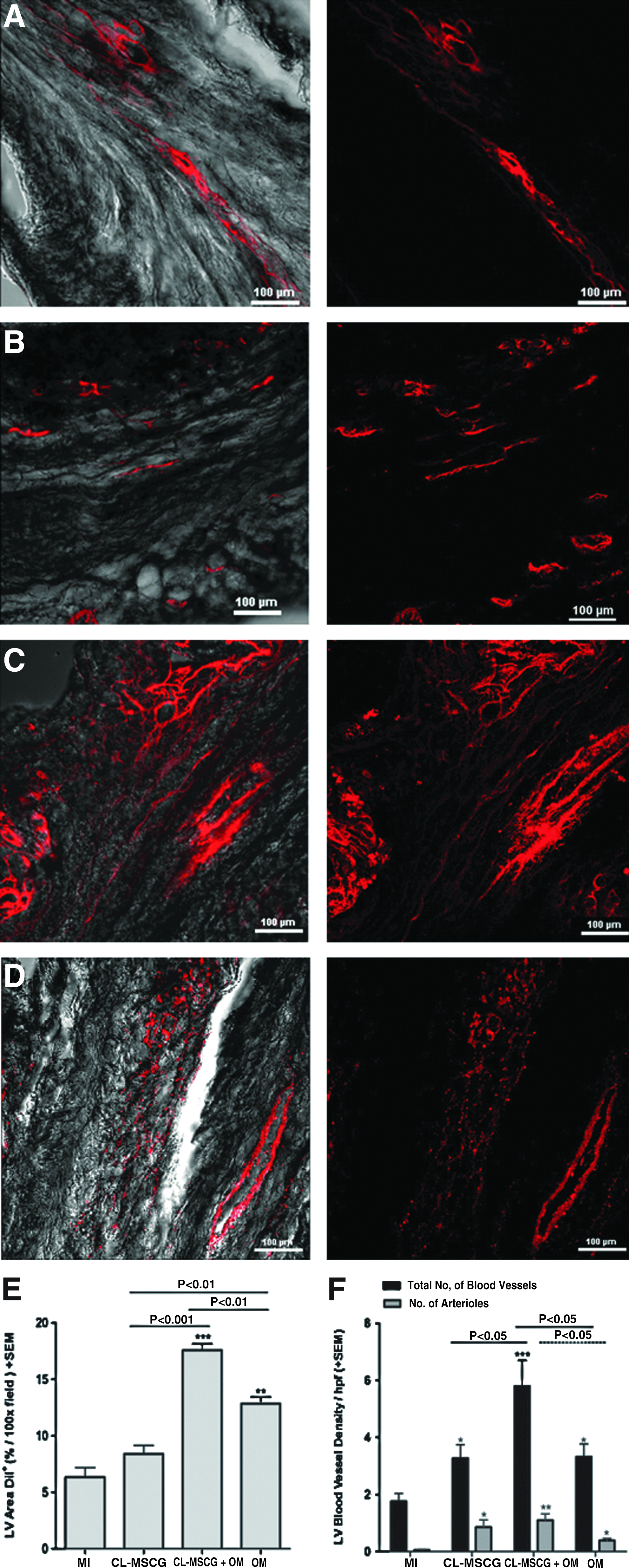
Confocal micrographs of the LV scar area after perfusion with 1,1′-dioctadecyl-3,3,3′,3′-tetramethylindocarbocyanine perchlorate (DiI) to visualize functional blood vessels in
Discussion
Here we introduce CL-MSC as a foundation for a combined strategy to treat the chronically injured myocardium. CL-MSC are likely to hold excellent therapeutic potential in the context of myocardial repair, as they are young MSC that are easy to expand and have immunomodulatory and immunosuppressive capabilities.10,11 Moreover, CL-MSC constituted a robust cell type that could endure the harsh microenvironment provided by a 3D static culture with a minimal apoptosis rate during the first 3 days in culture, as assessed by active caspase-3 staining. We also introduce an engineered tissue graft for cardiac repair that uses fibrin glue as a cell delivery and cell retention device. Fibrin glue is a readily available and a clinically established hemostatic compound that enables cell attachment, growth and differentiation and promotes tissue formation and organization. 23 Also, this scaffold material exhibits cytoprotective effects on MSC by providing a microenvironment that protects cells from deleterious effects triggered by hypoxia. 24
A noninvasive prospective evaluation of early donor cell survival in vivo indicated that this was comparable between CL-MSCG and CL-MSCG+OM, with a progressive decrease in cell bioluminescent signals from day 1 to 14 after an epicardial graft implantation. This survival pattern displayed by CL-MSC in vivo is consistent with a previous report in which it was also demonstrated that early survival times of CL-MSC are superior to BM-MSC in a xenotransplantation model in immunocompromised mice. 11 To note, CL-MSC within 3D grafts displayed acceptable early survival in vivo either with immediate vascular supply or not. Although several studies in animal models of MI have demonstrated the ability of transplanted BM-MSC to engraft and differentiate into cardiomyocytes and vasculature cells,25–27 we were not able to detect the expression of mature cardiomyocyte or vascular cell markers in engrafted CL-MSC despite their ability to express genes important in cardiac differentiation, such as Gata4 and NKX2.5 by CL-MSC before an epicardial graft implantation. Cardiomyogenic differentiation of BM-MSC has been reported in both allogeneic22,28 and xenograft models.29,30 Toma et al. found that human BM-MSC injected into healthy SCID/beige adult mice hearts underwent cardiomyogenic differentiation. 29 In vitro studies suggest that a cell-to-cell direct contact between resident cells and BM-MSC is critical in MSC differentiation into cardiomyocytes or smooth muscle cells. 31 However, our results are in agreement with reports that have not evidenced stem cell differentiation upon cardiac delivery.32–34 Recently, it has been reported that neither in vitro treatment of human and murine bone-marrow MSCs, nor allogeneic intramyocardial transplantation of murine BM-MSC resulted in MSC-derived functional cardiomyocytes. 32 Treatment of human MSCs (hMSCs) with cardiomyogenic differentiation media led to an enhanced expression of cardiomyogenic genes and proteins, yet no functional cardiomyogenic differentiation of hMSCs was observed in vitro. In another study, the fate of adult human bone marrow-derived MSC has been investigated after injection into the heart of immunocompetent SD rats, with or without immunosuppression and into the heart of athymic nude rats. 34 The authors found that when BM-MSC injected directly after LAD ligation are rejected in some of the nude animals, while delayed implantation lead to hMSC survival up to 6 weeks. Yet, the implanted BM-MSC did not undergo cardiomyogenic differentiation in this xenograft model. Since this is the first study using CL-MSC for postischemic myocardial repair, and both the source of MSCs as well as the implantation technique in our xenograft model differ from prior studies, we cannot draw definite conclusions regarding the possibility of in situ CL-MSC differentiation. Consistent with previous CL-MSC characterization studies, we detected the expression of early stem cell markers by CL-MSC in vitro.10,35,36 Since it has also been found that umbilical cord-lining cells lack tumorigenicity, 27 we do not intend to claim that CL-MSC are phenotypically equivalent to embryonic stem cells, but constitute an appealing alternative to BM-MSC.
Furthermore, postischemic therapy with a CL-MSCG supplemented with omental flap in a model of heart failure in nude rats improved myocardial function as assessed by measurement of LV pressure, contractility (dP/dt max), and the relaxation rate (dP/dt min) 6 weeks after myocardial injury. Treatment with a graft containing CL-MSC prevented further deterioration of cardiac function and led to a 2.04% increase in EF. Notably, a 20.32% increase in EF from week 2 after MI to week 6 (i.e., 4 weeks post-treatment) was evidenced in CL-MSC+OM-treated animals. Although this improvement did not reach a statistical significance, changes in LVEF of this magnitude accompanied with relief of heart failure have a clear clinical benefit. The epicardial implantation of a graft containing CL-MSC alone or in combination with omentopexy also led to an improved cardiac output and less LV remodeling. Histological morphometric studies demonstrated that treatment with CL-MSCG and CL-MSCG+OM led to an important decrease in the LV scar size. LV dimensions were also preserved to some extent in OM rats and this could be explained by the restrictive effect that omentopexy may have on the LV wall, thereby attenuating LV dilation. However, the latter was not associated to a significant reduction in LV fibrosis or to an improvement in the cardiac performance.
We and others have indicated the significance of structural support to the injured myocardium as an essential part of any restorative procedure.18,37–40 Key structural effects of myocardial injury include nonischemic expansion of the infarct, aneurysmal conversion of the scar region, and shift of muscular band shear stress lead to a loss of heart function. Reversing the increased circumferential wall stress and preventing LV dilation may be as important as the application of stem cells in restoring the ischemic myocardium. In this study, additive effects of both CL-MSC and omental flap wrapping may have prevented further LV dilation.
Treatment with either CL-MSCG or OM increased the arteriole density compared to untreated hearts. Yet, the combination CL-MSCG+OM had a superior impact on arteriogenesis and capillary formation. It has been shown that omentopexy may potentiate angiogenesis induced by cell therapy, 19 as the omentum may be a source of endogenous growth factors, which may have cardioprotective effects on the remaining viable cardiomyocytes. 17 While our study agrees with previous reports suggesting a beneficial effect of omentopexy on myocardial angiogenesis, and it may modulate negative remodeling through restricting the dilatation of the LV chamber, it is obvious that this approach by itself does not seem sufficient to restore the scarred myocardium or enhance the cardiac performance in failing hearts.
On the basis of our present results, we speculate that our CL-MSC-derived graft combined with omental flap has a synergistic effect that promotes myocardial revascularization. Both local25,27,41,42 and systemic 43 delivery of allogeneic MSC increases vasculogenesis, enhances myocardial perfusion,27,43 and improves postinfarct cardiac function. Growing evidence supports a paracrine-mediated stem cell action in tissue protection and repair. 44 It has been demonstrated that MSCs can secrete growth factors and cytokines, which promote cardiac repair in a paracrine fashion following a myocardial injury. It seems that these paracrine mediators are expressed or released in a temporal and spatial manner exerting different effects depending on local tissue factors after injury. 6 Upregulation of multiple paracrine factors, such as angiogenic cytokines (VEGF-A, HGF, bFGF, angiopoietin-1 and −2, and PDGF-B), cardiac transcription factors (GATA-4, Nkx2.5, and MEF2C), and antiapoptotic factors, have been found in hearts treated with human BM-MSCs. 8 Under hypoxic conditions, MSCs secrete several cytoprotective molecules involved in cell proliferation and survival and in angiogenesis.6,7,45 Also, MSCs exert antifibrotic paracrine effects through the expression of various molecules involved in biogenesis of the extracellular matrix. 46 Thus, it is likely that in the present study, paracrine factors released by CL-MSC modulated the amelioration of cardiac function through enhanced neovascularization and attenuation of LV remodeling via immune modulation, inhibition of apoptosis, and collagen deposition, while the omentum directly provided blood supply and possibly humoral factors. The omentum is also a source of mesothelial cells, which display similar morphological and functional properties to endothelial cells, and secrete various angiogenic growth factors that induced angiogenesis and arteriogenesis as well as attenuation of LV remodeling in ovine infarcted hearts. 47 The combination these effects derived from CL-MSC and the omentum may limit LV remodeling. Altogether, in our study, this additive effect resulted in the improvement of cardiac function and structure even after the onset of significant LV dysfunction.
The choice of a postacute myocardial injury model holds a translational value. It has been suggested that the optimal time for cell therapy is 1 week or more after MI, while a negligible benefit is seen after early treatment. 48 The majority of patients in need of a structurally relevant restorative procedure are those with ischemic myocardial injury in the chronic phase, symptoms of heart failure, reduced EF, and demarcated LV scars or aneurysms. Often, these patients have triple vessel coronary artery disease, which is not amenable to traditional revascularization modalities. The only alternative therapies in the advanced stage of disease are transplantation or assist device implantation, which may not be applicable to many candidates, the elderly in particular. To date, cell- or tissue-based restorative approaches have failed to reach broad clinical acceptance. Our strategy may provide an alternative as a stand-alone or supplementary treatment for these patients. Isolation and expansion of CL-MSC is easier compared to cord blood-MSC. 49 Furthermore, CL-MSC are obtained through a noninvasive alternative method compared to that involved in collection of bone marrow or adipose tissue for the isolation of MSC. Preparation of the compound will require storing the umbilical cord for use later in life, or using cord-lining cells from a ubiquitous pool, once immunogenic barriers have been overcome. The development of a large animal model exploring the strategy presented in this study may be useful to obtain a better approach to the clinical reality before the application of CL-MSC in first-in-man trials. Furthermore, the utilization of an alternative source of vascularized pedicle such as that recently reported by Bayes-Genis et al. 50 in which a pericardial vascularized adipose flap was used to treat infarcted heart in a porcine model, could be applied to facilitate the surgical approach to deliver a combined (CL-MSC+vascular pedicle) therapy.
In summary, we have shown the potential of CL-MSC supplemented with direct vascular supply to repair failing hearts. This strategy improved myocardial revascularization, attenuated remodeling and ameliorated cardiac dysfunction, and supports the notion of revascularization and paracrine factor-mediated myocardial repair instead of cell differentiation-mediated replacement of the injured myocardium.
Footnotes
Acknowledgments
Microscopy data and imaging for this study using a Nikon A1R confocal microscope were acquired and processed in the SBIC-Nikon Imaging Centre at Biopolis, Singapore. The authors would like to thank Mr. Jing Wang (Department of surgery, National University of Singapore), and Ms. Mary Joyce Galupo and Ms. Geronica Songco (Cardiac Department, National University Heart Centre, Singapore) for their technical support. This research was supported by Associate Professor Theo Kofidis' Biomedical Research Council grant (BMRC/07/1/21/19/510).
Disclosure Statement
Dr. TT Phan is the founder and shareholder of CellResearch Corp Pte Ltd. The other authors have no competing financial interests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.