
Abstract
Bone regeneration is one of the focus points in the field of regenerative medicine. A well-known stimulus of bone formation is bone morphogenetic protein-2 (BMP-2), which has already been extensively used in clinical applications. However, due to a short half-life, supraphysiological doses are applied resulting in severe side effects such as ectopic bone formation or even loss of bone. We compared the effectivity of transient BMP-2 gene delivery with the BMP-2 protein at clinical (high) and physiological (low) doses by subcutaneous implantation of alginate-based constructs in mice. After 6 weeks of implantation, both the protein laden constructs and BMP-2 plasmid DNA-based constructs showed similar early bone onset and elevated bone formation compared to controls without any BMP-2 added. We found no differences in efficiency by using BMP-2 plasmid DNA or any of the BMP-2 protein dosages. Therefore, we conclude that BMP-2 plasmid DNA-based gene therapy in alginate is a promising new strategy for BMP-2 administration for bone (re)generation.
Introduction
Gene therapy is most often applied by viral gene delivery, which results in high transfection efficiencies, but is associated with problems such as host immunogenicity and virus-dependent recombination risks.9–11 Nonviral gene delivery techniques aim at transient expression of the desired gene and are therefore not hampered by the risks of integration-dependent mutations. A disadvantage is that nonviral transfection methods are notoriously inefficient. Therefore, much effort has been invested in the development of an efficient nonviral gene delivery method, with the use of various transfection agents 12 and application matrices. 13 Our group developed a method for efficient gene delivery based on alginate hydrogel, which is compatible with simultaneous cell seeding. 14 Alginate was chosen, because this anionic polysaccharide that gelates with bivalent cations such as Ca2+15 is approved by the Food and Drug Administration (FDA), nontoxic, and biocompatible. Combined with other hydrogels or in the form of nanoparticles, it has been used as a vehicle for plasmid DNA before.16–18
In comparison to established nonviral gene delivery methods such as polyethylenimines (PEI), poly(lactic-co-glycolic acid) (PLGA), and chitosan, alginate is able to induce similar transfection efficiencies (PEI 50%, 19 PLGA 80%, 20 chitosan 20%, 21 and alginate 60%14,22). To reach these transfection efficiencies, the proteins or polymers are often combined with other materials. Increased polymer concentrations are associated with higher transfection efficiencies, but often lead to cell death. For alginate, this phenomenon has not been described, and low concentrations appear to be successful at inducing cell transfections. 14 In terms of practicality, the alginate gel simultaneously acts as a cell carrier, transfection agent, and protein release system. This combination of factors is not found in the other transfection agents. It has been successfully applied in bone tissue engineering applications both in vitro and in vivo,23,24 which makes it very suitable as a gene activated matrix for cell-seeded constructs.
Our aim is to apply BMP-2 plasmid DNA-based constructs for bone tissue engineering. The present study investigates whether BMP-2 plasmid DNA-based constructs can be as efficient in inducing bone formation as the recombinant BMP-2 protein.
Materials and Methods
Alginate gel
Autoclaved high-viscosity nonmedical-grade alginate powder (International Specialty Products, ISP) was dissolved at a concentration of 10 mg/mL in the alpha minimum essential medium (α-MEM; Gibco). The gel was polymerized by adding an equal volume of 100 mM autoclaved CaCl2 supplemented with 10 mM of 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid (HEPES) pH 7.4 (Gibco) for 10 min. The Ca2+ solution was then replaced by 1 mL of expansion medium.
Cell culture
Goat MSCs were isolated from bone marrow (BM), aspirated from the iliac wings of Dutch milk goats. The MSCs are isolated by adherence to tissue culture plastic and cultured in the expansion medium, containing αMEM (Gibco), supplemented with 15% (v/v) fetal calf serum (Cambrex), 100 U/mL penicillin, 100 μg/mL streptomycin, and 2 mM
Preparation in vivo implants
Four different constructs were made, each consisting of 200 μL alginate (10 mg/mL), 107 goat MSCs/mL gel, and 20% (w/v) biphasic calcium phosphate (BCP) particles (size 106–212 μm). The BCP particles consisted of 80%±5% (w/v) hydroxyapatite and 20%±5% (w/v) β-tricalcium phosphate, and total porosity was 70%±5%, macroporosity 55%±5%, and microporosity 20%±5% (kindly provided by Xpand Biotechnology). The BCP particles were cleaned in an ultrasonic bath and sterilized by autoclaving. The BMP-2 plasmid DNA construct contained the full-length human recombinant BMP-2 cDNA, whose expression was driven by the cytomegalovirus promoter in pcDNA3.1 (Invitrogen). Recombinant human BMP-2 protein (rhBMP-2) was obtained from a clinical kit (Infuse; Medtronic).
The four different constructs were further supplemented as follows: group (1) buffer (control), group (2) 25 ng/mL rhBMP-2 protein (BMP-2 low), group (3) 25 μg/mL rhBMP-2 protein (BMP-2 high), and group (4) 10 μg/mL of pcDNA3.1/hBMP-2 plasmid DNA. BMP-2 protein or plasmid DNA was added before alginate polymerization with 1 mL of 100 mM autoclaved CaCl2, supplemented with 10 mM of HEPES (pH 7.4; Gibco), for 10 min. The supernatant was removed and all implants were kept in the MSC culture medium until implantation (within 2 h)
Animals and implantation
Female nude mice (Hsd-cpb:NMRI-nu; Harlan) were anesthetized with 1.5% isoflurane, after which the implants were placed in four separate subcutaneous dorsal pockets per mouse (n=6 per group). To prevent mutual influence of neighboring samples, they are implanted in a randomized fashion. The animals were postoperatively treated with the analgesic buprenorphine (0.05 mg/kg, subcutaneously, Temgesic; Schering-Plough) and housed together at the Central Laboratory Animal Institute, Utrecht University. At 3 weeks after implantation, calcein green was administered s.c. (10 mg/kg; Sigma), and at 4 weeks after implantation, Xylenol orange was administered s.c. (30 mg/kg; Merck). 25 Experiments were conducted with the permission of the local Ethics Committee for Animal Experimentation and in compliance with the Institutional Guidelines on the use of laboratory animals.
Explantation and embedding
Six weeks after implantation, the constructs were retrieved to analyze general morphology, transfection, and bone histomorphometry. Samples were cut in two, one part was fixed overnight in 4% (v/v) formalin containing 100 mM CaCl2 and processed for 5-μm-thick decalcified paraffin sections through alcohol dehydration series. The other half was fixed in 4% (v/v) phosphate-buffered formalin, dehydrated by ethanol series, and embedded in polymethylmethacrylate (MMA), after which 10-μm-thick sections were sawn from the center and side of each implant using a sawing microtome (Leica). These sections remained unstained for fluorochrome analysis. The presence of each fluorochrome label was scored for all implants.
Immunocytochemistry
Paraffin sections were stained with hematoxylin/eosin (HE). Blinded samples were scored for morphology and presence of blood vessels by two observers (FW, YvdH).
Safranin O staining
Sections were deparaffinized and incubated with hematoxylin (Weigert's) for 5 min. After washing in running tap water, sections were dipped in distilled water and counterstained in a 0.4% (w/v) Fast Green Solution. Sections were rinsed in 0.17 M acetic acid until the color no longer runs and counterstained again in freshly prepared 0.125% (w/v) Safranin O (Merck) staining dissolved in distilled water. After a short dehydration protocol, sections were mounted in Depex. Two independent observers (FW, YvdH) scored for presence of cartilage.
Histological scoring
HE stained sections were scored for several general histological parameters (Table 1). Bone, BM, and cartilage were scored for the presence or absence of these features. For blood vessels, more than 10 vessels/microscopic field was scored as positive. For capsule formation, the criterium was a thickness of five cell layers; more than five cell layers received a positive score and less than five cell layers a negative score. All histological scorings were performed by two independent observers (FW, YvdH) in a blinded fashion. The incidences of parameters are calculated as% of the total number of animals.
Scorings of the percentage of samples with bone, BM, cartilage, blood vessels, and a fibrous capsule present (n=6 per group) in the in vivo samples after 6 weeks.
Significantly lower bone incidence compared to BMP-2 low and BMP-2 high.
Significantly higher BM incidence compared to the control and plasmid DNA group.
Significantly higher cartilage incidence compared to all other groups.
BMP-2, bone morphogenetic protein-2; BM, bone marrow.
Bone histomorphometry
High-resolution digital photographs were made from HE stained sections for histomorphometric analysis. Three pictures at predefined positions within the explant were taken from each sample. Bone and scaffold were pseudocolored using Adobe Photoshop CS3, whereafter histomorphometry was performed using Axiovision software (version 3; Zeiss). A custom macro was used to measure the region of interest, the area of scaffold, the area of bone, the scaffold outline available for bone apposition, and the contact length of bone and scaffold. This allowed the calculation of both the percentage bone per available space, called bone area% (=[bone area/total area−scaffold area]×100%), and the percentage bone apposition, called contact% (=[bone-to-scaffold contact length/scaffold outline] ×100%). 2
Fluorochrome analysis
The fluorochrome markers were analyzed from the unstained sections using a fluorescence microscope (Olympus BX51 microscope, Olympus DP70 camera) equipped with a quadruple filter block (XF57, dichroic mirror 400, 485, 558, and 640 nm; Omega Optics). Fluorochromes incorporated in the newly formed bone were scored for presence/absence. To discriminate between the bone and the underlying scaffold, the fluorescence signal was compared to the brightfield signal.
Statistics
The statistical significance of mutual differences between the control group, the low dosed BMP-2 protein group, the high dosed BMP-2 protein group, and the plasmid BMP-2 group in Figure 1 were assessed using a randomized block design. Multiple comparisons were generated using a Tukey post hoc correction to calculate the p-values. A p-value of<0.05 was considered significant.

Bone and cartilage formation in vivo.
For Table 1, a Chi-square test was performed to evaluate statistical differences between the control group, the high and low dosed BMP-2 protein groups, the BMP-2 plasmid DNA group, and the precultured plasmid DNA group for presence or absence of several histological features. Multiple comparisons were generated using a Bonferroni correction to calculate the p-values. A p-value of<0.05 was considered significant.
Results
From previous studies in which the alginate gel was combined with BMP-2 plasmid DNA and MSCs, it has become clear that this is a successful method to transfect cells. When BCP particles are added, osteogenic differentiation is induced in vivo as well. 14
To investigate whether bone formation induced by plasmid DNA can reach an efficiency similar to bone formation induced by BMP-2 protein, alginate-based samples were implanted subcutaneously in mice. Histology of the implanted constructs revealed abundant quantities of bone in all BMP-2 containing constructs. In the control group without BMP-2 in any form present, some bone formation was seen on the BCP particles. Large quantities of bone bridging the BCP particles were mainly found in the BMP-2 containing groups (Fig. 1a–d). Both the BMP-2 protein groups and the plasmid DNA group appear to induce similar amounts of bone. Besides bone, BM consisting of adipose tissue and heterogeneous small nucleated cells was present in all groups containing extensive bone formation. This was seen more often in the BMP-2 protein groups (Table 1, Fig. 1f ). All constructs were well vascularized, as seen by abundant blood vessels and no signs of an inflammatory response were present. Alginate remnants were not detected in any of the samples indicating that it had been degraded completely. Hardly any capsule formation was detected and if there was some fibrous tissue surrounding the implant this was less than five cell layers thick. In all groups containing bone, some cartilage formation was detected as well (Fig. 1g, h). Both the control group and the high and low dosed BMP-2 protein groups presented cartilage formation. In the plasmid DNA group, all implants containing bone also exhibited areas with cartilage formation (Table 1, Fig. 1g, h).
The onset of bone formation was investigated by fluorochrome analysis. Calcein green (green fluorescent label) was administered at week 3 and Xylenol orange (orange/red fluorescent label) was administered at week 4. The fluorochromes showed a general onset of bone formation in all BMP-2 constructs before week 3. No clear differences between the two different protein concentrations and the plasmid DNA-based group were found, although the BMP-2 protein high-concentration group was the only group in which we found both labels in all samples within the group. The control group contained one sample showing early bone formation and all other samples did not incorporate any of the labels (Fig. 2).
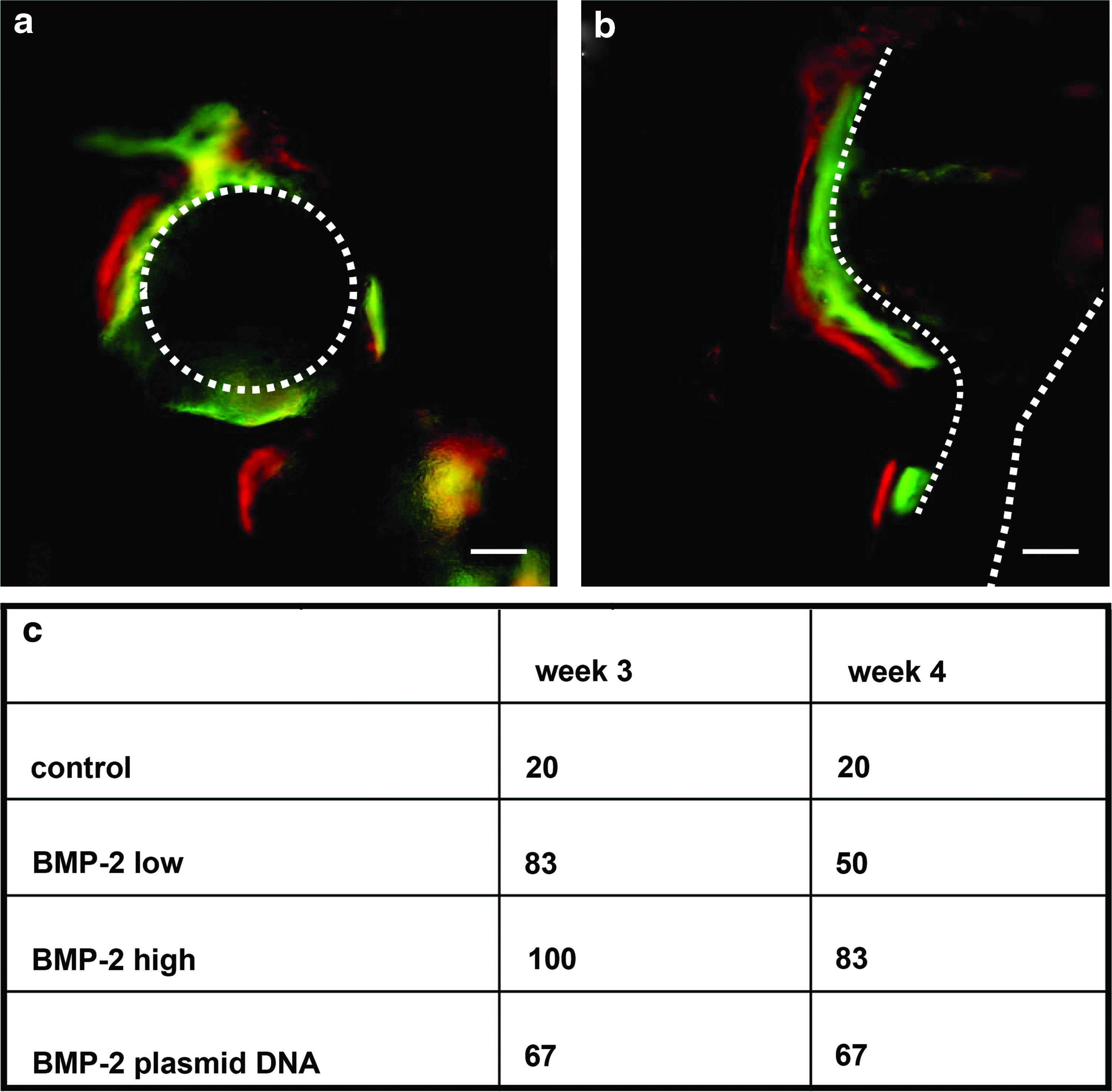
Bone onset analyzed by fluorochrome incorporation. Detection of calcein green, administered at week 3 after implantation and Xylenol orange, administered at week 4 after implantation.
To quantify the amount of bone in the implants, bone histomorphometry was performed on the HE stained sections for determination of both bone area% and bone contact% (Fig. 3). In the control group, an average of 15% bone area and 20% bone contact was found. Compared to the control, the BMP-2 protein low-concentration group showed a trend, though not statistically significant, toward a higher amount of bone formed: up to 30% bone area and 40% bone contact. Very similar results were found for the high dosed BMP-2 protein group with an average of 31% bone area and 41% bone contact (p<0.05 compared to control). The plasmid DNA laden group presented the highest amount of bone formation with an average bone area of 38% and bone contact of 44% (p<0.05 compared to control).

Quantification of bone formation. Analysis of bone area% and bone contact% (for details see Materials and Methods). *Significantly different from control group, p<0.05.
Discussion
This study investigated whether BMP-2 plasmid DNA-based gene delivery can be as efficient at inducing bone formation as rhBMP-2 protein application. To this end, we used a gene delivery method that was recently developed by us to express BMP-2 in hybrid constructs implanted subcutaneously in mice and compared this to two BMP-2 protein concentrations and unloaded controls. After 6 weeks in vivo, BMP-2 added in the form of plasmid DNA was very efficient in stimulating bone formation and performed at similar levels as BMP-2 protein at both concentrations tested.
Gene therapy based on nonviral plasmid DNA is pursued by many groups because of its clear advantages, like transient expression, efficient protein production at low cost, but is also known for low transfection efficiencies. 26 Gene delivery using alginate has proven to result in high (up to 62% based on GFP expression) transfection efficiencies in different cell types in vitro, and osteogenic differentiation in vivo. 14 In the present study, the design of the constructs was changed to stimulate bone formation in this ectopic setting. The addition of ceramic particles optimized osteogenicity, while still allowing sensitivity to BMP-2. The plasmid DNA group has shown to be successful and is clinically relevant, reason why we focused on comparing different BMP-2 delivery methods to a BMP-2-free control.
When monitoring bone onset in the various constructs using fluorochromes, we found that bone formation had started before week 3 in BMP-2 laden samples. Almost all of these samples showed the presence of the green fluorescent label, which is in line with literature. 27 Early onset was not always followed by the incorporation of the orange label, a week later. This might be explained by the notion that bone formation was already so robust that available space for expanding bone formation was filled, halting further label incorporation after week 3. Another explanation could be that pores in the constructs were often filled with cartilaginous and/or BM-like tissue, which do not bind the fluorescent labels (Table 1).
To optimize the constructs and provide a mineralized surface for bone formation, BCP particles were added to the alginate in the present study. The particles, known to promote osteogenesis, were combined with goat MSCs, which contribute to bone formation in tissue-engineered constructs. 28 Therefore, some bone was also formed in the control samples, which is in accordance with previous results.29,30 The addition of BMP-2 in any form at least doubled the amount of bone present. Both the high and low dose of BMP-2 protein induced similar amounts of bone. The use of a supraphysiological dose of BMP-2 protein is highly debated. Several severe side effects, including bone loss have been reported, and insufficient research has been performed to establish an optimal dose. 5 Therefore, inclusion of a low-concentration protein group alongside the plasmid DNA group is relevant when considering the efficacy and safety of BMP-2. In literature, little is found on the comparison of different concentrations of BMP-2 to establish a minimal effective dose, and furthermore, a few published results suggest that a higher dose does not automatically increase bone formation.31,32 The majority of bone tissue engineering based on BMP-2 focuses on the prolonged release of BMP-2 from different hydrogel or ceramic carriers, to lower the initially applied dose of BMP-2.14,33 In vitro the responsiveness of several cell lines such as the MC3T3-E1 cells was established up to 50 ng/mL, which is more than four decades lower than the clinically administered dose, which is a 1.5 mg/mL scaffold. When translated to mice, the local dosages applied are the used 25 ng and 25 μg of rhBMP-2/mL construct, representing physiological (low) and clinical (high) doses. The in vitro dosage of released BMP-2 protein after transfection with 1 μg BMP-2 plasmid is in the order of 10–20 ng/mL and thus more comparable to the lower administered protein dose with respect to the BMP-2 quantities, but not the release or delivery kinetics. 14 In mice, no significant differences in bone onset or amount of bone were found when comparing high and a low dosage of BMP-2 protein and the BMP-2 plasmid laden group. We conclude that applying a low dose is sufficient to significantly enhance bone formation in this setting. In addition, it is known from previous experiments and literature that alginate is a slow release system for BMP-2, and that most of the protein is retained in the gel.14,33 In vitro studies indicated a BMP-2 release in and from the gel up until 5 weeks. Whereas taking into account that in vitro and in vivo protein expression are not always comparable, the presence of the gel likely functions as a controlled release system preventing high BMP-2 dosage.
Significant differences in bone formation were found between the high dosed BMP-2 group and the plasmid DNA group compared to control samples. This illustrates the additive effect of BMP-2 on cell laden BCP constructs, which presented a basal average bone area of 20%. The fact that BMP-2 plasmid DNA induced bone formation ectopically is consistent with the majority of studies described in literature. Both intramuscular and ectopic, either transfected MSCs or delivered BMP-2 plasmid DNA significantly increase bone formation compared to negative controls. These studies all reported considerably lower bone volume percentages than we found and did not mention the presence of cartilage or BM.13,18,27,34 Semiquantitative scoring revealed that BM was seen more frequently in the BMP-2 protein group as compared with the the BMP-2 plasmid DNA and simultaneously more cartilaginous tissue was visible. This might indicate that in samples containing BMP-2 plasmid DNA, endochondral bone formation plays a more important role than in the protein groups. This may be the result of different dosage at the start of the implantation, because it takes a few days for the cells to become transfected and start to produce BMP-2, whereas the protein laden groups have BMP-2 available immediately after implantation. Since there is some BM present in the plasmid DNA group and some cartilage in the protein groups, the most likely explanation is that both forms of bone formation occurred in all groups, but one is favored over the other, which is in accordance with other studies.35,36 As only small amounts of plasmid DNA are necessary, this method creates a cheap, nonviral substitute for the clinically used BMP-2 protein treatment for bone regeneration.
Conclusion and Future Direction
Using a recently developed gene delivery system, BMP-2 protein was substituted with BMP-2 plasmid DNA, which resulted in efficient bone formation in an ectopic mouse model. We conclude that BMP-2 plasmid DNA is a low-cost, nonviral alternative for BMP-2 protein used in bone tissue engineering and in the clinic. Studies establishing its minimal effective dose and safety, as well as effectivity in orthotopic locations will be necessary before clinical translation can be made possible.
Footnotes
Acknowledgments
The authors gratefully acknowledge the support of the Smart Mix Program of the Netherlands Ministry of Economic Affairs and the Netherlands Ministry of Education, Culture and Science.
Disclosure Statement
No competing financial interests exist.