
Abstract
Current surgical techniques for osteochondral injuries in young active patients are inadequate clinically. Novel strategies in tissue engineering are continuously explored in this area. Despite numerous animal studies that have shown encouraging results, very few large-scale clinical trials have been done to address this area of interest. To facilitate the eventual translation from rabbit to human subjects, we have performed a study using bone marrow-derived mesenchymal stem cell (BMSC)–oligo[poly(ethylene glycol) fumarate] (OPF) hydrogel scaffold in a porcine model. Our objective was to analyze the morphology of BMSCs seeded into rehydrated freeze-dried OPF hydrogel and in vivo gross morphological and histological outcome of defects implanted with the BMSCs-OPF scaffold in a porcine model. The analyses were based on magnified histologic sections for different types of cartilage repair tissues, the outcome of the subchondral bone, scaffold, and statistical assessment of neotissue-filling percentage, cartilage phenotype, and Wakitani scores. The morphology of the BMSCs seeded into the rehydrated freeze-dried OPF scaffold was observed 24 h after cell seeding, through the phase-contrast microscope. The three-dimensional and cross-sectional structure of the fabrication was analyzed through confocal microscopy and histological methods, respectively. The BMSCs remained viable and were condensed into many pellet-like cell masses with a diameter ranging from 28.5 to 298.4 (113.5±47.9) μm in the OPF scaffold. In vivo osteochondral defect repair was tested in 12 defects created in six 8-month-old Prestige World Genetics micropigs. The implantation of scaffold alone was used for control. Gross morphological, histological, and statistical analyses were performed at 4 months postoperatively. The scaffold–MSC treatment led to 99% defect filling, with 84% hyaline-like cartilage at 4 months, which was significantly (p<0.0001) more than the 54% neotissue filling and 39% hyaline-like cartilage obtained in the scaffold-only group. The implantation of BMSCs in freeze-dried OPF hydrogel scaffold, which created a conducive environment for cell infiltration and clustering, could fully repair chondral defects with hyaline-like cartilage. This protocol provides a clinically feasible procedure for osteochondral defect treatment.
Introduction
The treatment of osteochondral injuries using microfracture techniques usually results in the formation of fibrocartilage that has inferior biomechanical properties. 5 Although osteochondral autografts are composed of hyaline cartilage, its transplantation is plagued by incomplete integration with the surrounding normal cartilage and donor-site morbidity issues. 6 ACI produces a better hybrid of fibrocartilage and hyaline cartilage, 7 but requires prolonged and complicated rehabilitative processes. In view of these limitations, new strategies are being explored.
The tissue engineering strategy presents promising new approaches for the treatment of the osteochondral defect by combination of cell therapy, scaffold implantation, and the application of various growth and differentiation stimuli. The usage of tissue-engineered scaffolds alone has been shown to be effective in osteochondral treatments carried out in animal studies 8 involving the rabbit 9 and sheep 10 models. Unfortunately, these results have yet to be duplicated in the trials involving equine 11 and porcine 12 models. While the delivery of growth factors have shown promise in enhancing cartilage healing,13,14 its mechanisms have not been clearly elucidated. Moreover, the applicability of growth factors is restricted by commercial viability and repeated high-dosage requirements due to their short half-lives. Systemic side effects have also been reported, 15 leading to continued efforts in the improvisation of cell-augmented implants without growth factors
The gold standard in the treatment of osteochondral defects have been the usage of autologous chondrocytes that have been used in human trials for decades. 4 It is limited by a low chondrocyte yield and the dedifferentiation process that it undergoes upon in vitro expansion. 16 Mesenchymal stem cells (MSCs) provide a pool of reserved cell source for postnatal tissue self-renewal and wound repair. 17 These pluripotent cells can be extracted from bone marrow with minimal invasion and associated donor-site mobility linked to the harvesting of adipose tissue, skeletal muscle, synovial membrane, and periosteum for pluripotent stem cells. Bone marrow-derived mesenchymal stem cells (BMSCs) have been expanded in vivo without undergoing dedifferentiation. In addition, the safe usage and comprehensive evaluation of BMSCs in human patients had been reported in several clinical trials.18–20
Although naturally derived materials can function as natural substrates, cell adhesion sites, and conductive structures for tissue engineering, 21 they suffer from batch-to-batch variability. 22 A variety of synthetic polymers had been developed for cartilage-defect regeneration, with various modifiable properties such as mechanical strength, degradation rate, and chemical modification, including easily scalable production. 23 Besides these benefits, polyethylene glycol (PEG)-based synthetic polymers can also be easily polymerized by photoinitiators or chemical methods. The crosslinked, super hydrophilic polymer generates osmotic pressure that mimics the natural mechanical environment in cartilage and functions to protect the chondrocytes from mechanical injuries 24 and facilitates nutrient maintenance. 25
Oligo[poly(ethylene glycol) fumarate] (OPF) is a PEG-based polymer. 26 It has been well studied in vitro27,28 and in vivo, 29 with BMSCs for chondrogenesis-related research, and has been shown to contribute to cartilage repair. However, the majority of previous cartilage tissue engineering work that involved hydrogels for cell delivery utilized hydrogel-encapsulated cells, and these studies were limited to rabbit models. Targeting for a preclinical evaluation of this scaffold, we investigated the effect of implanting freeze-dried OPF hydrogel seeded with BMSCs in a porcine model. We hypothesized that the use of rehydrated freeze-dried hydrogels seeded with BMSCs offers several advantages, including cell clustering, which would induce chondrogenic differentiation, and immediate infiltration of host cells facilitated by hydrogel swelling. We postulate that these conditions would lead to an increased percentage of hyaline-like cartilage repair tissue.
Materials and Methods
Fumarate hydrogel scaffold preparation
Fumarate hydrogel was fabricated with the OPF polymer and bisacrylamide according to a published method.26,30 Briefly, OPF was dissolved in distilled water containing N, N′-methylene bisacrylamide as a crosslinking agent. Tetramethylethylenediamine and ammonium persulfate were added to initiate the crosslinking reaction of OPF. After vortexing, the solution mixture was injected into a Teflon mold to form the crosslinked sample. The crosslinked OPF was subsequently removed and freeze-dried. Dialyzed against distilled water, the hydrogel was freeze-dried and sliced into 1-mm-thick pieces. 12 The scaffold was rehydrated with 106 BMSCs in 0.2 mL phosphate-buffered saline (PBS), before press-fit filling of the chondral defect. For in vitro evaluation, the BMSC-seeded scaffolds were cultured in a BMSC growth medium (Dulbecco's modified Eagle's medium low-glucose with 10% fetal bovine serum [Invitrogen]) and 100 U/mL penicillin–streptomycin (Invitrogen).
Autologous MSC isolation and culture
MSCs were isolated and cultured following a protocol developed in our laboratory. 31 All the protocols had been approved by the Institutional Animal Care and Use Committee at National University of Singapore (NUS). Briefly, 10 mL of bone marrow from the posterior superior iliac spine of each pig was aspirated into a heparinized syringe. The bone marrow was then diluted with 10 mL of the BMSC growth medium. All the cells were spun down in a 50-mL conical tube at 1500 rpm for 10 min. After removing the fat-rich upper supernatant layer, the solution was topped up to 40 mL with a growth medium. The cells were resuspended, transferred into two 175-cm3 cell culture flasks, incubated at 37°C with 5% CO2, and cultured without interference for 5 days, with a medium change every 2–3 days. The attached cells were subcultured at a ratio of 1 to 4 till 90% confluency, trypsinized, and harvested for seeding. Henceforth, the treatment group subjected to the implantation of empty scaffolds and BMSC-seeded scaffolds would be referred to as the scaffold and scaffold–BMSC groups, respectively.
For in vitro evaluation, the BMSC-seeded scaffolds were cultured in a growth medium for 24 h, and the images were taken using a microscope fitted with a digital camera (Nikon CoolPix 9700). Cell viability was evaluated through laser-scanning confocal microscopy (Olympus IX81) after acridine orange/propidium iodide (AO/PI) staining. The stain was prepared by mixing equal volumes of 5 mg FDA/mL acetone with 750 μmol PI/L and freshly diluted 250×and 5×, respectively, in PBS. The 0.22-μm filtered AO/PI stain was added to the BMSC-seeded OPF–hydrogel for 15 min in the dark. Images were taken at a 490-nm excitation wavelength. The interaction between BMSCs and scaffold was also microscopically evaluated from hematoxylin & eosin-stained cross-sections.
Animal surgery
Six Prestige World Genetics micropigs (8 months old, skeletally mature, 20 kg, female) were used to investigate the in vivo ability of the rehydrated freeze-dried hydrogels to repair cartilage defects. All the protocols had been approved by the Institutional Animal Care and Use Committee at the NUS. The micropigs were anesthetized, and a medial parapatellar incision and arthrotomy were carried out on the right knee to expose the distal femur. Bicondylar osteochondral defects (n=12) (6-mm diameter, 1-mm depth) were created on the weight-bearing region of the lateral and medial condyles (n=6 each) with a 6-mm punch. The created chondral defects had a sharp edge, with a full cartilage layer and a thin subchondral bone layer removed (Fig. 2). An identical-sized BMSC-seeded rehydrated gel scaffold was press-fit into one of the two defects at random (opaque envelope method). The other defect in the same knee was implanted with an empty rehydrated gel scaffold for control. The scaffolds were kept in place by the close contact between the femoral condyle and meniscus. Wound closure was accomplished with bioabsorbable sutures. Animals were monitored until full recovery and allowed free movement in cages, with adequate analgesia. The animals were euthanized with barbiturate overdose at 4 months postoperatively. After euthanasia, defects on the lateral and medial condyles were photographed and processed for histologic analysis.
Histological analysis
The extent of cartilage repair at the osteochondral defect was determined by a histologic assessment. The 12 specimens from both the medial and lateral femoral condyles were fixed in 10% formalin, decalcified, and sectioned longitudinally from the middle part of the defect area into eight 5-μm-thick sections. Four stains were performed in duplicate: Masson's trichrome (collagen), toluidine blue (glycosaminoglycan [GAG]), and immunohistochemical staining for type I and II collagen. Qualitative analysis of the neotissue was based on the cell morphology and extracellular matrix content. Hyaline cartilage is characterized by the presence of rounded cells in the lacunae that express GAG and Type II collagen only. Fibrocartilage is defined by cells that produce GAG and Type I collagen only. Hybrid cartilage exhibits positive staining for both collagen types and GAG, while fibrous tissue is only positive for type I collagen. We calculated the percentage of tissue filling in specimens using grid superimposition over the tissue slide. Three observers (XR, ZY, CTL; mean Fleiss' kappa=0.72, 0.70, 0.65, respectively) evaluated the tissue-filling percentage and neotissue phenotype and assessed the neotissue based on the scoring system of Wakitani et al. 32 to evaluate cell morphology, matrix staining, surface regularity, cartilage thickness, and integration with adjacent host cartilage (score of 0–14 points, with the best-possible score being 0 and the worst 14) (Table 1).
Contents of the hyaline, fibrocartilage, mixed cartilage. and fibrous tissue were determined as a percentage of the total tissue located at defect area (mean±SD). The tissue below the original contour line of the subchondral bone was not included. Statistics by one-way ANOVA.
Statistical analysis
Values are expressed as mean±SD. We determined the differences in the repair cartilage phenotype and tissue-filling percentages between the scaffold–BMSC and scaffold groups and between the 2- and 4-month time points using one-way ANOVA (VassarStats; http://vassarstats.net/anova1u.html). Wakitani scores of samples (n=6) were compared using a one-tailed Mann–Whitney U test (http://elegans.som.vcu.edu/∼leon/stats/utest.cgi).
Results
The BMSC clusters could be visually observed as opaque specks in the rehydrated freeze-dried OPF scaffold (Fig. 1A). Under phase-contrast microscope (Fig. 1B), cell clusters could be clearly seen. The size of these clusters ranged from 28.5 to 298.4 (113.5±47.9) μm. Three-dimensional confocal micrograph revealed close contact between the BMSCs, seen to be viable from the green fluorescence in the AO/PI stain (Fig. 1C). Cross-sections of the scaffold–BMSCs (Fig. 1D) revealed that the cells were distributed in the spaces between the scaffold walls and formed tissue-like structure. The cells that were adhered to the scaffold possessed an enlarged nucleus (arrowheads), which indicated that the cells were viable and were undergoing proliferation.

Gross morphological (Fig. 2) findings showed that the defects implanted with the scaffold and MSCs were covered with more white-colored tissue, and the concave grooves observed in the central portion of defects in the scaffold-alone group were not present when MSCs were included in the implanted scaffold. Histological observations (Fig. 3) revealed that the defect in the scaffold group (Fig. 3A) was 54% filled with newly formed tissue, while scaffold–BMSC treatment (Fig. 3B) led to a significantly increased, almost complete repair, at 99% with 7% outgrowth (Table 1). The repair tissue was observed to extend beyond the original cartilage contour line, and this value was found to be significant compared to the absence of outgrowth in the scaffold group. In the scaffold group, the predominant tissue was hyaline cartilage (39%), followed by hybrid cartilage (29%) and an equal amount of fibrocartilage and fibrous tissue. The pattern was similarly observed in the scaffold–BMSC group, with a much greater percentage of neotissue occupied by hyaline (84%), followed by hybrid cartilage (13%). The neotissue was seamlessly integrated with host cartilage and bone at the vertical and horizontal defect edges, respectively (Fig. 3). The junction between repair and original cartilage (OC) was hypocellular (Fig. 4, arrows).

Representative gross morphology of the chondral defects from the scaffold group

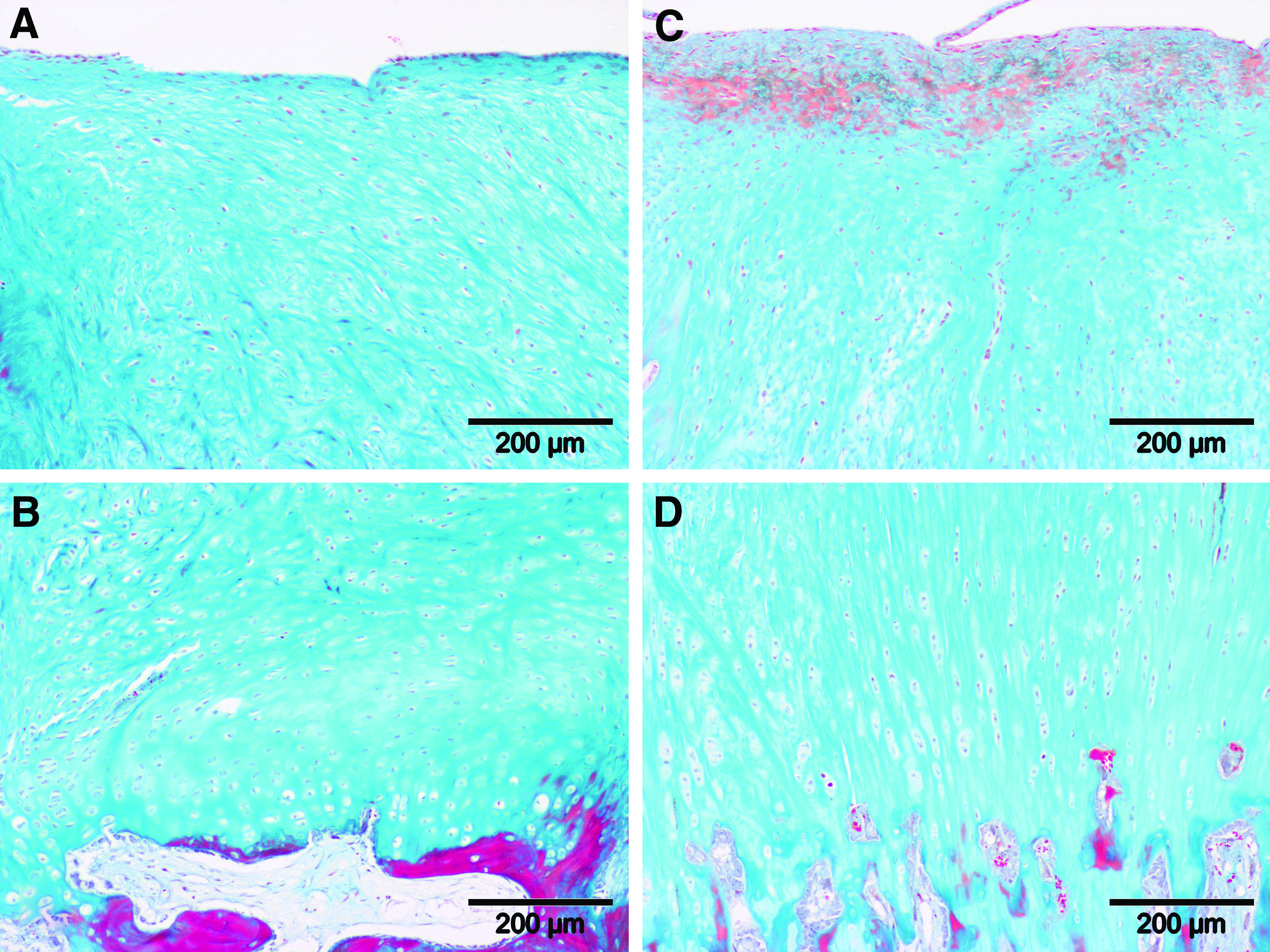
Representative microscopic images of samples in the scaffold and scaffold–BMSC groups at 4 months postoperatively are shown:
Representative microscopic images of a sample in the scaffold–BMSC group are shown:
Loss of subchondral bone native structure was noted in both groups (Fig. 3). In the scaffold group (Fig. 3A), the degeneration extended deeper into the subchondral bone compared to the scaffold–BMSC group (Fig. 3B). Trace amounts of undegraded scaffold could only be observed at the bottom part of the degenerated subchondral bone in the scaffold group (Fig. 3A).
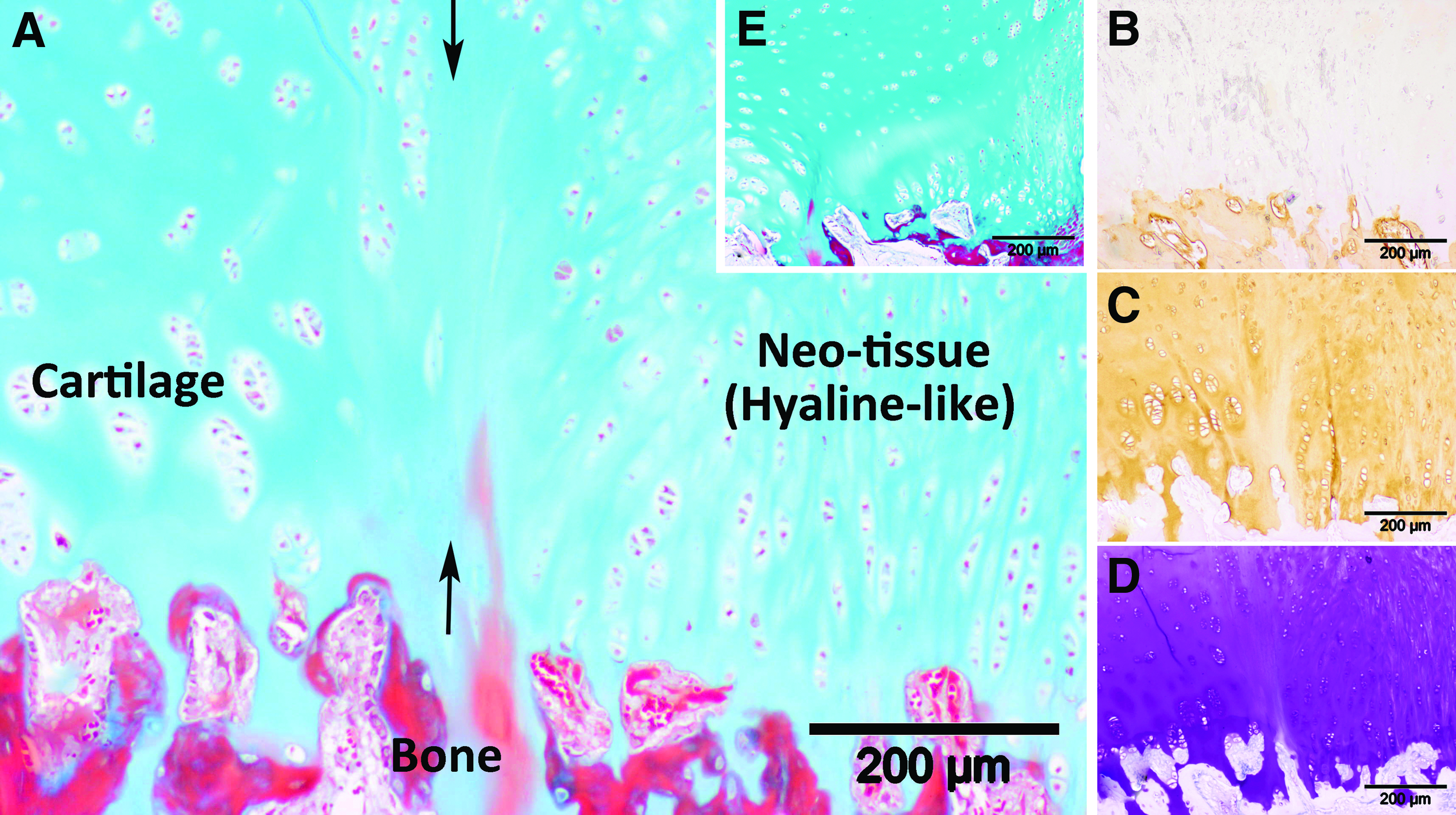
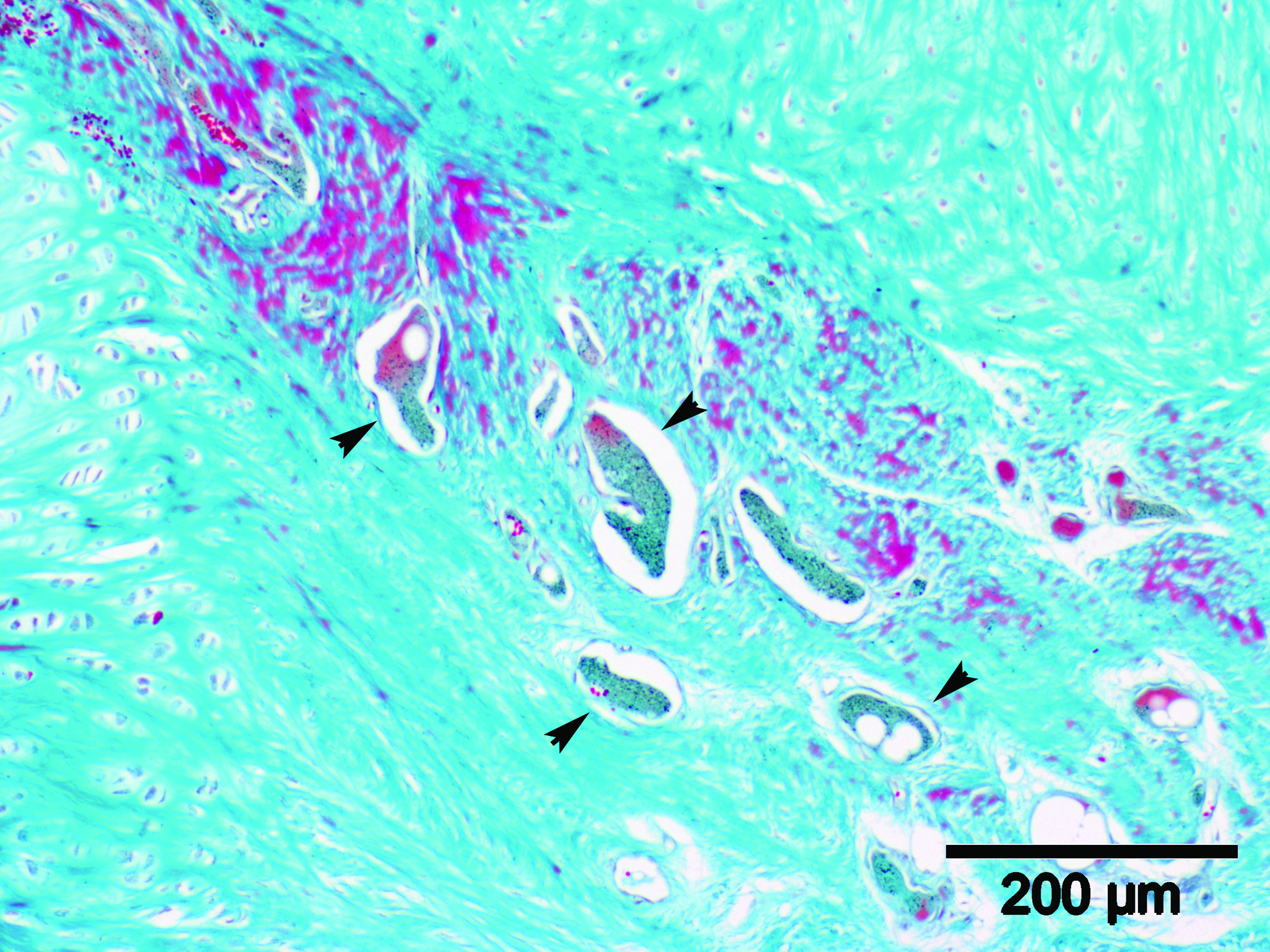
Histological analysis of the repaired defects in the scaffold–BMSC group showed that the interterritorial matrix was not uniform compared to the host cartilage (Fig. 4). High-magnification photomicrographs provided a clear image of the distribution of three distinct tissue zones in the scaffold–BMSC group, two of which were also present in the scaffold-alone group. The orientation of the collagen fibrils (Figs. 4 and 5A–D) from the bottom (near subchondral bone) to the top-central region of the neotissue was found to differ. Those found in the radial zone were oriented perpendicularly to the cartilage surface, with embedded round chondrocytes similarly arranged in columns (Figs. 4, and 5B, D). The collagen fibrils were parallel to the cartilage surface at the thin tangential zone, with small fibroblast-looking cells (Fig. 5A, C). Fibrils located in the transitional zone were arranged in a random wave-like manner with characteristics intermediate between both the tangential and radial zones, and were occupied by rounded chondrocytes. Histological staining revealed that the radial zone was hyaline, as it was negative for type I collagen and positive for GAG and type II collagen (Fig. 4). The tangential zone consisted of type I collagen-positive fibrous tissue. The transitional zone is made up of hybrid cartilage, deducible from the presence of GAG and both collagen types, and was noticeably absent from the scaffold group. The vertical length of the radial zone in the scaffold group was shorter and directly connected to the enlarged tangential zone, relative to the scaffold–BMSC group (Fig. 5B). Conversely, the radial and transitional zones formed the dominant portion of the neotissue in the scaffold–BMSC group. The repair tissue found at the bottom part of the defect in the scaffold-only group was fibrous and acellular (Fig. 6), but MSC supplementation led to the formation of fibrocartilaginous repair tissue, rich in cells and extracellular matrix (Fig. 7). Tiny pieces of undegraded scaffold fragments could only be seen in the radial zone of the scaffold group (Fig. 8)
Representative microscopic images of a sample from the
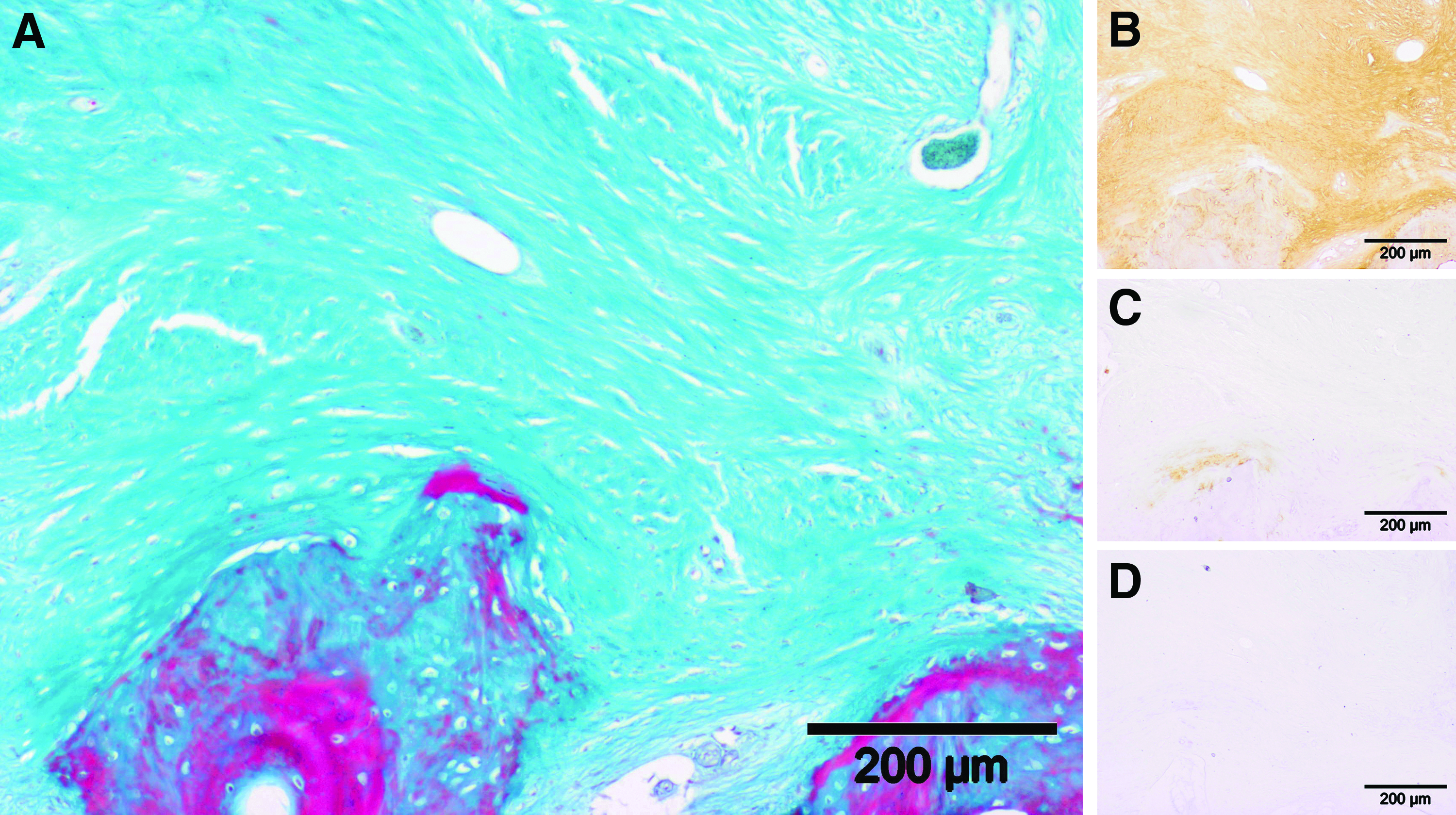
Representative microscopic images of a sample from the scaffold group are shown:
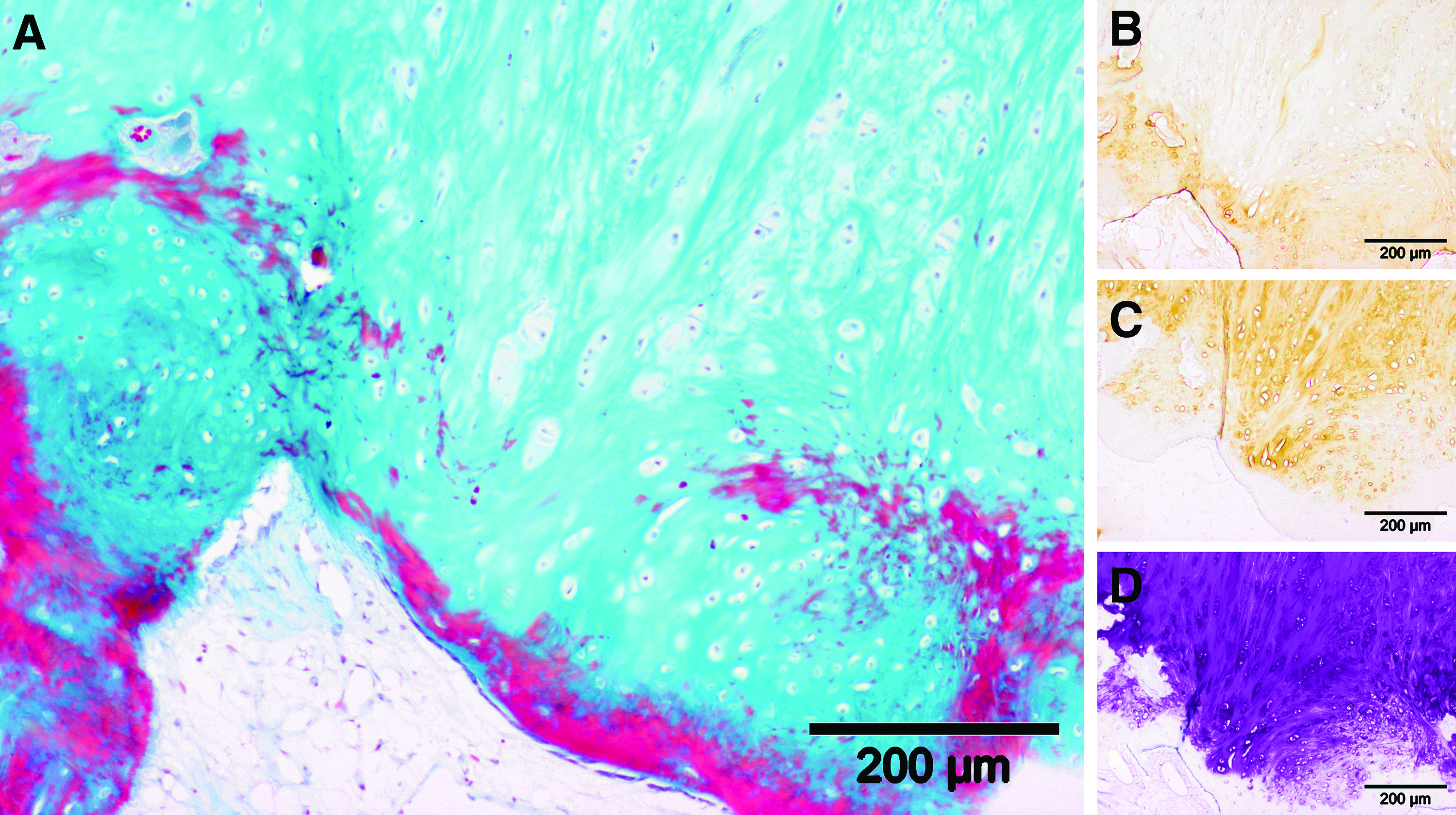
Representative high-magnification microscopic images of a sample from the scaffold–BMSC group are shown:
The micromorphology of the neotissue in the central region of the degenerated subchondral bone in the scaffold group is shown. Arrowheads indicate the location of the remaining scaffold debris (stain, Masson's trichrome; original magnification ×100). Color images available online at www.liebertpub.com/tea
One-way ANOVA analysis (Table 2) showed that the neotissue-filling percentage in the scaffold–BMSC group was significantly more than the scaffold group (p<0.0001). The percentage of hyaline neotissue in the scaffold–BMSC group was also significantly greater than that achieved in the scaffold group (p<0.0001). The Wakitani score (Table 2) of the repaired defects in the scaffold–BMSC group was significantly lower (1.83) than the scaffold-only group (4.83), as analyzed through one-tailed Mann–Whitney U test (p=0.02).
Five individual parameters were listed according to the Wakitani grading scale. All values were given as the mean and standard deviation for each parameter. Statistical differences were determined by one-tailed Mann–Whitney U tests.
BMSCs, bone marrow-derived mesenchymal stem cells.
Discussion
Since the advent of ACI, new therapies for osteochondral injuries have been continuously explored. While proposed new therapies have demonstrated promising results, very few have been translated into clinical practice.9,33,34 There is high demand for an effective therapy for osteochondral injuries, which commonly afflicts the young athletic population. In this study, we evaluated the in vivo ability of BMSC-seeded OPF hydrogel as a treatment for osteochondral defects. The cross-linked PEG-based hydrogel can generate osmotic pressure, which is beneficial to host cells,24,25 and had been well-tested with BMSCs in vitro27,28 and in the rabbit model. 9 However, the results from rabbits are not clinically relevant due to physiological differences in anatomy and repair mechanisms, compared to humans.
While the pluripotency of stem cells hallmark the potential in tissue engineering repair and regeneration techniques, biomaterials play a similar pivotal role in ensuring the success of these techniques. OPF–hydrogel scaffolds have been extensively studied in rabbits, but as rabbits have a strong inherent ability for osteochondral-defect healing, it is difficult to evaluate the treatment effect. Based on complete cartilage repair seen in the rabbit model, 9 we selected OPF hydrogel–BMSCs for a porcine translational study. The relatively larger size of pigs' joints and thicker cartilage allow the creation of full-thickness cartilage defects of 6 to 8 mm in diameter, making pigs' joints ideal for studying the potential effect of treatment modalities. It is important to note however that the skeletally mature minipigs might not be comparable to humans' chronological age and the minipig MSCs could be more robust. We have demonstrated the OPF scaffold's biocompatibility in the porcine model and reported its sequential degradation. 12 Four months was observed to be the optimal time point for evaluations due to the complete clearing of the scaffold debris, minimal inflammation, and lack of innate cartilage regeneration observed at that stage.
In embryonic development, chondrogenesis is triggered from MSC condensation. In in-vitro experiments, attempts have been made to replicate this naturally occurring event by culturing cells in three-dimensional forms such as pellet culture and porous scaffold35,36 to induce the differentiation of stem cells into chondrocytes and subsequently form cartilage-like tissue. Condensation was shown to enhance the chondrogenic potential of MSCs, seen in the increased production of the extracellular matrix rich in type II collagen and proteoglycans. 37 A traditional approach in seeding the hydrogel with MSCs involved the thorough mixing of the hydrogel scaffold components with stem cells before fabrication into the solid form,9,28,29 which would result in segregated MSC clumps. To achieve compact cellular condensation in the OPF hydrogel scaffold, the hydrogel was first freeze-dried. The freeze-dried process turned the transparent OPF hydrogel into a porous sponge-like scaffold. The pores ranged from 20 to 433 μm in diameter (136±86 μm), 12 and seeded cells were observed to form aggregated clusters. The rehydration step caused the scaffold to swell up with water, and we hypothesize that it reduced the available surface area for cells, led to close contact between cells, and thus formed a compact environment (Fig. 1). The process of freeze-drying and rehydration did not affect the scaffold's compressive stiffness, 12 and benefited the stem cell chondrogenic differentiation. Findings of cell clustering had been observed in chondroitin sulfate (CS)-PEG hydrogel and collagen I hydrogel.38,39 Comparing against the results of Varghese et al., our OPF hydrogel could attain the same cellular condensation without the addition of CS, perhaps due to the equally hydrophilic property of the OPF hydrogel, which mimics the naturally occurring extracellular matrix.
In contrast to a prior rabbit model study that reported the formation of zonally organized hyaline-like cartilage and bone formation in the subchondral region through the use of OPF scaffold only, 9 we found that the OPF scaffold alone was not sufficient for osteochondral defect regeneration in the porcine model (Fig. 3A). However, augmentation with BMSCs led to an increased defect-filling ratio of 98% (Fig. 3B and Table 2). Hyaline-like cartilage accounted for more than 83% of the neotissue in the defect site (Table 2), which is an improvement over other similar-reported studies in large-animal models.33,34 The additional presence of a transitional zone in the repair cartilage obtained after MSC inclusion could prove to be favorable, as collagen fibers provide resistance against both shearing and compressive forces, thus supporting the roles of the tangential and radial zones. The zonal arrangement observed in the repair cartilage bore a strong resemblance to native articular cartilage. These mirror the results obtained from the BMSC-seeded OPF hydrogel scaffold in the rabbit model 9 and thus provides a strong supporting evidence for its cartilage repair. Seeding BMSCs after OPF hydrogel scaffold fabrication instead of during scaffold fabrication enabled cellular condensation to occur and could be a contributing factor to the formation of the zonal arrangement, as enhanced matrix deposition that could stimulate cartilage remodeling had been reported in constructs seeded with microaggregates compared to single dissociated cells. 40
The presence of hyaline tissue indicates differentiation, but it could have been preceded by cell proliferation, as tissue repair outgrowth was observed. The concurrent proliferation and differentiation were also noted in MSCs seeded into a nanofibrous scaffold. 41 Despite the lack of discussion in the literature regarding outgrowth, we noticed that the repair cartilage in Wakitani et al.'s rabbit study 32 after MSC treatment extended beyond the original contour line for up to 24 weeks. The inclusion of cartilage outgrowth measurement in Nagai et al.'s cartilage repair classification 42 also reflects that outgrowth is not a novel finding. Biomechanical data would be needed to review if the presence of outgrowth compromises the knee-loading efficiency, including a longer time point to check if it would level down to the original cartilage contour line. MSC proliferation could be arrested through predifferentiation into chondrocytes before implantation, and studies have reported better cartilage repair compared to undifferentiated MSCs and chondrocytes.33,43 However, the reverse have also been reported, whereby undifferentiated MSCs led to the formation of cartilage repair tissue that scored better than TGFβ-induced differentiated MSCs. 44
Seamless integration of the host tissue and neotissue was observed in both groups, but was only hypocellular in the scaffold-only group (Fig. 5A, B). This distinct difference suggests that the implanted cells had populated the host repair tissue-integrated site, or possibly enhanced the host MSCs' cartilage repair response. A labeling study that involved the intra-articular injections of 3 H-thymidine revealed its take-up by undifferentiated mesenchymal cells, and progressive appearance in fibroblasts, osteoblasts, articular chondroblasts, and chondrocytes, thus indicating their origin from the MSCS. 45 However, the findings that bone marrow loading accelerated the first stages of repair in a hyaluronan scaffold 46 and synovial-derived MSCs secreted trophic factors that enhanced cartilage repair rather than directly differentiating into chondrocytes 47 lend support to the theory that MSCs may facilitate tissue repair by improving the microenvironment through the release of growth factors, in addition to cell replacement. 48
The depth of degenerated subchondral bone was less in the scaffold–BMSC group (Fig. 3) and could be due to two possible factors: one, subchondral bone reconstruction could have occurred after MSC implantation, but was incomplete, as MSCs have the potential to differentiate into bone and cartilage under appropriate stimuli. A longer postoperative time could be required for repair tissue remodeling. The formation of bone had been suggested to require a synergized effort between both host and implanted cells. 49 Future studies could investigate the stimuli compatible with the construct and the surrounding host tissue, to encourage more robust subchondral bone regeneration within a short time frame. Two, less-extensive subchondral bone damage due to accelerated scaffold degradation could be another possibility. The rate of scaffold breakdown was noted to be increased upon administration of MSCs and could be cell mediated, as polymerase chain reaction studies had highlighted increased enzymatic expression levels of lysozyme and hyaluronidase upon the presence of scaffold. 50 It could be a natural response by MSCs to infiltrate into the defect and affect repair, as the rapid scaffold degradation of the dextran hydrogel scaffolds enabled increased filtration of angiogenic cells into healing wounds. 51 Scaffolds present a stable physiologic environment for cells, which is necessary for tissue formation. However, its degradation is equally important, as it has been shown to elevate the collagen content and dynamic compressive modulus in engineered articular cartilage. 52 Statistical analyses in this study clearly showed seeding BMSCs in the OPF scaffold before implantation significantly enhanced both the percentage of tissue filling and hyaline cartilage formation.
Further studies are necessary to identify the factors contributing to subchondral bone degeneration. First, a longer time point would be needed to analyze the long-term repair, as although repair and host tissue may be fused initially, the formation of fissures have been reported in repair tissues. 45 Secondly, biomechanical assessment of the repair tissue's load deformation behaviour would be required to gauge its tensile strength. However, as the aim of this project was to analyze the short-term 4-month repair of a small sample size, we were unable to assess both. However, we were able to determine histologically that hyaline cartilage, known to be biomechanically strong, was formed, and that despite the high compressive loading in the porcine model that could propagate fissures, 53 the scaffold–BMSC group achieved a smooth articulating exterior. This is a significant outcome as the porcine joint simulates the biomechanical rigors experienced in the human joints. 54 Thirdly, we cannot conclude if the cell number seeded is optimal for repair, as the amount was determined from our own groups' cartilage experience. Further studies would be required in this aspect. Lastly, the contribution of the seeded MSCs was not conclusive due to lack of cell labeling, but was deducible through comparison against the scaffold-only group.
We have demonstrated that the BMSC-seeded OPF scaffold enhanced the in vivo regeneration of articular cartilage, but not the subchondral bone formation. This study has provided a strong basis for the bench-to-bedside application of this polymer in osteochondral joint defects.
Footnotes
Acknowledgment
We thank the National Medical Research Council (Singapore, Ministry of Health) for the funding given to this project (NMRC-1142-2007).
Disclosure Statement
No competing financial interests exist