
Abstract
Objective:
This study aimed to investigate the regenerative capacity of chondrocytes derived from debrided defect cartilage and healthy cartilage from different regions in the joint to determine the best cell source for regenerative cartilage therapies.
Methods:
Articular cartilage was obtained from Outerbridge grade III and IV cartilage lesions and from macroscopically healthy weight-bearing and nonweight-bearing (NWB) locations in the knee. Chondrocytes isolated from all locations were either pelleted directly (P0 pellets) or after expansion (P2 pellets) and analyzed for glycosaminoglycan (GAG), DNA, and cartilage-specific gene expression. Harvested cartilage samples and cultured pellets were also analyzed by Safranin O histology and immunohistochemistry for collagen I, II, and X. Immunohistochemical stainings were quantified using a computerized pixel-intensity staining segmentation method.
Results:
After 4 weeks of culture, the P0 pellets derived from grade III or healthy weight-bearing chondrocytes contained more (p<0.015) GAG and GAG normalized per DNA compared to those from grade IV and NWB locations. After expansion, these differences were lost. Cartilage-specific gene expression was higher (p<0.04) in P0 pellets from grade III chondrocytes compared to grade IV chondrocytes. Semiquantitative immunohistochemistry showed a more intense (p<0.033) collagen I and X staining for grade IV debrided cartilage compared to grade III and weight-bearing cartilage. Also, collagen type X staining intensity was higher (p<0.033) in NWB cartilage compared to grade III and weight-bearing regions.
Conclusion:
Chondrocytes derived from debrided cartilage perform better than cells from the NWB biopsy site, however, this difference is lost upon expansion. Based thereon, the debrided defect cartilage could be a viable donor site for regenerative cartilage surgery.
Introduction
A
Several treatment modalities for focal cartilage defects are based on the use of autologous tissue or cells from areas in the affected joint that are not exposed to mechanical loading. The development and maturation of articular cartilage is directed by the influence of mechanical loading,5,6 where physiological loading steers the metabolic activity of articular chondrocytes leading to a resistance of the cartilage to the loading patterns it is exposed to.7,8 For this reason, adult articular cartilage has distinct biochemical and biomechanical characteristics based on the differences in topographical loading within the joint.9,10 In human cadaveric studies, articular cartilage in nonweight-bearing (NWB) areas showed signs of chondropenia as reflected by a reduction in proteoglycan staining11,12 in an overall macroscopically healthy joint.13,14 In addition, by mathematical modeling, already in the late 1990s, chondropenic conditions in NWB areas in the joint were suggested. 15
Autologous chondrocyte implantation (ACI) is a widely used technique for the treatment of focal articular cartilage lesions in the knee. During a first arthroscopic procedure, a small cartilage biopsy is taken from the NWB lateral margin of the trochlea. From this biopsy, chondrocytes are isolated and expanded until enough cells are available for reimplantation. 16 During a second surgical procedure, remnants of articular cartilage in the lesion are debrided, to create a clear surgical defect with stable base and rim, before the expanded cells are reimplanted. Despite recent advances in ACI, including the introduction of matrices as carriers for the cells, clinical results are still not always optimal. Moreover, the induced damage during biopsy could also have a negative impact on the joint homeostasis and thereby on the function of reimplanted cells and clinical outcome after ACI. Instead of a cartilage biopsy, the debrided defect cartilage could also be used as donor tissue for ACI. Chondrocytes from debrided cartilage already showed to be capable of redifferentiation in various in vitro culture models and their gene expression was found to be similar to that of healthy chondrocytes.17–19 Although these studies demonstrated the regenerative capacity of the chondrocytes from debrided defect cartilage, no distinction was made between defect grades and no comparison was made with chondrocytes derived from the regular harvest location. The fibrous cartilage in Outerbridge grade IV is likely to harbor chondrocytes that are phenotypically different from the cells isolated from the macroscopically intact remnant cartilage matrix around Outerbridge grade III lesions, 20 with possible implications for their use in ACI.
Therefore, the aim of the current study was to determine the regenerative capacity of chondrocytes from different types of focal cartilage lesions in combination with a re-evaluation of the suitability of cartilage from NWB locations in the knee thereby providing valuable additional information on the feasibility of debrided defect cartilage as a possible donor site in ACI.
Materials and Methods
Patient characteristics
All use of patient material in this study was approved by the institutional ethics committee. Macroscopically healthy articular cartilage was, under sterile conditions and within 24 h of postmortem, harvested from full-weight- and nonweight-bearing locations of the knees of five different donors during autopsy at the Department of Pathology. NWB cartilage was obtained from the lateral margin of the trochlea and full-weight-bearing (FWB) cartilage from the weight-bearing femoral condyles.
A total of 20 samples of debrided tissue from focal lesions in 20 patients during microfracture or ACI surgery were obtained from March 2009 to April 2010 at the Department of Orthopedics. Among the 20 samples of debrided cartilage, 12 were classified as Outerbridge grade III and 8 were classified as grade IV. 20
Isolation and culture of chondrocytes
Cartilage samples were rinsed in phosphate-buffered saline (PBS), diced into small pieces, and digested overnight at 37°C in a 0.15% collagenase type II solution (Worthington) in the Dulbecco's modified Eagle's medium (DMEM; Gibco) with penicillin/streptomycin (100 U/100 μg; Invitrogen). After enzymatic digestion, the cell suspension was filtered through a 70-μm cell strainer (BD Biosciences) and washed in PBS. Isolated chondrocytes were counted and viability was assessed in Trypan Blue (Sigma-Aldrich) using a Burker-Turk hemocytometer. A total of 1.5×106 isolated chondrocytes were pelleted, by a 10-min centrifugation (P0 pellets) at 300 g, at 250,000 cells/pellet. The remaining chondrocytes were expanded in culture flasks at a seeding density of 5000 chondrocytes/cm2. After expansion, the population doublings per day were calculated based on the initially seeded P0 cells and their final number at passage 1. At passage 2, the expanded chondrocytes were pelleted (P2 pellets) by centrifugation, also at 250,000 cells/pellet. All pellets were cultured for 4 weeks in the DMEM (Invitrogen), 0.2 mM
Biochemical analysis
After 4 weeks of culture, the pellets were digested overnight in the papain buffer (250 μg/mL papain; Sigma-Aldrich, in 50 mM EDTA and 5 mM
The DNA content per pellet was determined from the papain digest using a picogreen DNA assay (Invitrogen) in accordance with the manufacturer's instructions.
Histological and immunohistochemical analysis
Histological and immunohistochemical staining was performed on NWB, FWB, debrided grade III and grade IV cartilage tissue, and on P0 and P2 pellets cultured from cells from the above-mentioned locations. Also, an additional CBFA1 staining was performed on the tissue sections of the NWB, FWB, debrided grade III and grade IV samples.
Explants and pellets were fixed in 10% buffered formalin, dehydrated in alcohol, rinsed in xylene, and infiltrated and embedded with paraffin. For histology, 5-μm sections were stained with Safranin O (Merck) for GAG and counterstained with Weigert's hematoxylin (Klinipath) and 0.4% fast green (Merck) for nuclei and cytoplasm, respectively.
Immunohistochemistry for collagen I, II, and X and CBFA1 was also performed on 5-μm sections. Antigen retrieval steps, 30 min pronase (1 mg/mL in PBS; Roche) followed by 30 min hyaluronidase (10 mg/mL in PBS at 37°C; Sigma-Aldrich), were performed for both the collagen type I and II staining. For collagen type X staining, antigen retrieval was performed by a 2-h pepsin (1 mg/mL in 0.1 N HCl; Sigma-Aldrich) step at 37°C followed by hyaluronidase incubation (10 mg/mL in PBS; Sigma-Aldrich) for 30 min at 37°C. For the CBFA1 staining, antigen retrieval was performed using the citrate buffer for 1 h at 80°C. After antigen retrieval, the sections were blocked using a PBS-bovine serum albumin (BSA) 5% solution for 30 min followed by overnight incubation at 4°C with the primary antibodies against human collagen type I (20 μg/mL in 5% PBS/BSA; Merck), collagen type II (1/100 in 5% PBS/BSA; DSHB), collagen type X, clone 53 (1/20 in 5% PBS/BSA; Quartett), and CBFA1, sc-101145 (mouse monoclonal, 1/20 in 5% TBS/BSA; Santa Cruz). For CBFA1, the samples were incubated with the RUNX2 (27-K) antibody during 1 h at 37°C. For collagen type I and collagen type X and CBFA1, a biotinylated secondary anti-mouse antibody was used (1/200 in 5% PBS/BSA for Col I and X; GE Healthcare, RPN1001V, 1/200 in TBS/BSA 5% for CBFA1; GE Healthcare) for 1 h at RT, followed by incubation with streptavidin/peroxidase (1/500 in 5% PBS/BSA; Beckman Coulter) 1 h at RT. The collagen type II primary antibody was followed by a secondary anti-mouse antibody conjugated with peroxidase (10 μg/mL, 1 h at RT; Dako). Antibody binding was visualized using 3-diaminobenzidine (DAB; Sigma-Aldrich). All immunohistochemical sections were counterstained using Mayer's hematoxylin.
Immunohistochemical staining segmentation
Immunohistochemical staining for collagen type I, II, and X was semiquantitatively analyzed using pixel intensity staining segmentation (Positive Pixel Count algorithm in ImageScope v8.0; Aperio Technologies). Pixels were identified as positive or negative based on user-defined settings using reference sections. The RGB code for positive staining was extracted from the average RGB settings (R: 0.15, G: 0.58, B: 0.78) in 15 different randomly selected positively stained region-of-interests (ROIs) from 10 different samples. The intensity of positive staining was subcategorized into weak, moderate, or strong based on the positive pixel count algorithm settings. These settings were further optimized by testing for false-positive or false-negative pixels in a set of 30 additional ROIs at 20 sections, which were stained during the same run. Following this, the optimized algorithm was applied to two serial sections taken from the middle of all donor samples. Per section, the whole field or section was analyzed. This resulted in a color-based staining intensity picture (Fig. 1) and a semiquantitative determination of the percentage of weak, moderate, and strongly stained pixels for the different sections. Percentage of positive staining was defined as the sum of weak-, moderate-, and strong-positive stain.
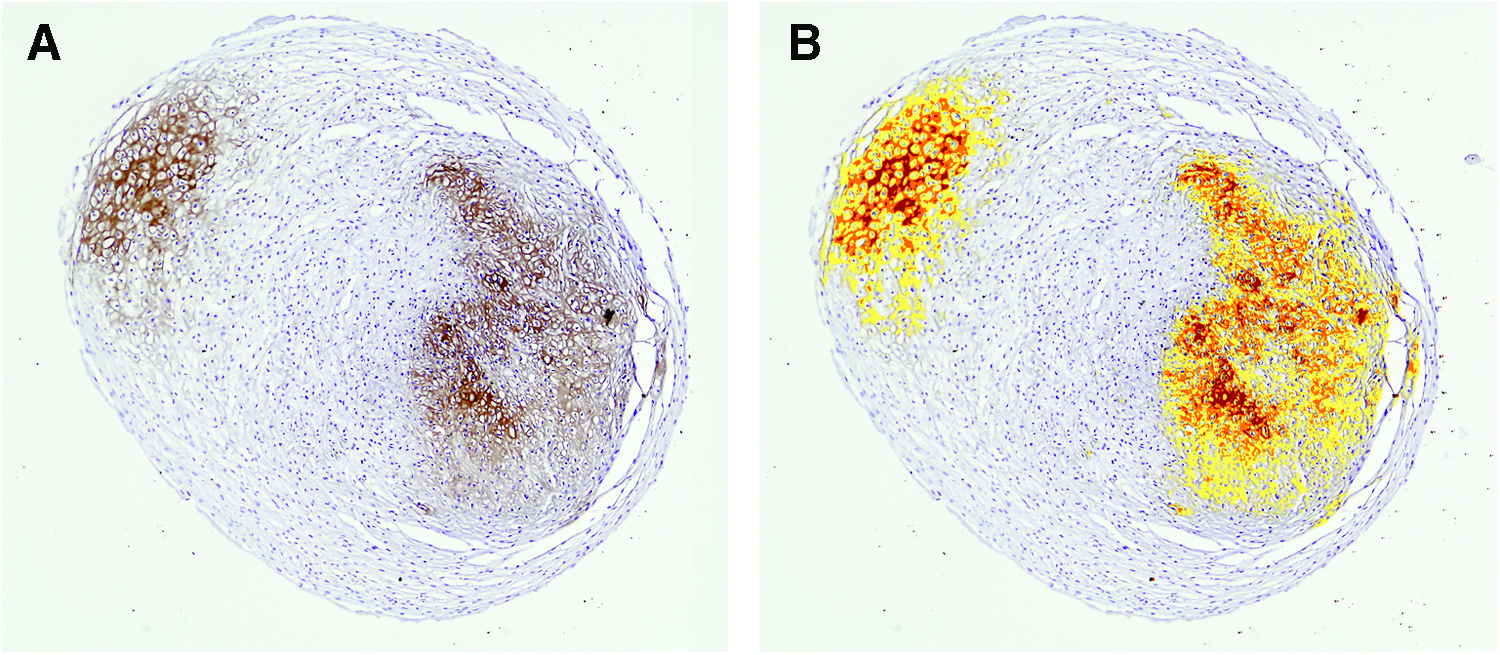
Immunohistochemical staining segmentation. A color-based staining intensity output with the staining intensity on the original picture
Gene expression analysis
To further characterize the isolated chondrocytes from grade III and IV debrided defect cartilage, PCR was performed directly after isolation and after 4 weeks of pellet culture at P0. Gene expression analysis was performed as previously described. 22 All expression levels were normalized to GAPDH expression. A set of five genes was selected based on their functional role in cartilage biology.22,23 Aggrecan (ACAN), cartilage link (HAPLN1), and collagen type II (COL2A1) gene expression were defined as positive markers of chondrocyte biology, whereas microfibrillar associated protein 5 (MFAP5) and collagen type I (COL1A1) were related to a more fibrocartilaginous phenotype. 23 In addition, the identity index, postulated previously to be positively correlated to the chondrogenic phenotype, 23 was calculated by extracting MFAP5 expression from HAPLN1 expression.
Statistical analysis
All statistical analysis was performed using SPSS version 15.0. The statistical analysis of the GAG and GAG per DNA and the immunohistochemical staining segmentation analysis were performed using a one-way ANOVA with the post hoc Bonferroni test to test for differences in the performance of cells from different regions. The differences in gene expression between grade III and grade IV cells and pellets were analyzed by a one-way ANOVA followed by an independent Student's t-test. A p-value of p<0.05 was considered statistically significant.
Results
Cell viability and proliferation
The weight of the debrided cartilage ranged from 0.447 to 1.551 g and yielded 0.96–3.1×106 chondrocytes after overnight isolation (Table 1). The percentage of dead cells after overnight isolation was higher (p<0.001) in grade IV tissue compared to grade III, NWB and FWB locations (Table 1). In addition, the total number of cells per gram cartilage was statistically significantly lower (p<0.05) for the grade IV debrided cartilage when compared to grade III, NWB and FWB cartilage samples (Table 1). The capacity of the freshly isolated P0 cells to expand in culture flasks, as expressed by the population doublings per day, did not show a statistically significant difference (p>0.107) between the grade IV, grade III, NWB and FWB cells (Table 1).
FWB, full-weight bearing; NWB, nonweight bearing.
DNA content
After 4 weeks of culture, the total amount of DNA did not differ for the P0 (p>0.076) nor the P2 (p>0.217) pellets between the grade III (P0: 1.06±0.49 μg, P2: 0.67±0.0.32 μg), grade IV (P0: 1.00±0.68 μg, P2: 0.41±0.21 μg), NWB (P0: 0.79±0.02 μg, P2: 0.84±0.36 μg), and FWB (P0: 1.12±0.64 μg, P2: 0.80±0.12 μg) samples.
GAG content
The ability of chondrocytes to produce GAG in culture, expressed by the GAG content normalized by DNA showed more efficient GAG production per cell (p<0.001) in P0 pellets from grade III (46.76±16.41 μg GAG/μg DNA) and FWB chondrocytes (39.55±7.64 μg GAG/μg DNA) compared to grade IV (11.54±9.71 μg GAG/μg DNA) and NWB pellets (16.54±4.95 μg GAG/μg DNA) (Fig. 2). After expansion, no differences (p>0.105) were observed in the GAG/DNA and GAG content between the different biopsy sites (Fig. 2).
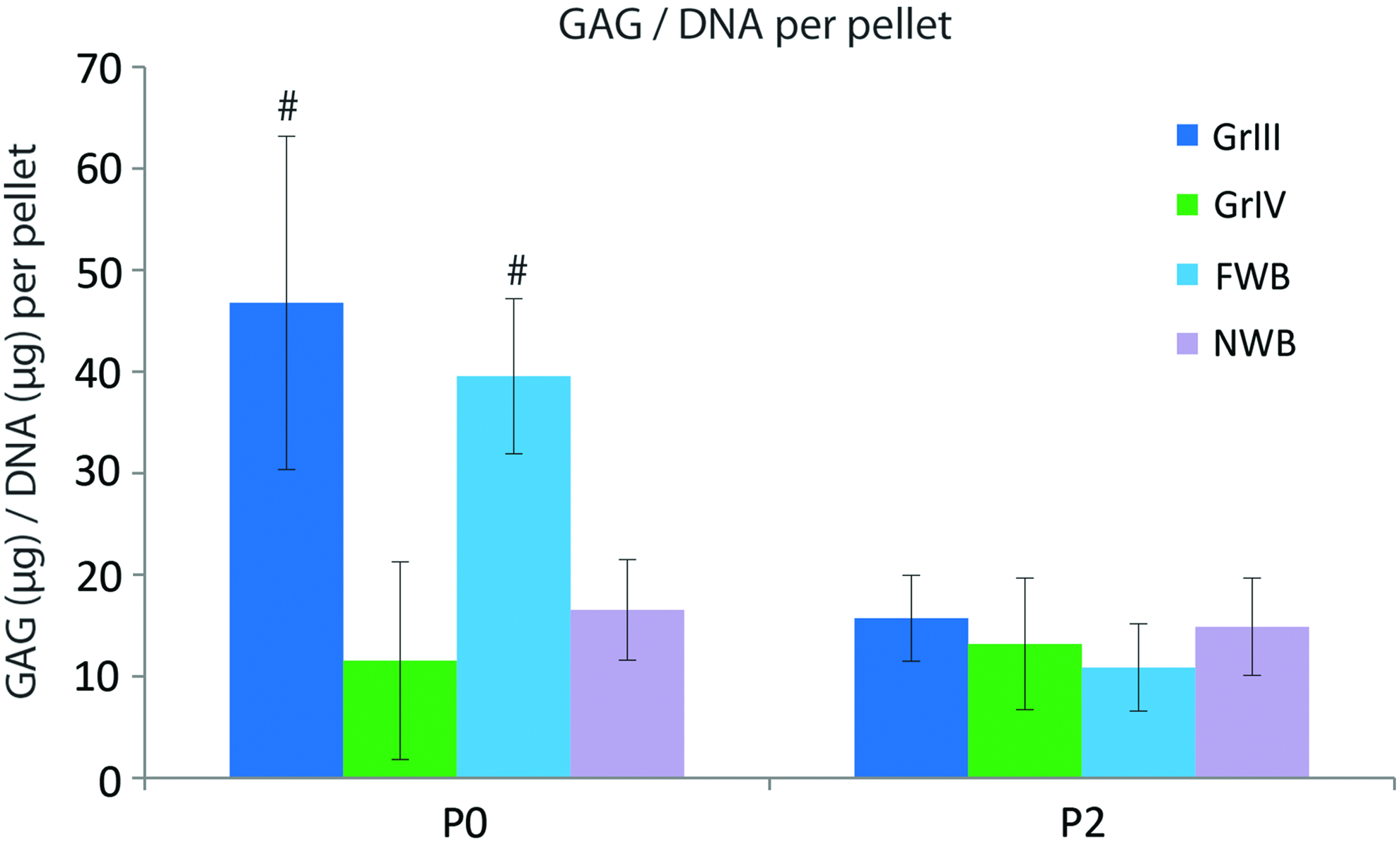
Glycosaminoglycan (GAG) content per DNA of P0 and P2 pellets at different biopsy sites. P0 pellets derived from grade III and full-weight-bearing (FWB) chondrocytes produce more GAG/DNA compared to P0 pellets from grade IV and nonweight-bearing (NWB) chondrocytes (#p<0.002). Color images available online at www.liebertpub.com/tea
Absolute GAG production per pellet was higher (p<0.015) in pellets from grade III (46.45±19.73 μg/pellet) and FWB (31.19±9.57 μg/pellet) chondrocytes compared to pellets from grade IV (9.89±5.04 μg/pellet) and NWB (17.99±11.90 μg/pellet) chondrocytes (Fig. 2).
Histological and immunohistochemical staining analysis
Light microscopy of Safranin O-stained tissue sections showed a less intense staining for GAGs for grade IV tissue sections compared to grade III, NWB and FWB tissue. In accordance with the biochemical data, the staining for GAGs in P0 pellets from grade III and FWB chondrocytes appeared more intense compared to the grade IV and NWB P0 chondrocyte pellets. No or only slightly positive Safranin O staining was observed for the regenerated cartilage of the P2 pellets.
Collagen type II staining was strongly positive in grade III, FWB and NWB tissue sections. From light microscopy and semiquantitative analysis, staining of grade IV tissue sections for collagen type II was less positive (p<0.05) compared to the other tissue sections (Figs. 3 and 4). P0 pellets for all the cartilage samples showed a strongly positive collagen type II staining (Fig. 3). Staining of the P2 grade IV and NWB pellets appeared less positive (Fig. 3) compared to the grade III and FWB P2 pellets, however, did not reach statistically significant differences at staining analysis (Figs. 3 and 4).

Histological and immunohistochemical staining. A characteristic decrease in Safranin O and increase in collagen I staining in P2 pellets compared to tissue sections are noted for all the samples from different locations. Tissue sections from grade IV (Gr IV) defect cartilage show a less intense Safranin O and collagen type II staining compared to grade III (Gr III) and FWB tissue sections. Also, collagen type X staining is more pronounced in grade IV and NWB cartilage when compared to grade III and FWB tissue sections. The scale bar at the right bottom represents 100 μm and reflects the magnification of all images within the figure. Color images available online at www.liebertpub.com/tea

Immunoquantification. Quantification of immunohistochemical staining (collagen I, II, and X) for grade III (Gr III), grade IV (Gr IV), NWB and FWB tissue sections and pellet cultures. Tissue sections (*p<0.001) and P0 pellet cultures (#p<0.015) from grade IV chondrocytes show more collagen type I staining compared to tissue sections and P0 pellets from grade III, full-weight- and nonweight-bearing samples. Also, collagen type II staining intensity is lower (§p<0.05) in grade IV tissue sections compared to the other locations. Collagen type X staining in NWB and grade IV tissue sections is higher (+p<0.033) compared to FWB and grade III tissue sections. For grade IV P0 pellets, the collagen type X expression is also higher (xp<0.025) in P0 pellets compared to the other locations. Color images available online at www.liebertpub.com/tea
Collagen type I staining was strongly positive for grade IV tissue and slightly positive for the P0 pellets, whereas for all the other biopsy sites collagen type I staining was negative for tissue and P0 pellets (Fig. 3). Semiquantitative analysis confirmed that the percentage of positive collagen type I staining was significantly higher for grade IV tissue compared to the other tissue samples (p<0.001) and grade IV P0 pellets versus the pellets derived from the other locations (p<0.015), respectively (Fig. 4). Collagen type I staining for the P2 pellets was positive in all samples, regardless of tissue origin.
Collagen type X staining was negative for tissue and P0 and P2 pellets from grade III and FWB cartilage. Overall, tissue and P0 pellets of grade IV tissue were positive for collagen type X and the staining intensity differed from grade III and FWB tissue sections (p<0.033) and P0 pellets derived from these locations (p<0.025) (Figs. 3 and 4). Interestingly, also, the NWB cartilage was positive, which was significantly different (p<0.033) compared to grade III and FWB tissue sections, for collagen type X staining. After culturing P0 or P2 cells in pellets, these differences were less clear (Fig. 3).
Additional CBFA1 staining showed positive staining in the majority of nuclei and cytoplasm of chondrocytes present in tissue samples derived from NWB and grade IV cartilage defects (Fig. 5). Also, in FWB tissue samples, some chondrocytes stained positive, whereas CBFA1 staining was negative in samples derived from grade III tissue sections (Fig. 5).
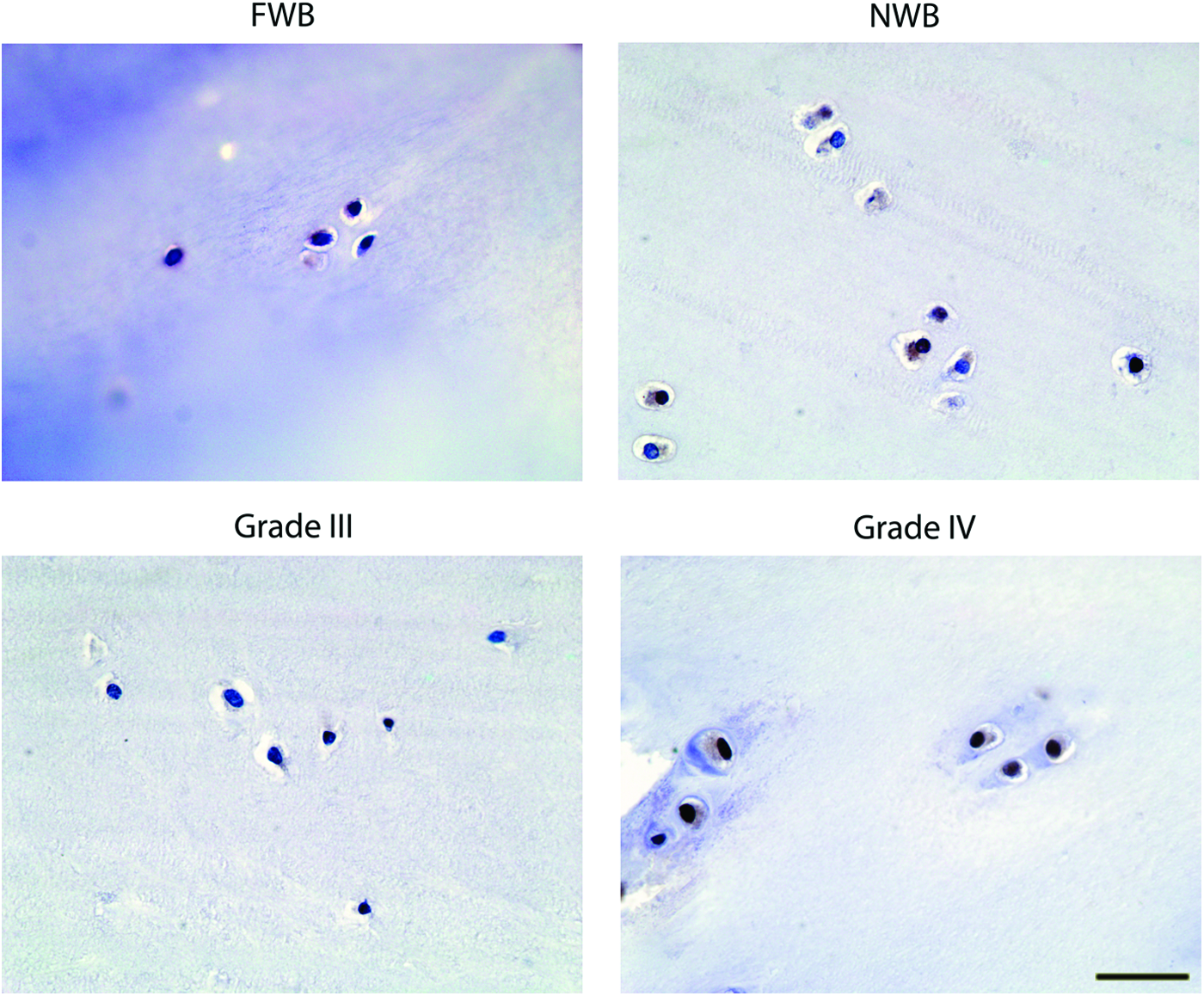
CBFA1 staining. CBFA1 staining for tissue sections of FWB, NWB, grade III and grade IV cartilage samples. At the NWB, grade IV and to a lesser extent some FWB cells, the nucleus, and cytoplasm of the chondrocytes show positive staining for CBFA1, whereas this was hardly seen in tissue sections derived from grade III cartilage defects. Scale bar at the right bottom represents 40 μm. Color images available online at www.liebertpub.com/tea
Gene expression in defect cartilage chondrocytes
To further analyze the nature of the differences in matrix production between the P0 chondrocytes from the defect locations, gene expression analysis for various differentiation and dedifferentiation markers was performed. Gene expression levels of MFAB-5 and collagen type I and collagen type II were higher (p<0.04) for freshly isolated P0 grade IV chondrocytes compared to grade III chondrocytes, whereas aggrecan expression and the identity index were lower (p<0.04) in the freshly isolated cells from grade IV compared to the freshly isolated cells from grade III (Fig. 6). The expression pattern of the P0 chondrocytes changed after 4 weeks of pellet culture. In contrast to the freshly isolated cells, the expression of the positive markers for chondrocyte biology (aggrecan, cartilage link protein, and collagen type II) was all higher (p<0.04) for the cells in the grade III P0 pellets compared to those in the grade IV P0 pellets (Fig. 6).
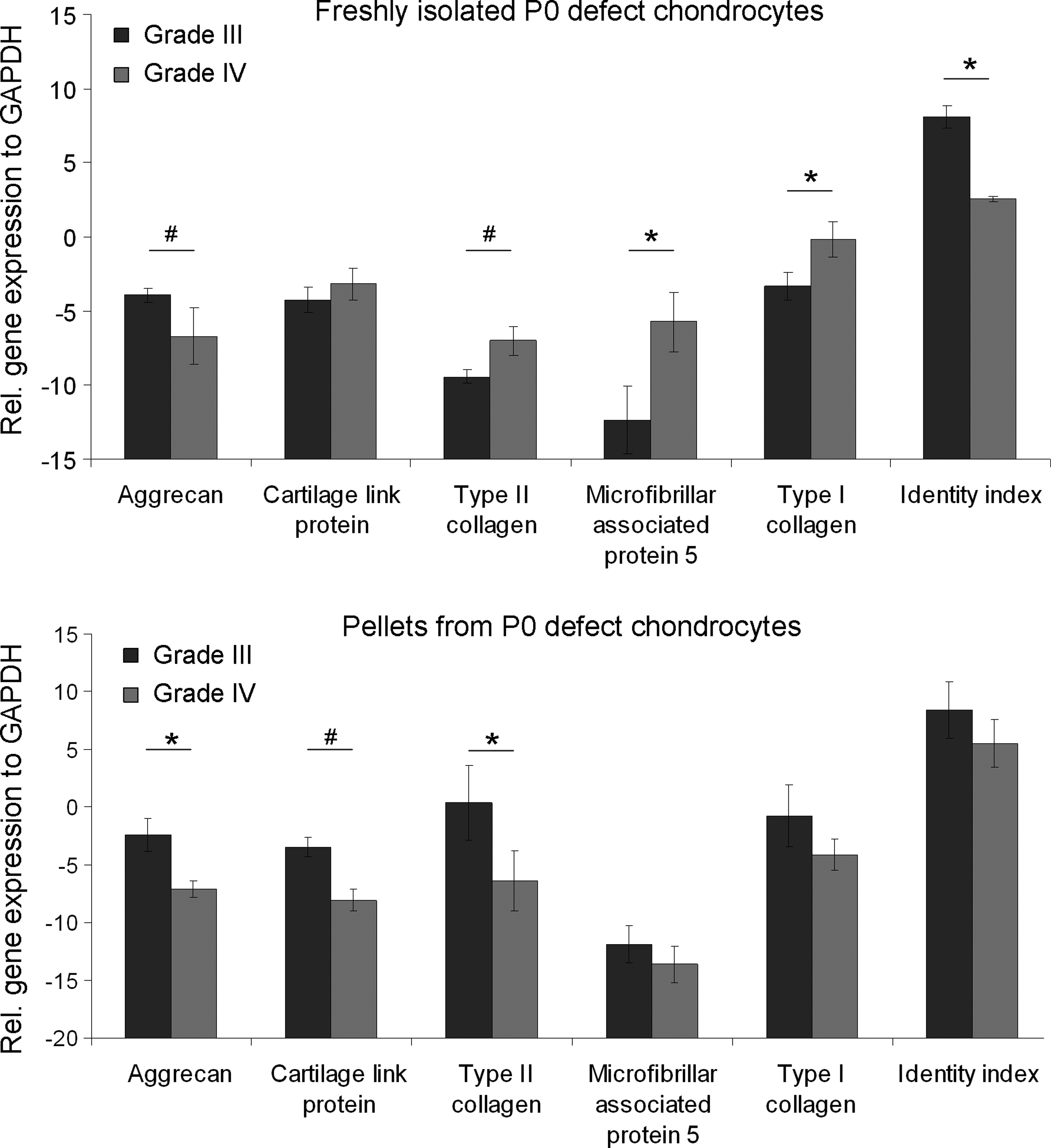
Gene expression in debrided defect chondrocytes. In freshly isolated grade IV (Gr IV) chondrocytes, the expression of microfibrillar associated protein 5 (MFAP5), collagen type I (COL1A1), and collagen type II (COL2A1) is higher, whereas the Identity index (HAPL1/MFAP5) and aggrecan (ACAN) expression is lower compared to grade III (Gr III) chondrocytes. The expression of positive markers of chondrocyte biology (ACAN, cartilage link protein [HAPLN1], COL2A1 is higher) in P0 pellets from grade III compared to grade IV chondrocytes. #p<0.04, *p<0.001.
Discussion
This study, for the first time, shows that NWB articular cartilage in the knee is a suboptimal source for chondrocytes for (matrix-assisted) autologous chondrocyte implantation (mACI), as shown by hypertrophic differentiation (positive collagen type X and CBFA1 staining) and decreased matrix production of unpassaged cells of this region. Moreover, unpassaged chondrocytes from debrided articular cartilage from Outerbridge grade III focal lesion were found to outperform cells from NWB locations in terms of cartilage-specific matrix production. Articular cartilage debrided from grade IV lesions showed, both in native tissue and after pellet culture, more deviations from a hyaline phenotype as judged by higher collagen type I and X and lower GAG content at the biochemical and histological level, compared to grade III and FWB tissue and pellets cultured from cells derived from the latter two locations. Also, cartilage-specific gene expression was lower in P0 pellets from grade IV chondrocytes compared to grade III chondrocytes. Compared to nonweight-bearing cartilage, which is the currently preferred biopsy site for ACI, chondrocytes from grade III lesions produced more GAGs when cultured at P0.
The observed differences in chondrogenic potential between grade III and grade IV derived chondrocytes were as expected and in line with the macroscopic appearance of the lesions in vivo. The fibrous-like morphology of the cartilage remnants in grade IV lesions fitted the observed fibrocartilaginous regeneration in pellets derived from these chondrocytes. Also, the high chondrogenic capacity of grade III derived chondrocytes was in line with the healthy appearing remnants of cartilage in these lesions.
Although not described before, the degenerative aspect of NWB cartilage does not come as a surprise. Articular cartilage adapts to the exposed loading patterns in life. 7 Habitual disuse of cartilage will lead to chondropenic changes in an overall macroscopically healthy joint, as previously shown for the articular cartilage of the hip and the lateral facet of the tibia.13,14 In this study, we showed similar findings for the NWB cartilage of the trochlea, which is the current biopsy site for regenerative cell-based cartilage surgery. Both terminal differentiation, as reflected by collagen type X production, and degeneration, shown by a decreased Safranin O staining, was observed in the NWB trochlear tissue. Moreover, this was accompanied by an actual change in cell phenotype as judged by the decreased capacity of the resident cells to generate hyaline cartilage tissue.
The use of debrided defect cartilage as a cell source for ACI has several advantages over chondrocytes derived from NWB cartilage. First, no difference in redifferentiation capacity was observed between passaged cells from debrided cartilage and NWB cartilage. Apparently, the dedifferentiation of chondrocytes due to the in vitro expansion is not dependent on the harvest location. This would indicate that at the passaged stage, the chondrocytes derived from a chondral lesion are as potent as those derived from macroscopically healthy NWB cartilage. Therefore, the use of chondrocytes from the debrided tissue from grade III or grade IV defects would be a logical adjustment to the ACI procedure, as no additional damage to the joint cartilage would need to be inflicted. A second advantage of using defect chondrocytes is the relatively large number that can be isolated from the debrided material. The standard trochlear cartilage biopsy for ACI yields around 0.18–0.46×106 chondrocytes, 16 requiring at least two passages, whereas the range of 0.96–3.1×106 cells isolated from the debrided focal defect cartilage in the current study would only need one passage to obtain enough cells for reimplantation. This is likely to enhance tissue quality, as dedifferentiation has been shown to increase and the redifferentiation capacity to decrease with each subsequent passage.17,24,25
For future applications where isolated cells are used without prior expansion, debrided defect cells would be suitable as well. The combination of freshly isolated chondrocytes with various other cell types as part of the new one-stage surgical-based approach toward ACI has recently gained attention and has been shown to improve cartilage matrix production.18,26–28 Partial replacement of articular chondrocytes by, for example, bone marrow or adipose-derived stem cells, would directly provide sufficient cells for reimplantation, thereby enabling a one-stage cell-based cartilage therapy. In this case, P0 chondrocytes of debrided grade III cartilage will have a clear advantage over the use of NWB chondrocytes, in addition to circumventing surgery-induced damage to the nonweight-bearing areas. Also, grade IV chondrocytes are suitable for such a one-stage procedure as their chondrogenic potential does not seem to be different from NWB chondrocytes. Further evaluation of the behavior of defect chondrocytes combined with, for example, bone marrow-derived stem cells may represent a logical next step toward a one-step cell-based cartilage therapy.
Finally, although this study was aimed at defining the best cell source for mACI, concerns may also be raised about other treatments for cartilage trauma, such as mosaicplasty procedures. During this procedure, osteochondral plugs from the NWB region are transplanted to the focal cartilage lesion. 29 Next to the frequently occurring donor-site morbidity, our results suggest that actually, cartilage in a chondropenic state is being used to fill the defect in this procedure. However, alternative harvesting sites are not available, unless of heterologous origin, which would entail other problems, such as risk of disease transmission and reduced functionality due to the required devitalisation procedures. Further research may be needed to indicate the necessity for such alternatives or the use of synthetic plugs.
In conclusion, this study shows that chondrocytes derived from debrided defect cartilage could, without loss of quality and quantity of cartilage-specific matrix production, be a suitable cell source for ACI. In addition, chondrocytes derived from different lesion grades were showed to harbor different chondrogenic potentials. Combined, these two observations could have major implications for future ACI treatments, in particular, those based on one-stage procedures.
Footnotes
Acknowledgments
The authors greatly acknowledge the support of the TeRM Smart Mix Program of the Netherlands Ministry of Economic Affairs and the Netherlands Ministry of Education, Culture and Science. L.B.C. is funded by the Dutch Arthritis Foundation.
Disclosure Statement
The authors have nothing to disclose and did not receive any financial support related to this work that could create a potential conflict of interest.