
Abstract
This study evaluated the osteoinductive effect of the recombinant human bone morphogenetic protein-2 (rhBMP-2)-coated biphasic calcium phosphate (BCP) carrier system on the grafted sinus area, including surrounding tissues and the Schneiderian membrane. A total of 18 male rabbits were used in this study; two for in vitro and 16 for in vivo experiments. Schneiderian membranes taken from two animals were cultured with or without rhBMP-2, and quantitative reverse transcriptase-polymerase chain reaction analysis was performed. Both maxillary sinuses in each of the 16 animals were used to compare the in vivo effects of rhBMP-2-coated BCP (experimental group) and BCP alone (control group). In each animal, rhBMP-2-coated BCP was grafted into one of the maxillary sinuses, and the same amount of BCP alone was grafted into the contralateral site in random order. Radiologic and histometric analyses were performed at 2 and 8 weeks after surgery. After 2 days of culturing with or without rhBMP-2, a significant increase in the expression of early osteoblasts (RUNX2, type I collagen, alkaline phosphatase, and osteopontin) could be observed. Different histologic healing patterns were observed in experimental and control sites: newly formed bone lining the reflected sinus membrane without bone formation was observed at the central areas of experimental sites (window=0.06%; center=0%; membrane=20.86% of new bone), whereas evenly distributed new bone formation was observed at the control sites (window=7.27%; center=7.41%; membrane=15.58% of new bone).The augmented volume was well maintained at both the experimental and control sites during the experimental period, but at 2 weeks, the augmented volume was greater at the experimental sites than at the control sites (232.62 and 195.29 mm3, respectively; p<0.001). These results suggest that good space maintenance in sinus augmentation is achieved with BCP, while the osteoinductive potential of the sinus membrane is activated at the early stage of healing with rhBMP-2.
Introduction
There have been many attempts at sinus augmentation using the recombinant human bone morphogenetic protein-2 (rhBMP-2) as an osteoinductive factor to accelerate bone regeneration,9–12 and rhBMP-2 with an absorbable collagen sponge (ACS) was approved for clinical use in sinus augmentation and ridge augmentation by the United States Food and Drug Administration (FDA) in 2007. 13 However, because of its rapid resorption rate and lack of structural durability, the clinical use of the ACS with rhBMP-2 has some limitations in sinus augmentation procedures.14,15 A previous study evaluating the stability of NB in the rabbit sinus after filling with blood clots found that the augmented height was significantly decreased during the early stage of bony regeneration. 16 In another previous study using a rabbit sinus model, rhBMP-2-loaded ACS also resulted in a reduced augmented membrane height in spite of rapid bone regeneration rate. 15 These findings suggest that the space making ability of the ACS is not sufficient for the sinus graft procedure.
Biphasic calcium phosphate (BCP) is a bone substitute material that comprises hydroxyapatite (HA) and β-tricalcium phosphate (β-TCP) in a specific ratio; its space-providing and osteoconductive properties have been well documented.17–20 BCP has been also used as a carrier for rhBMP-2 in the alveolar ridge defect 21 and spine fusion22,23 models. Jung et al. 24 evaluated rhBMP-2-loaded HA/TCP in the rabbit calvarial onlay model, and concluded that this might be an ideal carrier system for rhBMP-2.
An appropriate degradation rate of biomaterials is a requirement for the ideal carrier/scaffold. The resorption rate of BCP can be controlled by altering the ratio of HA and β-TCP. It has been found that BCP with a high ratio of HA results in successful bone regeneration in various types of osseous defect models.20,25–27 The HA content of the scaffold can help provide the space for a new bone formation; however, its low biodegradation rate means that the biomaterial could be left unresorbed over a prolonged period of time. 20 In contrast, a higher proportion of β-TCP in BCP increases the resorption rate, and therefore would be replaced more rapidly by NB. Ultimately, the desired outcome is the replacement of grafted biomaterials with natural bone structures containing osteons. Therefore, in the present study, we used BCP with a high β-TCP ratio as the carrier for rhBMP-2.
While soaking of BCP in a solution of rhBMP-2 is an FDA-approved loading method, there are concerns that this may result in uncontrolled flow and uneven distribution of the growth factor. 28 Kim et al. 28 introduced the use of BCP coated with Escherichia coli-derived rhBMP-2 (ErhBMP-2), which is easy to store and handle at room temperature. In that study, particle- and block-type graft materials loaded with rhBMP-2 using the soaking method exhibited enhanced bone induction in rat calvarial defects.
The purpose of the present study was to (1) elucidate the osteoinductive effect of ErhBMP-2 with the BCP carrier system on the grafted sinus area and surrounding tissues, including the Schneiderian membrane, and (2) to determine the space making ability of BCP in a standardized rabbit sinus model.
Materials and Methods
Animals
Thirty-six sinuses of 18 male New Zealand white rabbits weighing 2.5–3 kg were used, including two animals for the in vitro test and 16 animals for the in vivo test. Animals were housed in separate cages under standard laboratory conditions, with ad libitum access to water and a standard laboratory pellet diet. The animal selection and management, surgical protocol, and preparation followed routines approved by the Institutional Animal Care and Use Committee of Yonsei Medical Center, Seoul, Korea.
Preparation of ErhBMP-2-coated BCP particles
ErhBMP-2 was provided by the Cowellmedi research institute (Busan, Korea). Microporous BCP (particle type, 0.5–1.0 mm, 70% porosity; Bio-C, Cowellmedi) with a HA:β-TCP ratio of 3:7 was used as the ErhBMP-2 carrier. Details of the coating of BCP particles with ErhBMP-2 are available elsewhere. 28 Briefly, the ErhBMP-2 solution (0.67 mL in 1.5 mg/mL buffer) was added to 1 g of BCP particles and lyophilized in a freeze dryer. The solution was frozen by placing the ampoule on precooled shelves and cooling it to −43°C. The formulations were dried in a condenser at −40°C (primary drying) and maintained at this temperature for 3 h. They were then placed in a pressure chamber at 5 mTor for 2 h. Secondary drying was performed on a shelf using the following sequence: −20°C for 4 h, −10°C for 4 h, 0°C for 2 h, and 20°C for 20 h. The chamber pressure remained constant throughout the procedure.
In vitro culture
Schneiderian membranes from four normal sinuses of two animals were dissected for the in vitro test and washed in DMEM with 10% fetal bovine serum. Membranes were divided into several small pieces (3×3 mm) and cultured in vitro with the Trowell-type organ culture method in the osteogenic medium (containing α-MEM with 15% fetal bovine serum, 2 mM L-glutamine, 2 mM β-glycerophosphate, 100 mM L-ascorbic acid 2-phosphate, 10−8 dexamethasone, 55 mM 2-mercaptoethanol, 100 U/mL penicillin, and 100 mg/mL streptomycin) with/without ErhBMP-2 (10 μg/mL) for 2 days.
Quantitative reverse transcriptase-polymerase chain reaction analysis
RNA was extracted from the Schneiderian membrane at 2 days after being incubated in the osteogenic medium in vitro with or without the BMP protein (with BMP protein, n=8; without BMP protein, n=8).
Quantitative reverse transcriptase-polymerase chain reaction (RT-qPCR) was performed using a Thermal Cycler Dice Real-Time System and SYBR Premix EX Taq (Takara, Japan) according to the manufacturer's instructions. PCR amplification was performed with specific primers by using standard protocols; GAPDH forward: 5′-GAGCTGAACGGGAAACTCAC-3′, GAPDH reverse: 5′-CACTGTTGAAGTCGCAGGAG-3′, osteocalcin (BGLAP-like) forward: 5′-AGAGTCTGGCAGAGGCTCA-3′, osteocalcin reverse: 5′-CTCGCACACCTCCCTCTT-3′, osteopontin (SPP1) forward: 5′-GGCTAAACCCTGACCCATCT-3′, osteopontin reverse: 5′-GTGGTCATCGTCCTCATCCT-3′, type I collagen (COL1A1) forward: 5′-GGCGATCGTGGTGAGACT-3′, type I collagen reverse: 5′-ACCCTGGAGACCGGAGAA-3′, alkaline phosphatase (ALPL) forward: 5′-CGTGTTCACCTTTGGAGGAT-3′, alkaline phosphatase reverse: 5′-TTGTGAGCGTAGTCCACCAT-3′, RUNX2 forward: 5′-CCCTGAACTCTGCACCAAGT-3′, RUNX2 reverse: 5′-GTGCCTCGTGTGGAAGACA-3′. For RT-qPCR, the reaction mixture was initially incubated for 10 s at 95°C. The amplification program comprised 45 cycles of denaturation at 95°C for 5 s, annealing at 53°C–60°C for 20 s, and extension at 72°C for 20 s. The RT-qPCR for each sample was performed in triplicate and the amount of each of the RT-qPCR products was normalized using GAPDH as an internal control. The data were analyzed with the Thermal Cycler Dice Real-Time System analysis software and the 2−DDCt method. The statistical calculations were performed using the t-test of variables to determine significant changes at the 95% confidence level (p<0.05).
In vivo study design and surgical procedures
The overall surgical procedure followed the protocol of our previous study. 15 General anesthesia was induced via intramuscular injection, using a mixture of ketamine hydrochloride (Ketalar, Yuhan, Seoul, Korea) and xylazine (Rumpun, Bayer Korea, Seoul, Korea), and local anesthesia was administered with 2% lidocaine (lidocaine HCl, Huons, Seoul, Korea). Following shaving and local disinfection with iodine, a straight incision was made along the midline on the dorsal area of the nasal bone, and a full-thickness flap was elevated laterally to expose the nasal bone. A circular reamer (C-reamer, Neobiotech, Seoul, Korea) with a diameter of 5.5 mm that was designed to minimize membrane perforation was used to prepare the windows bilaterally. The positions of the windows were the same as those determined by Asai et al. 29 and Choi et al. 15 The prepared bony window was removed and the sinus membrane was carefully elevated. To ensure that the same histologic position was sectioned in each animal, metal pins (Dentium, Seoul, Korea) were inserted on the nasal midline between the prepared windows, at the central-most point of each circular window (Fig. 1).

Surgical procedure.
In each animal, each of the sinuses was randomly allocated to either the ErhBMP-2 or control (BCP alone) group (thus, both the experimental and control groups were represented in each animal). In the ErhBMP-2 group, 0.15 g of graft material (BCP coated with ErhBMP-2) was inserted to the sinus, so that 150 μg of ErhBMP-2 was applied. In the contralateral sinus, 0.15 g of uncoated BCP was grafted as a control. After implantation of the graft material, the flap was sutured layer by layer with 4-0 monosyn (glyconate absorbable monofilament; B-Braun, Aesculap, PA). The animals were sacrificed at 2 weeks (n=8) or 8 weeks (n=8) postoperatively by an anesthetic overdose.
Radiographic analysis with microcomputed tomography
Block sections, including the experimental site and the surrounding area were removed and immediately fixed in 10% buffered formalin for 10 days. Microcomputed tomography (micro-CT, Skyscan 1072; Skyscan, Aartselaar, Belgium) images of these block specimens were then taken at a resolution of 35 μm (100 kV and 100 μA). The scanned CT images were processed in the DICOM format and three-dimensionally reconstructed with PC-based software (On-Demand3D; Cybermed, Seoul, Korea).
Both sides of the sinuses were visualized using the threshold of 275, as mentioned in previous publications. 30 The augmented area inside of the nasal bone was identified and color coded using the software program; the experimental and control sinuses were colored in red and blue, respectively. The volumes of the colored areas were calculated automatically (in mm3).
Histologic and histomorphometric analyses
The rinsed block sections were decalcified in 5% formic acid for 14 days, and then embedded in paraffin. Serial 5-μm-thick sections were cut coronally along the center of the window. The two central-most sections were selected from each block, and stained with hematoxylin–eosin and Masson's trichrome. The histologic slides were observed and the images were digitally acquired with the aid of a light microscope (BX50; Olympus, Tokyo, Japan).
Histomorphometric measurements of the captured images were made using a PC-based image analysis system (Image Pro Plus; Media Cybernetics, Silver Spring, MD). The composition of the total augmented sinus was identified, and the relative areas of NB, residual materials (RM), and soft tissue (ST) were separately detected and calculated (in mm2). The total area of the augmented sinus was measured and the proportions (in%) of each composite (i.e., NB, RM, and ST) were obtained. To evaluate the distribution of regenerated bone in the grafted sinus area as a secondary outcome variable, the above-mentioned parameters were measured in specific standardized areas of window, central, and membrane regions. The areas were randomly selected and photomicrographs were taken in original magnification ×200. The window region was selected within the grafted area interfacing the imaginary extensions of the pre-existing cortical bone at the margins of the window, and the center region was at the middle of the whole augmented sinus. The membrane region was chosen from just above the Schneiderian membrane. (Fig. 2).

Histomorphometric analysis. The proportions of NB and graft RM were measured on the total augmented area (dotted line), and three randomly selected regions
Statistics
The statistical analysis was performed using a standard software program (SPSS 15.0; SPSS, Chicago, IL). Independent t-tests were carried out to compare the results obtained from RT-qPCR in ErhBMP-2-treated and control tissues, and in vivo test at 2 and 8 weeks. Paired t-tests were used to evaluate the differences between ErhBMP-2-treated and control groups in in vivo tests (p<0.05). The data are presented as mean±SD values.
Results
Quantitative RT-PCR
Quantitative RT-PCR with RNA extracted from the Schneiderian membrane of adult rabbits showed an extensively increased expression of early osteoblasts, such as RUNX2, type I collagen, alkaline phosphatase, and osteopontin. However, the expression level of late osteoblasts like osteocalcin was not significantly changed by BMP. (Fig. 3).

Osteoblastic gene transcriptional changes in the Schneiderian membrane after treatment of Escherichia coli-derived rhBMP-2 (ErhBMP-2). Quantitative reverse transcriptase-polymerase chain reaction (RT-qPCR) analysis shows the significant upregulation of RUNX2, type I collagen (COL1A1), alkaline phosphatase (ALPL), and osteopontin (SPP1) after treatment of ErhBMP-2 for 48 h (asterisks, p<0.05). The expression level of osteocalcin (BGLAP-like) was not evidently changed after ErhBMP-2 treatment. Error bars indicate standard deviations on the normalized ratio.
In vivo test
Clinical observations
During the surgical procedure, membrane perforation of less than 1 mm occurred in two sinuses from the 2-week survival group: one in the ErhBMP-2-treated group and the other in the control group. All of the rabbits recovered well and without any adverse healing events such as wound dehiscence or postoperative infection.
Radiographic analysis: micro-CT
The sinus cavity was filled with radiopaque materials in all groups. Internally, the augmented sinus had a dome shape (Fig. 4A, B). At 2 weeks after surgery, the three-dimensionally reconstructed appearance of the augmented sinuses differed between the experimental and control groups. The spherical shape of the grafted biomaterials was clearly evident in the control group, and the implanted materials resided within high density. In contrast, RM were only sparsely observed in the ErhBMP-2-grafted sinus, and the surfaces of augmented sites exhibited a finely irregular appearance. At 8 weeks of healing, the appearance and surface of the augmented areas in both the experimental and control sites were similar.

Radiographic analysis. The augmented sinuses were identified and color coded on three-dimensionally reconstructed micro-CT images. The experimental (ErhBMP-2-treated) sinus was coded in red, and the contralateral, control (biphasic calcium phosphate [BCP]-alone) sinus was coded in blue.
The measured total augmented volume (in mm3) of each group is shown in Figure 4C. At the 2-week healing point, the volume of the augmented sinus was significantly larger in the ErhBMP-2-treated group (232.62±23.24 mm3) than in the control group (195.29±42.32 mm3; p<0.001). Conversely, there was no significant difference between the ErhBMP-2 and control groups at the 8-week healing point (227.72±52.59 vs. 223.24±17.37 mm3, p=0.434). The change in dimensions of the experimental sites between the two observation periods was also analyzed. The volume in the control group increased significantly as time passed (p=0.012), while there was no significant difference in dimensions in the ErhBMP-2-grafted sinus, although the volume appeared to have slightly decreased at 8 weeks (p=0.06).
Histologic observations
NB and RM were seen in both the ErhBMP-2 and control groups at the 2-week healing point (Fig. 5). The cross-sectional shape of the augmented sinus was convex in all animals, and the window area was not yet completely regenerated. The Schneiderian membrane was intact, with no signs of inflammation; numerous serous glands could be seen. The sinus shape in the two rabbits that experienced membrane perforation during the surgical procedure was the same as that in the unperforated rabbits.
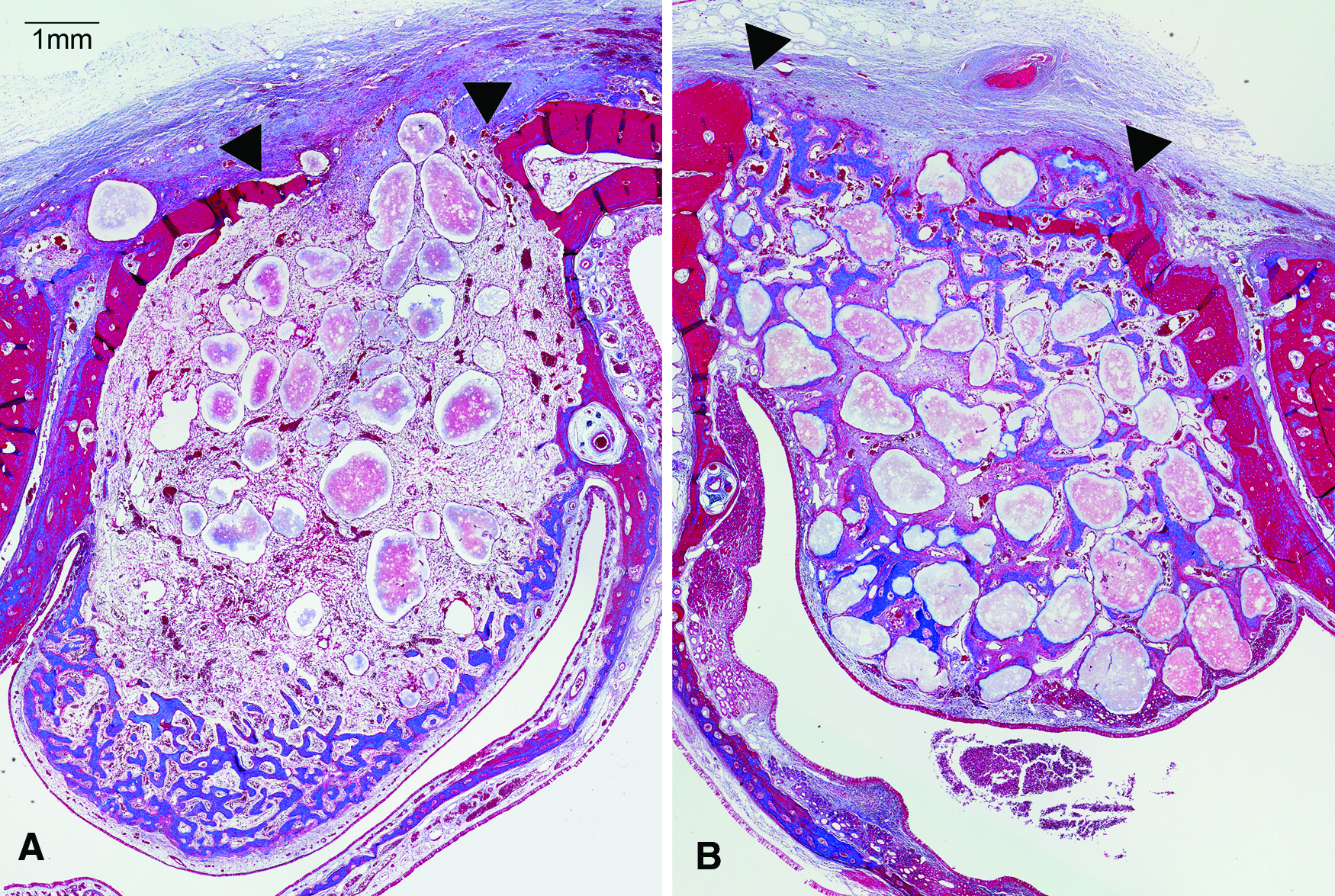
Histologic findings after 2 weeks of healing. NB and RM were seen in both groups. The surgically created windows were clearly distinguished (arrowheads).
Regenerated bone was found mostly near the sinus membrane in the ErhBMP-2 group (Fig. 5A). A trabecular pattern of NB was observed along the Schneiderian membrane and in direct contact with it. In contrast, there was no evidence of regenerated bone in the window and central regions. The RM were sparsely observed, and extensive blood vessels and connective tissues filled in the space between the biomaterials. The remaining BCP particles were irregular in shape with unclear edges (Fig. 6A, C, E).
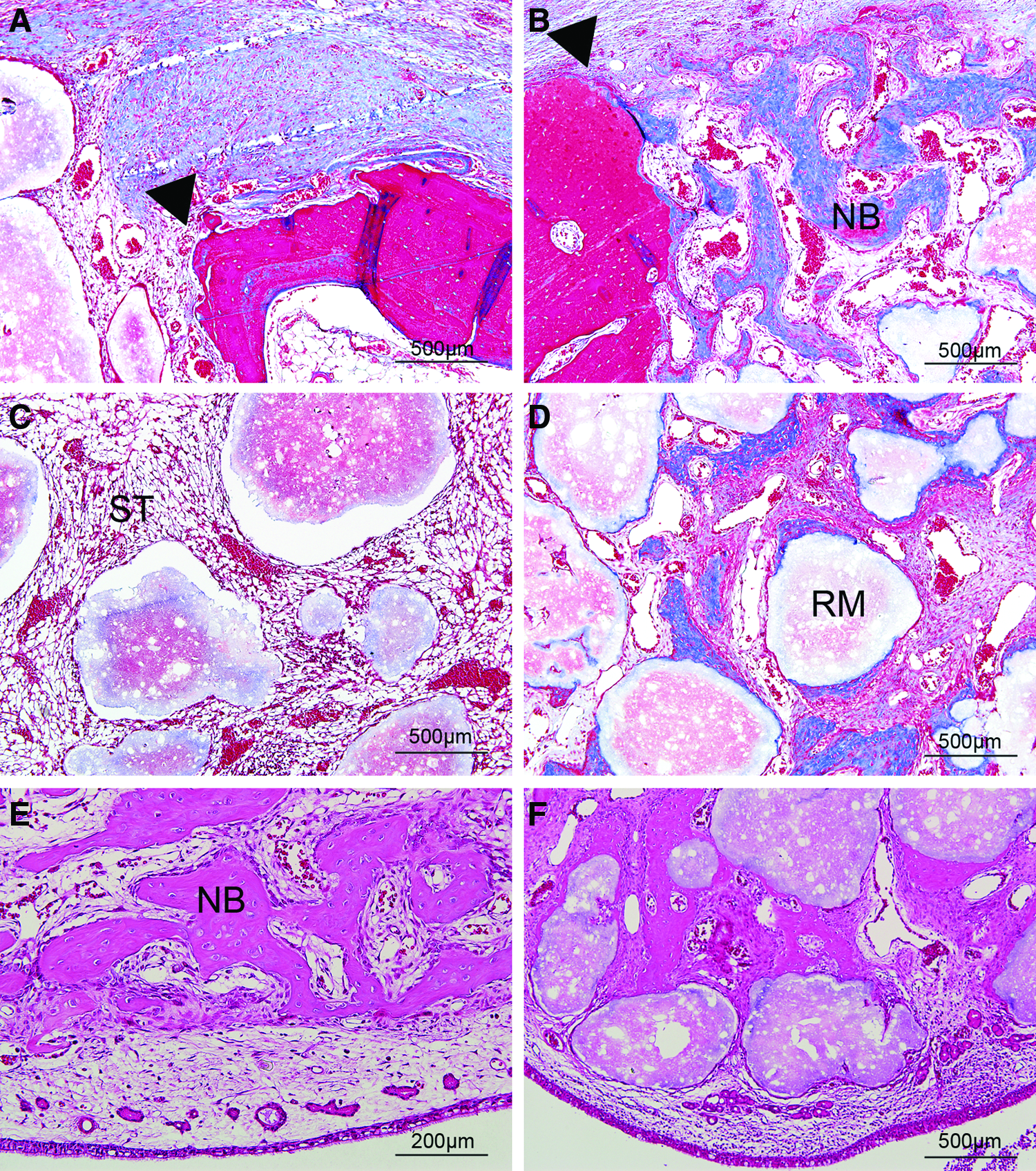
Histologic findings after 2 weeks of healing. The regenerated sinus was divided into three regions: window
Regenerated bone was observed all around the augmented area in the control group (Fig. 5B). However, NB was observed more extensively at the area adjacent to the existing alveolar bone rather than along the Schneiderian membrane (Fig. 6B, D, F). NB sprouted out from the lateral surface inside of the augmented sinuses. There were more BCP particles in the sinus sites of the control group than the ErhBMP-2 group. In addition, remnant particles were larger and they were closer to each other at the control sites than at the ErhBMP-2-treated sites.
The two groups exhibited a similar pattern of bone formation and appearance of RM at the 8-week healing point (Fig. 7). The newly formed woven bone was replaced by the lamellar bone, and a trabecular pattern was observed. The intertrabecular space was filled with RM, fibrovascular tissue, and bone marrow. The window area was almost completely closed with NB, and corticalization between the prepared sites had restored the original curvature of the nasal bone.
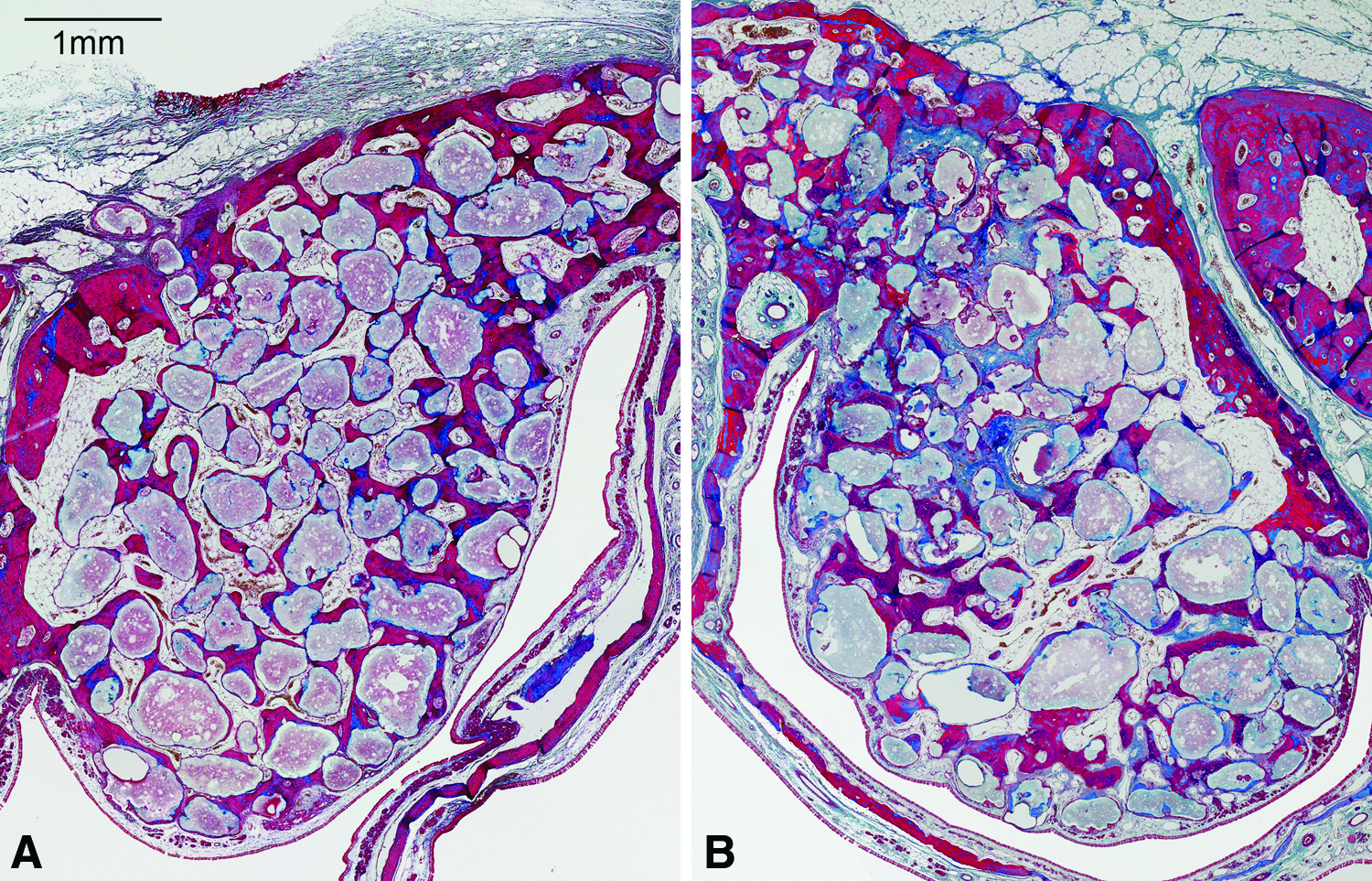
Histologic findings after 8 weeks of healing. The NB was the lamellar bone, and a trabecular pattern was observed. The intertrabecular space was filled with RM, fibrous tissue, and bone marrow. The window area was almost completely closed.
Histomorphometric analysis
The differences in the total area of augmented sinus (Fig. 8) confirmed the radiographic volumetric analysis. The total augmented area at the 2-week healing point was significantly larger in the ErhBMP-2 group (43.02±7.90 mm2) than in the control group (29.64±6.64 mm2; p<0.001). At the 8-week healing point, this parameter did not differ significantly between the two groups.
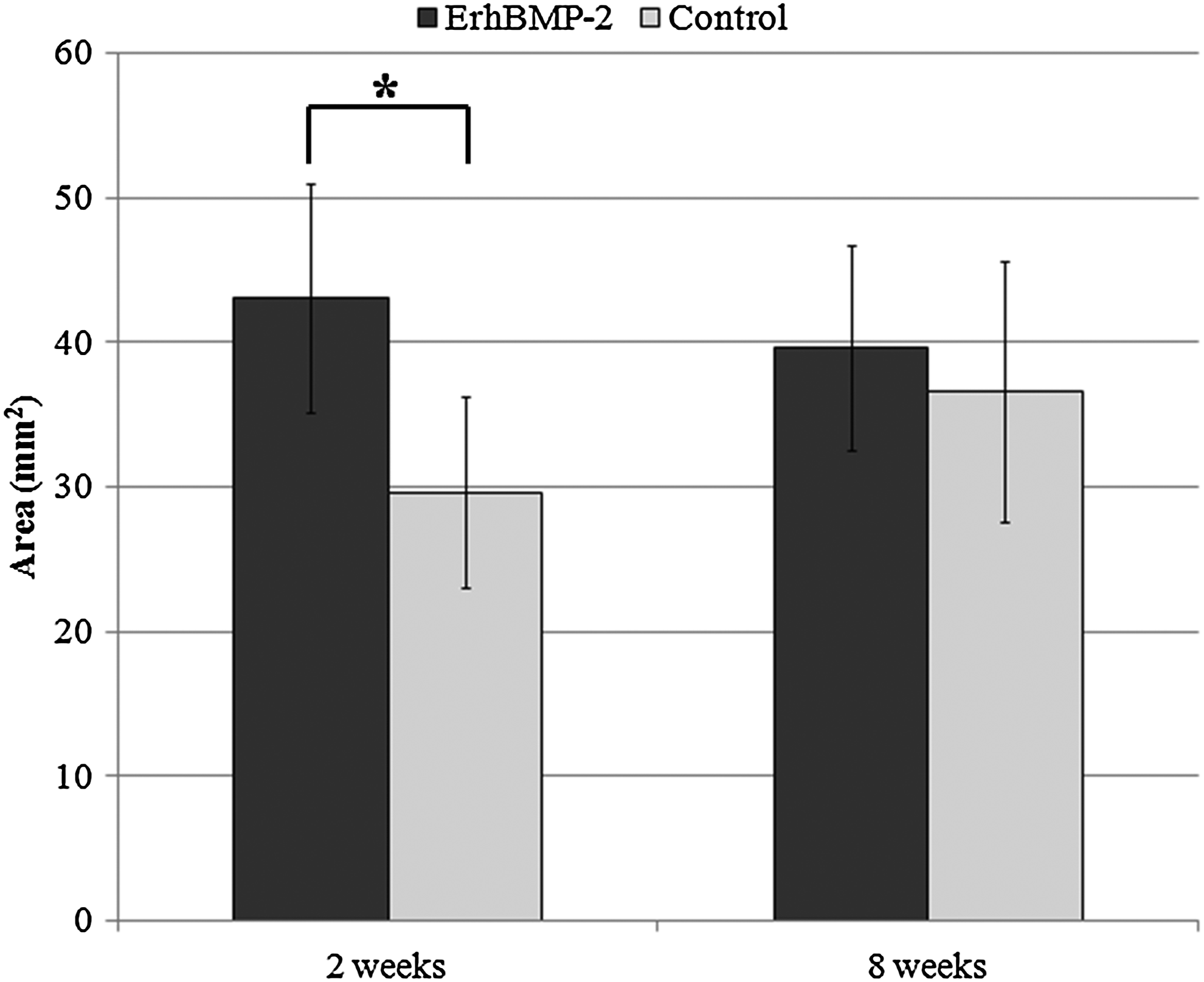
Total area. The total augmented area was larger in the ErhBMP-2 group than in the control group at the 2-week healing point (p<0.001), but did not differ between the two groups at the 8-week point.
The results of the histomorphometric analysis in specific regions are summarized in Figure 9 and Tables 1–4. At the 2-week healing period, the proportions of NB, RM, and ST in the totally augmented area differed between the ErhBMP-2 and control groups (Fig. 9A, Table 1). The proportions of NB and RM were greater in the control group than in the ErhBMP-2 group (p=0.013 and 0.002, respectively). Likewise, there were significant differences in the relative area of NB between the control and ErhBMP-2 groups in specific regions at the 2-week healing point (Fig. 9B–D, Tables 2–4). Typically, the results in the membrane region of all of the samples were opposite those seen in the window and central regions. Although NB was minimally observed at the window and central regions in ErhBMP-2-grafted sinuses, a significantly increased amount of NB was evident along the Schneiderian membrane of ErhBMP-2-grafted sinuses (p=0.031). At the 8-week healing point, the sinuses of the two groups were filled with similar compositions of NB, RM, and ST.

Fraction of the augmented area.
Significantly different from the group with the same protocol at 8 weeks (p<0.05).
Significantly different from the group with the control group at the same observation period (p<0.05).
NB, newly formed bone; RM, residual materials; ST, soft tissue; ErhBMP-2, Escherichia coli-derived rhBMP-2.
Significantly different from the group with the same protocol at 8 weeks (p<0.05).
Significantly different from the group with the control group at the same observation period (p<0.05).
Significantly different from the group with the same protocol at 8 weeks (p<0.05).
Significantly different from the group with the control group at the same observation period (p<0.05).
Significantly different from the group with the control group at the same observation period (p<0.05).
Significantly different from the group with the same protocol at 8 weeks (p<0.05).
Discussion
ErhBMP-2-coated BCP particles were used in the present study to reinforce the space-making ability and enhance the bone quality in sinus augmentation. Using the ACS carrier for rhBMP-2 accelerated bone regeneration, but a large amount of shrinkage was also observed in the rabbit sinus model. 15 In the present study, the grafted BCP maintained the augmented volume, with excellent NB occurring during the experimental periods. No reduction of the augmented volume was observed; rather, the total volume of sinus was increased in the control group. This finding might be associated with the increased new bone volume being added to the maintained BCP volume. Thus, BCP appears to be a better carrier than ACS with respect to volume maintenance. However, it failed to show the superiority of ErhBMP-2-coated BCP to the control in bone formation. Contrary to our expectation of accelerated bone formation in the experimental group, there was little bone formation around the ErhBMP-2-coated BCP particles at the 2-week healing point.
The differences in healing patterns between the two treatment groups at the early stage are notable. The augmented volume and area were larger in the ErhBMP-2 group than in the control group at the 2-week healing point. These findings were attributed to postoperative swelling at the surgical site. Although many studies have shown that rhBMP-2 has osteoinductive potential, complications such as postoperative swelling have also been reported.31–33 The amount of swelling is thought to depend upon the total dose of rhBMP-2 delivered to the surgical site. 31
Our histologic and histomorphometric analyses revealed specific atypical features in the ErhBMP-2 group at the 2-week healing point. Little NB was found around the lateral bony wall and the grafted BCP, while most of the NB was formed along the reflected Schneiderian membrane without the intervention of BCP particles. On the other hand, newly formed trabecular bone projected from the lateral bone to the center of the sinus in the control group, and was in direct contact with the grafted BCP particles near to the parent bone. The orientation of bone healing appeared to differ between the two groups.
Some researchers have proposed that the Schneiderian membrane contains osteogenic progenitor cells, and that bone regeneration originates from the sinus membrane.34–36 Srouji et al. 34 evaluated the cells derived from the human maxillary sinus membrane, and found that these cells were positive for mesenchymal stem cell markers, and underwent osteogenic differentiation both in vitro and in vivo. However, another recent in vivo study revealed limited influence of the Schneiderian membrane on bone formation after sinus floor elevation. 37 The results of the present study could support these two opposite studies, which showed different healing patterns around the Schneiderian membrane in ErhBMP-2-treated and control sites. A seam of NB was found along the Schneiderian membrane in the experimental group of the present study, even at 2 weeks. Results from RT-qPCR also showed increased expression of early osteoblasts, such as RUNX2, type I collagen, alkaline phosphatase, and osteopontin. It can be assumed that ErhBMP-2 might provoke osteogenic differentiation of progenitor cells of the Schneiderian membrane in the early healing phase. From the clinical point of view, early corticalization of the outer sinus surface could protect the augmented space from the volume shrinkage by remodeling or the pressure during respiration. Therefore, it may provide a suitable environment for increasing the bone formation throughout the grafted area.
On the other hand, most bone substitute materials such as BCP are osteoconductive materials that cannot induce a new bone formation on their own. The trabecular bone sprouted mainly from the lateral bony wall in the control group, and less bone formation was observed around the Schneiderian membrane in the control group compared with the experimental group.
The experimental and control groups showed similar results at 8 weeks, unlike at 2 weeks, where a significant difference between the two groups was shown. The remaining materials were rather increased in the membrane region of the ErhBMP-2 group compared to 2 weeks. It can be assumed that the new bone layer formed in the early stage in the membrane region has been resorbed due to pneumatization caused by air pressure during the remodeling process. Nevertheless, the total augmented volume was only slightly decreased because of the space-making ability of BCP particles. This suggests that the ratio of remaining particles might be higher at 8 weeks in the ErhBMP-2 group.
Our results demonstrate an osteoinductive effect of ErhBMP-2 in the membrane region, but the total amount of NB was less in the ErhBMP-2 group than in the control group at the 2-week healing point, although it was similar at 8 weeks. In contrast to the membrane region, the center region of the experimental group was filled mainly with the connective tissue and carrier materials. There were many blood vessels, and the density of particles was lower than that in the control group. RhBMP-2 is known to induce both angiogenesis and osteogenesis, through chemotaxis of osteoblasts and endothelial cells. 38 It is inferred that swelling by angiogenesis and chemotaxis of rhBMP-2 may have resulted in the relatively sparse presence of the particles.
It is unclear why the new bone formation did not occur around the graft particles in the experimental group at 2 weeks. One possibility is that the high dose of rhBMP-2 impaired healing. The effective dose of BMP-2 is known to differ between species and in various types of animal models. In general, a much smaller amount of rhBMP-2 is sufficient to induce bone formation in small animals such as rabbits than in human beings. BCP particles coated with 1.5 mg/mL of the ErhBMP-2 solution were grafted in this study; it is possible that this constitutes an overdose in rabbits. Zara et al. 33 reported on the adverse effects of high-dose BMP-2. They found that BMP-2 had dose-dependent side effects, such as cyst-like bone void formation. In the present study, it can be assumed that the membrane region spatially distant from the particles was stimulated by the diluted signal of the released rhBMP-2, while osteogenic differentiation was inhibited at the area near to the particle due to the high concentration of rhBMP-2. The other possibility is that the method used to load the rhBMP-2 molecule onto the BCP particles in the present study—whereby the rhBMP-2 solution was lyophilized to the BCP particle surface—or the process of its release altered the biological activity of the rhBMP-2 molecules. Further study is required to clarify these potentially adverse effects.
Conclusion
Within the limitations of the study, it can be concluded that BCP exhibits good space maintenance in sinus augmentation, and that ErhBMP-2 may stimulate the osteoinductive potential of the sinus membrane at the early stage of healing, although there was no significant superiority in ultimate bone formation.
Footnotes
Acknowledgment
This research was supported by a Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education, Science, and Technology (no. 2011-0007795).
Disclosure Statement
No competing financial interests exist.